Original Article
Braz J Oral Sci.January | March 2014 - Volume 13, Number 1
Tooth erosion and dental caries in schoolchildren:
is there a relationship between them?
Mabel Miluska Suca Salas¹, Raquel Venâncio Fernandes Dantas¹, Hugo Ramalho Sarmento¹,
Fabiana Vargas-Ferreira², Dione Torriani¹, Flávio Fernando Demarco
1,2¹Universidade Federal de Pelotas - UFPel, Dental School, Departament of Restorative Dentistry, Pelotas, RS, Brasil ²Universidade Federal de Pelotas - UFPel, Dental School, Area of Epidemiology, Pelotas, RS, Brasil
Correspondence to:
Flávio Fernando Demarco Faculdade de Odontologia Universidade Federal de Pelotas Rua Gonçalves Chaves 457 CEP: 96015568 - Pelotas, RS, Brasil Phone: +55 53 3222 6690 E-mail: [email protected]
Abstract
Aim: To identify a possible association between the occurrence of dental caries and tooth erosion and to correlate the dietary factor with an increased risk of dental caries. Methods: A cross-sectional study in a multistage random sample of 1,211, 8 to 12-years-old Brazilian schoolchildren in private and public schools was conducted in Pelotas, Brazil. The prevalence of dental caries and tooth erosion was assessed. Dietary habits data were collected by a structured questionnaire. Data were analyzed using Poisson regression model taking into account the cluster sample (Prevalence ratio - PR; 95% Confidence Interval - CI). Results: The prevalence of dental caries and tooth erosion was 32.4% (95% CI: 30.0; 35.2) and 25.0% (95% CI: 23.4; 29.0), respectively. Most children had high consumption of sweets (65%). Consumption of fruits, such as oranges (31%), strawberries (23.6%), pineapple (12%), and natural fruit juices (oranges, lemon) was low. Soft drinks consumption, 3 or more times a week was observed in 40% of the children. Conclusions: Dental caries was not statistically associated with tooth erosion. The consumption of acidic fruits/drinks was not associated with dental caries. Dental caries and dental erosion were not associated with each other and with acidic fruits or drinks consumption.
Keywords: dental caries; tooth erosion; epidemiology; child; diet.
Introduction
Dental caries is the main oral disease affecting children and adolescents, particularly among underprivileged groups in the developed and developing countries1. Data from Brazil in 2010 show that 43.5% of 12-year-old children had
dental caries, with a mean DMFT (decayed, missed, filled teeth) of 2.072. Despite
the high prevalence of caries in children, there is a worldwide trend of caries reduction3, raising interest for other oral health problems, such as the increase of
tooth erosion, mainly in young individuals4.
Tooth erosion has been defined as a progressive loss of hard dental tissue due to a chemical process that does not involve bacteria5. It has the potential to
substantially impact on dentition, due to its cumulative and progressive nature6.
The prevalence of tooth erosion in Brazilian children (age 6 to 16 years old) ranged from 7.2 to 26 percent7-10.
It is well established that dietary habits play an important role in promoting and maintaining oral health among individuals. Dietary habits are important risk factor for dental caries11 and also main source of acids, contributing to the
development of tooth erosion10. It has been suggested that children with dental
caries may also be predisposed to tooth erosion12. Many types of food and soft
drinks are not only acidic but also contain high percentage of sugar13 and, therefore,
Received for publication: January 13, 2014
dental erosion and caries may occur simultaneously in the same individual, but on different tooth surfaces14-15.
However, this potential association remains unclear and contradictory, while some studies found an association between the two diseases, others did not find any association12,14,16. Variability between investigations regarding
localization and the studied population may influence the results14-15. We hypothesized that presence of caries is
associated with tooth erosion and diet.
The aim of this study was to test if dental caries occurrence may be associated with tooth erosion in Brazilian schoolchildren. Additionally, it was tested whether dietary habit patterns may increase the risk for dental caries.
Material and methods
Study population and design
In 2010, a cross-sectional study was performed in the city of Pelotas, RS, Brazil, using a multi-stage random representative sample of 8-12-year-old schoolchildren of the city. Pelotas is a middle-sized city of the southern region of Brazil, which has 328,275 inhabitants, nearly 85% residing in the urban area. More detailed information can be found elsewhere17.
