ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Association
between
academic
performance
and
cognitive
dysfunction
in
patients
with
juvenile
systemic
lupus
erythematosus
Renan
Bazuco
Frittoli
a,
Karina
de
Oliveira
Pelic¸ari
a,
Bruna
Siqueira
Bellini
a,
Roberto
Marini
b,
Paula
Teixeira
Fernandes
c,
Simone
Appenzeller
b,d,∗aRheumatologyLaboratory,FaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil
bDepartmentofPediatrics,PediatricRheumatologyUnit,FaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas
(Unicamp),Campinas,SP,Brazil
cDepartmentofSportsSciences,FaculdadedeEducac¸ãoFísica,UniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil
dDepartmentofMedicine,RheumatologyUnit,FaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas(Unicamp),
Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1September2015 Accepted12January2016 Availableonline18April2016
Keywords:
Juvenilesystemiclupus erythematosus Cognitivedysfunction Academicperformance
a
b
s
t
r
a
c
t
Objective:Todeterminewhetherthereisanassociationbetweentheprofileofcognitive dys-functionandacademicoutcomesinpatientswithjuvenilesystemiclupuserythematosus (JSLE).
Methods:Patientsaged≤18yearsattheonsetofthediseaseandeducationlevelatorabove thefifthgradeofelementaryschoolwereselected.Cognitiveevaluationwasperformed accordingtotheAmericanCollegeofRheumatology(ACR)recommendations.Symptoms ofanxietyanddepressionwereassessedbyBeckscales;diseaseactivitywasassessedby SystemicLupusErythematosusDiseaseActivityIndex(SLEDAI);andcumulativedamage wasassessedbySystemicLupusInternationalCollaboratingClinics(SLICC).Thepresence ofautoantibodiesandmedicationusewerealsoassessed.Asignificancelevelof5%(p<0.05) wasadopted.
Results:41patientswithameanageof14.5±2.84yearswereincluded.Cognitivedysfunction wasnotedin17(41.46%)patients.Therewasasignificantworseninginmathematical perfor-manceinpatientswithcognitivedysfunction(p=0.039).Anxietysymptomswereobserved in8patients(19.51%)andwereassociatedwithvisualperception(p=0.037)andsymptoms ofdepressionwereobservedin1patient(2.43%).
Conclusion:PatientswithJSLEconcomitantlywithcognitivedysfunctionshowedworse aca-demicperformanceinmathematicscomparedtopatientswithoutcognitiveimpairment.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](S.Appenzeller).
http://dx.doi.org/10.1016/j.rbre.2016.03.005
Associac¸ão
entre
desempenho
acadêmico
e
disfunc¸ão
cognitiva
em
pacientes
com
lúpus
eritematoso
sistêmico
juvenil
Palavras-chave:
Lúpuseritematososistêmico juvenil
Disfunc¸ãocognitiva Desempenhoacadêmico
r
e
s
u
m
o
Objetivo: Determinarseháassociac¸ãoentreoperfildedisfunc¸ãocognitivaeosresultados acadêmicosempacientescomlúpuseritematososistêmicojuvenil(LESj).
Métodos: Foramselecionadospacientescomidadedeiníciodadoenc¸a≤18anosecom escolaridade mínima doquinto anodoEnsino Fundamentalseguidosem um hospital universitário.Aavaliac¸ãocognitivafoifeitadeacordocomasrecomendac¸õesdoColégio AmericanodeReumatologia(ACR).Ossintomasdeansiedadeedepressãoforamavaliados pelasescalasBeck,aatividadedadoenc¸afoiavaliadapeloSystemicLupusErythematosus DiseaseActivityIndex(Sledai)eodanocumulativopeloSystemicLupusInternational Col-laboratingClinics(Slicc).Tambémforamavaliadosapresenc¸adeautoanticorposeousode medicac¸ão.Adotou-seníveldesignificânciade5%(p<0,05).
