w w w . r b o . o r g . b r
Original
article
Arthroplasty
of
the
distal
ulna
distal
in
managing
patients
with
post-traumatic
disorders
of
the
distal
radioulnar
joint:
measurement
of
quality
of
life
夽
Marcio
Aurélio
Aita,
Daniel
Schneider
Ibanez
∗,
Gabriel
Cunha
Barbosa
Saheb,
Rafael
Saleme
Alves
FaculdadedeMedicinadoABC(FMABC),SantoAndré,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1October2014 Accepted21October2014 Availableonline23October2015
Keywords:
Arthroplasty
Fracturesoftheradius Fracturesoftheulna Jointprosthesis
a
b
s
t
r
a
c
t
Objective:Tomeasurethequalityoflifeandclinical–functionalresultsfrompatients diag-nosedwithosteoarthrosisofthedistalradioulnarjointwhounderwentsurgicaltreatment usingthetechniqueoftotalarthroplastyoftheulna,withatotalor partialAscension® prosthesisofthedistalulna.
Methods:Tenpatientswereevaluatedafter12monthsoffollow-upsubsequenttototalor partialarthroplastyofthedistalulna.Allofthempresentedpost-traumaticosteoarthrosis and/orchronicsymptomaticinstabilityofthedistalradioulnarjoint.Thestudywas prospec-tive.Sevenpatientshadpreviouslyundergonewristprocedures(twocaseswithDarrach, threewithSauvé–Kapandjiandtwowithligamentreconstructionofthefibrocartilage com-plex)andthreepresentedfracturesofthedistalulnathatevolvedwithpain,instability andosteoarthrosisofthedistalradioulnarjoint.Thefollowingwereassessed:qualityoflife (DASHscale);percentagedegreeofpalmgripstrength(kgf)andpronosupinationrangeof motioninrelationtotheunaffectedside;pain(VAS);returntowork;subjectiveevaluation ofradiography;andcomplications.
Results:Thepatientspresentedameanrangeofmotionof174.5◦(normalside:180◦).Quality
oflifewasanalyzedbyapplyingtheDASHquestionnaireandthemeanvaluefoundwas5.9. ThemeanpainscoreusingtheVASwas2.3.Themeandegreeofpalmgripstrength(kgf) was50.7,whichrepresented90.7%ofthestrengthontheunaffectedside.Thecomplication ratewas10%:thispatientpresentedslightdorsalinstabilityoftheulnaandpersistentpain, anddidnotreturntowork.Thispatientisstillbeingfollowedupintheoutpatientclinic andoccupationaltherapysector,withlittleimprovement.Hedoesnotwishtoundergoa newprocedure.Themeanlengthoffollow-upwas16.8months,withaminimumof10and maximumof36months.
夽
WorkperformedintheHandSector,DepartmentofOrthopedicsandTraumatology,FaculdadedeMedicinadoABC(FMABC),Santo André,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.S.Ibanez). http://dx.doi.org/10.1016/j.rboe.2015.09.008
Conclusion: Thisconceptissubjecttothetestoftime.Implantationofaprosthesisisavery interestingadditiontothesurgicalarsenalforthosewhoarespecialistsinhandsurgery. Arthroplastyofthedistalulnaisasafeandeffectivemethodwithclinical–functionaland quality-of-lifeimprovementsforpatientsandpresentsalowcomplicationrate.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Artroplastia
de
ulna
distal
no
manejo
dos
pacientes
com
distúrbios
pós-traumáticos
da
articulac¸ão
radioulnar
distal:
mensurac¸ão
da
qualidade
de
vida
Palavras-chave:
Artroplastia Fraturasdorádio Fraturasdaulna Prótesearticular
r
e
s
u
m
o
Objetivo:Mensuraraqualidadedevidaeosresultadosclínico-funcionaisdospacientescom diagnósticodeosteoartrosedaradioulnardistalsubmetidosaotratamentocirúrgicopela técnicadeartroplastiatotaldaulnacomaprótesetotalouparcialAscension®daulnadistal.