For the sample calculation to assess the prevalence and association between dental caries and independent variables, the following parameters were used: caries prevalence of 39.3 percent18, a standard error of 4 %, a confidence interval (CI)
of 95% and power equal to 80%. A design effect of 1.4 9 was
considered and the sample size was increased by 20% for possible refusals or losses. The ratio of unexposed to exposed tooth erosion was 3:1 and the prevalence ratio to be detected was at least 1.6, and the minimum sample size to satisfy these requirements was 616 children. A two-stage random sampling procedure was adopted to select the sample. The first stage units were public and private schools of the city. Twenty schools were randomly selected. The second stage units were the classrooms. In each school, five classes, from 2nd to 6th grade, were randomly selected and all children
enrolled in these classes were initially eligible for the study. Subjects intellectually and physically able to answer the questionnaire were included in the study.
From the 1,744 children invited to participate, 1,211 children were enrolled in the study with a 70% response rate. Reasons for non-participation were mainly due to the lack of parental consent and absence on the examination day. The actual sample size was larger than the minimum size to satisfy the sample size requirements because this study was part of a major project including other outcomes that required a larger sample.
Data were collected with structured interviews and clinical oral examinations, and six calibrated dentists participated. The calibration included theoretical activities for the diagnostic criteria for dental caries (DMFT)19 and
tooth erosion20. To assess inter-examiner consistency for caries,
a calibration exercise was performed on 10 children that were not included in the final sample, which were re-examined
by the same examiners 2 weeks after the first examination. For tooth erosion, a range of different levels of erosion – based on the diagnosis of photographic images – was used in the calibration exercise (in lux), in agreement with the literature. For dental caries and tooth erosion, inter-examiner kappa values ranged from 0.68 to 0.90 and from 0.60 to 0.65, respectively.
Examinations were conducted in the classrooms, with children in a sitting position, under artificial light, using periodontal probes (CPI; “ball point”) and dental mirrors. Sterile gauze pads were used to clean and dry the tooth surfaces. Dental caries was assessed in all teeth, using the DMFT – decayed, missed, filled teeth index according to the
WHO recommendations19 which measure the lifetime
experience of tooth caries in permanent dentition. Tooth
erosion was assessed by the modified version8 of the
O´Sullivan index20 on maxillary incisors, by visual
examination of facial, lingual, and incisal surfaces20. For this
study, tooth erosion was dichotomized as present or not. The presence of one erosive lesion was considered “with tooth erosion”. Site of erosion, severity and affected tooth surface area were not analyzed.
A previously used questionnaire based on the literature7,9, was employed to investigate dietary habits (type
and frequency of consumption of acidic drinks, including non-diet/non-light and diet/light soft drinks, fruit and sweets). Data were completed in schoolroom before the clinical examination. Dietary foods and drinks consumption was initially recorded by three frequencies: never, 1 or 2 times and 3 times or more (during a week) and later dichotomized in two categories: low (never or 1-2 times a week consumption) and high (3 or more times a week consumption)9. This cut off was chosen because in Brazilian
children, the acidic uptake more than three times a week was observed to increase twice the chances for tooth erosion7. To
assess the applicability of the questionnaire, a pre-test was performed with 10 % of the study population before the survey, showing satisfactory levels of acceptability and ease of completion.
Data analyses were performed using STATA software 12.0 (Stata Corp., College Station, TX, USA). Descriptive and bivariate analyses were conducted to provide summary statistics and preliminary assessment of the association of predictor variables and the outcome (dental caries) was performed using the chi-square Pearson and Mann-Whitney test. Poisson regression model taking into account the cluster sample (prevalence ratio and 95 percent confidence interval) was performed to assess the association between the predictor variables and the outcome. A backward stepwise procedure was used to include or exclude explanatory variables in the fitting of models. Explanatory variables presenting a p-value < 0.20 in the assessment of correlation with each outcome (bivariate analyses) were included in the fitting of the model. Explanatory variables were selected for the final models only if they had a p-value < 0.05 after adjustment.
protocol n°160/2010) and informed consent was obtained prior of starting data collection.
