High priority was given to relieving epidemiologists of the numerous administrative tasks they now have to perform and to seeking means of avoiding the fre-quent turnover of personnel in local and district service units.
Immediate Measures
As a result of their deliberations on priorities, the participants in the meeting agreed to recommend to the Minister of Health and Social Welfare the establish-ment by resolution of a Working Group or Committee for the Integral Development of the Teaching and Prac-tice of Epidemiology in Venezuela. The members of the group should be representatives of the different agencies of the Ministry of Health and Social Welfare, other health institutions, and teaching and research centers, and be advised by PAHO.
In the immediate future the group will execute the following activities:
1. Frame and propose policies for epidemiological research.
2. Define and propose a career post of epidemi-ologist and the incentives needed for its consolidation.
3. Establish flexible mechanisms for the
dissemina-tion of scientific informadissemina-tion in epidemiology, includ-ing a technical periodical.
4. Arrange technical events in epidemiology and promote the conduct and publication of research by epidemiologists.
5. Review the epidemiological reporting systems at all levels.
6. Establish model protocols for research on diag-nosis, health profiles, and related matters, and promote the mobilization of technical and financial resources for carrying them out.
7. Formulate a plan for the integral development of the teaching and practice of epidemiology in Venezuela and propose specific projects suitable for cooperative execution by local and international agencies.
To ensure the continuity of the work, it was recom-mended that membership in this group be based on institutional and not personal affiliations.
Finally, it was considered advantageous for the com-mittee established in 1984, and which performed the national evaluation and arranged the meeting, to con-tinue to function until the proposed working group is set up. That committee should go on working to create favorable conditions for implementation of the recom-mendations approved at the meeting.
Inventory of Human Resources in Epidemiology
The Epidemiology Unit of the Pan American Health Organization is developing an information system of human resources in epidemiology. The Unit will use this inventory of professionals to identify consultants in specific areas, candidates for job openings, and re-source persons for seminars and workshops. To this end, qualified and interested readers of the Bulletin
are invited to participate by having their name and specialized background included in the inventory. Aside from mailing address, the following should be specified: present employment and relevant employ-ment history, educational background, and area of special experience and/or training in epidemiology.
Leading Causes of Death, Canada, 1983
Most recent mortality rates for Canada, calculated from data provided by Statistics Canada, are presented in Table 1. Ischaemic heart disease is still the single most important cause of death for males and females in the 25-74 age range (Table 2). However, in the period 1969 to 1983 the age-standardized mortality rate for ischaemic heart disease declined by 32.1% for males and 37.0% for females. The all-cause mortality rates declined by 19.4% for males and 22.0% for
females in this period. Over the same period, the male cancer mortality rate increased by 6.4% and the female rate decreased by 1.7%. Figures 1 and 2 indicate the time-trend rates for the leading five causes of death for both males and females. The most significant in-crease is for female lung cancer mortality, 152.3% from 1969 to 1983. In the September 1982 issue of
Chronic Diseases a prediction was made that if current trends continued for female lung cancer mortality a
e
1 --
~~~
, oe Ca4 x ofi 9o~
e 0N o00 0'0
00 r4 CD 00 m In
_ x t
"-NX00 vi '00
-9 0' en'01
0 t o
-o n e 00
-oo~ -~~\
X' N_ r> _ 0 mu 0' 0'h F-x
0'b N_
'0 \ r-e---0
00o e'- N
'0F- en'
-0'v> Ni
n 00 0 o -D n
_m U)c t so
0'o en N e- 0 e
000 en'0
-ol N
08 0 en fe N ee
ob r -x
0' F en 0 0'0
clq <:p
0-: en- -O
gvi N_
X 0 - en
--N enr r.
o V N
-0'fe N
a<, CD .