Resultados: Foramincluídos41pacientescommédiade14,5±2,84anos.Disfunc¸ão cog-nitivafoiobservadaem 17(41,46%).Observou-sepioriasignificativanodesempenhode matemáticaempacientescomdisfunc¸ãocognitiva(p=0,039).Sintomasdeansiedadeforam observadosemoitopacientes(19,51%)eestavamassociadosàpercepc¸ãovisual(p=0,037)e sintomasdedepressãoforamobservadosemumpaciente(2,43%).
Conclusão: Pacientescom LESjcom disfunc¸ão cognitivaapresentam pior desempenho acadêmicoemmatemáticaemrelac¸ãoapacientessemdisfunc¸ãocognitiva.
©2016ElsevierEditoraLtda.EsteéumartigoOpenAccesssobalicençadeCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Systemiclupuserythematosus(SLE)isachronicand autoim-muneinflammatorydiseaseofconnectivetissue.Ofunknown etiology,SLEislinkedtogenetic,hormonal, environmental factors,and tothe use ofsome medications.This disease mostlyaffectswomeninchildbearingage,especiallybetween 15and50years.However,approximately20%ofpatientsare affected duringchildhoodor adolescence(JSLE), being pre-dominantlyoffemalegender.1–3
JSLE patients show a more severe form of the disease anddevelopneuropsychiatricsymptomsathigher frequen-ciesthaninadultpatients.4Cognitivedisordersarecommon
andaffectmainlyattention,concentration,learning,memory, informationprocessingandexecutivefunctions,eveninthe apparentabsenceofdiseaseactivityorofother neuropsychi-atricevents.5–8
Fewstudies available inthe literaturesuggest that JSLE patientsareatriskofpooracademicperformance,9,10
espe-cially causing difficulties in arithmetic learning, reading comprehension,visualmemory andinability tosolve com-plexproblems.10Forthesereasons,patientswithSLEcanmeet
fewereducationalmilestones,forexample,notfinishinghigh schoolorcollegegraduation–factorsassociatedwithalower probabilityofemploymentandofsuccessatwork.10–12Inthis
scenario,theaimofthisstudywastodeterminewhetherthere isanassociationbetweentheprofileofcognitivedysfunction andacademicoutcomesinpatientswithJSLE.
Materials
and
methods
ConsecutivepatientswithJSLEseenatthePediatric Rheuma-tologyOutpatientClinic,HospitaldasClínicas,Universidade
Estadual de Campinas (UNICAMP), whose clinical and lab-oratory manifestationswere routinely studied accordingto analreadyestablishedprotocol,wereselected.13,14Inclusion
criteriawere:patientswithageofonsetofdisease≤18,15and
withfifthgradeofelementaryschoolastheminimumlevelof scholarship.ThestudywasapprovedbytheResearchEthics Committee(CEPNo.920/2007)ofUNICAMPandallthe partic-ipantsandlegalguardianssignedaninformedconsentform (FICF).
Cognitive assessment was performed by a qualified psychologist through the application of a survey battery lasting about two hours, consisting of tests adapted to the juvenile population and validated for the Portuguese language and selected from the battery recommended by the American College of Rheumatology (ACR).16 The
fol-lowing tests for evaluation of cognitive functions were selected:
• Picture Arrangement Test: evaluates temporal reasoning17,18
• CodeTest:evaluatesprocessingspeed17,18
• PictureCompletionTest:evaluatesvisualperception17,18
• CubeTest:evaluatesspatialreasoning17,18
• DigitTest:assessesimmediateandworkingmemory17,18
• VocabularyTest:evaluatessemanticmemory,educational backgroundandgeneralintelligence17,18
• ReyComplexFigureTest:evaluatesperceptualorganization, planning,praxisandmemory19
• BostonNamingTest:evaluatesvisualrecognitionand nam-ingcapacity20
• FAZ Verbal Fluency Test: assesses verbal-phonological fluency21
• StroopNeuropsychologicalScreeningTest:evaluates selec-tiveattention,inhibitorycontrolandmentalflexibility23
