r e v b r a s o r t o p . 2015;50(5):546–549
w w w . r b o . o r g . b r
Original
Article
Saphenous
nerve
injury
during
harvesting
of
one
or
two
hamstring
tendons
for
anterior
cruciate
ligament
reconstruction
夽
Vitor
Barion
Castro
de
Padua
∗,
Paulo
Emílio
Dourado
Nascimento,
Sergio
Candido
Silva,
Sergio
Marinho
de
Gusmão
Canuto,
Guilherme
Nunes
Zuppi,
Sebastião
Marcos
Ribeiro
de
Carvalho
SchoolofMedicine,UniversidadedeMarília,Marília,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received16July2014 Accepted17August2014 Availableonline29August2015
Keywords:
Anteriorcruciateligament Paresthesia
Hamstring
a
b
s
t
r
a
c
t
Objective:Theaimofthisstudywastoassesswhetherharvestingoftwohamstring ten-dons(semitendinosusandgracilis)hasthesamerateofnerveinjuryasharvestingofthe semitendinosustendonalone,usedasatriplegraft.
Methods:Changesinsensitivityrelatingtoinjuryoftheinfrapatellarbranchofthe saphe-nousnervewereevaluatedin110patientssixmonthsaftertheyunderwentanteriorcruciate ligament(ACL)reconstructionusinghamstringtendons.Theyweredividedintotwogroups: oneinwhichonlythesemitendinosuswasusedandtheother,thesemitendinosusand gracilis.
Results:Thegroupinwhichonlythesemitendinosuswasusedasagraftpresentedanerve injuryrateof36.1%.Inthegroupinwhichthesemitendinosusandgracilistendonswere used,58.1%ofthepatientspresentedalteredsensitivity.Inthegeneralassessmentonall thepatients,thenerveinjuryratewas50.9%.
Conclusion:Harvestingthesemitendinosusaloneandusingitintripleformisaviableoption forACLreconstructionandmaygiverisetofewernerveinjuriesrelatingtobranchesofthe saphenousnerve.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Lesão
do
nervo
safeno
na
retirada
de
1
ou
2
tendões
flexores
na
reconstruc¸ão
do
ligamento
cruzado
anterior
Palavras-chave:
Ligamentocruzadoanterior Parestesia
r
e
s
u
m
o
Objetivo:Avaliarsearetiradadosdoistendõesflexores(semitendíneo[ST]egrácil[GC])tem omesmoíndicedelesãonervosaquearetiradaisoladadotendãoSTusadocomoenxerto triplo.
夽
WorkperformedintheDepartmentofOrthopedicsandTraumatology,SchoolofMedicine,UniversidadedeMarília,Marília,SP,Brazil. ∗ Correspondingauthor.
E-mails:[email protected],[email protected](V.B.C.dePadua).
http://dx.doi.org/10.1016/j.rboe.2015.08.007
rev bras ortop.2015;50(5):546–549
547
Tendõesflexores Métodos: Foiavaliadaaalterac¸ãodesensibilidaderelacionadaàlesãodoramoinfrapatelar donervosafenoem110pacientesseismesesapósseremsubmetidosàreconstruc¸ãodo LCAcomousodostendõesflexores,divididonumgruponoqualseusousomenteoSTe outrocomoSTeoGC.
Resultados: OgruponoqualseusousomenteoSTcomoenxertoapresentouumíndice delesãonervosade36,1%enogrupocomostendõesSTeGC58,1%dospacientestiveram alterac¸ãodasensibilidade.Naavaliac¸ãogeraldetodosospacientesoíndicedelesãonervosa foide50,9%.
Conclusão: A retirada do ST isolado e usado de forma tripla é uma opc¸ãoviável na reconstruc¸ãodoLCAepodeocasionarummenornúmerodelesãonervosarelacionada aramosdonervosafeno.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Anteriorcruciateligament(ACL)injuries,whichare incapaci-tatingforcertainphysicalactivitiesbecauseoftheinstability that is caused, predispose toward meniscal and cartilage lesions that may evolve to arthrosis.1 ACL reconstruction
seekstorestorejointstability.
