Health care utilization and survival among
patients with AIDS in Belo Horizonte,
M inas Gerais, Brazil
Utilização d e cuid ad o s d e saúd e e so b re vid a
e ntre p acie nte s co m AIDS e m Be lo Ho rizo nte ,
Minas Ge rais, Brasil
1 Dep artam en to d e Farm ácia Socia l e Cu rso d e Dou t ora d o em Ciên cia An im a l, Un iv ersid a d e Fed era l d e M in a s Gera is. Av. Olegá rio M a ciel 2360, Belo Horiz on t e, M G 30180- 112, Bra sil. 2 Dep artam en to d e Est a t íst ica , Un iv ersid a d e Fed era l d e M in a s Gera is. Av. An t on io Ca rlos 6627, Belo Horiz on t e, M G 31270- 901, Bra sil. 3 Dep artam en to d e Med icin a Prev en t iv a e Socia l, Un iv ersid a d e Fed era l d e M in a s Gera is. Av. Alfred o Ba len a 190, 10oa n d a r, Belo Horiz on t e, M G, 30130- 100, Bra sil.
Fra n cisco d e Assis Acu rcio 1 Cib ele Com in i Cesa r 2
M a rk Drew Crosla n d Gu im a rã es 3
Abst ract A h ist orica l coh ort st u d y w a s con d u ct ed in t h ree p u b lic AIDS referra l serv ices in Belo Horiz on t e, M in a s Gera is, t o a ssess t h e rela t ion sh ip b et w een h ea lt h ca re u t iliz a t ion a n d p a t ien t su rv ival follow in g AIDS d iagn osis. A rev iew of m ed ical an d laborat ory record s w as p erform ed for HIVin fect ed p at ien t s seek in g care for t h e first t im e in 198992. Am on g 291 p at ien t s in it ially cat -egoriz ed a s “A” [a sym p t om a t ic, a cu t e H IV, or p ersist en t gen era liz ed lym p h a d en op a t h y- PGL] or “B” [sym p t om a t ic, n on - ”A”, or AIDS- in d ica t or con d it ion s] (CDC, 1992) a n d w h o p rogressed t o AIDS, 57.0% d ied . M ort a lit y ra t e w a s 34.9/1.000 p erson - m on t h s. Ov era ll m ed ia n su rv iv a l t im e follow in g AIDS d ia gn osis w a s 14.3 m on t h s. M u lt iv a ria t e a n a lysis sh ow ed t h a t la ck of AZ T u se (RR = 1.87; 95% CI = 1.34- 2.61), a d v a n ced in it ia l st a gin g (RR = 1.68; 95% CI = 1.20- 2.35), 9 or m o re i n p a t i en t d a ys (RR = 1.55; 95% CI = 1.11- 2.17), a n d i n t erv a ls b et w een o u t p a t i en t v i si t s lon ger t h a n 6 m on t h s (RR = 0.30; 95% CI = 0.16- 0.56) w ere a ssocia t ed w it h d ea t h . T h e a n a lysis su ggest s t h a t : Pa t ien t s w h o u sed h ea lt h serv ices m ore oft en h a d p oorer p rogn osis; Pa t ien t s w h o receiv ed AZ T su rv iv ed lon ger t h a n t h ose w h o d id n ot ; a n d Va ria b les u sed t o a ssess h ea lt h ca re u t iliz at ion act u ally ex p ress t h e en d of a p rocess in v olv in g seek in g an d obt ain in g care.
Key words AIDS; Su rv ival; Healt h Care; HIV
Resumo Para an alisar a relação en t re u t iliz ação d e cu id ad os d e saú d e e sobrev id a d e p acien t es com AIDS foram rev isad os regist ros m éd icos d e p acien t es sorop osit iv os ad m it id os n os serv iços d e referên cia p a ra AIDS em Belo Horiz on t e/M G, en t re 1989- 92. D os 291 p a cien t es q u e ev olu íra m p ara AIDS, 57,0% faleceram . O coeficien t e d e m ort alid ad e foi d e 34,9/1.000 p essoas-m ês. A m ed i-a n i-a d o t em p o d e sobrev id i-a globi-a l foi d e 14,3 m eses. A i-a n á lise m u lt iv i-a rii-a d i-a m ost rou qu e in d iv í-d u os qu e n ão u t iliz aram AZ T (RR = 1,87; IC 95% = 1,34-2,61), qu e foram classificaí-d os com o est a-d iam en t o in icial “B”[sin t om át icos, n ão AIDS] (RR = 1,68; IC 95% = 1,20-2,35) e qu e t iv eram n ov e ou m a is d ia s d e in t ern a çã o h op it a la r (RR = 1,55; IC 95% = 1,11- 2,17) a p resen t a ra m m a ior risco d e ev olu írem p a ra ób it o. Já in d iv íd u os q u e regist ra ra m p elo m en os u m in t erv a lo m a ior d e seis m eses en t re con su lt a s (RR = 0,30; IC 95% = 0,16- 0,56) a p resen t a ra m m en or risco d e ev olu irem p a ra ób it o. Os resu lt a d os su gerem : In d iv íd u os com p iores resu lt a d os n a sa ú d e t en d em a u t iliz a r m a is os serv iços e os m a is com p lex os; Pessoa s q u e u t iliz a ra m AZ T sob rev iv era m m a is t em p o; Os m a rca d ores d e u t i li z a çã o a d ot a d os ex p ressa m o fi n a l d e u m p rocesso d e b u sca e ob t en çã o d a at en ção.