Eachpatienthadhis/herscorescountedindividually. Seventy-onecontrolsmatchedforgender,ageand socio-economicstatuswereincludedinordertoobtainnormative dataofappliedtests.Presenceofcognitiveimpairmenthas beendefinedincasesofcognitivefunctionwithameanZ -score≤−2SDortwoormorefunctionswithameanZ-score between−1and−2SD.24
Onthedayofthecognitivetests,theschoolreportofthe lastacademicsemesterofeachparticipantwasrequested.The participantsweregroupedbydiscipline:Portuguese/English/ Spanish; Geography/History; Physical/Chemical/Biological Sciences; Mathematics;Physical Education; Arts; and Soci-ology/Philosophy. School grades ≥7 (70% success) were consideredassatisfactory.24–28
DiseaseactivitywasassessedbytheSystemicLupus Ery-thematosusDiseaseActivityIndex(SLEDAI)questionnaireand thediseasewasconsideredactiveifthesumofSLEDAIpoints was>3.29Cumulativedamagewasassessedbytheapplication
ofaquestionnairespecificallydevelopedforthispurpose,the SystemicLupusInternationalCollaboratingClinics/American College of Rheumatology Damage Index (SDI) (SLICC/ACR-DI).30
Toassessthepresenceofdepressivesymptoms,the Chil-dren’sDepressionInventory–CDI31 forsubjects between7
and 17 years32 was applied; this tool is an adaptation of
theBDI(BeckDepressionInventory).Anxietysymptomswere assessedusingtheBeckAnxietyInventory–BAI.33,34
Lab work-up ofautoantibodies was carried out; routine techniquesusedintheClinicalPathologyLaboratoryandin theAllergyand ImmunologyResearchLaboratoryat Hospi-taldas Clínicas,UNICAMP wereused.Antinuclear antibody (ANA)(byindirectimmunofluorescence;positiveiftitle>1:40); anti-DNA antibody (by indirect immunofluorescence with
Crithidialuciliaeassubstrate)35;anti-Smithantibody(by
dou-ble immunodiffusion); anticardiolipin antibody (by enzyme immunoassay);andlupusanticoagulant(by TTPAand Rus-sell method) were determined.36 Anti-ribosomal P protein
antibody(anti-P)wasmeasuredbyEnzymeLinkedImmuno SorbentAssay(ELISA).
Medicationsprescribedonthedateofthecognitivetests were taken into account in this study. The drugs were corticosteroids, anti-malarials (chloroquine and hydroxy-chloroquine),andotherimmunosuppressivedrugs (azathio-prine, cyclophosphamide, cyclosporine, methotrexate and mycophenolatemofetil).
StatisticalanalysiswasperformedusingtheStatisticaland GraphicalSoftware(Systat)program.Shapiro–Wilknormality test was applied forobtaining results. For statistical anal-ysis, nonparametric Kruskal–Wallis and Fisher’s exact test were performed. The significance level was set at5%, i.e.,
p<0.05.
Results
Forty-onepatientswithJSLE(meanage,14.5±2.84years),of whom38(92.68%)werefemales,wereincludedandassessed
Table1–Demographic,clinicalandimmunologicaldata ofjuvenilesystemiclupuserythematosuspatientswith andwithoutcognitiveimpairment.
Variables Patientswith cognitive dysfunction
n=17
Patients without cognitive dysfunction
n=24
p-Value
Female 17(100%) 21(87.5%) 0.128
Ageat diagnosis (mean/SD) 11.47years (2.47) 13.37years (3.53) 0.038a Disease duration (mean/SD)
5.11years(4.21) 7.58years(4.93) 0.102
Active disease 5patients (29.41%) 6patients (28.57%) 0.756 Cumulative damage 3patients (17.64%) 5patients (20.83%) 0.75
Anxiety 5patients
(29.41%)
3patients (12.5%)
0.241
Depression 1patient (5.88%)
0patient(0%) 0.235
Anti-P 5patients
(29.41%)
3patients (12.5%)
0.589
ANA 17patients
(100%)
18patients (75%)
0.033a
Anti-DNA 10patients (58.82%)
16patients (66.66%)
0.745
Anti-Smith 7patients (41.17%)
7patients (29.17%)
0.430
Anticardiolipin 6patients (35.29%) 5patients (20.83%) 0.476 Lupus antico-agulant 6patients (35.29%) 13patients (54.16%) 0.342
a p<0.05.
