Assessment of weight gain during pregnancy
in general prenatal care services in Brazil
Avaliaç ão d e g anho p o nd e ral intra-g e stac io nal
e m se rviç o s d e assistê nc ia p ré -natal no Brasil
1 Departam en to de Medicin a Social, Facu ld ad e d e M ed icin a, U n iversid ad e Fed eral d o Rio Gran d e d o Su l. Av. Ram iro Barcelos 2600, sala 414, Porto Alegre, RS 90035-003, Brasil. 2 U n iversid ad e d e Fortalez a. Ru a Dr. José Lou ren ço 1500, sala 501, Bloco A, Fortalez a, CE 60115-281, Brasil.
Lu cian a Bertold i N u cci 1 Bru ce Barth olow Du n can 1 Sotero Serrate M en gu e 1 Lean d ro Bran ch tein 1 M aria In ês Sch m id t 1 En i Teresin h a Fleck 2
Abstract Obesity is an em ergin g m ajor h ealth risk for w om en arou n d th e w orld . In th is regard , little atten tion h as been given to p regn an cy, a m om en t of risk n ot on ly for m ajor w eigh t gain in th ese w om en , bu t also for m acrosom ia in th eir offsp rin g. Th e objective of th is stu d y is to evalu ate w eigh t gain d u rin g p regn an cy. Data p ertain s to a coh ort of p regn an t w om en atten d in g gen -eral p ren atal care clin ics in six state cap itals in Braz il, from 1991 to 1995. W e stu d ied w om en aged 20 years an d ov er w it h sin glet on p regn an cies an d n o d iagn osis of d iabet es ou t sid e p reg-n areg-n cy, ereg-n rolled at ap p roxim ately 20 – 28 w eek s of gestatioreg-n . Accord ireg-n g to th e Ireg-n stitu te of M ed i-cin e criteria, 38% (95%CI: 36-40%) of th e w om en stu d ied gain ed less an d 29% (95%CI: 28-31%) h ad m ore t h an t h e recom m en d ed t ot al w eigh t gain . Th ese p rop ort ion s v ary accord in g t o p re-p regn an cy n u trition al statu s. Giv en th e in creasin g ere-p id em ic of obesity, th e h igh re-p rev alen ce of overw eigh t an d obesity in Braz ilian w om en p rior to p regn an cy, an d th e lack of ach ievem en t of recom m en d ed w eigh t ga in d u rin g p regn a n cy, m ore effect iv e m ea n s of m a n a gin g w eigh t ga in d u rin g p regn an cy are n ecessary.
Key words Obesity; Pregn an cy; W eigh t Gain ; Bod y M ass In d ex
Resumo Obesid ad e é u m fator d e risco p ara a saú d e d a m u lh er qu e vem crescen d o em m u itos p aíses. A esse resp eito, p ou ca aten ção real tem sid o d ad a à gravid ez , u m m om en to d e risco n ão a p en a s p elo elev a d o ga n h o d e p eso d a s m u lh eres, m a s t a m b ém p ela m a crossom ia em seu s recém -n ascid os. O objetivo d este estu d o é avaliar o gan h o d e p eso d u ran te a gravid ez . Trata-se d e u m estu d o d e coorte d e m u lh eres aten d id as em serviços d e p ré-n atal geral d o Sistem a Ún ico d e Sa ú d e, em seis ca p it a is b ra sileira s, en t re 1991 e 1995. Pa rt icip a ra m d a p esq u isa m u lh eres com 20 ou m ais an os d e id ad e, sem d iagn óstico d e d iabetes fora d a gravid ez , com ap roxim ad a-m en te 21-28 sea-m an as d e gestação, sea-m gestações a-m ú ltip las. De acord o coa-m o critério d o In stitu te of M ed icin e, 38% (IC95%: 36-40%) d as m u lh eres estu d ad as gan h aram abaixo e 29% (IC95%: 28-31%) acim a d o gan h o total recom en d ad o. Essas p rop orções variam d e acord o com as categorias d e p eso p ré- gra v íd ico. Da d o o a u m en t o n a ep id em ia d e ob esid a d e, a a lt a p rev a lên cia d e so-brep eso e obesid ad e p révios à gravid ez em m u lh eres brasileiras e a falta d e con trole d o gan h o d e p eso recom en d ad o d u ran te a gestação, p od ese ver qu e m eios m ais eficien tes d e con d u zir o gan -h o d e p eso d u ran te a gestação são n ecessários.
Introduction
Ob esity, wh ich con fers in creased risk for severa l d isesevera ses – severa m o n g th em d isevera b etes severa n d co ro -n ary h eart d isease, is a-n i-n creasi-n gly com m o-n con d ition . Accord in g to th e World Health Orga-n iza tio Orga-n ( WH O, 1998), th is iOrga-n crea se ca Orga-n b e ch a ra cterized a s a p a n d em ia o f m a jo r p u b lic h ea lth co n cern . Da ta co n cern in g over weigh t an d ob esity in recen tly p u b lish ed stu d ies sh ow over on e-th ird of th e ad u lt p op u lation in m an y co u n tries to b e over weigh t (Al-Isa , 1998; Alli-son et al., 1997; Flegal et al., 1998; Foreyt & Pos-ton , 1998; Grol et al., 1997; Rozowski & Arteaga, 1997). Alth o u gh th e p reva len ce o f o b esity is greater in m ore d evelop ed cou n tries, it h as in -crea sed d ra m a tica lly in severa l d evelo p in g cou n tries over recen t d ecad es (WHO, 1998).