Introduction
In Brazil, th e first case of Acq u ired Im m u n od eficie n cy Syn d ro m e (AIDS), ca u se d b y th e Hu -m an I-m -m u n od eficien cy Viru s (HIV), was d iag-n osed iiag-n 1980, aiag-n d u iag-n til 1987 th e ep id em ic was re stricte d to th e m a in u rb a n ce n te rs o f th e So u th ea stern , So u th ern , a n d Cen tra l-Western re gio n s. Sin ce th e n , th e e p id e m ic h a s sp re a d co n tin u o u sly th ro u gh o u t th e co u n try. Assess-m e n ts o f th e e p id e Assess-m ic’s p ro gre ssio n p o in t to a n in cre a sin g in cid e n ce o f AIDS a m o n g p a -tie n ts fro m th e lowe st so cio e co n o m ic gro u p s (Fio cru z, 1996). As of Ma y 1997, 110,872 ca ses h a d b e e n re p o rte d to th e Min istr y o f He a lth (Brazil) with a cu m u lative in cid en ce of 79.5 p er 100,000 p op u lation an d 54,813 (49.4%) d eath s (MS, 1997), m akin g th e ep id em ic on e of Brazil’s m a in p u b lic h e a lth p ro b le m s. Th e im p a ct o n th e h ealth care system h as d em an d ed in creas-in g e ffo r ts b y th e gove rn m e n t to p re ve n t a n d con trol th e d isease. However, p reven tive m ea-su res are still d eficien t in term s of b oth coverage an d effectiven ess. Desp ite recen t d evelop m en ts in AIDSrelated kn owled ge an d d evelop m en t of n ew d ru gs an d treatm en t, p rop er m an -agem en t of th e d isease is a m ajor ch allen ge for cou n tries with u n equ al d istrib u tion of p rop h y-la ctic a n d th era p eu tic reso u rces. It is th u s es-sen tial to b road en ou r kn owled ge of social an d h u m a n co sts o f H IV in fe ctio n , n e e d s a n d re -q u ire m e n ts o f in fe cte d p a tie n ts, a n d b a rr ie rs towa rd s h e a lth ca re a n d co n se q u e n ce s o f d e-layed care. Stu d ies on u se of h ealth care (on e of th e m a in co m p o n e n ts in e va lu a tin g a cce ss to th e h ealth care system by HIV-p ositive in d ivid-u a ls) a re ra re in Bra zil. Little in fo rm a tio n is availab le on eith er p attern s in th e u tilization of h ea lth ca re by su ch in d ivid u a ls o r fa cto rs th a t m ay in terfere with it. Neith er is it clear to wh at exten t su ch b arriers in terfere with p atien t su r-vival followin g AIDS d iagn osis.
Th e p re se n t stu d y e va lu a te s th e re la tio n -sh ip b e twe e n so cio d e m o gra p h ic/ b e h a vio ra l factors, an d , esp ecially, variab les related to u ti-lization of h ealth care an d p rogression to d eath a m on g AIDS p a tien ts u sin g p u b lic AIDS refer-ral services.
M aterials and methods
Population
A h isto rica l co h o rt stu d y wa s co n d u cted in th ree p u b lic AIDS referral services in Belo Hori-zo n te, Bra zil: 1) a n ou tp a tien t clin ic for AIDS/ Sexu ally Tran sm itted Diseases (STDs), th e
Ores-tes Din iz Train in g an d Referen ce Cen ter (CTR) from th e Belo Horizon te Mu n icip al Health De-p a rtm en t a n d th e Fed era l Un iversity o f Min a s Ge ra is (U FMG); 2) th e Ed u a rd o d e Me n e ze s Hosp ital (HEM) of th e Min as Gerais State Hos-p ital Fou n d ation ; an d 3) th e Un iversity HosHos-p i-tal (HCL) u n d er th e UFMG.
Th e stu d y p o p u la tio n co n sisted o f a ll co n -firm e d H IV-p o sitive p a tie n ts a d m itte d to th e CTR fo r th e first tim e fro m Ja n u a r y 1, 1989, th ro u gh De ce m b e r 31, 1992. Pa tie n ts ca te go -rized accord in g to clin ical categories p rop osed by th e Cen ters for Disease Con trol (CDC, 1992) a s “A” (a sym p tom a tic, a cu te HIV, or p ersisten t gen era lized lym p h a d en o p a th y) o r “B” (sym p -tom atic, n ot “A” or AIDS-in d icator con d ition s) at th is first ou tp atien t visit an d wh o p rogressed to AIDS (Category “C”, CDC) th ereafter were as-se sas-se d fo r su r viva l sta tu s u n til De ce m b e r 31, 1994. On ly p a tien ts a d m itted to th e CTR were fo llowe d to ch e ck fo r h o sp ita liza tio n a t H EM an d HCL.
Su rvival tim e was d efin ed as th e p eriod b e-tween th e d a te o f AIDS d ia gn o sis reco rd ed o n m e d ica l file s a n d d a te o f d e a th a s re p o rte d to th e Min a s Ge ra is Sta te He a lth Au th o rity o r record ed in th e m ed ical files. Search for rep ort-ed d eath on ly occu rrort-ed seven m on th s after th e en d of th e follow-u p p eriod . Th is allowed su ffi-cie n t tim e fo r d e te ctin g la te re p o rtin g. It wa s th u s p ossib le to red u ce th e likelih ood of u n d er-record in g of d eath s d u rin g th e stu d y p eriod .
A stan d ard ized form was u sed to collect d a-ta fro m clin ica l a n d la b o ra to r y re co rd s fro m e a ch se r vice. So cio d e m o gra p h ic a n d b e h a v-io ra l va ria b les in clu d ed a ge, sex, ra ce, m a rita l statu s, city of resid en ce, ed u cation , in d ivid u al m on th ly in com e, socia l secu rity covera ge, h e-m o p h ilia , b lo o d tra n sfu sio n o r h e e-m o d ia lysis, sexu al in tercou rse with HIV-p ositive p erson (s), sexu al in tercou rse with m en , sexu al in tercou rse with wo m e n , n u m b e r o f life tim e se xu a l p a r tn ers, p ro stitu tio tn , co tn d o m u se, u se o f a tn y itn -je cte d d ru g [licit o r illicit], a n d sh a re d n e e d le u se. All sociod em ograp h ic d ata were b ased on in form ation collected at th e first visit with th e h ealth care facilities. Con tin u ou s variab les were ca te go rize d a n d th e m e d ia n wa s co n sid e re d th e cu t-off p oin t.
n u m b er of in tervals lon ger th an six m on th s b e-tween two o u tp a tien t visits, AZT u se, n u m b er of in p atien t d ays followin g AIDS d iagn osis, an d calen d ar year of first ou tp atien t visit.
Statistical analysis
Un ivariate an alysis was con d u cted to exam in e th e association b etween each variab le an d p ro-gre ssio n t o d e a t h . Th e Ka p la n -Me ie r m e t h o d (Ka h n & Se m p o s, 1989) wa s u se d t o e st im a t e th e cu m u la tive p ro b a b ility o f p a tien t su r viva l tim e. Co m p a riso n o f d iffe re n t cu r ve s a cco rd -in g to su b grou p s was con d u cted u s-in g th e log-ra n k test. Sign ifica n ce level a d o p ted wa s 0.05. Relative h azard s of d eath after AIDS, with 95% con fid en ce in terval, was assessed th rou gh Cox Pro p o rtio n a l Ha za rd s m o d e l (Cox & Oa ke s, 1984) for b oth u n ivariate an d m u ltivariate esti-m ates.
Th e in d e p e n d e n t e ffe ct o f se le cte d va ri-a b les o n p ro gressio n to d eri-a th wri-a s ri-a ssessed in th e m u ltivariate an alysis. Variab les statistically a sso cia ted (p <0.10) with p ro gressio n to d ea th in th e u n ivariate an alysis as well as th ose con sid e re d clin ica lly a n d e p id e m io lo gica lly re le -van t were fitted . Mod elin g b egan with all varia b les fo llowed b y seq u en tivaria l d eletio n varia cco rd -in g to th e ir sta tistica l im p o r ta n ce. Ea ch va ri-ab le was assessed an d m od els were com p ared u sin g th e likelih ood ratio test (SERC, 1993).