Métodos: Foramavaliados10pacientescom12mesesdeseguimentodeartroplastiatotal ouparcial de ulnadistal.Todosapresentavam osteoartrosepós-traumática e ou insta-bilidadecrônicaesintomáticadaarticulac¸ãoradioulnardistal.Oestudofoiprospectivo. Setepacientestinhamprocedimentospréviosnopunho(2-darrach,3-Sauvé-kapandji, 2-reconstruc¸õesligamentaresdocomplexodafibrocartilagem)etrêsapresentaramfraturas daulnadistalqueevoluíram comdor,instabilidadeeosteoartrosedaradioulnardistal. Foramanalisadosaqualidadedevida(DASH),aporcentagemdograudeforc¸adepreensão palmar(kgf)eoarcodemovimentodepronossupinac¸ãoemrelac¸ãoaoladonãoafetado,a dor(VAS),oretornoaotrabalhoeaavaliac¸ãosubjetivadaradiografiaedascomplicac¸ões.
Resultados: Ospacientesapresentaram,emmédia,oarcodemovimentode174,5◦eolado
normal180◦.Aqualidadedevidafoianalisadapelaaplicac¸ãodoquestionárioDASHeovalor
médioencontradofoi5,9.Aavaliac¸ãodador,comousodaescalaVAS,foide2,3,emmédia.O graudeforc¸adepreensãopalmar(kgf)foide50,7,emmédia,oquerepresenta90,7%daforc¸a doladonãoacometido.Ataxadecomplicac¸õesfoide10%.Essepacienteapresentoudiscreta instabilidadedorsaldaulna,dorpersistenteenãoretornouaotrabalho.Essepacientesegue noambulatórioenosetordeterapiaocupacional,compoucamelhoria.Nãodesejafazer novoprocedimento.Otempodeseguimento,emmédia,foide16,8meses,commínimode 10emáximode36meses.
Conclusão:Esseconceitoestáatestedotempo.Aimplantac¸ãodeumapróteseéumaadic¸ão muitointeressanteaoarsenalcirúrgicoparaaquelesquesãoespecializadosemcirurgia damão.Aartroplastiadeulnadistaléummétodoseguro,eficaz,commelhoria clínico-funcionaledaqualidadedevidadospacienteseapresentabaixoíndicedecomplicac¸ões.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Fractures of the distal portions of the radius and ulna, ligament injuries of the triangular fibrocartilage complex, Essex-Loprestifracturesanddegenerativeosteoarthrosisdue torheumatoidarthritisarethemainprimarycausesof disar-rayofthedistalradioulnarjoint.Theintegrityofthisjoint isthe critical pointformaintaining the stabilityand func-tionalityofthe upperarmandforearm. Chronicinstability andosteoarthrosisleadtopainanddiminishedcapacityfor pronation–supination, grip strength and activities of daily living.1
Severalsurgicalsalvagemethodsforaddressing complica-tionsofthisjoint(osteoarthrosisand/orchronicinstability)are
known,2andtheseincludetheSauvéandKapandji,3Darrach4
and Bowers5 procedures.Thelimitations ofthesemethods
includeinstabilityofthedistalradioulnarjoint,impactofthe ulna onthe radiusand,consequently, residualpain inthis wrist.
In seeking integrity of the distal radioulnar joint, with mechanicalfulfillmentoftherelationshipbetweenthebones of the forearm along its entire extent, and reinsertion of the main ligament stabilizers of this joint, which enables pronation–supinationandloadtransmissionbytheulnar col-umnofthewrist,6–10prosthesesforthedistalulnahavebeen
developed.2
reasons,wedecidedtoconductthepresentstudy,inwhich arthroplastyofthedistalulnawasusedtotreatcomplications ofthedistalradioulnarjoint.