Usin g WHO weigh t sta tu s criteria , d efin ed as a b od y m ass in d ex (BMI) of < 18.5kg/ m2for u n d er weigh t, ≥25.0kg/ m2a n d < 30kg/ m2fo r p re-ob esity, an d ≥30.0kg/ m2for ob esity (NIH/ NH LBI, 1998; WH O, 1998), th e freq u en cy o f ob esity am on g Brazilian wom en , for exam p le, in crea sed over 60% fro m 1975 to 1989 (Mo n -teiro et a l., 1995; Sich ieri et a l., 1994). A m o re recen t su r vey in th e No rth ea st a n d So u th ea st region s of th e cou n try con firm s a con tin u ed in -crease in ob esity am on g Brazilian wom en of re-p rod u ctive age esre-p ecially am on g th e econ om i-ca lly less p rivileged , su ggestin g th a t th e freq u en cy of ob esity con tin u es to in crease (Mon -teiro et al., 2000).
Th e u p p er lim it of th e id eal weigh t (or BMI) fo r a wo m a n wh o wa n ts to b eco m e p regn a n t a n d th e m a xim u m id ea l weigh t ga in d u rin g p regn an cy h ave received relatively little stu d y (IOM, 1990; Rosso, 1985). As th e m oth er is th e on ly sou rce of fetal n u trition , trad ition al con -cern h as focu ssed u p on b ein g u n d erweigh t for p re-p regn a n cy a n d low weigh t ga in d u rin g p regn an cy (Cn attin giu s et al., 1998). In con so-n aso-n ce with th ese coso-n cerso-n s, recom m eso-n d ed ges-ta tio n a l weigh t ga in n ea rly d o u b led fro m th e 1930’s through the 1980’s – from 6.8kg to a ran ge o f 11.4kg to 15.9kg. However, so cio eco n o m ic d evelo p m en t a n d fo o d su p p lem en ta tio n p ro gra m s h a ve red u ced th e in cid en ce o f in tra -u terin e growth retard ation , com m on ly eval-u at-ed by low b irth weigh t for gestation al age (IOM, 1990). Th u s, m o re recen tly, co n cern o f excessive gesta tio n a l weigh t ga in h a s received in -creasin g atten tion .
Bra zil is a ver y h etero gen eo u s co u n tr y. Prob lem s of ob esity a n d excessive gesta tion a l weigh t gain coexist with low n u trition an d in -su fficien t gestation al weigh t gain . Th ou gh b oth co n d itio n s a re a sso cia ted with p ro b lem s o f
grea t p u b lic h ea lth co n cern , th e freq u en cy o f in su fficien t a n d excessive ga in a m o n g Bra zil-ian p regn an t wom en h as yet to b e rep orted in a large, m u lti-cen ter stu d y.
Th e o b jective o f th is stu d y is to eva lu a te gesta tio n a l weigh t ga in in wo m en a tten d in g p re-n atal clin ics of th e n ation al h ealth system in d ifferen t state cap itals of Brazil.
M ethods
Data from a coh ort stu d y of con secu tive p regn aregn t wom eregn are p reseregn ted . Th e stu d y was coregn -d u cte-d in gen eral p ren atal care clin ics (Sistem a Ú n ico d e Saú d e– SUS) in six sta te ca p ita ls o f Brazil, from 1991 to 1995. A total of 5,564 wom en a ged 20 yea rs a n d over, a p p roxim a tely 20-28 weeks p regn a n t with n o d ia gn o sis o f d ia b etes o u tsid e p regn a n cy were in ter viewed a n d h a d an th rop om etric m easu res ob tain ed . Of th is to-tal, 73 wom en were exclu d ed d u e to n o record of m easu red weigh t after week 20 of gestation , 248 d u e to m issin g in fo rm a tio n n ecessa r y to ca lcu la te p re-p regn a n cy BMI a n d 51 wo m en b eca u se o f m u ltip le gesta tio n . Da ta o n p re-p regn an cy BMI th u s re-p ertain to 5,192 wom en .
All a d d itio n a l p regn a n cy d a ta were o b -ta in ed th ro u gh ch a rt review, wh ich wa s n o t a va ila b le fo r m a n y wo m en , p rin cip a lly d u e to th e facts th at th eir p re-n atal visits an d d eliver-ies o ccu rred in o th er ser vices o r th a t th ey re-tu rn ed in freq u en tly for fu rth er p re-n atal care. Fo r ca lcu la tio n s p erta in in g to weigh t ga in , 1,123 (22%) wom en were th u s exclu d ed for n ot h avin g a record ed weigh t b eyon d th e 28th ges-ta tion a l week. For ca lcu la tion s of toges-ta l weigh t gain , 987 (19%) ad d ition al wom en were exclu d -ed for lack of su fficien t m easu rem en ts to esti-m a te 3rdtrim ester ga in or la ck of in form a tion o n gesta tio n a l a ge a t b irth , lea vin g 3,082 fo r an alyses.
At en rollm en t, a stan dardized qu estion n aire was com p leted in clu d in g in form ation on p re-p regn an cy weight. Weight an d height were m ea-su red in d u p licate accord in g to a stan d ard p rotocol. Th e in terviewer defin ed eth n icity accord -in g to th e color of th e p articip an t’s sk-in .
with n eo n a ta l exa m in a tio n o r u terin e h eigh t fo r 22%; a n d o n a n u ltra so u n d a fter week 26 co n sisten t with n eo n a ta l exa m in a tio n o r la st m en stru a l p erio d fo r 14%. In th e rem a in in g 12% of p regn an cies, gestation al age was b ased o n ju st o n e criterio n (eith er u terin e h eigh t, n eo n a ta l exa m in a tio n , u ltra so u n d a fter week 26 or last m en stru al p eriod ).