Results
Descriptive statistics
Th e stu d y in clu d ed 291 H IV-p o sitive su b jects registered at th e CTR b etween Jan u ary 1, 1989, a n d De ce m b e r 31, 1992, wh o p ro gre sse d to AIDS b y De ce m b e r 31, 1994. Mo st p a tie n ts we re re fe rre d to th e CTR fo r th e first tim e b y p h ysician s (63.6%) an d reason s in clu d ed : con -firm ation of HIV d iagn osis (42.3%), follow-u p / tre a tm e n t o f AIDS (23.7%), in itia l H IV te stin g (22.3%), an d u n kn own (11.7%). Du rin g th e followu p p e rio d , 228 (78.3%) p a tie n ts we re re -fe rre d fo r a d m issio n to th e two h o sp ita ls a n d 220 (75.6%) we re a ctu a lly a d m itte d a t le a st on ce. HEM wa s th e first h osp ita l of a d m ission fo r 141 (64.1%) a n d H CL fo r 37 (16.8%) p a -tien ts. Sociod em ograp h ic an d b eh avioral ch ar-a cte ristics/ so u rce o f in fe ctio n o f th e p ar-a tie n ts a re sh own in Ta b le 1. Mo st p a tien ts were a ged 30 o r over, sin gle, m a le, wh ite, h a d 8+ yea rs o f sch o o lin g, re sid e d in Be lo Ho rizo n te, h a d in -co m e s u n d e r th re e tim e s th e m in im u m wa ge [i.e., le ss th a n a p p roxim a te ly U$325/ m o n th –
Tran slator’s n ote], an d h ad social secu rity cove ra gcove. On ly 15.1% rcove p o rtcove d a t lcove a st 50% co n -d om u se -d u rin g sexu al in tercou rse, 79.4% h a-d a h istory of STDs, 60.8% h ad u sed licit or illicit in jecta b le d ru gs, 32.6% rep o rted sexu a l in ter-cou rse with HIV-p ositive p erson (s), an d 24.8% h ad 100+ lifetim e sexu al p artn ers.
Resu lts of variab les in d icatin g u tilization of h e a lth ca re sh owe d th a t: 1) m e a n n u m b e r o f ou tp atien t visits p er year followin g d iagn osis of AIDS was 26.9 (m ed ian = 17.1); 2) AZT u se was reco rd ed in 149 (51.4%) o f th e p a tien t files; 3) m ean n u m b er of in p atien t d ays followin g AIDS d iagn osis was 20.1 (m ed ian = 8.0); 4) m ean in -terval b etween first an d secon d ou tp atien t visit was 50.1 d ays (m ed ian = 20.0); 5) m ean in ter val b etween b lood sam p le an d com m u n icatin g th e first ELISA resu lt was 50.4 d ays (m ed ian = 23.0); 6) m e a n in te r va l b e twe e n a n H IV te st re su lt p rio r to a d m issio n to th e h e a lth ca re fa cility an d first ou tp atien t visit was 150.6 d ays (m ed i-a n = 47.0); i-a n d h ) m ei-a n in ter vi-a l b etween first
Tab le 1
So cio d e mo g rap hic and b e havio ral characte ristics/ so urce o f infe ctio n amo ng p atie nts ad mitte d to O re ste s Diniz Training and Re fe re nce Ce nte r who d e ve lo p e d AIDS, Be lo Ho rizo nte , Brazil, 1989-1994.
Characteristic n* %
Sociodemographic
Ag e (≥30 ye ars) 178 61.2
Sing le 213 73.4
Male 245 84.2
White 167 59.2
Scho o ling (8+ ye ars) 167 58.8
Re sid e nt in Be lo -Ho rizo nte 192 66.0
Mo nthly inco me (< 3 minimum wag e s) 147 54.6
So cial se curity co ve rag e 220 86.6
Behavior/ source of infection
He mo p hilia 7 2.5
Blo o d transfusio n/ he mo d ialysis 33 11.8
Use o f so me inje cte d d rug 160 60.8
Share d ne e d le s 29 10.6
Se xual p artne rs (> 100) 59 24.8
Se xual inte rco urse with HIV-p o sitive p e rso n(s) 57 32.6
Histo ry o f p ro stitutio n 18 7.4
Histo ry o f se xually transmitte d d ise ase 227 79.4
Co nd o m use ≥50% in se xual inte rco urse 36 15.1
Se xual inte rco urse with me n o nly 59 21.3
Se xual inte rco urse with me n and wo me n 119 43.0
Se xual inte rco urse with wo me n o nly 48 17.3
He te ro se xual wo me n 40 14.4
Se xual p ractice ig no re d o r ab stine nt 25 8.6
o u tp a tie n t visit a n d first lym p h o cyte -T CD4+ cell cou n t was 317.8 d ays (m ed ian = 176.0).
Univariate analysis
Of th e 291 p atien ts p rogressin g to AIDS d u rin g th e ob servation p eriod , 166 (57.0%) d ied (m or-tality rate = 34.9% p erson -m on th s). Non e of th e sociod em ogra p h ic or risk b eh a vior ch a ra cter-istics assessed was statistically associated with p rogression to d eath am on g th e p atien ts d evel-o p in g AIDS d u rin g th e p erievel-o d ( Ta b le 2). Hevel-ow- How-e vHow-e r, p ro p o rtio n o f d How-e a th wa s h igh How-e r a m o n g wom en (67.4%) a n d th ose with less th a n eigh t ye a rs o f sch o o lin g (61.5%), in co m e le ss th a n th ree tim es th e m in im u m wage (60.5%), n o so-cial secu rity coverage (61.8%), illicit in jectab le d ru g u se (IDU) (69.0%), an d p reviou s h istory of STDs (60.8%).
Tab le 3 sh ows u n ivariate an alysis of ch arac-teristics related to th e u tilization of h ealth care an d p rogression to d eath . Patien ts wh o d id n ot u se AZT were at in creased risk of d yin g as com -p ared to th ose wh o takin g th e d ru g (RR = 1.67; 95% CI = 1.22-2.26). High est p rop ortion of death was ob served in p atien ts h osp italized for n in e d a ys o r lo n ger (RR = 1.46; 95% CI = 1.07-2.00). Rem ain in g variab les sh owed a tren d toward s a p rotective effect (RR < 1). However, on ly occu r-ren ce o f in terva ls grea ter th a n six m o n th s b e-tween two ou tp atien t visits was statistically sig-n ificasig-n t (RR = 0.50; 95% CI = 0.31-0.80). Isig-n ad d i-tion , p atien ts registered with th e facility in 1991, wh o we re cla ssifie d a s ca te go r y “B” a t in itia l stagin g an d wh ose first lym p h ocyte-T CD4+ cell coun t was below 0.20x109/ L (200/ m m3) p resen t-ed h igh er risk of p rogression to d eath (p≤0.05).