The objective was to measure the quality of life and clinical–functional results of patients with a diagnosis of osteoarthrosisofthedistalradioulnarjointwhounderwent surgicaltreatmentbymeansofthetechniqueoftotalulna arthroplastyusingtheAscension®totalorpartialprosthesis oftheulnarhead.
Materials
and
methods
BetweenJanuary2012andJuly2014,10patientswereattended at the outpatient clinic of the hand sector of our institu-tion(Table1).Allofthemhadadiagnosisofpost-traumatic osteoarthrosisand/orinstabilityofthedistalradioulnarjoint. They were included in the study and underwent physical examinationandsimpleradiographyinposteroanterior(PA), lateraland Leesand Scheckerviews,11 inordertoevaluate
theimpactoftheulnaontheradiusinpatientswhohad pre-viouslyundergoneDarrachandSauvé–Kapandjiprocedures, andalsounderwentmagneticresonanceimagingofthewrist inT1andT2weightings.
Theinclusioncriteriathatwereestablishedwerethatthe patients needed to be adults between 18 and 65 years of age,ofbothsexes,withclinicalandimagingdiagnoses,and thattheyneededtohavefilledoutastatementoffreeand informedvoluntaryconsentandaconflict-of-interest proto-col, as requiredbythe research ethics committee(CAAE – 12759113.7.0000.0082).
Patientswereexcludediftheypresenteddistalradioulnar instabilitywithout osteoarthrosisor if theyabandoned the treatmentatanystage.
Thefunctionalevaluationwasperformedbyprofessionals inthehandoccupationaltherapysector.
The clinical–functional measurements consisted of measuring the range of motion (ROM) of wrist pronation–supination in degrees, using a single specific goniometer. The clinical analysis on pain was performed using a visual analog scale (VAS) from one to ten, for subjectiveassessment.
Thequality-of-lifeassessmentwasmadeusingtheDASH questionnaire,whichisaninstrumentvalidatedfortheupper
limbs,andalsoaccordingtowhetherthepatientreturnedto work(ornot).
Thepostoperativeradiographicevaluationonthewristwas performed serially, atoutpatient consultations, inorder to checkonthepositioningoftheprosthesis.Thecomplication ratewasanalyzedthroughoutthefollow-up.
The distal ulna prostheses used were the First Choice Ascension®(partialcases)andtheModularUlnarHead(MUH) Ascension®(totalcases).Bothofthesearemodular endopros-thesis thatconsistofa headofhemispherical shape(total orpartial),madeofchromium–cobalt,whichisconnectedby meansofaneck,alsomadeofchromium–cobalt,withspecific orifices inits distalcomponent.Thisfits into theproximal portion,whichisanintramedullary nailcoveredwithpure titanium,in apress-fit system,which isaccommodatedin the diaphysis ofthe ulna. Several sizesor head, neck and nail are available,andthesecan becombined accordingto thesizeofthepatient’sulna.Theheadhasorificestoenable passageofsuturingthreadfromthetriangularfibrocartilage complex.
Descriptionofthesurgicaltechnique
1. Usualorthopedicpreparationforthepatient,inthesupine position.
2. Theaccessrouteisdorsaland arc-shapedinthewrist, underthedistalradioulnarjoint,outliningtheulnarhead, oflengthapproximately7cm.
3. Alllayersaredissected,undertheVextensortunnel. 4. Thedorsalcapsuleisopenedandarthrotomyofthedistal
radioulnarjointisperformed.
5. Replacementarthroplastyisperformed,withremovalof theulnarhead(partiallyortotally),usingaspecific micro-saw.
6. The distal and proximal components are placed after measurementusingspecificguidesandmillingcutters, withtheaidofradioscopy.
7. Reinsertionofthetriangularfibrocartilagecomplexinthe distalprosthesis.
8. Revisionofhemostasis,localcleaningandsuturingin lay-ers,includingthedorsal capsuleand thesheathofthe ulnarextensorofthecarpus,undertheprosthesis. 9. Suturingofthe retinaculumofthe extensors,
subcuta-neouscellulartissueandskin.