WiththeevolutionofsurgicalproceduresforACL recon-struction, patients’ expectations regarding the results are becominggreater.Theyseektoreturntotheirdailyactivities earlierandwithlessmorbidity.2
Thetendonsthataremostusedforthisprocedurearethe flexortendons(semitendinosusandgracilis)andthecentral thirdofthepatellarligament.Theliteratureshowsthatthe resultsfrom using thesetwo grafts are similar,3–6 but it is
believedthatusingtheflexortendonsleadstolower postop-erativemorbidity.7
However,graftharvestingisnotrisk-free.Thecommonest complicationisregionalparesthesiaoranesthesiaintheleg, causedbyinjurytotheinfrapatellarbranchofthesaphenous nerve(IPSN). There have been reportsof incidencegreater than70%.8,9
Toreducetheincidenceofthiscomplication,someauthors havechosentouse amoreoblique incision,10whileothers
haveattemptedtoexploreandidentifythenerveatthetime ofharvestingthegraft.2
Theaimof the present study was to compare whether harvesting a flexortendon (semitendinosus) has the same incidenceofnerveinjuriesasdoesharvestingofbothtendons (semitendinosusandgracilis)bymeansofaverticalincision, foruseasgraftsinACLreconstruction.
Materials
and
methods
Sixmonthsaftertheoperation,110patientswhohad under-goneACLreconstructionusingflexortendonswereassessed. Atriplegraftfromthesemitendinosustendonwasusedwhen remnantsofthetornACL hadbeenpreservedorwhenthe diameterofthegraftwasgreaterthan8mm,foratotalof36 patients.
WhentherewasnoremnantACLorthesemitendinosus tendondidnotreachadiameterof8mm,thereconstruction
was done usinga quadruple graft from the flexortendons (semitendinosusandgracilis),whilealwaysmaintainingtheir distalinsertioninthetibia,foratotalof74patients.
Patients whohad notundergonesuturingofthemedial meniscususingthe“in-out”or“out-in”technique(inwhich asmallmedialincisionwasmade)werenotincludedinthe evaluation.Likewise,patientswithscarsorprevioussurgery onthekneewerealsonotincluded.
Surgicaltechnique
ACLreconstructionwasperformedusingatourniquetatthe baseofthethighandspinalanesthesiainallcases.
Theprocedurewas startedwithharvesting ofthe semi-tendinosustendonbymeansofaverticalincisionthatwas madeapproximately1.5cmmediallyanddistallytothe ante-riortuberosityofthetibia,withanaveragelengthof2.8cm. Thefasciaofthesartorius,whichcoverstheflexortendons, wasopenedhorizontallyand,withtheaidoftwo“mixters”, thesemitendinosuswasisolatedandharvestedbymeansof an openstripper (pigtailtype),whilemaintaining itsdistal insertioninthetibia.6
The muscle portion was cleaned and the arthroscopic procedure was started through conventional anteromedial and anterolateral portals. After treatment of the asso-ciated lesions, the existence of any viable remains of the ACL was ascertained. The femur was then prepared for drilling the tunnel, which was done by means of independent “out-in” drilling, following the technique of Chambat.11
Inthetibia,whentherewereviableremainsoftheACL,we didthedrillingusingtheremainsasthelocation.Withtheaid ofashaver,apathwithintheremainswascreated.12
When there were no remainsofthe ACL or thesewere unviable,thetibialtunnelwasconstructedwithinthetibial footprint,usingtheanteriorcornuofthelateralmeniscusand themedialtibialspineasthelocationparameter.Inthiscase, orwhenthetriplegraftfromthesemitendinosuspresented a diameterof less than 8mm, wereturned to theincision overtheflexorsandharvestedthegracilistendoninthesame manner.