Pre-p regn a n cy weigh t wa s self-rep o rted . Pre-p regn an cy weigh t statu s was classified ac-cord in g to th e WHO (1998) recom m en d ation s, an d , to p erm it com p arison s with recom m en d -ed ga in s, a lso a cco rd in g to sim ila r, b u t n o t id en tica l criteria o f th e In stitu te o f Med icin e (IOM, 1990). Ad d ition al p ren atal weigh ts were extracted from clin ic record s.
Mea n BMI a t ea ch week o f gesta tio n a l a ge wa s ca lcu la ted u sin g weigh ts reco rd ed fo r a ll wo m en h a vin g clin ic visits a t th a t gesta tio n a l age. Trim esters were d efin ed as first (less th an 14 co m p lete weeks), seco n d (14-27 co m p lete weeks) an d th ird (28 weeks th rou gh d elivery).
Average w eek ly w eigh t gainfor secon d an d th ird trim esters was estim ated u sin g th e d iffer-en ce b etweiffer-en th e first a n d th e la st weigh ts record ed d u rin g th at trim ester, d ivid ed by th e n u m b er of weeks sep a ra tin g th e two ob serva tion s. Trim ester weekly weigh t gain was calcu -lated p rovid ed th at weigh ts sp aced at least fou r co m p lete weeks a p a rt were a va ila b le. Weekly weigh t gain over th e join t p eriod of th e secon d a n d th ird trim esters wa s estim a ted sim ila rly, p rovided th at an in terval of at least 10 com p lete weeks b etween m easu rem en ts was availab le.
Given th e sm a ll n u m b ers o f reco rd ed weigh ts d u rin g first trim ester, wh ich occu rred p rio r to stu d y en ro llm en t, th e fo llowin g a p -p roach es were u sed to estim ate first trim ester weekly weigh t ga in , u sin g th e p re-p regn a n cy weigh t referred by th e p atien t.
If a first trim ester weigh t wa s a va ila b le, 1st trim ester gain per w eekwas estim ated as:
Weigh t at last record ed 1sttrim ester visit – p rep regn an cy weigh t Gestation al age at last record ed
1sttrim ester weigh t
If n o first trim ester weigh t wa s a va ila b le, then 1sttrim ester gain per w eekwas estim ated as:
(Weigh t at 1strecord in g – p re-p regn an cy weigh t) – [(Gestation al age at 1strecord in g –
14) x 2n dtrim ester weekly gain ] 14
Total w eigh t gain wa s estim a ted a s la st record ed weigh t m in u s p re-p regn an cy weigh t.
As th e last recorded weigh t was frequ en tly m ea-su red a t a p ren a ta l visit, if gesta tio n a l a ge a t last record ed weigh t was less th an gestation al a ge a t d elivery, th en tota l weigh t ga in wa s a d -ju sted to estim ate total gain at deliveryas:
(La st reco rd ed weigh t – p re-p regn a n cy weigh t) + [weekly 3rdtrim ester weigh t ga in x
(gestation al age at d elivery – gestation al age at last weigh t)]
Total w eigh t gain for trim esterwas estim at-ed m u ltip lyin g sp ecific trim ester weekly weigh t gain by th e n u m b er of weeks d u rin g trim ester (14 fo r first a n d seco n d trim esters a n d 12 fo r th e th ird trim ester). Th e th ree trim ester to ta l weigh t ga in s were a d d ed to estim a te th e gain for gestation of 40 w eek s len gth.
An a lyses were p erfo rm ed u sin g SAS so ft-wa re p a cka ge (SAS In stitu te, 1998). An a lyses are d escrip tive in n atu re, in clu d in g freq u en cy d istrib u tio n s, freq u en cy d istrib u tio n cu r ves, p ercen tiles a n d m ea n (± sta n d a rd d evia tio n ), when ever appropriate. Statistical tests for m ean s (ANOVA) a n d p ro p o rtio n s (Qu i-sq u a re) were u sed to com p are grou p s.
Lo ca l in stitu tio n a l eth ic co m m ittees a p -p roved th e stu d y -p rotocol at each cen ter.
Results
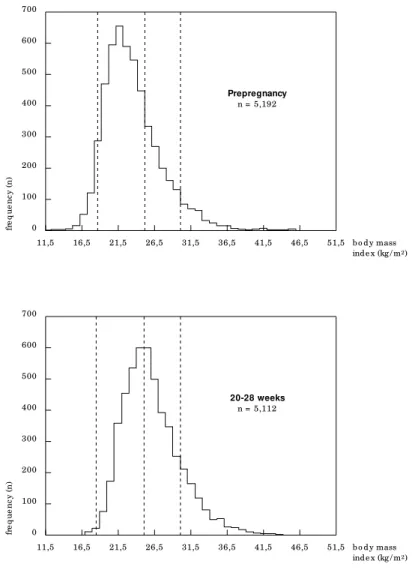
Ta b le 1 p resen ts d escrip tive sta tistics fo r th e 3,082 wom en for wh om total weigh t gain to d e-livery co u ld b e ca lcu la ted a n d fo r th o se 2,110 wh o cou ld n ot. Freq u en cy d istrib u tion s of th e ch aracteristics p resen ted are gen erally sim ilar b etween th e two gro u p s, th e o n ly im p o rta n t d ifferen ce b ein g th e som ewh at u n equ al d egree of follow-u p at th e d ifferen t cen ters. Pre-p reg-n areg-n cy weigh t statu s was q u ite sim ilar b etweereg-n th ese two grou p s of wom en (for exam p le 6.6% of each were ob ese at con cep tion ). Mean esti-m a ted weigh t ga in fro esti-m co n cep tio n th ro u gh en ro llm en t wa s 6.5kg (± 4.9) fo r a ll 5,192 wom en , an d 6.4kg (± 5.0) for th e 3,082 wom en followed th rou gh d elivery.
a re in d ica ted to h igh ligh t th e lim ita tio n s o f th eir u se fo r th e a ssessm en t o f weigh t sta tu s d u rin g p regn an cy.