10. Releaseofthetourniquetandpreparationofdressings.
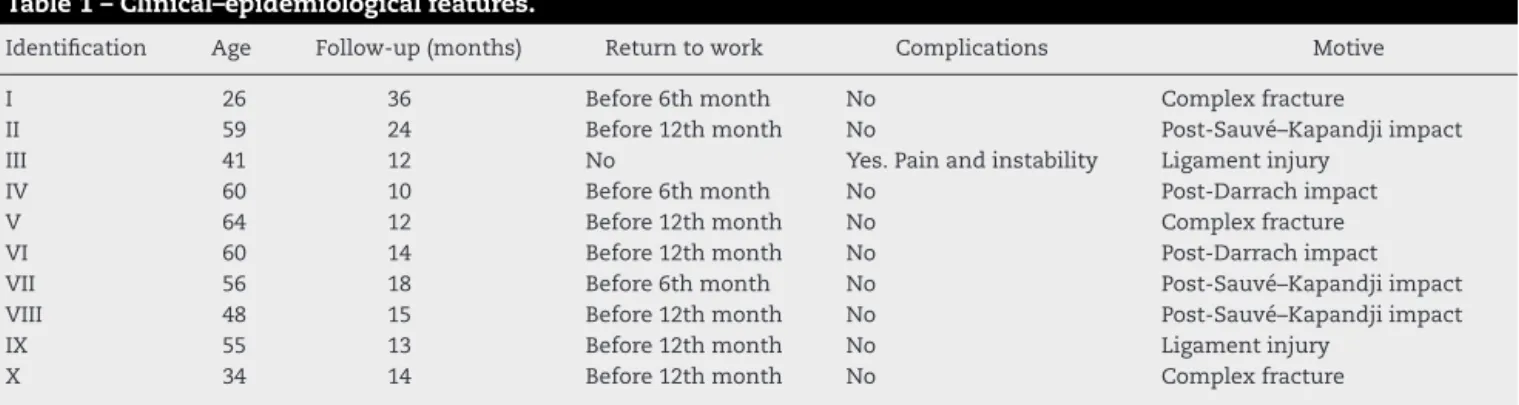
Table1–Clinical–epidemiologicalfeatures.
Identification Age Follow-up(months) Returntowork Complications Motive
I 26 36 Before6thmonth No Complexfracture
II 59 24 Before12thmonth No Post-Sauvé–Kapandjiimpact
III 41 12 No Yes.Painandinstability Ligamentinjury
IV 60 10 Before6thmonth No Post-Darrachimpact
V 64 12 Before12thmonth No Complexfracture
VI 60 14 Before12thmonth No Post-Darrachimpact
VII 56 18 Before6thmonth No Post-Sauvé–Kapandjiimpact
VIII 48 15 Before12thmonth No Post-Sauvé–Kapandjiimpact
IX 55 13 Before12thmonth No Ligamentinjury
X 34 14 Before12thmonth No Complexfracture
180.00 174.50 1 year Normal
ROM 181.00
180.00
179.00
178.00
177.00
176.00
175.00
174.00
173.00
172.00
171.00
ROM
Fig.1–Comparisonoftherange-of-motion(ROM)variable frombeforetoaftertheoperation.
Aftertheprocedure,thepatientswerekeptimmobilizedby meansofaplaster-castsplintfromtheaxillatothepalm,for uptosixweeks.Subsequently,thepatientunderwent rehabil-itationintheoccupationalsectorofthisinstitution,usinga preestablishedspecificprotocol.
Results
Thepatients presenteda mean range ofmotion of174.5◦,
whilethenormalsidewas180◦(Fig.1).
QualityoflifewasanalyzedbyapplyingtheDASH ques-tionnaire,which rangesfrom1to100, andthemean value foundwas5.9.