X~ Oe V-o
-4 '0N en
N0 Nr N X
O n N _
_- mr
r4>eF
A_ r4 _ - r4 _' < M>
00
N o
"
Q o 0 -l "f N SV N O _ '0 0 N _ ' '0b \00
x _ nx -rI r o -0 9 000 C. o e n- -I
en0E Q\ t- '00 - i .0 en0 7 O N or- o o 000 ow'
oa 00t x -"0
~~:oo
0o o - -m = o o; %m 00 00 "o; M00' sfi ; " 0'0 · D "- eno m - N r q (7rI N , - 0 N - -- C N0 N N- N
'0N Oe 0- 00 en oe 0 -'o -~ (smiN 'l 'o N
'e n N0 ' 0c N 0' - en F40' en- ere 000' en- '0
rIN - 00N en I - - - F0' o e n -m
oE X u oi 09 p o
~
o - r-N
an m - -a - 00 0-0 , r- NO N'i al
r--eNns - xe O - F- ri r- - o v og 0 en- 9
--al oc _ xD v r\ CD x o a, n o_ a, m
r-x en e xe x 00 - N r- 0 NN ' 0 ' >-o Oe -' o
-o 00 fl c-'o Or - en NO 0'n 00' e-
enI--NN -~· OON - ''--ne c
eN Nv n - -' .n 0 x e ' r. o 0'- v Fv 0_ o
0'e N 0 X -0 N = e eo_ _ 'fl'n oN
NN - P 00N en - 0- enm en
en-0'0' N(b .-.0 d \O ' 00 -o 'oF- -m -vi N'0\
00en NN In00 a,' - N en N- C'
tr-- 0 -i - -- eo ;n en,· en-:
-- No d 00 '0 0"0 r-F- 0- '-e- '000 oen
alN o00 -i O - N en- 000' al -
~0
t - NN r4NN -] 00- - -- en v e
-ene 0'- st0' '0)
0 en N 00 m.0
riN - _- '
en enr r.r 0' '00 S n0 x ' en en c -'0 r. e m X e- -N
_ _ _- E en - -O
00' lN t m e00 oN N
NN - 10-t - -- v V e ) 0 o (N
e-De 0e e n - 0' m m rm N0 0 00 -0r- x o x n
nN -t rm- 0 -4 rm N 'N X -Sm a,\
oai-N O r4 m en m e r.0' en- '00 7NN N rm N
-r. S-r. m--= - en N '00 00- eN0' en0 0Xi r i 0
NN X - rO ^ - - -- X.en 's en NC
NN -t '- - - -- r.en '0e e
-E L L ErI L CL L u, EiL.L Ç ECi. ZS L
en
en-m
r
--r N~
'0
t m n O
r. _ 00 _ 0 - <N en O oen O . 0'
-0' en
1 enm
r.
en - 1- -:7
(<;' _m l_ _
fe s -0 0 o0
xN en- v
00N00 (7'0a
N i N
'0- vf O b
-v;, o; r- CS N - N
--m en 0 O N
v~ F- - 000
ni - N·
-v o- xo oD F-~ Sfe'0 roN
0- 00
c - N
-r- t x- x
N - N
-'0 00X- 'e _
N -_
c-0' r. o N
'0 0
X
-0 -0
N r. '00
X -en -en
X 0'
'o 00
N n
u>m 00
-enr4
n en
00 1,1
00 t
0 00 en N 00 0D
. eV N m en O 'ON
en - N- r_-0
00
r-'0N '00 000' -r.
r.en enen '0I- Nr.
en- N- 0"0O 00
'0 -N 7 en 0Xfe
ro .ríq i vi t 9 ri n - m0 0
X~ q° >~v S= m
O 09 o;' 00 Xt
X ,t _0In°
r.'0 N0 N-- o.'0
0. r_ e r.- 'ON
en- N - 00 r 00
00 '00' -0 00'0
en- N- 0'
0'
~
r.en -0 00' o 00 o
- N- 00
m 0' on CD m oL ,6 0' 0' o C)en 0' wu
e00 m
0 r~~~~~~~~~~~~~~~~~~~~r1
~~~~~~~~~~~~~-
0 .0U
o O 0o mO c 10 0.e>e o O .
E E 0o E E1 0 o E~E ej pa o>~0
0>~
~ ~
-0 >~ ~
-. 0 - - - e > - - . . ~~
E e- o o e ." o o
~
o 'D~
~>
oo. j 0O > 0 .> "~~ > e o ._. _ e 0 > 1 . 0 > -° 0 - ce O"~'
eO O - C O O - O 0 > 0 0 >
-~~ - EO PE -o r .0 E e Pž~
-- o u u z
· c C
:~~-
:~ :~~
E:-
e e 3 e
~ 00; a' e-E; 6, o e-a o..1
6 o.~e.
6 o E N 6~ '< -a 00 0' o\ r. 0' m r-N r. 0' r° r-0' 0' '0 0' u0 .0 o u U, .0 o UOE , r._B0
-
>--CC
zO
=> .0
o
-NO " 0>
0 O
0> zcC;
.0-m0
e,
eOU
Figure 1. Time trends of major causes of death for Canadian males, 1969-1983.
Figure 2. Time trends of major causes of death for Canadian females, 1969-1983.
200 r
O--C-
o
100-_90
800_
70
60
f 50
40
.30
20
-o
8~~~~~~~~~~~~~~2
$===
o
o
-
.
1969 70 71 72 73 74 75 76 77 78 79 80 81 82 83
Year
I 1 1 I I I I I l 1 1 1 l
1969 70 71 72 73 74 75 76 77 78 79 80 81 82 83
Year
Table 2. Leading causes of death, Canada, 1983.