Results
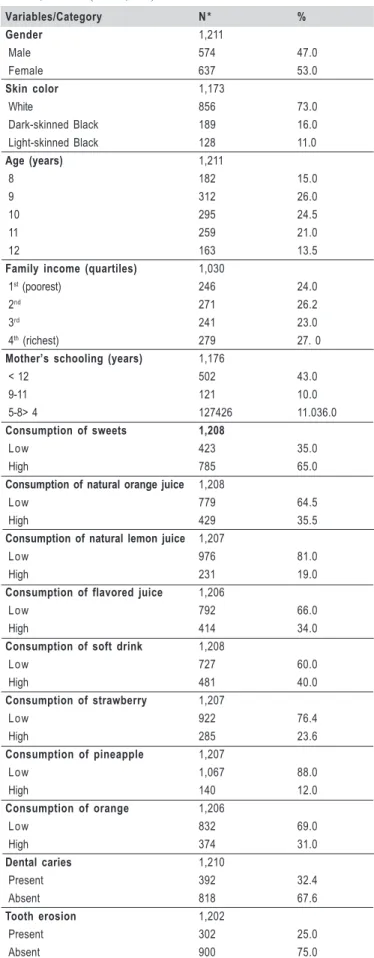
Demographic, socioeconomic, behavioral and clinical characteristics of the sample are presented in Table 1. There were 574 (47.4%) boys and 637 (52.6%) girls. Prevalence of dental caries and tooth erosion were 32.4% (95%CI 30.0; 35.2) and 25.0% (95%CI 23.4; 29.0) respectively. In relation to sweets consumption, a prevalence of 65% was found. For the 1,211 schoolchildren the DMFT index result was 0.64 (Standard Deviation ± 1.18). The mean DMFT index was not statistically different for children with tooth erosion 0.75 (± SD 1.35) compared with those without erosion 0.59 (±SD 1.11). In the preliminary assessment, the outcome (dental caries) was not associated with any dietary or clinical factors (tooth erosion) (Table 2). In the multivariate analysis, dental caries was not associated with dietary habits (PR:1.15; 95% CI: 0.97;1.35) (Table 3). Similarly, dental caries was not associated with tooth erosion (PR: 1.15; 95% CI: 0.96;1.37) (Table 3).
Discussion
In this study a prevalence of 32.4% of dental caries was found among 8- to 12-year-old children (95% CI: 30.0;35.0). This prevalence was lower than observed in other studies21,22.
A significant decrease in caries prevalence in Brazilian
children was observed in the last decades10,23. Some
longitudinal investigations indicated an increase of erosion incidence in children24-25. The prevalence found in this study
(25.0%) was higher than those observed in other Brazilian studies investigating mixed and/or permanent dentitions8-9.
Different indexes used or dietary habits between countries and regions may account for this variability. Younger children (aged 8 to 12 years) were included in the present study, turning the acidic contact with tooth structure as the main potential etiologic factor7.