ThepainevaluationusingtheVAS(Fig.2)showedamean valueof2.3.
Themeanpalmargripstrength(kgf)was50.7.This repre-sented90.7%ofthestrengthoftheunaffectedside.
Thecomplication rate was 10%. This patient presented slightdorsalinstabilityoftheulnaandpersistentpain,and didnotreturntowork.Thispatientcontinuestoattendthe outpatientclinicandoccupationaltherapysector,withlittle improvement.Hedoesnotwishtoundergoanotherprocedure (Figs.3–5).
Themean lengthoffollow-up was 16.8 months,with a minimumof10andmaximumof36months.
1 year Normal
2.13 1.00
2.50
2.00
1.50
1.00
0.50
0.00
VAS
V
AS
Fig.2–Comparisonofthevisualanalogscale(VAS) variablefrombeforetoaftertheoperation.
Statisticalanalysis
Forthestatisticalanalyses,weusedthesignificancelevelof 5%(0.050) forapplyingthestatistical tests.Inother words, whenthecalculatedsignificancevalue(p)waslessthan5% (0.050),therewouldbeastatisticallysignificantdifference(in thecaseofcomparisons)orastatisticallysignificant relation-ship(inthecaseofrelationships),i.e.an“effectivedifference” inthecaseofcomparisonsora“strongrelationship”inthe caseofrelationships,respectively.Whenthecalculated sig-nificance value(p)was greater than orequalto5%(0.050), there would bea statisticallynon-significant difference(in the case of comparisons) or a statistically non-significant relationship(in thecaseofrelationships),i.e.a“similarity” inthe caseofcomparisonsor a“weakrelationship” inthe case of relationships, respectively. We used the Microsoft Excelelectronicspreadsheet(MS-Office2010version)to orga-nizethedataandtheIBMSPSSsoftware(StatisticalPackage fortheSocialSciences),version22.0,inordertoobtain the results.
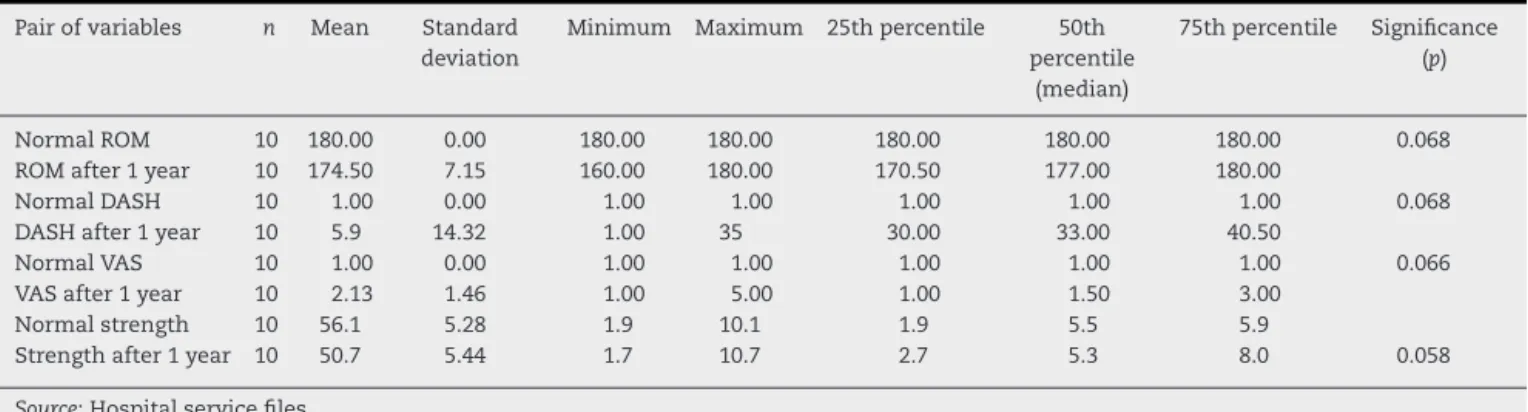
TheWilcoxonsigned-ranktestwasappliedwiththeaim ofinvestigatingpossibledifferencesbetweenthetwo obser-vationtimes(Table2),foreachvariableofinterest.