548
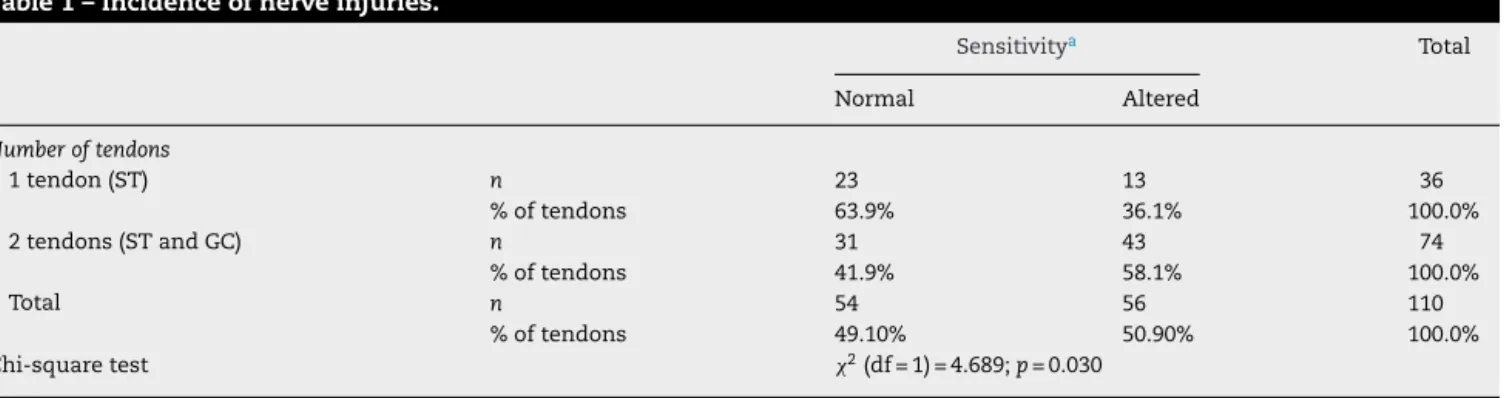
rev bras ortop.2015;50(5):546–549Table1–Incidenceofnerveinjuries.
Sensitivitya Total
Normal Altered
Numberoftendons
1tendon(ST) n 23 13 36
%oftendons 63.9% 36.1% 100.0% 2tendons(STandGC) n 31 43 74
%oftendons 41.9% 58.1% 100.0%
Total n 54 56 110
%oftendons 49.10% 50.90% 100.0% Chi-squaretest 2(df=1)=4.689;p=0.030
a Forcolumnswithdifferenceletters,theirproportionspresentasignificantdifferenceattheprobabilitylevelof5%.
inthetibia.Thefixationwasdoneusinginterferencescrews, firstlyinthetibiaandsecondlyinthefemur,fromouttoin, closetotheextension.
No drains were used. The patients were released 24h after the operation, and at this time physiotherapy was started,withprogressivepartialweight-bearingwiththeaid ofcrutchesfor15days.
The patients were assessedsix monthsafter the oper-ation and they were asked to define the area over which altered sensitivity was present in the leg that had been operated.
Statisticalanalysis
The data were summarized in tables showing the total numbersofindividualsandtheabsolutefrequenciesand per-centagesforthequalitativevariables.
Associationsbetweensensitivity(normaloraltered)and thenumber oftendons(semitendinosus orsemitendinosus plusgracilis)wereascertainedusingthePearsonchi-square test,andtheztestwasusedtomakecomparisonsbetween theproportionsofthecolumns.13
Results
Alteredsensitivitywasfoundin36.1%(13/36)ofthepatients inwhomonlythesemitendinosustendonhadbeenusedas agraft;and in58.1% (43/74)ofthe patients inwhom both tendonhad beenused(semitendinosus andgracilis).Inthe generalevaluationwithallthepatients,50.9%(56/110) pre-sentednerveinjuries(Table1).