Figu re 2 sh ows fo r ea ch gesta tio n a l week th e BMI va lu e of p ercen tiles eq u iva len t to th e WHO p re-p regn an cy BMI cu t p oin ts for u n d weigh t (h ere p ercen tile 6.2), p re-ob esity (p er-cen tile 73.1) an d obese (p erer-cen tile 93.6) wom en for th is sam p le. In gen eral, on e sees very m od -est in creases of BMI d u rin g th e first trim -ester, b u t it clea rly in crea ses th erea fter. Alth o u gh grea ter va ria tio n in th e d istrib u tio n o f weigh t in o b ese wo m en crea tes so m e irregu la rity, in gen eral, all cu rves follow a sim ilar p attern .
Th e a vera ge ra te o f weigh t ga in d u rin g p regn a n cy in th e first trim ester wa s 0.18kg/ week (± 0.35). Ob ese a n d p re-o b ese wo m en ten d ed to ga in less weigh t, 0.14kg/ week (± 0.40) an d 0.09kg/ week (± 0.41). Du rin g th e 2n d
a n d 3rdtrim esters, weigh t ga in s were 0.43kg/
week (± 0.27) an d 0.40kg/ week (± 0.30), resp ec-tively, with a sligh t ten d en cy for lower gain s in th e p re-obese an d obese wom en . As th e rates of
weight gain were sim ilar in these two trim esters, th ey can b e exp ressed join tly as an overall rate o f 0.41kg/ week (± 0.19), 0.39kg/ week (± 0.21) for p re-ob ese wom en an d 0.32kg/ week (± 0.22) for ob ese.
Estim a ted weigh t ga in d u rin g th e first t rim e st e r wa s 2.5kg (± 5.0) a s sh own in Ta b le 2. Ob e se a n d ove r we igh t wo m e n h a d le sse r gain s (p < 0.001). Du rin g 2n dan d 3rdtrim esters, weigh t ga in s were 6.0kg (± 3.7) a n d 4.8kg (± 3.6), resp ectively. Th e to ta l ga in over 2n da n d 3rdtrim esters wa s 10.6kg (± 5.1). As exp ected ,
o b ese a n d over weigh t wo m en sh owed lower weigh t gain s (p < 0.001).
To ta l weigh t ga in over a ll trim esters wa s 12.7kg (± 6.2) with lower weigh t ga in s fo r th e over weigh t (11.5kg ± 6.5) a n d o b ese (9.2kg ± 8.4) a n d h igh er ga in s fo r th e u n d er weigh t (14.2kg ± 5.5) wom en (p < 0.001). Com p arison o f weigh t ga in s o b ser ved with th o se reco m -m en d ed b y th e In stitu te o f Med icin e in 1990 sh ows th at for overweigh t wom en (th e In stitu te o f Med icin e ca tego r y ro u gh ly eq u iva len t to
Tab le 1
Charac te ristic s o f ad ult p re g nant wo me n in the c o ho rt stud y, 1991 to 1995.
Characteristics Those followed through delivery Excluded
(n = 3,082) (n = 2,110)
n* % n* %
Study center
Po rto Ale g re 686 22.3 364 17.3
São Paulo 618 20.1 598 28.3
Rio d e Jane iro 404 13.1 132 6.3
Salvad o r 519 16.8 343 16.3
Fo rtale za 719 23.3 372 17.6
Manaus 136 4.4 301 14.3 p < 0.001
Skin color
White 1,416 46.1 927 44.2
Mixe d 1,242 40.4 892 42.5
Blac k 413 13.5 279 13.3 p = 0.311
Pre-pregnancy weight status (WHO )
Und e rwe ig ht (BMI < 18.5kg / m2) 172 5.6 132 6.3
No rmal (18.5kg / m2≤BMI < 25.0kg / m2) 2,020 65.5 1,438 68.2
Pre -o b e sity (25.0kg / m2≤BMI < 30kg / m2) 686 22.3 402 19.1
O b e sity (BMI ≥30.0kg / m2) 204 6.6 138 6.5 p = 0.038
Education
< 8 ye ars 1,328 43.2 916 43.5
8-11 ye ars 1,466 47.7 956 45.4
> 11 ye ars 278 9.1 235 11.2 p = 0.029
p re-ob esity, as d efin ed by th e WHO) th e m ean is at th e u p p er level of th e recom m en d ed ran ge a n d fo r o b ese wo m en th e m ea n ga in is a lso h igh com p ared to th e In stitu te of Med icin e rec-om m en d ation s.