In this study, 8.9% of children had caries and tooth erosion. However, the mean DMFT scores were not statistically different for children with tooth erosion (0.75) compared to those without erosion (0.59). Similar findings were observed in children aged 13-14 years in Brazil, England and Libya10,15,26. In a Brazilian study with adolescents, while
35% of them had dental caries and tooth erosion, 32% without caries had also tooth erosion, and no association was detected between the two outcomes10. In Australia,
children who had caries were more likely to have severe tooth erosion in both dentitions12. In an English cohort, tooth
erosion was associated with dental caries and with high consumption of carbonated drinks at age 1216. In Saudi
Arabia, direct relationship between tooth erosion and dental caries was observed, suggesting that the carious process could be a potential risk factor for tooth erosion, with possible common risk factors14. Children may fail to maintain a
non-cariogenic diet, which could also be a potentially erosive
Variables/Category N * %
Gender 1,211
Male 574 47.0 Female 637 53.0
Skin color 1,173
White 856 73.0 Dark-skinned Black 189 16.0 Light-skinned Black 128 11.0
Age (years) 1,211
8 182 15.0
9 312 26.0
10 295 24.5
11 259 21.0
12 163 13.5
Family income (quartiles) 1,030
1st (poorest) 246 24.0
2nd 271 26.2
3rd 241 23.0
4th (richest) 279 27. 0
Mother’s schooling (years) 1,176
< 12 502 43.0 9-11 121 10.0 5-8> 4 127426 11.036.0
Consumption of sweets 1,208
Low 423 35.0
High 785 65.0
Consumption of natural orange juice 1,208
Low 779 64.5
High 429 35.5
Consumption of natural lemon juice 1,207
Low 976 81.0
High 231 19.0
Consumption of flavored juice 1,206
Low 792 66.0
High 414 34.0
Consumption of soft drink 1,208
Low 727 60.0
High 481 40.0
Consumption of strawberry 1,207
Low 922 76.4
High 285 23.6
Consumption of pineapple 1,207
Low 1,067 88.0 High 140 12.0
Consumption of orange 1,206
Low 832 69.0
High 374 31.0
Dental caries 1,210
Present 392 32.4 Absent 818 67.6
Tooth erosion 1,202
Present 302 25.0 Absent 900 75.0
Table 1- Table 1- Table 1- Table 1-
Table 1- Clinical, demographic, behavioral and socioeconomic characteristics of the sample. Pelotas, Southern Brazil, 2010. (N=1,211)
Dental caries p value*
Tooth erosion 0.117
Without 622 278
With 194 108
Natural orange juice 0.439
Low 532 246
High 284 145
Natural lemon juice 0.627
Low 662 313
High 153 78
Flavored fruit juices 0.342
Low 527 264
High 287 127
Soft drinks 0.116
Low 504 223
High 312 168
Strawberry 0.904
Low 624 297
High 192 93
Pineapple 0.889
Low 722 344
High 94 46
Orange 0.541
Low 568 264
High 248 125
Sweets 0.922
Low 82 40
High 734 351
* Chi-squared (÷²) test
Table 2 – Table 2 –Table 2 – Table 2 –
Table 2 – Prevalence of dental caries and associated factors, Pelotas, Southern Brazil, 2010. (N=1,211)
diet15. Higher levels of mutans streptococci were found in
children at risk of tooth erosion27. The loss of protective
factors, such as saliva, may place the children at risk for both diseases12.
Tooth erosion and caries have a multifactorial etiology5.
The acids responsible for erosion are not produced by the oral biofilm, but derived from dietary intrinsic acids or occupational sources5. On the opposite, caries development
relies on the acids produced by the oral biofilm. Studies have shown an association between tooth erosion, dental caries and dietary habits14,16. In the present study it was
assessed the type and frequency of consumption of acidic food and drinks. These variables were not statistically associated with caries, in agreement with another previously reported investigation10. This result could be attributed to the
frequency of consumption of acidic diet. Frequent consumptions, more than 3 times a day, increased the risk for both oral conditions 1.5 times16. The increased consumption
of beverages and foods, containing high percentage of sugar and acidic products rises concerns for their impact on general health, especially in children and adolescents, being associated with cardiopathy, diabetes and obesity12.
It should be highlighted that the process and site specificity are different for both conditions. In general, the surfaces more prone to erosion are not those where caries occurs26 and tooth erosion is often located in plaque-free
areas, in opposition to dental caries, which is located in plaque accumulation sites5. Dental caries and tooth erosion
can occur independently. The association between them may not always be found, and in some cases, the rapid and destructive nature of caries may force removal of the clinical evidence of erosion5.
The lack of association between dental caries, tooth erosion and dietary habits may be due to the influence of other factors, such as quantity and composition of saliva, tooth composition and structure, oral hygiene practices and medical conditions4,7,10. Moreover, tooth erosion has been
mostly studied in populations where the prevalence of dental caries is low and the association may be more difficult to demonstrate14. Studies have focused on dietary habits because
there is a possible connection between the two conditions by one common item, sugary and acidic “soft drinks”14.
To have a better understanding of dietary consumption, for both oral conditions, one possibility is to evaluate the diet for 3 days at least6,14. This could not be done in the
present study together other oral and systemic health outcomes because it was carried out in schools making it difficult to include extensive questionnaires or successive visits were investigated.