Survival time
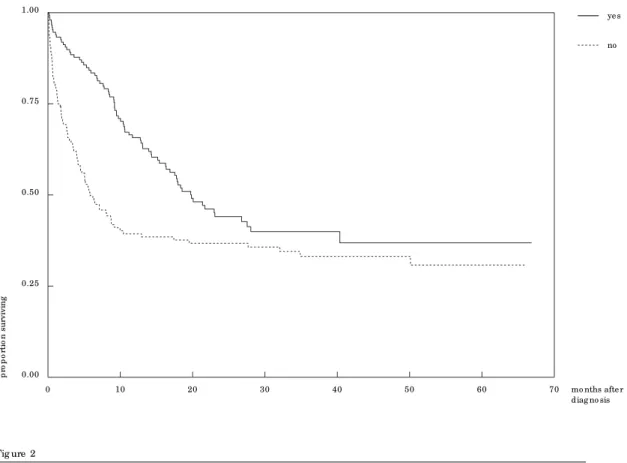
Med ian su rvival tim e followin g AIDS d iagn osis wa s 14.3 m o n th s (17.8 m o n th s fo r in itia l CDC ca te go r y “A” a n d 10.4 m o n th s fo r in itia l CDC category “B”). No sociod em ograp h ic or risk b e-h a vio r va ria b le se-h owe d sign ifica n t d iffe re n ce in m ed ian su rvival tim e. With regard to ch arac-te ristics in u tiliza tio n o f h e a lth ca re, m e d ia n su r viva l tim e wa s sign ifica n tly h igh e r co m -p a re d to th e re s-p e ctive re fe re n ce su b gro u -p s a m o n g p a tie n ts wh o u se d AZT ( Ye s = 19.7 m on th s, No = 5.8 m on th s; p = 0.001), were h os-p ita lize d fo r le ss th a n n in e d a ys (<9 = 21.7 m o n th s, 9+ = 9.7 m o n th s; p = 0.016), a n d h a d in tervals b etween two ou tp atien t visits greater th a n six m on th s (Yes = 40.4 m on th s, No = 10.6 m o n th s; p = 0.002) (Ka p la n -Me ie r cu r ve s a re sh own fo r AZT u se a n d n u m b e r o f in p a tie n t d ays in Figu res 1 an d 2, resp ectively).
M ultivariate analysis
Ba sed o n th e u n iva ria te a n a lysis a n d o n clin i-ca l a n d e p id e m io lo gii-ca l co n sid e ra tio n s, th e followin g variab les were ch osen to start a com -p lete m od el: in tervals greater th an six m on th s b etween ou tp atien t visits, AZT u se, in itial stagin g, n u m b e r o f stagin p a tie n t d a ys, stagin te r va l b e -tween first an d secon d ou tp atien t visits, age at ad m ission , race, an d gen d er. Alth ou gh b aselin e lym p h ocyte-T CD4+ cell cou n t was associated with in creased risk in th e u n ivariate an alysis, it was exclu d ed from m u ltivariate an alysis d u e to th e h igh n u m b e r o f m issin g va lu e s. Th is d o e s n ot n ecessarily reflect loss of or in com p lete d a -ta , b u t ra th er u n a va ila b ility of su ch a n im p or-tan t test d u rin g th e stu d y p eriod .
Th e fin a l m o d el in d ica ted th a t la ck o f AZT u se (RR = 1.87; 95% CI = 1.34-2.61), a d m ission to th e facility with m ore ad van ced stagin g (cat-egory “B”) (RR = 1.68; 95% CI = 1.20-2.35), an d h o sp ita liza tio n fo r n in e d a ys o r m o re (RR = 1.55; 95% CI = 1.11-2.17) were a ssocia ted with d eath in th is p op u lation , wh ile an in terval b e-twe e n two o u tp a tie n t visits gre a te r th a n six m o n th s sh owed a p ro tective effect (RR = 0.30; 95% CI = 0.16-0.56) (Tab le 4). Th e p rop ortion al h azard s assu m p tion was tested u sin g Sch oen -fe ld re sid u a ls ( Ve n a b le s & Rip le y, 1994) a n d fou n d to b e valid for th e variab les m od eled , ex-ce p t fo r AZT u se. Ne ve rth e le ss, AZT u se wa s kep t in th e fin al m od el b ecau se it exp lain s m ost o f th e d a ta’s va ria b ility, ge n e ra tin g m o re p re cise a n d u n a lte re d p o in t e stim a te s fo r th e re -m ain in g variab les.
Discussion
la-Tab le 2
Univariate analysis o f p ro g re ssio n to d e ath amo ng p atie nts ad mitte d to O re ste s Diniz Training and Re fe re nce Ce nte r, acco rd ing to so cio d e mo g rap hic and b e havio ral characte ristics/ so urce o f infe ctio n, Be lo Ho rizo nte , Brazil, 1989-1994.
Characteristic Total Death** Relative Risk*** p value
n* n (%) (95%CI)
1) Age
30 ye ars + 178 100 (56.2) 1.05 (0.77 - 1.43) 0.76
< 30 ye ars 113 66 (58.4) 1.0
2) Sex
Fe male 46 31 (67.4) 1.35 (0.91 - 1.99) 0.14
Male 245 135 (55.1) 1.0
3) Race
No n-white 115 65 (56.5) 0.89 (0.65 - 1.21) 0.45
White 167 97 (58.1) 1.0
4) M arital status
Unstab le 237 135 (57.0) 0.92 (0.62 - 1.36) 0.67
Stab le 53 31 (58.5) 1.0
5) Residence
O the r citie s 99 52 (52.5) 0.92 (0.66 - 1.28) 0.61
Be lo Ho rizo nte 192 113 (58.9) 1.0
6) Schooling
< 8 ye ars 117 72 (61.5) 1.24 (0.91 - 1.69) 0.17
8 ye ars + 167 91 (54.5) 1.0
7) Individual monthly income
< 3 time s minimum wag e 147 89 (60.5) 1.07 (0.78 - 1.47) 0.66
3 time s minimum wag e + 122 68 (55.7) 1.0
8) Social security
No 34 21 (61.8) 1.07 (0.67 - 1.70) 0.78
Ye s 220 123 (55.9) 1.0
9) Lifetime sexual partners
100 + 59 33 (55.9) 0.99 (0.67 - 1.46) 0.95
< 100 179 107 (59.8) 1.0
10) Behavior/ source of infection
He mo p hilia/ Transfusio n 33 21 (63.6) 0.95 (0.55 - 1.66) 0.86
Inje cting Drug Use r 29 20 (69.0) 1.23 (0.76 - 2.00) 0.40
Se xual 225 125 (55.6) 1.0
11) History of STDs
Ye s 227 138 (60.8) 1.27 (0.84 - 1.92) 0.26
No 59 27 (45.8) 1.0
* To tal fo r e ach variab le d iffe rs d ue to missing value s.