Tab le 3 sh ows th e frequ en cy of wom en wh o gain ed less th an , with in or m ore th an th e ran ge reco m m en d ed b y In stitu te o f Med icin e, a c-cord in g to p re-p regn an cy weigh t categories. An u p p er lim it o f 11.5kg, eq u a l to th a t fo r over-weigh t wom en (Cogswell et al., 1995) was ch o-sen for ob ese wom en for th ese calcu lation s, as th e In stitu te of Med icin e d id n ot d efin e an u p -p er lim it fo r th is cla ss o f wo m en . Overa ll, less th a n o n e-th ird o f wo m en h a d weigh t ga in s with in th e recom m en d ed ran ge. Gain s ou tsid e th is ran ge were esp ecially com m on for wom en wh o were o b ese p re-p regn a n cy. On ly 22% o f th ese wo m en h a d weigh t ga in with in th e d esired ran ge. Excessive weigh t gain was p articu -la rly h igh in th e over weigh t wo m en ; in a d e-qu ate gain in th e lean (p < 0.001).
Rean alysis of the fraction s of wom en ach iev-in g weigh t ga iev-in go a ls, u siev-in g WH O BMI cu t p oin ts in stead of th ose of th e In stitu te of Med i-cin e to d efin e b aselin e n u trition al statu s cate-go ries, resu lted in sim ila r p ercen ta ges (d a ta n ot sh own ).
Discussion
We fo u n d h igh p re-p regn a n cy freq u en cies o f p reob esity an d ob esity (28% togeth er) in com -p arison with u n d erweigh t (6%) am on g Brazil-ia n wo m en receivin g p re-n a ta l ca re th ro u gh th e n ation al h ealth system in m ajor cities. Th e n a tio n a l h ea lth system p rovid es ca re fo r th e ap p roxim ately 75% of Brazilian s, with ou t em -p loym en t rela ted o r -p riva te m ed ica l covera ge (Faquim , 1999). This sam p le of Brazilian wom en p resen ts a p ictu re b ein g in creasin gly rep orted fo r wo m en a ro u n d th e wo rld , th a t o f h igh p revalen ce of p re-ob esity an d ob esity (Ben icio et al., 1995; Mon teiro et al., 2000; Sich ieri et al., 1994), in an era in wh ich ob esity is in creasin gly a m ajor factor for fu tu re h ealth risks in wom en . Fu rth er, we fo u n d th a t reco m m en d ed weigh t gain du rin g p regn an cy is in frequ en tly ach ieved, esp ecia lly in o b ese a n d over weigh t wo m en , categories in wh ich we estim ate th at less th an 30% ach ieved recom m en d ed gain s.
Given th e im p o rta n ce o f o b esity, a n d th e freq u en t clin ica l u n certa in ty a b o u t rep o rted p re-p regn an cy weigh t, it is con ven ien t to try to estim ate b aselin e ob esity statu s from weigh t at th e in itia l p ren a ta l visit. Figu re 2 p erm its th is estim a tio n o f WH O n u tritio n a l cla ssifica tio n
category in p regn an t wom en at d ifferen t gesta-tio n a l a ges. Th is ch a rt th u s m a y b e o f u se fo r estim atin g b aselin e n u trition al class, an d th u s recom m en d ed weigh t gain , for wom en with ou t reliab le p re-p regn an cy weigh t. For exam p le, a wom en with BMI of 26.0kg/ m2at 20 weeks ges-tation , th ou gh p re-ob ese by stan d ard criteria, p resen ts weigh t with in th e n o rm a l ra n ge, a s evalu ated u sin g Figu re 2.
Few o th er stu d ies h a ve d o cu m en ted th e cu rren t d istrib u tion of p re-p regn an cy weigh ts a n d weigh t ga in d u rin g p regn a n cy. Of n o te is o n e stu d yin g wo m en a tten d in g p u b lic clin ics in Lo s An geles, Ca lifo rn ia fro m 1983 to 1986
Fig ure 1
Distrib utio n o f b o d y mass ind e x (kg / m2) b e fo re and d uring p re g nanc y (at stud y
e nro llme nt) in wo me n ag e d 20 to 48. Wo rld He alth O rg anizatio n stand ard c ut p o ints
fo r o utsid e o f p re g nanc y are ind ic ate d fo r und e rwe ig ht, p re -o b e sity and o b e sity.
0 100 200 300 400 500 600 700
46,5 51,5 b o d y mass ind e x (kg / m2) 41,5
36,5 31,5 26,5 21,5 16,5 11,5
fr
e
q
u
e
n
c
y
(
n
)
Prepregnancy n = 5,192
0 100 200 300 400 500 600 700
46,5 51,5 b o d y mass ind e x (kg / m2)
41,5 36,5 31,5 26,5 21,5 16,5 11,5
fr
e
q
u
e
n
c
y
(
n
)
(Siega-Riz et al., 1994). In th is p op u lation , n ear-ly 17.4% o f wo m en were overweigh t, a p p roxi-m a tely 10.5% o f th ese o b ese, a n d weigh t ga in goa ls were a lso in freq u en tly a ch ieved (52% of th e overweigh t wom en ). An oth er, m ore recen t, U.S. stu d y in low-in com e wom en sh owed even less a ch ievem en t o f weigh t ga in go a ls: 68% o f overweigh t an d 52% of ob ese wom en gain ed in excess o f th e reco m m en d a tio n s (Co sgwell et al., 1995).