The reliability of self-reporting dietary habits by the schoolchildren may be an other limitation, as there is possibility of under- or over-reporting10. Unfortunately, there is no
standardized questionnaire for tooth erosion in epidemiological surveys and this may be associated to those findings9.
The obtained data must be considered with caution. The findings are limited by the cross-sectional nature of data collection. This study design cannot show the temporal effect27
of the diet on the development of caries and/or tooth erosion. Dental caries and tooth erosion may not occur together in some point of the time. The severity of tooth caries and tooth erosion could make the presence of both conditions in the same individual more or less obvious. In permanent teeth, superimposition of a greater and more rapid destruction of caries could mask or remove any evidence of erosion14.
Further investigations with longitudinal designs using the life course epidemiology approach28 are required to
confirm these findings and to clarify the association between dental caries and tooth erosion.
With Dental caries
Variables PRc (95%CI) p value* PRadj(95%CI) p value*
Tooth erosion 0.111 0.130
Without 1.00 1.00
With 1.16 (0.97;1.39) 1.15 (0.96;1.37)
Soft drinks 0.114 0.101
Low 1.00 1.00
High 1.14 (0.97;1.34) 1.15 (0.97;1.35)
Table 3 – Table 3 – Table 3 – Table 3 –
Table 3 – Prevalence of dental caries and associated factors (Prevalence Ratio: 95% CI), Pelotas, Southern Brazil, 2010. (N=1,211)
*Wald test; PRc = Crude prevalence ratio; PR adj. = Adjusted prevalence ratio;
It has been shown that dental caries is suffering a phenomenon called polarization, with most of the disease concentrated in a small part of the population, especially those more deprived. Therefore, the investigation of factors that could be associated with caries occurrence should be investigated in epidemiological surveys in order to establish preventive measures29.
In the present study, there was no statistically significant association between dental caries and tooth erosion in Brazilian schoolchildren. Dietary habits were not associated with all dental caries.
Acknowledgments
The authors are grateful to the State secretary of Education, the Municipal Secretary of Education and the Direction of Private Schools, which allowed the study to be performed. Also, the authors would like to thank Brazilian National Council for Scientific and Technological Development (CNPq) for the research grant (process #402350/ 2008-1 and 579996/2008-5) provided to the Principal Investigator (FFD). Also, the authors would like to thank the TWAS (the world academy of sciences for the advancement of science in developing countries - Process # 190268/2010-7) for the scholarship provided to the first author (MMSS).
References
1. Traebert J, Guimaraes L do A, Durante EZ, Serratine AC. Low maternal
schooling and severity of dental caries in Brazilian preschool children. Oral Health Prev Dent. 2009; 7: 39-45.
2. Freire MCM, Reis SCGB, Figueiredo N, Peres KG, Moreira RS, Antunes
JLF. Individual and contextual determinants of dental caries in Brazilian 12-year-olds in 2010. Rev. Saude Publica 2013; 47:40-9.
3. Whelton H. Overview of the impact of changing global patterns of dental
caries experience on caries clinical trials. J Dent Res. 2004; 83 Spec No C: C29-34.
4. Truin GJ, van Rijkom HM, Mulder J, van’t Hof MA. Caries trends
1996-2002 among 6- and 12-year-old children and erosive wear prevalence among 12-year-old children in The Hague. Caries Res. 2005; 39: 2-8.
5. Taji S, Seow WK. A literature review of dental erosion in children. Aust
Dent J. 2010; 55: 358-67.
6. Okunseri C, Okunseri E, Gonzalez C, Visotcky A, Szabo A. Erosive
tooth wear and consumption of beverages among children in the United States. Caries Res. 2011; 45: 130-5.
7. Correr GM, Alonso RC, Correa MA, Campos EA, Baratto-Filho F,
Puppin-Rontani RM. Influence of diet and salivary characteristics on the prevalence of dental erosion among 12-year-old schoolchildren. J Dent Child. (Chic) 2009; 76: 181-7.