Ranka Male ASMR" Female ASMR
I Ischaemicheartdisease 254.6 Ischaemicheartdisease 84.3
2 Malignant neoplasm of trachea, bronchus and 91.1 Malignant neoplasm of female breast 40.2
lung; and of pleura
3 Cerebrovascular disease 38.6 Cerebrovasculardisease 28.1
4 Suicide and selfinflicted injury 30.0 Malignant neoplasm of trachea, bronchus and 27.5
lung; and of pleura
5 Malignant neoplasm of colon; and of rectum, 28.9 Malignant neoplasm of colon; and of rectum, 21.6
rectosigmoidjunction and anus rectosigmoidjunction and anus
6 Chronic obstructive pulmonary disease 27.9 Malignant neoplasm of ovary and other uterine 10.5
adnexa
7 Chronic liver disease and cirrhosis 21.6 Suicide and selfinflicted injury 10.5
8 Motor vehicle traffic accidents 21.5 Chronic obstructive pulmonary disease 10.2
9 Malignant neoplasm of prostate 14.2 Diabetes mellitus 9.1
10 Malignant neoplasm of pancreas 13.9 Chronic liver disease and cirrhosis 9.0
11 Malignant neoplasm of stomach 13.0 Motor vehicle traffic accidents 8.7
12 Diabetes mellitus 11.0 Malignant neoplasm of pancreas 8.3
13 Nephritis, nephrotic syndrome and nephrosis; 5.3 Malignant neoplasm of stomach 5.6
and other kidney diseases
14 Gastric, duodenal, peptic, and gastrojejunal 3.6 Nephritis, nephrotic syndrome and nephrosis; 4.1
ulcers and other kidney diseases
15 ... Gastric, duodenal, peptic, and gastrojejunal 1.4
ulcers
aRanked by 1983 age-standardized mortality rate (ASMR), ages 25-75, per 100,000 population. s00o
400
.
3001
200-100 90
80
70
60
50
40
30
20-.
lfl lU .. ' '...
11.~~~~
.^·
e
a.
i;
0
1 q
rate of 35/100,000 could be achieved by 1986. The
reported 1983 rate of 27.5/100,000 is rapidly
approach-ing that prediction.
(Source: Walter Litven, Elen Smith and Patricia Milks, Non-Communicable Disease Division, Bureau of
Epidemiology, Health and Welfare Canada.)
Editorial Comment
The data presented underscore the importance of mortality statistics for the formulation and evaluation of health policies. They also serve as a reminder that gradual changes in mortality similar to those described for Canada can be expected over the medium and long term in the countries of Latin America and the Carib-bean, where health profiles are changing rapidly in the same direction.
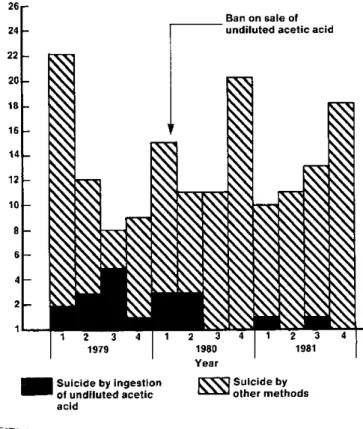
Health authorities in Suriname have maintained sur-veillance for suicide and have collected data for that cause of death since 1976. The number of deaths due to suicide by ingestion of agricultural insecticides and chemicals and other methods between 1976 and 1983 is shown in Table 1. Deaths due to the ingestion of the pesticide paraquat are also shown for 1980-1983. In recent years. a change has been observed in the methods used for suicide. Whereas before 1979 hang-ing and hang-ingestion of undiluted acetic acid were com-mon, the latter practically disappeared as a method of suicide after the Government banned the sale of undi-luted acetic acid. The impact of the ban can be seen
Table 1. Deaths by suicide due to poisoning and other methods in Suriname, from 1976 to 1983.
in Figure 1. However, various toxic substances and chemical pesticides are readily available in stores, and they are commonly found in homes and on small farms throughout the country. A secondary effect of the ready availability of agricultural pesticides has been the in-creasing use of these substances for suicide (Table 1). In 1978, only 11% of the total number of suicidal deaths were due to toxic agricultural compounds, and three of the four deaths reported were accidental. By
Figure 1. Number of suicides in Suriname per quarter year, 1979-1981.
26
24
22
20
18
16
14
12
Ingestion of toxic substances
Other insecticides Other Total number
Year Paraquat and chemicals methods of deaths
1976 0 5 28 33
1977 0 0 22 22
1978 0 4 32 36
1979 0 12 37 49
1980 12 5 41 58
1981 23 10 19 52
1982 35 0 29 64
1983 59a ... ...
'Reports from two hospitals. ... Data not available.
'Based on a presentation to the CAREC Epidemiologists Meeting in June 1984, by Dr. Wim Bakker, Chief, Epidemiology Unit, Ministry of Health, Suriname.
101-8
6
4
2
1
1979
Suicide by ingestic
of undiluted acetic acid
Ban on sale of undiluted acetic acid
1 2 3 4 1 2 3981
1980 1981
4
Year
Suicide by
M other methods
in