Th e fu tu re h ealth risks associated with th e extrem es of n u trition al statu s d u rin g p regn an -cy a n d a t b irth a re b ein g in crea sin gly reco g-n ized . Low b irth weigh t, associated with b eig-n g u n d erweigh t p rior to p regn an cy an d h avin g in a d eq u a te weigh t ga in d u rin g p regn a n cy, in -crea ses fu tu re risk o f d ia b etes, h yp erten sio n , an d card iovascu lar d isease (Barker et al., 1993; Hales et al., 1991; Ph illip s, 1998). On th e oth er h a n d , o b esity d u rin g p regn a n cy (Cn a ttin giu s et al., 1998; Faú n d es et al., 1988) an d excessive weigh t gain (IOM, 1990) are associated with an in crease in m orb id ity b oth for th e m oth er an d th e fetu s (NIH/ NHLBI, 1998), in clu d in g m ater-n al weigh t reteater-n tioater-n (Sch oll et al., 1995). Ad d
i-tio n a lly, excess b irth weigh t a p p ea rs to b e a s-sociated with excess weigh t later in life (Ch ar-n ey et al., 1976). Th e im p act of ob esity aar-n d ex-cessive weigh t gain d u rin g p regn an cy on ad u lt d iseases is d ifficu lt to stu d y, as ob esity as cu r-re n t ly p r-re se n t in wo m e n o f ch ild b e a rin g a ge wa s a re la t ive ly in fre q u e n t fin d in g u n t il re -cen tly.
Lim ita tio n s to o u r stu d y sh o u ld b e n o ted . Th e lack of active follow-u p an d th e accom p a-n yia-n g ia-n a b ility to p erfo rm ch a rt review o a-n a la rge fra ctio n o f th e wo m en in itia lly en ro lled m a ke o u r estim a tes less rep resen ta tive o f th e in itial cohort. Due to the characteristics of stu d y sam p le selection , ou r stu d y sam p le can n ot b e con sid ered d irectly rep resen tative of Brazilian p regn a n t wo m en . However, co m p a riso n s o f d a ta o n ed u ca tio n a l level, n u tritio n a l sta tu s a n d gesta tio n a l a ge a t d eliver y (IBGE, 1996) su ggest th a t ch a ra cteristics o f o u r sa m p le a re com p arab le with th ose of p regn an t wom en , at lea st in th e la rge m etrop olita n a rea s of Bra zil. An a d d itio n a l lim ita tio n is th a t 1sttrim ester weigh t ga in , a s it o ccu rred p rio r to th e stu d y en ro llm en t, relies o n referred p re-p regn a n cy
Fig ure 2
Bo d y mass ind e x (BMI) ac c o rd ing to g e statio nal ag e fo r p re g nant wo me n at p e rc e ntile s e q uivale nt to tho se o f Wo rld
He alth O rg anizatio n p re p re g nanc y BMI c ut p o ints fo r und e rwe ig ht (18.5kg / m2), p re -o b e se (25kg / m2) and o b e sity
(30kg / m2), and the 50thp e rc e ntile .
B
M
I
(k
g
/m
2)
16 18 20 22 24 26 28 30 32 34 36 38 40
Pe rce ntile 93.6 (~ o b e sity)
Pe rce ntile 73.1 (~ p re -o b e se )
Pe rce ntile 50.0 (~ me d ian)
Pe rce ntile 6.2 (~ und e rwe ig ht)
40 42 g e statio nal ag e (we e ks) 38
36 34 32 30 28 26 24 22 20 18 16 14 12 10 8 6 4 2 0
Body mass index (kg/ m2) Gestational age (weeks)
14 20 24 28 32
O b e se 31.1 31.6 33.0 33.4 34.5
Pre -o b e se 26.1 27.1 28.4 28.8 29.8
weigh t, wh ich is su b ject to recall b ias. However, o n th e b a sis o f o u r p revio u s fin d in gs co n -cern in g weigh t reca ll fo r Bra zilia n wo m en stu d ied o u tsid e o f p regn a n cy (Sch m id t et a l., 1993), we b elieve th at th is m easu rem en t b ias is p rob ab ly sm all.
In co n clu sio n , in a p o p u la tio n gen era lly rep resen ta tive o f wo m en a tten d in g Bra zilia n p u b lic h ealth clin ics in m ajor cities, th e p reva-len ce of p re-ob esity an d ob esity p rior to p reg-n areg-n cy was h igh , areg-n d ap p roxim ately two-th ird s of th e wom en d id n ot a ch ieve th e weigh t ga in reco m m en d ed b y th e In stitu te o f Med icin e. Given th e in crea sin g ep id em ic of ob esity, a n d
th e in creasin g evid en ce th at b oth low an d h igh b irth weigh ts in crease risk for ch ron ic d isease, m o re a tten tio n sh o u ld b e given , to th e q u es-tion of ach ievin g ad eq u ate weigh t gain d u rin g p regn a n cy a s well a s to th e d evelo p m en t, im -p lem en tation , an d evaluation of effective strate-gies of weigh t m an agem en t in p regn an cy.
Tab le 2
Me an (± stand ard d e viatio n) e stimate d to tal we ig ht g ain (kg ) ac c o rd ing to p re -p re g nanc y Institute o f Me d ic ine
we ig ht status* amo ng wo me n ag e d 20 to 48, 1991 to 1995.