8. Peres KG, Armenio MF, Peres MA, Traebert J, De Lacerda JT. Dental
erosion in 12-year-old schoolchildren: a cross-sectional study in Southern Brazil. Int J Paediatr Dent. 2005; 15: 249-55.
9. Vargas-Ferreira F, Praetzel JR, Ardenghi TM. Prevalence of tooth erosion
and associated factors in 11-14-year-old Brazilian schoolchildren. J Public Health Dent. 2011; 71: 6-12.
10. Auad SM, Waterhouse PJ, Nunn JH, Moynihan PJ. Dental caries and its association with sociodemographics, erosion, and diet in schoolchildren from southeast Brazil. Pediatr Dent. 2009; 31: 229-35.
11. Perera I, Ekanayake L. Relationship between dietary patterns and dental
caries in Sri Lankan adolescents. Oral Health Prev Dent. 2007; 8: 165-72. 12. Kazoullis S, Seow WK, Holcombe T, Newman B, Ford D. Common dental conditions associated with dental erosion in schoolchildren in Australia. Pediatr Dent. 2007; 29: 33-9.
13. Yip HH, Wong RW, Hagg U. Complications of orthodontic treatment: are soft drinks a risk factor? World J Orthod. 2009; 10: 33-40.
14. Al-Malik MI, Holt RD, Bedi R. The relationship between erosion, caries and rampant caries and dietary habits in preschool children in Saudi Arabia. Int J Paediatr Dent. 2001; 11: 430-9.
15. Huew R, Waterhouse P, Moynihan P, Kometa S, Maguire A. Dental caries and its association with diet and dental erosion in Libyan schoolchildren. Int J Paediatr Dent. 2012; 22: 68-76.
16. Dugmore CR, Rock WP. A multifactorial analysis of factors associated with dental erosion. Br Dent J. 2004; 196: 283-6.
17. Goettems ML, Correa MB, Vargas-Ferreira F, Torriani DD, Marques M, Domingues MR,et al. Methods and logistics of a multidisciplinary survey of schoolchildren from Pelotas, in the Southern Region of Brazil. Cad Saude Publica. 2013; 29: 867-78.
18. Piovesan C, Antunes JL, Guedes RS, Ardenghi TM. Impact of socioeconomic and clinical factors on child oral health-related quality of life (COHRQoL). Qual Life Res. 2010; 19: 1359-66.
19. World Health Organization. Oral Health Survey: basic methods. Genebra: WHO; 1997.
20. O’Sullivan EA. A new index for the measurement of erosion in children. Eur J Paediat Dent. 2000; 2: 69-74.
21. Eslamipour F, Borzabadi-Farahani A, Asgari I. The relationship between aging and oral health inequalities assessed by the DMFT index. Eur J Paediatr Dent. 2011; 11: 193-9.
22. Peres MA, Barros AJ, Peres KG, Araujo CL, Menezes AM. Life course dental caries determinants and predictors in children aged 12 years: a population-based birth cohort. Community Dent Oral Epidemiol 2009; 37: 123-33.
23. Pereira SM, Tagliaferro EP, Ambrosano GM, Cortelazzi KL, Meneghim M de C, Pereira AC. Dental caries in 12-year-old schoolchildren and its relationship with socioeconomic and behavioural variables. Oral Health Prev Dent. 2007; 5: 299-306.
24. El Aidi H, Bronkhorst EM, Huysmans MC, Truin GJ. Multifactorial analysis
of factors associated with the incidence and progression of erosive tooth wear. Caries Res. 2011; 45: 303-12.
25. Nunn JH, Gordon PH, Morris AJ, Pine CM, Walker A. Dental erosion —
changing prevalence? A review of British National childrens’ surveys. Int J Paediatr Dent. 2003; 13: 98-105.
26. Bardolia P, Burnside G, Ashcroft A, Milosevic A, Goodfellow SA, Rolfe
EA, et al. Prevalence and risk indicators of erosion in thirteen- to fourteen-year-olds on the Isle of Man. Caries Res. 2010; 44: 165-8.
27. Linnett V, Seow WK. Dental erosion in children: a literature review. Pediatr
Dent. 2001; 23 : 37-43.