Thereweresimilarresultsforallthe variablesanalyzed, thusshowingthattheoperatedsidewassimilartothenormal side.
Table2–Comparisonofthevariablesofinterestbetweenthepreandpostoperativetimesofobservation.
Pairofvariables n Mean Standard deviation
Minimum Maximum 25thpercentile 50th percentile
(median)
75thpercentile Significance (p)
NormalROM 10 180.00 0.00 180.00 180.00 180.00 180.00 180.00 0.068 ROMafter1year 10 174.50 7.15 160.00 180.00 170.50 177.00 180.00
NormalDASH 10 1.00 0.00 1.00 1.00 1.00 1.00 1.00 0.068
DASHafter1year 10 5.9 14.32 1.00 35 30.00 33.00 40.50
NormalVAS 10 1.00 0.00 1.00 1.00 1.00 1.00 1.00 0.066
VASafter1year 10 2.13 1.46 1.00 5.00 1.00 1.50 3.00
Normalstrength 10 56.1 5.28 1.9 10.1 1.9 5.5 5.9
Strengthafter1year 10 50.7 5.44 1.7 10.7 2.7 5.3 8.0 0.058
Source:Hospitalservicefiles.
Discussion
There is no unanimity regarding the procedure of arthro-plasty of the distal ulna in our setting and no Brazilian articleshaveyetbeenpublished.However,inseeking stabi-lizationofthedistalradioulnarjoint,especiallyaftersalvage procedures2–5thatimprovepronation–supinationbutleadto
theulnaimpactingontheradiusinasymptomaticmanner1
whilestillmaintainingradioulnarjointinstability,weapplied adistalulnaprosthesisinordertoattempttoresolvethese complications.
Fig.4–Radiographicappearanceofthewristinlateral view,sixmonthsaftertheoperation,showingdorsal subluxationoftheprosthesisofthedistalulna(patientIII).
Biomechanical studies have presented statistically sig-nificant evidence showing that the prosthesis favors sta-bility, diminishes impaction on the radius and recovers pronation–supination,incomparisonwithothersalvage tech-niquescitedabove.8,12
Incomparingtheresultsfromourstudywiththosefrom othercaseseriesinwhichtheSauvéandKapandjiprocedure
apudCarterandStuart13wasappliedtodisordersofthedistal
radioulnarjoint,weobservedthattherewasbetterrecoveryof rangeofmotion(174.5◦versus172◦)andalowercomplication
rate(10%versus33.5%)inourpresentseries.
VanSchoonhoven etal.14 published amulticenterstudy
with long-term results (41 months of follow-up) from 23 patientswhoweretreatedusingtheHerbertUHP®prosthesis. Allthepatientspresentedstabledistalradioulnarjoints,none ofthepatientswasreoperatedandtheVASpainmeasurement was2.2.Thepronation–supinationrangeofmotionwas175◦
andthepalmargripstrengthrecoveredto81%inrelationto theunaffectedside.Allthepatientspresentedbone absorp-tioninthemostproximalregionofthenail(stressshielding) andremodelingofthesigmoidfossaoftheradius.Therewas nolooseningorfracturingoftheimplants,andthese radio-graphicfindings didnot show any clinical symptoms. Our studypresentedonecaseofinstabilityandresidualpaininthe distalradioulnarjoint,withstrengthrecoveryof90%,VASof 2.3andrangeofmotionof174.5◦.Wealsodidnotobserveany
radiographicalterationsinourpatients.Ourresultswere sim-ilartothoseoftheabovestudy,evenwithashorterfollow-up (16.8monthsversus41months).