Trimesters Pre-pregnancy weight status
Und e rwe ig ht No rmal O ve rwe ig ht O b e sity To tal p
First (n = 3,354) 3.8 (± 4.8) 2.4 (± 4.7) 1.9 (± 5.6) 1.2 (± 5.8) 2.5 (± 5.0) < 0.001
Se c o nd (n = 3,247) 6.1 (± 3.7) 6.3 (± 3.5) 5.8 (± 4.3) 4.2 (± 4.1) 6.0 (± 3.7) < 0.001
Third (n = 3,063) 4.8 (± 3.8) 4.9 (± 3.4) 4.7 (± 4.1) 4.4 (± 4.0) 4.8 (± 3.6) 0.1455
Se c o nd and third (n = 3,826) 10.7 (± 4.7) 11.0 (± 4.9) 10.0 (± 5.6) 8.3 (± 5.7) 10.6 (± 5.1) < 0.001
O ve rall (n = 3,082) 14.2 (± 5.5) 13.0 (± 5.7) 11.5 (± 6.5) 9.2 (± 8.4) 12.7 (± 6.2) < 0.001
Re c o mme nd e d b y IO M 12.5–18.0 11.5–16.0 7.0–11.5 > 6.8
* BMI c ut p o ints ac c o rd ing to Institute o f Me d ic ine : und e rwe ig ht < 19.8kg / m2; o ve rwe ig ht > 26.0kg / m2
and < 29kg / m2; and o b e se > 29.0 kg / m2. Se e te xt fo r fo rmula d e finitio ns.
Tab le 3
Fre q ue nc y o f e stimate d we ig ht g ain le ss than, within, o r mo re than the rang e re c o mme nd e d b y the Institute
o f Me d ic ine * ac c o rd ing to p re -p re g nanc y we ig ht status†.
Pre-pregnancy weight status Weight gain
Le ss than W ithin re c o mme nd atio ns (% ) Mo re than re c o mme nd e d (% ) re c o mme nd e d (% ) De live ry‡ 40 we e ks§ De live ry‡ 40 we e ks§ De live ry‡ 40 we e ks§
Und e rwe ig ht (n = 479) 40.3 37.3 38.8 39.4 20.9 23.3
No rmal (n = 1,943) 39.7 37.4 34.2 33.1 26.1 29.5
O ve rwe ig ht (n = 382) 23.3 22.2 27.2 25.1 49.5 52.7
O b e se (n = 278) 40.3 38.1 21.9 22.8 37.8 39.2
All wo me n (n = 3,082) 37.8 35.6 32.9 32.1 29.2 32.3
* To tal we ig ht g ain re c o mme nd e d b y Institute o f Me d ic ine : 12.5–18.0kg fo r und e rwe ig ht, 11.5–16.0kg fo r no rmal we ig ht, 7.0–11.5 fo r o ve rwe ig ht and > 6.8 fo r o b e se wo me n.
†BMI c ut p o ints ac c o rd ing to Institute o f Me d ic ine : und e rwe ig ht < 19.8kg / m2; o ve rwe ig ht > 26.0kg / m2
and < 29kg / m2; and o b e se > 29.0kg / m2.
‡Calc ulate d up to d e live ry.
§Extrap o late d fro m d e live ry to c o mp le te 40 we e ks.
References
AL-ISA, A., 1998. Bod y m ass in d ex an d p revalen ce of
ob esity ch an ges am on g Ku waitis. Eu ropean Jou
r-n al of Clir-n ical Nu tritior-n, 51:743-749.
ALLISON, D. B.; EDLEN-NEZIN, L. & CLAY-WILLIAMS, G., 1997. Obesity am on g African Am erican wom en : Prevalen ce, con seq u en ces, cau ses, an d d evelop
-in g research . W om en ’s Health : Research on Gen
-der, Beh avior, an d Policy, 3:243-274.
BARKER, D.; H ALES, C.; FALL, C.; OSMOND, C.; PHIPPS, K. & CLARK, P., 1993. Typ e 2 (n on -in su lin d ep en d en t) d iab etes m ellitu s, h yp erten sion an d h yp erlip id em ia (syn d ro m e X): Rela tio n to
re-d u cere-d fetal growth . Diabetologia, 36:62-67.
BENICIO, D. A.; MONTEIRO, C. A.; CONDE, W. & POPKIN, B. M., 2000. Sh iftin g o b esity tren d s in
Bra zil. Eu rop ean Jou rn al of Clin ical N u trition,
54:342-346.
CAPURRO, H .; KONICH EZKY, S.; FONSECA, D. & CALDEIRO-BARCIA, R., 1978. A sim p lified m eth od fo r d ia gn o sis o f gesta tio n a l a ge in n ewb o rn in
-fan t. Jou rn al of Pediatrics, 93:120-122.
CHARNEY, E.; CHAMBLEE, H.; McBRIDE, M.; LYON, B. & PRATT, R., 1976. Ch ild h o o d a n teced en ts o f a d u lt o b esity. Do ch u b b y in fa n ts b eco m e o b ese
adu lts? New En glan d Jou rn al of Medicin e, 295:6-9.
CNATTINGIUS, S.; BERGSTROM, R.; LIPWORTH, L. & KRAMER, M. S., 1998. Prep regn a n cy weigh t a n d
th e risk o f a d verse p regn a n cy o u tco m es. N ew
En glan d Jou rn al of Medicin e, 338:147-152. COGSWELL, M. E.; SERDULA, M. K.; HUNGERFORD,
D.W. & YIP, R., 1995. Gesta tio n a l weigh t ga in am on g average-weigh t an d overweigh t wom en –
Wh at is excessive? Am erican Jou rn al of Obstetrics
an d Gyn ecology, 172:705-712.