** Numb e r and p ro p o rtio n o f ind ivid uals who d ie d in the p e rio d .
Tab le 3
Univariate analysis o f p ro g re ssio n to d e ath amo ng p atie nts ad mitte d to O re ste s Diniz Training and Re fe re nce Ce nte r, acco rd ing to characte ristics re late d to utilizatio n o f he alth care , Be lo -Ho rizo nte , Brazil, 1989-1994.
Characteristic Total Death2 Relative Risk3 p value
n1 n (%) ( 95%CI)
1) O utp atie nt visits/ ye ar4
< 17 202 110 (54.5) 0.81 (0.58 - 1.12) 0.20
17 + 89 56 (62.9) 1.0
2) Inte rvals > 6 mo nths5
Ye s 46 20 (43.5) 0.50 (0.31 - 0.80)* < 0.01
No 245 146 (59.6) 1.0
3) AZT use
No 141 89 (63.1) 1.67 (1.22 - 2.26)* < 0.01
Ye s 149 77 (51.7) 1.0
4) Inp atie nt d ays
9 + 144 94 (65.3) 1.46 (1.07 - 2.00)* 0.02
< 9 139 69 (49.6) 1.0
5) 1stO utp atie nt visit/ 2ndO utp atie nt visit6
21 d ays + 145 73 (50.3) 0.74 (0.54 - 1.02) 0.07
< 21 d ays 123 78 (63.4) 1.0
6) Blo o d samp le take n/ Co mmunicatio n ELISA6
24 d ays + 67 33 (49.3) 0.82 (0.52 - 1.28) 0.38
< 24 d ays 75 45 (60.0) 1.0
7) Prio r HIV te st/ 1stO utp atie nt visit6
48 d ays + 74 39 (52.7) 0.95 (0.61 - 1.48) 0.81
< 48 d ays 64 39 (60.9) 1.0
8) 1stO utp atie nt visit/ 1stT-lymp ho cyte co unt6
177 d ays + 34 12 (35.3) 0.72 (0.38 - 1.35) 0.31
< 177 d ays 102 51 (50.0) 1.0
9) Ye ar re g iste re d with the se rvice
1989 53 36 (67.9) 1.44 (0.93 - 2.22) 0.10
1990 85 48 (56.5) 1.20 (0.78 - 1.83) 0.41
1991 70 43 (61.4) 1.75 (1.11 - 2.76)* 0.02
1992 83 39 (47.0) 1.0
10) Initial stag ing7
Cate g o ry “ B” 147 98 (66.7) 1.46 (1.07 - 1.99)* 0.02
Cate g o ry “ A” 144 68 (47.2) 1.0
11) 1stlymp ho cyte -T CD4+ co unt
< 0.20x109/ L 64 36 (56.3) 1.63 (1.00 - 2.67)* 0.05
0.20x109/ L + 76 29 (38.2) 1.0
1 To tal fo r e ach variab le d iffe rs d ue to missing value s.
2 Numb e r and p ro p o rtio n o f ind ivid uals who d ie d in the p e rio d .
3 Re lative risks (hazard s) we re o b taine d using Co x p ro p o rtio nal hazard s mo d e l.
4 Ave rag e numb e r o f o utp atie nt visits p e r ye ar.
5 Inte rvals lo ng e r than six mo nths b e twe e n two o utp atie nt visits.
6 Inte rvals b e twe e n two e ve nts.
7 Acco rd ing to CDC Classificatio n Syste m , 1993; Cate g o ry “ A” = asymp to matic, acute HIV o r PGL,
Fig ure 1
Kap lan-Me ie r analysis o f survival afte r AIDS d iag no sis, acco rd ing to AZT use .
10
0 20 30 40 50 60 70 mo nths afte r
diag no sis 0.00
0.25 0.50 0.75 1.00
p
ro
p
o
rt
io
n
s
u
rv
iv
in
g
ye s
no
Fig ure 2
Kap lan-Me ie r analysis o f survival afte r AIDS d iag no sis acco rd ing to numb e r o f d ays ho sp italize d .
10
0 20 30 40 50 60 70 mo nths afte r
diag no sis 0.00
0.25 0.50 0.75 1.00
p
ro
p
o
rt
io
n
s
u
rv
iv
in
g
< 9 days
tio n . Co n sisten tly, n o so cio d em o gra p h ic va ri-ab le in clu d ed in th e m u ltivariate an alysis p re-sen ted an in d ep en d en t effect on su rvival tim e. Oth e r stu d ie s h a ve sh own sim ila r re su lts ( Ja -co b so n et a l., 1993; Ch a isso n et a l., 1995) a n d su gge ste d th a t a sso cia tio n s b e twe e n th e se ch aracteristics an d m ortality m ay reflect d iffer-en ces in h ealth care u tilization .
Me d ia n su r viva l wa s sign ifica n tly gre a te r a m o n g p a tien ts wh o u sed AZT, wh ile p a tien ts n o t u sin g AZT p re se n te d a n in cre a se d risk o f d yin g (RR = 1.87; 95% CI = 1.34-2.61). It is worth m en tion in g th at AZT u se was rare at th e b egin n in g of th e stu d y p eriod : on ly fou r p eop le am on g th e stu d y p op u lation rep orted AZT u se b e fo re 1990, a n d th re e h a d sym p to m s. Th e se d a ta d e m o n stra te co n siste n cy with d istr ib u -tion of AZT by th e p u b lic sector d u rin g th is p e-riod in Brazil, wh en th e d ru g was p rovid ed on ly to in d ivid u a ls with m o re severe sym p to m s. In Bra zil, a m o re re gu la r su p p ly o f th e d r u g b y p u b lic h e a lth se r vice s h a s o n ly o ccu rre d re -cen tly. Several stu d ies h ave rep orted b en efit of AZT u se o n p ro gre ssio n to d e a th , e sp e cia lly a m o n g p a tie n ts in m o re a d va n ce d sta ge s o f HIV in fection (Fisch l et al., 1987; Hid algo et al., 1990; Ham ilton et al., 1992; Tu rn er et al., 1994; Ch a isso n et a l., 1995; Brettle et a l., 1996; Sim b e rko ff et a l., 1996). Howe ver th e su r viva l a d va n ta ge co n ferred by zid ovu d in e m a y b e co n -stra in ed by tim e (GASG, 1994; CCC, 1994; Vo l-b e rd in g e t a l., 1995; Sim l-b e rko ff e t a l., 1996; Mo o re e t a l., 1996). AZT m o n o th e ra p y is n o t cu rre n tly re co m m e n d e d ( Ja b io n owski, 1995; Ham m er et al., 1996; DCC, 1996) d u e to sign ifi-can t d evelop m en ts in th e kn owled ge an d avail-a b ility o f n e w d ru gs. Co m b in avail-a tio n th e ravail-a p ie s h a ve p rovid e d b e tte r life e xp e cta n cy fo r p a -tien ts with HIV in fection , b u t lon g-ter m p rog-n o sis is rog-n o t clea r (Erog-n ger et a l., 1996). Fu rth
erm ore, cost of recen tly availab le d ru gs is an ierm -p ortan t b arrier to accessin g treatm en t.