forcognitiveimpairmentandacademicnotes.Twenty-three (56.09%)patientswereelementaryeducationlevelstudents, three(7.31%)hadcompletedelementaryschoolanddidnot continuetheirstudies,and15(36.58%)werehighschool stu-dents.Themeanageofonsetofthediseasewas12.58±3.24 years;andthediseaseduration,untilthetimeoftesting,was 2.4±2.63years.Eleven(26.82%)patientshadactivediseaseat thetimeoftesting(meanofSLEDAI,7.27±2.62).
Thecontrolgroupwascomposedof71healthyvolunteers (90.14%women)withmeanageof16.37±5.21years.No sta-tisticallysignificantdifferenceswerefoundbetweenpatients and controlsregardinggenderand age,and socioeconomic status. According to the criteria adopted forthe definition ofcognitivedysfunction,17(41.46%)patientsand26(36.6%) controlshadcognitiveimpairment(p=0.08).
JSLEpatientsweredivided intotwosubgroupsaccording tothe presenceor absenceofcognitivedysfunction.Itwas observedthatthepresenceofcognitiveimpairmentwas asso-ciatedwithyoungerageatdiagnosisofJSLE(p=0.038)andan associationbetweencognitiveimpairmentandANA(p=0.033) wasnoted.Demographic,clinicalandimmunologicaldataare listedinTable1.
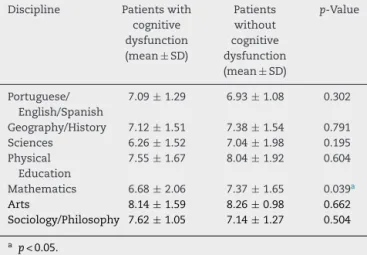
Table2–Schoolgradesbetweenpatientswithjuvenile systemiclupuserythematosuswithandwithout cognitiveimpairment.
Discipline Patientswith cognitive dysfunction (mean±SD)
Patients without cognitive dysfunction (mean±SD)
p-Value
Portuguese/ English/Spanish
7.09±1.29 6.93±1.08 0.302
Geography/History 7.12±1.51 7.38±1.54 0.791 Sciences 6.26±1.52 7.04±1.98 0.195 Physical
Education
7.55±1.67 8.04±1.92 0.604
Mathematics 6.68±2.06 7.37±1.65 0.039a
Arts 8.14±1.59 8.26±0.98 0.662
Sociology/Philosophy 7.62±1.05 7.14±1.27 0.504
a p<0.05.
ofcognitiveimpairment(p=0.988).Symptomsofdepression wereobserved in1(2.43%)patient andagain therewasno associationwithcognitiveimpairment(p=1.0).Noassociation wasobservedbetweensymptomsofanxietyanddepression, whencomparedwithacademicgrades.
Noassociationofcognitiveimpairmentwithany medica-tion(corticosteroids,p=0.988;immunosuppressants,p=0.75 andantimalarials,p=0.988)wasobserved.
Whencomparingpatientswithversuswithoutcognitive impairment,school performanceshowed significant differ-encebetweengroupsonlyformathgrades(p=0.039)(Table2).
Discussion
Inour sample,the frequency ofcognitive dysfunctionwas 41.46%;thisfindingwasconsistentwithotherstudiesreported intheliterature.4,6,8,24
Thepresenceofcognitiveimpairmentwasassociatedwith poorerperformanceinmathematicsinourpatients.Another study found that children with JSLE had poorer academic results versus individuals without this disease.9 It is
sug-gested thatdeficits in language abilityare amongthe first markers of presence of neurological disorder in patients with JSLE,and that this difficulty may be present even in patients without neuropsychiatric manifestations.6 In this
study,therewasnosignificantdifferenceinlanguage-related disciplines.