FAQUIM, L., 1999. Plan os d e saú d e. Os d ois lad os d a
regu la m en ta çã o. Recu rsos Hu m an os em Sín tese,
27. Ma rço / Ab ril 1999. 12 Ago sto 2000 <h ttp :/ / www.gestaoerh .com .b r/ artigos/ legi_010.sh tm l>. FAÚNDES, A.; PASSINI, R. J.; SILVA, J. L. P.; DIAZ, A. J.;
SILVA, J. C. G. S. & PINOTTI, J. A., 1988. Stu d y of altern ative m ean s of m atern al weigh t evalu ation
as p red ictors of b irth weigh t. Revista Brasileira de
Gin ecologia e Obstetrícia, 10:199-204.
FLEGAL, K. M.; CARROLL, M. D.; KUCZMARSKI, R. J. & JOHNSON, C. L., 1998. Overweigh t an d ob esity in th e Un ited States: Prevalen ce an d tren d s,
1960-1994. In tern ation al Jou rn al of Obesity an d
Relat-ed Metabolic Disorders, 22:39-47.
FOREYT, J. P. & POSTON II, W. S., 1998.Ob esity: A n
ev-er-en d in g cycle? In tern ation al Jou rn al of Fertility
an d W om en ’s Medicin e, 43:111-116.
GROL, M. E.; EIMERS, J. M.; ALBERTS, J. F.; BOUTER, L. M.; GERSTENBLUTH, I.; HALABI, Y.; VAN SON-DEREN, E. & VAN DEN H EUVEL, W. J., 1997. Ala rm in gly h igh p reva len ce o f o b esity in Cu ra -cao: Data from an in terview su rvey stratified for
so cio eco n o m ic sta tu s. In tern ation al Jou rn al of
Obesity an d Related Metabolic Disorders, 21:1002-1009.
HALES, C.; BARKER, D. & CLARK, P., 1991. Feta l a n d in fan t growth an d im p aired glu cose toleran ce at
age 64. BMJ, 303:1019-1022.
IBGE (Fu n d a çã o In stitu to Bra sileiro d e Geo gra fia e
Estatística), 1996. DATASUS. 5 Au gu st 2000 <h ttp :
/ / www.d atasu s.gov.b r/ tab n et/ tab n et.h tm >.
IOM (In stitu te of Med icin e), 1990. N u trition Du rin g
Pregn an cy. Wa sh in gto n , DC: Su b co m m ittee o n Nu trition al Statu s an d Weigh t Gain Du rin g Pregn aPregn cy/ Su b com m ittee oPregn Dietary IPregn take aPregn d Nu -trien t Su p p lem en ts Du rin g Pregn an cy/ Com m it-tee o n Nu tritio n a l Sta tu s Du rin g Pregn a n cy a n d La cta tio n / Fo o d a n d Nu tritio n Bo a rd / Na tio n a l Acad em y of Scien ce.
MONTEIRO, C. A.; MONDINI, L.; MEDEIROS-DE-SOUZA, A. L. & POPKIN, B. M., 1995. Th e n u
tri-tio n a l tra n sitri-tio n in Bra zil. Eu rop ean Jou rn al of
Clin ical Nu trition, 49:105-113.
NIH (Nation al In stitu tes of Health )/ NHLBI (Nation al
Heart, Lu n g, an d Blood In stitu te), 1998. Clin ical
Gu id elin es on Id en tification , Evalu ation , an d Treatm en t of Overw eigh t an d Obesity in Ad u lts – Th e Evid en ce Rep ort. 2 Octo b er 1998 <h ttp :/ / www.n h lb i.n ih .gov/ gu id elin es/ ob esity/ ob _gd ln s. h tm >.
PHILLIPS, D., 1998. Birth weigh t an d th e fu tu re d
evel-op m en t of d iab etes: A review of th e evid en ce.
Di-abetes Care, 21/ 22:B150-B155.
ROSSO, P., 1985. A n ew ch art to m on itor weigh t gain
d u rin g p regn a n cy. Am erican Jou rn al of Clin ical
Nu trition, 41:644-652.
ROZOWSKI, J. & ARTEAGA, A., 1997. Th e p rob lem of ob esity an d its sh ockin g ch aracteristics in Ch ile. Revista Medica de Ch ile, 125:1217-1224.
SAS INSTITUTE, 1998. SAS/STAT U ser’s Gu id e,
Ver-sion 6, Fou rth Ed ition , Volu m e 1-2.Cary: SAS In -stitu te In c.
SCHMIDT, M.; DUNCAN, B. & TAVARES, M., 1993. Va-lid ity o f self-rep o rted weigh t – A stu d y o f u rb a n
Bra zilia n a d u lts. Revista d e Saú d e Pú blica, 27:
271-276.
SCH OLL, T. O.; H EDIGER, M. L.; SCH ALL, J. I.; AN-CES, I. G. & SMITH , W. K., 1995. Gesta tio n a l weigh t ga in , p regn a n cy o u tco m e, a n d p o stp a
r-tu m weigh t reten tio n . Obstetrics & Gyn ecology,
86:423-427.
SICHIERI, R.; COITINHO, D. C.; LEÃO, M. M.; RECINE, E. & EVERHART, J. E., 1994. High tem p ora l, geograp h ic, an d in com e variation s in b od y m ass in
-d ex a m o n g a -d u lts in Bra zil. Am erica Jou rn al of
Pu blic Health, 84:793-798.
SIEGA-RIZ, A. M.; ADAIR, L. S. & HOBEL, C. J., 1994. In stitu te o f Med icin e m a tern a l weigh t ga in rec-om m en d ation s an d p regn an cy ou tcrec-om e in a p
re-d o m in a n tly Hisp a n ic p o p u la tio n . Obstetrics &
Gyn ecology, 84:565-573.
WH O ( Wo rld Hea lth Orga n iza tio n ), 1998. Obesity –