Incomparingstudiesthatuseddifferenttotalprostheses in2009,Yen Shipleyetal.15 presentedaseries of22 wrists
in20 patients(14 UHPs® and 7uHeads®)with afollow-up of53.4months.Tenpatients presentedexcellentand good resultsaftertreatmentforosteoarthrosisconsistingofa pri-maryprosthesis,withoutanypreviousprocedure.Amongthe other12patientswhohadundergoneothertreatmentsprior to the prosthesis, 75% of the results were good or excel-lent.Their complicationrate was13% (threepatients):two patients evolved with dorsal subluxation and were subse-quently treated by means of ligament reconstruction; and onepatientpresentedpost-traumaticfracturingoftheulnar diaphysis. These three patients also evolved with good or excellent results.Ourcomplication ratewas 10%, compris-ingonepatientwithinstabilityanddorsalsubluxationofthe prosthesisthatremainsunresolved.
We had a single patient with a partial prosthesis (II),
who presentedosteoarthrosisonlyofthe radialulna,after chronicligamentinjuryofthetriangularfibrocartilage com-plex.Twenty-fourmonthsafterarthroplasty,rangeofmotion of180◦ wasobtained,withVASandDASHof1andrecovery
of96%ofthepalmargripstrength.Garcia-Elias16conducteda
studyonthreepatientswith11monthsoffollow-up,inwhich anEclypse®partialprosthesismadeofpyrocarbonwasused. Sofar,thesepatientsremainfreefrompain:theycanlift4kg weightwiththeirwristanddonotpresentanyinstabilityof thedistalradioulnarjoint.
AnotherseriespublishedbyFernandezetal.17presented
10patientswithafollow-up of2.6years.All ofthemwere treatedusingasphericalprosthesisproximaltotheulnarhead andsigmoidfossa ofthe radius.Allthe patientspresented failureoftheSauvé–Kapandjiprocedureandthisprosthesis wasplacedatthepseudarthrosisoftheulna,without remov-ing its head, and was connected to the region just below thesigmoidfossaoftheradiusand,superiorly,tothemost proximalpartoftheulnar head.All thepatients’ painand impaction of the ulna on the radius improved, and their degree ofpalmar grip strength recovered from 27% before thesurgeryto55%afterthesurgery,inrelationtothe unaf-fectedside.Therangeofmotionrecoveredtotally inseven patients, partiallyintwo and notatall inone.90% ofthe patientsreturned towork.Thecomplicationratewas 10%,
andthispatientcontinuedtopresentpainanddidnotrecover his pronation–supination movement.None ofthe patients presentedinstabilityoftheprosthesis.Inoursetting,useof theSauvé–Kapandjitechniqueisverycommonand compli-cationratesof13–39%havebeen reportedintheliterature. This prosthesisiswell indicated insuchcases: it isstable anddoesnotaltertherelationshipbetweentheulnarandthe carpus.
Savvidou etal.18 showedlong-termresults(fiveyearsof
follow-up)from35patientswhounderwenttotalarthroplasty ofthedistalradiususingthe AptisDRUJ® semi-constricted prosthesis.Thisprosthesisisindicatedfortreatmentofcases offailureofprimaryarthroplasty,andforpathological condi-tionsthataffecttheligamentstabilizationsystemofthedistal radioulnarjointdistal,suchascongenital,traumatic, degen-erativeandautoimmunepathologicalconditions.Itpresents not onlyproximaland distal ulnar components but alsoa radialcomponentthatcovers thesigmoidfossa.This func-tions as a bipolar prosthesis and is used in pathological conditions ofthe hip. Mostofthose authors’patients pre-sentedafunctionalrangeofmotionforpronation–supination, recovered their palmar grip strength and were able to do theiractivitiesofdailyliving(ADLs)inasatisfactorymanner, withoutpain.Twelvepatientspresentedcomplicationsbefore the surgery. Amongthese, there were casesof tendinopa-thy and insufficiency of the ulnar extensor of the carpus, heterotopicossification,bonereabsorptionwithlooseningof theprimaryprosthesisandinfection.ThetotalAptisDRUJ® prosthesis was shown to be a safe option that promoted improvementofpronation–supination,palmargripstrength and return toactivities of dailyliving. That study showed solutions for failure of primary arthroplasty of the distal ulna.