Itis a very difficult taskto define school performance, in the face of the multiple variables used to assess this phenomenon.25 Unsatisfactoryperformancewasdefinedby
McCallastheperformanceofanindividualwhodoesnot nec-essarilyobtainlowgrades,butwhosegradesarebelowhis/her expectations.26Thereisgreaterconsensusinconsideringas
unsatisfactory a performance substantially below expecta-tionsforthestudent’sowncognitiveability.25,26
Itisalsodifficulttoassessschoolperformance,sincethis parameter dependson differentfactors, amongwhich are: schoolphysicalcharacteristics,teacherqualifications, educa-tionlevelofparents,andeducationlevelofthestudent.28In
theliterature,severalmeasuresareavailableforevaluationof
schoolperformance,including:graderepetition,suspension, gradeslowerthantheexpectedforthestudent’scoefficientof intelligence,andlowgrades.37Inourstudy,inthedefinition
ofpoorschoolperformanceweconsideredtheoccurrenceof unsatisfactorynotes,i.e.educationalachievement<70%fora certainclasscontent.25–28
Itisknownthatcognitivedysfunctionisassociatedwith high morbidity in patients withJSLE.5,12 However,a major
obstacletounderstandingtheneuropsychological function-ingofthesepatientsisthelackofastandardizedcriterionfor theidentificationofthisdysfunction.8,24
The cognitive impairment evaluation consisted oftools adaptedtojuvenileagegroupandselectedfromthebattery suggestedbyACR16 forevaluationofcognitive dysfunction
inadults,and alsowithbatteriesusedinrecent studiesin patientswithJSLE.4,6,8,9,24
Inthisstudy,wefoundnoevidencethatdiseaseactivity playsaroleincognitive function.Thisfindingissupported by two recently published pediatric studies, in which the authors foundno association betweendisease activity and cognitivedysfunction.4,8Ontheotherhand,whenindividuals
withmoresevereconditions,e.g.,hospitalizedpatients,were included, wecouldobserveanassociation betweendisease activityandcognitivedysfunction.12
Other authors found no association between cognitive deficitandcumulativedamage38ormedication,39whichwas
confirmedinourstudy.
Inchildren,reportsofanassociationofautoantibodieswith cognitiveimpairmentaresparseandinconclusive;moreover, such studies alsodid notidentify intheir sample adirect associationbetweenthepresenceofantibodiesandcognitive dysfunction.4,8However,inourstudywefoundanassociation
withANAandcognitiveimpairment,suggestingthatthereis alinkbetweenautoimmunityandcognitivefunctioning.
Itisknownthatlivingwithachronicdiseasecancause majoradaptiveproblemsassociatedwithemotionaldistress, suchasirritability,insomnia,lossofappetite,emotional insta-bility,andchangesinmemoryandconcentration,whichmay be reflected in school performance.27,28,40 For this reason,
someauthorspointout behaviordifficultiesasariskfactor forpooracademicperformanceofindividualswithJSLE.8,11,41
Behaviordifficulties,althoughbeingavariablenotevaluated inthisstudy,areimportantinpatientswithchronicdisease, especiallyinadolescents;thesefactorsmayhavehadsome bearingontheresults.
Althoughcognitivedisorderfrequencyhasbeencompared againsthealthyindividuals,unfortunatelywedidnotcompute theacademicperformanceofthesecontrolsforcomparison.
Inconclusion,patientssufferingfromJSLEandwith cog-nitiveimpairmentexhibitaworseacademicperformancein math, comparedtoJSLE patientswithout cognitive impair-ment.
Funding
2009-4 and 471343/2011-0 and 302205/2012-8; and CNPq 473328/2013-5,466715/2014-5).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. PapadimitrakiED,IsenbergDA.Childhood-andadult-onset lupus:anupdateofsimilaritiesanddifferences.ExpertRev ClinImmunol.2009;5:391–403.
2. MinaR,BrunnerHI.Pediatriclupus–aretheredifferencesin presentation,genetics,responsetotherapy,anddamage accrualcomparedwithadultlupus?RheumDisClinNorth Am.2010;36:53–80.