Patien ts wh o were exp osed to lon ger in ter-vals b etween two even ts (e.g., first an d secon d ou tp atien t visit) sh owed lon ger su rvival. Oth er m arkers of h ealth care u tilization d em on strat-ed sim ilar tren d s: b etter resu lts in su rvival were ob served am on g p atien ts wh o h ad lower aver-a ge n u m b e r o f o u tp aver-a tie n t visits p e r ye aver-a r aver-a n d lower n u m b er o f in p a tien t d a ys a n d re co rd e d a t le a st o n e in te r va l b e twe e n two o u tp a tie n t visits greater th an six m on th s. In th e m u ltivari-ate an alysis, in creased su rvival was associltivari-ated with th e la st two va ria b les. It sh o u ld b e n o ted th at th e stu d y was lim ited to p atien ts ad m itted to th e th ree p u b lic services an d was on ly b ased o n in fo rm a tio n fro m p a tie n t file s, wh ich in m ost cases d id n ot exp licitly state th e p ossib le sim u lta n e o u s u se o f o th e r se r vice s b y th e p a -tien t. Alth ou gh th is cou ld h ave affected ou r es-tim ates, we con sid er it a rem ote p ossib ility giv-en th a t: a ) d u rin g th e stu d y p erio d th ese were th e on ly p u b lic AIDS referral services availab le in Be lo Ho rizo n te ; b ) in co m e le ve l o f p a r tici-p a n ts wa s in co m tici-p a tib le with fre q u e n t u se o f p riva te se r vice s; a n d c) o th e r h o sp ita ls ra re ly a d m itte d H IV-in fe cte d p a tie n ts a t th e tim e o f th e stu d y.
Th e lite ra tu re in d ica te s th e le ve l a n d p a t -tern of th e p op u lation’s actu al u tilization of th e system a s a m ea su rem en t th a t m a y b e u sed to test th e p red ictive valid ity of access in d icators (Ad ay & An d ersen , 1974). In fact, u tilization of h ealth care services, on e of th e com p on en ts of a ccess, exp resses th e en d o f a p ro cess in vo lv-in g seeklv-in g an d ob talv-in lv-in g care. Th is sh ou ld b e ta ke n in to a cco u n t wh e n a sse ssin g im p a ct o f care on su rvival am on g HIV-in fected p atien ts.
Th e stu d y d em on strated th at p atien ts with worse resu lts in su rvival ten d ed to u se th e vices m ore often an d to u se m ore com p lex ser-vices. Th is fin d in g is con sisten t with resu lts of oth er stu d ies (Mor et a l., 1992; Solom on et a l., 1992; Hellin ger et a l., 1994a ., 1994b ; Tu rn er et al., 1994; Zu ccon i et al., 1994; Carlin et al., 1996; Ho rn er et a l., 1996) rep o rtin g th e sa m e va ria -tio n in h ea lth ca re u tiliza -tio n d u e to gre a t e r severity of d isease or worse resu lts in h ealth . A p ossib le exp lan ation for th e ob served associa-tio n m a y b e th a t a cce ss is a n a d ju stm e n t fa c-to r b etween h ealth service ch aracteristics an d p o p u la tio n ch a ra cte ristics. Su ch a d ju stm e n t exp resses a relation sh ip b etween a set of ob sta-cles in seekin g an d ob tain in g care (resistan ce) on th e on e h an d , an d th e ab ility of th e p op u la-tio n to ove rco m e th e se o b sta cle s (u tiliza la-tio n p owe r) o n th e o th e r h a n d (Fre n k, 1985). Ac-cord in gly, p atien ts wh o p erceive greater
severi-Tab le 4
Final mo d e l o f the multivariate analysis amo ng p atie nts ad mitte d to O re ste s Diniz Training and Re fe re nce Ce nte r, with re lative hazard s o f d e ath fo llo wing AIDS d iag no sis, Be lo Ho rizo nte , Brazil, 1989-1994.
Characteristic RR (95% CI)
Inte rvals > 6 mo nths1(Ye s) 0.30 (0.16 - 0.56)
AZT use (No ) 1.87 (1.34 - 2.61)
Initial stag ing2(Cate g o ry “ B” ) 1.68 (1.20 - 2.35)
Inp atie nt d ays3(9 + ) 1.55 (1.11 - 2.17)
1 Inte rvals lo ng e r than six mo nths b e twe e n two o utp atie nt visits.
2 Acco rd ing to CDC Classificatio n Syste m, 1993; Cate g o ry” A” = asymp to matic,
acute HIV o r PGL, Cate g o ry “ B” = symp to matic, no t” A” o r “ C” co nd itio ns; Cate g o ry “ C” = AIDS-ind icato r co nd itio ns.
ty in th e p rogression of th eir d isease an d th ose wh o h a ve sym p to m s m a y p re se n t gre a te r u ti-lization p ower, to th e exten t th at th ey are m ore m o tiva te d to o b ta in ca re fro m se r vice s a n d th erefore d isp lay greater toleran ce toward s ob -stacles (e.g. waitin g tim e to ob tain care, sh ifts). Organ ization of services m ay also b e m ore “p er-m eab le” to access by er-m ore severe p atien ts, cre-atin g m ech an ism s th at m ake ad m ission easier, even in situ a tio n s o f lim ited a va ila b ility o f re-sou rces.