Conclusion
This concept is subject to the test of time. Implantation of a prosthesisis a very interesting addition to the surgi-cal arsenal for those who are specialists in hand surgery. Arthroplastyofthedistalulnaisasafeandeffectivemethod withclinical–functionalandquality-of-lifeimprovementsfor patientsandpresentsalowcomplicationrate.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WillisAA,BergerRA,CooneyWP3rd.Arthroplastyofthe distalradioulnarjointusinganewulnarhead
endoprosthesis:preliminaryreport.JHandSurgAm. 2007;32(2):177–89.
2.GordonKD,DunningCE,JohnsonJA,KingGJ.Kinematicsof ulnarheadarthroplasty.JHandSurgBr.2003;28(6):551–8. 3.SauveL,KapandjiM.Nouvelletechniquedetraitement
4. DarrachW.Anteriordislocationoftheheadoftheulna.Ann Surg.1912;56:802–3.
5. BowersWH.Distalradioulnarjointarthroplasty.Current concepts.ClinOrthopRelatRes.1992;275:104–9.
6. RotsaertP,CermakK,VancabekeM.Casereport:revisionof failedSauvé–Kapandjiprocedurewithanulnarhead prosthesis.ChirMain.2008;27(1):47–9.
7. DeSmetL,PeetersT.SalvageoffailedSauvé–Kapandji procedurewithanulnarheadprosthesis:reportofthree cases.JHandSurgBr.2003;28(3):271–3.
8. PalmerAK,WernerFW.Biomechanicsofthedistalradioulnar joint.ClinOrthopRelatRes.1984;187:26–35.
9. SauerbierM,FujitaM,HahnME,NealePG,BergerRA.The dynamicradioulnarconvergenceoftheDarrachprocedure andtheulnarheadhemiresectioninterpositionarthroplasty: abiomechanicalstudy.JHandSurgBr.2002;27(4):307–16. 10.MasaokaS,LongsworthSH,WernerFW,ShortWH,GreenJK.
Biomechanicalanalysisoftwoulnarheadprostheses.JHand SurgAm.2002;27(5):845–53.
11.LeesVC,SchekerLR.Theradiologicaldemonstrationof dynamiculnarimpingement.JHandSurgBr.1997;22: 448–50.
12.SauerbierM,Arsalan-WernerA,EnderleE,VetterM,VonierD. Ulnarheadreplacementandrelatedbiomechanics.JWrist Surg.2013;2(1):27–32.
13.CarterPB,StuartPR.TheSauve–Kapandjiprocedurefor post-traumaticdisordersofthedistalradio-ulnarjoint.JBone JointSurgBr.2000;82(7):1013–8.
14.vanSchoonhovenJ,Mühldorfer-FodorM,FernandezDL, HerbertTJ.Salvageoffailedresectionarthroplastiesofthe distalradioulnarjointusinganulnarheadprosthesis: long-termresults.JHandSurgAm.2012;37(7):1372–80. 15.YenShipleyN,DionGR,BowersWH.Ulnarheadimplant
arthroplasty:anintermediatetermreviewofonesurgeon’s experience.TechHandUpExtremSurg.2009;13(3):160–4. 16.Garcia-EliasM.Eclypse:partialulnarheadreplacementfor
theisolateddistalradio-ulnarjointarthrosis.TechHandUp ExtremSurg.2007;11(1):121–8.
17.FernandezDL,JoneschildES,AbellaDM.Treatmentoffailed Sauvé–Kapandjiprocedureswithasphericalulnarhead prosthesis.ClinOrthopRelatRes.2006;445:100–7. 18.SavvidouC,MurphyE,MailhotE,JacobS,SchekerLR.