3. vonSchevenE,BakkalogluA.What’snewinpediatricSLE. BestPractResClinRheumatol.2009;23:699–708.
4. MuscalE,BreyRL.Neurologicmanifestationsofsystemic lupuserythematosusinchildrenandadult.NeurolClin. 2010;28:61–73.
5. BenselerSM,SilvermanED.Neuropsychiatricinvolvementin pediatricsystemiclupuserythematosus.Lupus.
2007;16:564–71.
6. DiFrancescoMW,HollandSK,RisMD,AdlerCM,NelsonS, DelbelloMP,etal.Functionalmagneticresonanceimagining assessmentofcognitivefunctioninchildhood-onset systemiclupuserytrhematosus:apilotstudy.Arthritis Rheum.2007;56:4151–63.
7. LevyDM,ArdoinSF,SchanbergLE.Neurocognitive
impairmentinchildrenanadolescentswithsystemiclupus erythematosus.NatClinPractRheumatol.2009;5:106–14.
8. WilliamsTS,AranowC,RossGS,BarsdorfA,ImundoLF, EichenfieldAH,etal.Neurocognitiveimpairmentin childhood-onsetsystemiclupuserythematosus: measurementissuesindiagnosis.ArthritisCareRes (Hoboken).2011;63:1178–87.
9. ZelkoF,BeebeD,BakerA,NelsonSM,AliA,CedenoA,etal. Academicoutcomesinchildhood-onsetsystemiclupus erythematosus.ArthritisCareRes(Hoboken).2012;64:1167–74.
10.MoorthyLN,PetersonMG,HassettA,BaratelliM,LehmanTJ. Impactoflupusonschoolattendanceandperformance. Lupus.2010;19:620–7.
11.WyckoffPM,MillerLC,TuckerLB,SchallerJG.
Neuropsychologicalassessmentofchildrenandadolescents withsystemiclupuserythematosus.Lupus.1995;4:217–20.
12.SibbittWLJr,BrandtJR,JohnsonCR,MaldonadoME,PatelSR, FordCC,etal.Theincidenceandprevalenceof
neuropsychiatricsyndromesinpediatriconsetsystemic lupuserythematosus.JRheumatol.2002;29:1536–42.
13.TanEM,CohenAS,FriesJF,MasiAT,McShaneDJ,RothfieldNF, etal.The1982revisedcriteriafortheclassificationof systemiclupuserythematosus.ArthritisRheum. 1982;25:1271–7.
14.HochbergMC.UpdatingtheAmericanCollegeof Rheumatologyrevisedcriteriafortheclassificationof systemiclupuserythematosus.ArthritisRheum. 1997;40:1725.
15.SilvaCA,AvcinT,BrunnerHI.Taxonomyforsystemiclupus erythematosuswithonsetbeforeadulthood.ArthritisCare Res(Hoboken).2012;64:1787–93.
16.ACRAdHocCommitteeofNeuropsychiatricLupus Nomenclature.TheAmericanCollegeofRheumatology nomenclatureandcasedefinitionsforneuropsychiatriclupus syndromes.ArthritisRheum.1999;42:599–608.
17.FigueiredoVLM.WISC-III.EscaladeInteligênciaWechsler paracrianc¸as:manual/DavidWechsler.3ed:Adaptac¸ãoe Padronizac¸ãodeumaamostrabrasileira.1ed.SãoPaulo: CasadoPsicólogo;2002.
18.NascimentoE.WAIS-III.EscaladeInteligênciaWechslerpara adultos:manual/DavidWechsler:Adaptac¸ãoepadronizac¸ão deumaamostrabrasileira.1ed.SãoPaulo:CasadoPsicólogo; 2004.
19.OliveiraM.FigurascomplexasdeRey–Testedecópiae reproduc¸ãodememóriadefigurasgeométricascomplexas: adaptac¸ãobrasileira.SãoPaulo:CasadoPsicólogo;1999.