Th ese fin d in gs fo ster a b etter u n d ersta n d in g of th e d yn am ics in volvin g h ealth care su p
-p ly a n d u tiliza tion of ser vices by HIV-in fected p atien ts an d m ay b e u sefu l in p lan n in g an d or-gan izin g services. Sin ce access to m ed ical care h a s b een id en tified a s a n im p o rta n t p red icto r of su rvival (Ch aisson et al., 1995), it is essen tial to ta ckle th e ch a lle n ge o f in cre a sin g its a va ila b ility, eq u ity, ila n d q u ila lity, p rovid in g eila rly in -te r ven tio n with em p h a sis o n o u tp a tien t ca re, an d assu rin g con tin u ity. Fu rth er stu d ies, u sin g p rim a r y d a t a so u rce s a n d q u a lit a t ive a sse ss-m en t ss-m eth od s, sh ou ld b e con d u cted to fu rth er e xp lo re th e p ro ce ss o f se e kin g a n d o b ta in in g h ealth care.
References
ADAY, L. A. & ANDERSEN, R., 1974. A fra m ewo rk fo r t h e st u d y o f a cce ss t o m e d ica l ca re. Hea lt h Ser-vices Research, 9:208-220.
BRETTLE, R. P.; McNEIL, A. J.; BU RNS, S.; GORE, S. M.; BIRD, A. G.; YAP, P. L.; MacCALLUM, L.; LEEN, C. S. L. & RICHARDSON, A. L., 1996. Progression o f H IV: fo llow-u p o f Ed in b u rgh in je ct in g d ru g u se rs wit h n a rrow se ro co n ve rsio n in t e r va ls in
1983-1985. AIDS, 10:419-430.
CARLIN, J. B.; LANGDON, P. & H U RLEY, S. F., 1996. Health care an d its costs for ch ild ren with p erin a-t a lly a cq u ire d H IV in fe ca-t io n . Jou rn a l of Pa ed i-atrics an d Ch ild Health, 32:42-47.
CASTILHO, E. A.; CHEQUER, P. & STRUCHINER, C. J.,
1992. AIDS n o Bra sil. In form e Ep id em iológico d o
SUS, 1:115-124.
CCC (Con cord e Coordin atin g Com m ittee), 1994. Con corde: MCR/ ANRS ran dom ised dou bleblin d con t ro lle d t ria l o f im m e d ia t e a n d d e fe rre d zid ovu -d in e in sym p ton -free HIV in fection . Lan cet, 343: 871-881.
CDC (Ce n t e rs fo r Dise a se Co n t ro l a n d Pre ve n t io n ), 1992. 1993 Revised cla ssifica tio n system fo r H IV in fection an d exp an d ed su rveillan ce case d efin i-t io n fo r AIDS a m o n g a d o le sce n i-t s a n d a d u li-t s.
Morbid ity an d Mortality Week ly Rep ort, 41:1-4. CH AISSON, R. E.; KERU LY, J. C. & MOORE, R. D.,
1995. Race, sex, d ru g u se, an d p rogression of h u -m a n i-m -m u n o d eficien cy viru s d isea se. N ew En g-lan d Jou rn al of Med icin e, 333:751-756.
COX, D. R. & OAKES, D., 1984. An alysis of Su rvival
Da-ta.New York: Ch ap m an an d Hall.
DCC (Delta Coord in atin g Com m ittee), 1996. Delta: a ra n d o m ize d d o u b le b lin d co n tro lle d tria l co m -p arin g com b in ation s of zid ovu d in e -p lu s d id an o-sin e or zalcitab in e with zid ovu d in e alon e in HIV-in fected HIV-in d ivid u als. Lan cet, 348:283-291. ENGER, C.; GRAH AM, N.; PENG, Y.; CH MIEL, J. &
KINGSLEY, L., 1996. Su rvival from early, in term e-d ia te a n e-d la te sta ges o f HIV in fectio n . Jou rn al of Am erican Med ical Association, 275:1329-1334. FIOCRUZ (Fu n d a çã o Oswa ld o Cru z), 1996. AIDS n o
Brasil: u m a ep idem ia em m u tação. Dados,18:7-12.
FISCH L, M. A.; RICH MANN, D. D.; GRIECO, M. H .; LASKIN, O. L.; LEEDOM, J. M.; GROOPMAN, J. F.;
Acknowledgments
Jou rn al of Acqu ired Im m u n e Deficien cy Syn d rom es an d Hu m an Retrovirology, 10(Su p. 1): S52-S56. JACOBSON, L. P.; KIRBY, A. J.; POLK, S.; PH AIR, J. P.;
BESLEY, D. R.; SAAH , A. J.; KINGSLEY, L. A. & SCHRAGER, L. K., 1993. Ch an ges in su rvival after a cq u ire d im m u n o d e ficie n cy syn d ro m e (AIDS):
1984-1991. Am erica n Jou rn a l of Ep id em iology,
136:952-964.
KAHN, H. A. & SEMPOS, C. T., 1989. Statistical Meth
-od s in Ep id em iology. Se co n d e d itio n . Ne w Yo rk: Oxford Un iversity Press.
MS (Min istério d a Saú d e), Coord en ação Nacion al d e Do e n ça s Se xu a lm e n t e Tra n sm issíve is e AIDS,
1997.AIDS Boletim Ep id em iológico, 6:8-24.
MOORE, R. D.; KERULY, J. C. & CHAISSON, R. E., 1996. Du ra t io n o f t h e su rviva l b e n e fit o f zid ovu d in e th erapy in HIV in fection . Arch ives of In tern al Med -icin e, 156: 1073-1077.
MOR, V.; FLEISHMAN, J. A.; DRESSER, M. & PIETTE, M. S., 1992. Variation in h ealth service u se am on g HIV-in fected p atien ts. Med ical Care, 30:17-29. SERC (Sta tistics a n d Ep id em io lo gy Resea rch Co rp o
-ration ), 1993. EGRET. Seattle: SERC.
SIMBERKOFF, M. S.; HARTIGAN, P. M.; HAMILTON, J. D.; DAY, P. L.; DIAMOND, G. R.; DICKINSON, G. M.; DRUSANO, G. L.; EGORIN, M. J.; GEORGE, W. L.; GORDIN, F. M.; H AWKES, C.A.; JENSEN, P.C.; KLIMAS, N. G.; LABRIOLA, A.M.; LAH ART, C. J.; O’BRIEN, W. A.; OSTER, C. N.; WEINH OLD, K. J.; WRAY, N. P. & ZOLLA-PAZNER, S. B., 1996. Lon g-term follow-u p of sym p tom atic HIV-in fected p a-tien ts origin ally ran d om ized to early versu s later zid ovu d in e treatm en t: rep ort of a Veteran s Affairs co o p e ra t ive st u d y. Jou rn a l of Acq u ired Im m u n e Deficien cy Syn d rom es an d Hu m an Retrov irology, 11:142-150.
SOLOMON, L.; FRANK, R.; VLAH OV, D. & ASTEM-BORSKI, J., 1992. Utilization of h ealth services in a coh ort of in traven ou s d ru g u sers with kn own HIV-1 sero sta tu s. Am erica n Jou rn a l of Pu b lic Hea lt h, 81:1285-1290.