20.MorrisJC,HeymanA,MohsRC,TheConsortiumtoEstablisha RegistryforAlzheimer’sDisease(Cerad).PartI–Clinicaland neuropsychologicalassessmentofAlzheimer’sdisease. Neurology.1989;39:1159–65.
21.SpreenO,StraussE.Acompendiumofneuropsychological test:administration,norms,andcommentary.2nded.New York:OxfordUniversityPress;1998.
22.LezakMD,HowiesonDB,LoringDW.Neuropsychological assessment.4thed.NewYork:OxfordUniversityPress;2004.
23.TrenerryMR,CrossonB,DeBoeJ,LeberWR.Stroop
neuropsychologicalscreeningtestpsychologicalassessment. Odessa:PsychologicalAssessmentResources;1989.
24.BrunnerHI,RuthNM,GermanA,NelsonS,PassoMH, Roebuck-SpencerT,etal.Initialvalidationofthepediatric AutomatedNeuropsychologicalAssessmentMetricsfor childhoodonsetsystemiclupuserythematosus.Arthritis Rheum.2007;57:1174–82.
25.HinshawSP.Academicunderachievement,attentiondeficits, andaggression:comorbidityandimplicationsfor
intervention.JConsultClinPsychol.1992;60:893–903.
26.McCallRB.Academicunderachievers.CurrDirPsycholSci. 1994;3:15–9.
27.DaviesSM,RutledgeCM,DaviesTC.Theimpactofstudent learningstylesoninterviewingskillsandacademic performance.TeachLearnMed.1997;9:121–35.
28.AraújoA.Avaliac¸ãoemanejodacrianc¸acomdificuldade escolaredistúrbiodeatenc¸ão.JPediatr.2002;78:S104–10.
29.YeeC,FarewellVT,GrifftithsB,TehL,BruceLN,AhmadY, etal.TheuseofSystemicLupusErythematosusDisease ActivityIndex-2000todefineactivediseaseandminimal clinicallymeaningfulchangebasedondatafromalarge cohortofsystemiclupuserythematosuspatients. Rheumatology(Oxford).2011;50:982–8.
30.GladmanDD,UrowitzMB,GoldsmithCH,FortinP,GinzlerE, GordonC,etal.ThereliabilityoftheSystemicLupus InternationalCollaborationgClinics/AmericanCollegeof RheumatologyDamageIndexinpatientswithsystemiclupus erythematosus.ArthritisRheum.1997;40:809–13.
31.KovacsM.Children’sDepressionInventoryCDI:manual. Multi-HealthSystems:NewYork;1992.
32.CruvinelM,BoruchovitchE,SantosAAA.Inventáriode DepressãoInfantil(CDI):análisedosparâmetros psicométricos,20.Fractal:RevistadePsicologia;2008.p. 473–90.
33.BeckAT,SteerRA.BeckAnxietyInventory:manual.San Antonio:PsychologicalCorporation;1993.
34.CunhaJA.ManualdaversãoemportuguêsdasEscalasBeck. SãoPaulo:CasadoPsicólogo;2001.
35.HarrisEN,GharaviAE,PatelSP,HughesGR.Evaluationofthe anti-cardiolipinantibodytest:reportofaninternational workshopheld4April1986.ClinExpImmunol. 1987;68:215–22.
37.PasturaGMC,MattosP,AraújoAPQC.Desempenhoescolara transtornododéficitdeatenc¸ãoehiperatividade.Revistade PsiquiatriaClínica.2003;32:324.
38.MikdashiJ,HandwergerB.Predictorsofneuropsychiatric damageinsystemiclupuserythematosus:datafromthe Marylandlupuscohort.Rheumatology.2004;43:1555–60.
39.KozoraE,ThompsonLL,WestSG,KotzinBL.Analysisof cognitiveandpsychologicaldeficitsinsystemiclupus
erythematosuspatientswithoutovertcentralnervoussystem disease.ArthritisRheum.1996;39:2035–45.
40.IversonGL.Theneedforpsychologicalservicesforpersons withsystemiclupuserythematosus.Psychology.
1995;40:39–49.