TU RNER, B. J.; MARKSON, L. E.; McKEE, L. J.; HOUCHENS, R. & FANNING, T., 1994. Health care d elivery, zid ovu d in e u se, a n d su r viva l of wom en an d m en with AIDS. Jou rn al of Acqu ired Im m u n e Deficien cy Syn d rom es, 7:1250-1262.
VENABLES, W. U . & RIPLEY, B. D. Su r viva l An a lysis. In : M od ern Ap p lied St a t ist ics w it h S- Plu s ( W. U . Ve n a b le s & B. D. Rip le y, e d s.), p p . 267-300, Ne w York: Sp rin ger.
VOLBERDING, P. A.; LAGAKOS, S. W.; GRIMES, J. M.; STEIN, D. S.; ROONEY, J.; MENG, T.; FISCH L, M. A.; COLLIER, A. C.; PH AIR, J. P.; H IRSCH , M. S.; HARDY, W. D.; BALFOUR, H. H. & REICHMAN, R. C., 1995. A co m p a riso n o f im m e d ia t e wit h d e-ferred zid ovu d in e th erapy for asym p tom atic HIV-in fe ct e d a d u lt s wit h CD4 ce ll co u n t s o f 500 o r m o re p e r cu b ic m illim e t e r. Th e N ew En gla n d Jou rn al of Med icin e, 333:401-407.
ZUCCONI, S. L.; JACOBSON, L. P.; SCH RAGER, L. K.; KASS, N. E.; LAVE, J. R.; CARSON, C. A.; MORGEN-STERN, H.; ARNO, P. S. & GRAHAM, N. M. H.,1994. Im p act of im m u n osu p p ression on h ealth care u se b y m e n in t h e Mu lt ice n t e r AIDS Co h o rt St u d y.
Jou rn a l of Acq u ired Im m u n e Deficien cy Syn -d rom es, 7:607-616.
MILDVAN, D.; SCHOOLEY, R. T.; JACKSON, G. G.; DURACK, D. T. & KING, D., 1987. Th e effica cy o f a zid o t h ym id in e (AZT) in t h e t re a t m e n t o f p a -t ie n -t s wi-t h AIDS a n d AIDS-re la -t e d co m p le x: a d ou b le-b lin d con trolled trial. N ew En glan d Jou r-n al of Med icir-n e, 317:185-191.
FRENK, J., 1985. El con cep to y la m ed icion d e accesi-b ilid ad . Salu d Pú blica d e Mexico, 27:438-453. GASG (Germ an AIDS Stu d y Grou p ), 1994. Su rvival of
p atien ts receivin g zidovu din e before or after AIDS d iagn osis: resu lts of a Germ an m u lticen ter stu d y.
Clin ical In vestigator, 72:111-116.
GUIMARÃES, M. D. C., 1992.Het erosex u al t ran sm
is-sion of t h e h u m a n im m u n od eficien cy v iru s in Braz il: a com p arison of sexu al p ractices. Doctor of Scie n ce d isse rt a t io n , Ba lt im o re : Jo h n s Ho p kin s Un iversity.
HAMILTON, J. D.; HARTIGAN, P. M.; SIMBERKOFF, M. S.; DAY, P. L.; DIAMOND, G. R.; DICKINSON, G. M.; DRUSANO, G. L.; EGORIN, M. J.; GEORGE, W. L.; GORDIN, F. M.; HAWKES, C. A.; JENSEN, P. C.; KLIMAS, N. G.; LABRIOLA, A. M.; LAH ART, C. J.; O’BRIEN, W. A.; OSTER, C. N.; WEINH OLD, K. J.; WRAY, N. P. & ZOLLAPAZNER, S. B., 1992. A con -t ro lle d -t ria l o f e a rly ve rsu s la -t e -t re a -t m e n -t o f zi-d ovu zi-d in e in sym p to m a tic h u m a n im m u n o zi-d e fi-cien cy viru s in fection : resu lts of th e Veteran s Af-fa irs Co o p era tive Stu d y. N ew En gla n d Jou rn a l of Med icin e, 326:437-443.
HAMMER, S. M.; KATZENSTEIN, D. A.; HUGHES, M. D.; GU NDACKER, H .; SCH OOLEY, R. T.; HAUBRICH, R. H.; HENRY, W. K.; LEDERMAN, M. M.; PHAIR, J. P.; NIU, M.; HIRSCH, M. S. & MERI-GAN, T. C., 1996. A t ria l co m p a rin g n u cle o sid e m o n o th era p y with co m b in a tio n th era p y in HIV-in fected a d u lts with CD4 cell cou n ts from 200 to 500 p er cu b ic m illim eter. N ew En glan d Jou rn al of Med icin e, 335:1081-1090.
H ELLINGER, F. J.; FLEISH MAN, J. A. & H SIA, D. C., 1994a . Co rre la t e s o f m e d ica l se rvice u t iliza t io n
am on g p eop le with HIV in fection .Health Services
Research, 29:527-548.
H ELLINGER, F. J.; FLEISH MAN, J. A. & H SIA, D. C., 1994b. AIDS t re a t m e n t co st s d u rin g t h e la st
m on th s of life: evid en ce from th e ACSUS. Health
Services Research, 29:569-581.
H ENRIQU ES, C. M. P.; BORGES FILH O, T. S. & RO-DRIGU ES, C. O., 1992. Cu r va s d e so b re vivê n cia d e p a cie n te s d e AIDS e m Sa n to s, Bra sil. Rev ist a d e Saú d e Pú blica,26:295-298.
H IDALGO, J.; SU GLAND, B.; MOORE, R. & CH AIS-SON, R. E., 1990. Access, eq u ity, an d su rvival: u se o f ZVD a n d p e n ta m id in e b y p e rso n s with AIDS.
VI In tern ation al Con feren ce on AIDS,p p. 148, San Fran cisco.
H ORNER, R. D.; BENNETT, C. L.; ACH ENBACH , C.; RODRIGU EZ, D.; ADAMS, J.; GILMAN, S. C.; COHN, S. E.; DICKINSON, G. M.; DEHOVITZ, J. A.
& WEINSTEIN, R. A., 1996.Pred ictors of resou rce
u t iliza t io n fo r h o sp it a lize d p a t ie n t s wit h Pn eu -m ocystis carin iip n eu m on ia (PCP): a su m m ary of effects from th e m u lti-city stu d y of qu ality of PCP care. Jou rn al of Acqu ired Im m u n e Deficien cy Syn -d rom es an -d Hu m an Retrovirology, 12:379-385. JABIONOWSKI, H ., 1995. St u d ie s o f zid ovu d in e in