The result from the chi-square test was significant (p=0.030)andmadeitpossibletostatethattherewasgreater occurrenceofalteredsensitivityafterthesurgerywhenboth ofthetendons(semitendinosusandgracilis)wereused.Inthe groupinwhichonlyonetendon(semitendinosus)wasused, itwas observedthattheproportionoftheindividuals who presentednormalsensitivity(63.9%)wasgreaterthanthe pro-portionwithalteredsensitivity(36.1%).Thiswastheinverse ofthesituationinthegroupinwhichtwotendons (semitendi-nosusplus gracilis)were used, sincethe proportionofthe individualswithnormalsensitivity(41.9%)waslowerthanthe proportionwithnervelesions(58.1%).
Discussion
ACLreconstructionusingflexortendonsisnotfreefrom com-plications.Thecommonestoftheseisinjurytoabranchofthe saphenousnerve,forwhichthereportedincidencecanbeas highas77%.8,9
Thisismostcommonlyseenintheinfrapatellarbranch (IPSN), which crosses the anterior regionof theknee, well belowthepatella.14Thisbranchisperpendicularandatrisk
ofinjurybecauseoftheverticalincisionthatismadefor har-vestingtheflexortendonsandbecauseofthewoundcaused bythearthroscopyportal.14,15
Luoetal.10comparedtheincidenceofnerveinjuriesin
rela-tiontoflexortendonharvesting,betweenuseofobliqueand verticalincisions,andconcludedthatobliqueincisionsledto anerveinjuryrateof24%versus56%forverticalincisions.
Papastergiouetal.16usedverticalincisionstoharvestthe
patellarligament andfoundthat39.7% ofthepatients pre-sented nerve injuries. Saglione et al.8 harvested only the
semitendinosus and found that 37.5% presented injuries, whichwassimilartothefindingsfromourgroupthatused thesemitendinosusalone,inwhichtheratewas36.1%.
Mochizukiet al.17 reportedthattheincidenceofaltered
sensitivity through harvesting of the flexor tendons was 58%, which was similar to the findings from ourgroup in whichbothflexortendonswereharvestedandtheratewas 58.1%.
During the procedure for harvesting grafts from the flexortendons,MirzatolooeiandPisoodeh2isolatedsuperficial
branchesofthesaphenousnerveandpreservedthem.They reportedthattheirnerveinjuryratewas20.5%,incomparison witharateof72%amongpatientsinwhom thesuperficial nervebrancheswerenotfound.Theyalsoreportedthat9.8% of the patientswho presentedaltered sensitivitysaid that this wason themedialfaceoftheleg, andmadethe sup-positionthatthisalterationwasnotrelatedtoinjuryofthe IFSNbranchbutrather,toinjuryofthesartoriusbranchofthe saphenousnerve(SBSN).Thelatterpresentsaninitially verti-calpathtogetherwiththesartoriusmuscleanditemergesin thesubcutaneouslayerbetweenthetendonofthesartorius andthegracilis.Itthencontinuesdistallytogetherwiththe saphenousveinandisresponsiblefortheinnervationofthe knee,lowerlegandankle.3,18Thistypeofinjuryisthoughtto
rev bras ortop.2015;50(5):546–549
549
SBSNinjurieswere alsodescribed bySanders etal.19 In
theirstudyon164patients, theyfoundthat 23%presented injuryoftheSBSNaloneand19%oftheIPSNalone,while32% hadtheseinjuriesconcomitantly.TheyconcludedthatSBSN injuriesduetopassageofthestrippermaybemorecommon thanisreportedintheliterature,becausethepathofthisnerve isveryclosetothegracilisinthedistalregionofthethigh.
Inourstudy,36.1%ofthecasesofharvestingthe semitendi-nosusalonepresentednervealterations,whereas58.1%with harvestingofthesemitendinosusandgracilisdidso.This dif-ferencewasstatisticallysignificant.Weonlyhadonecasein whichalteredsensitivitywasreportedtobeexperiencedin theregionoftheSBSN,inapatientfromwhombothtendons wereharvested.
InanattempttoavoidSBSNinjury,someauthors20 have
advisedthattheflexortendons(andespeciallythegracilis) shouldbeharvestedwiththekneeina“figure-four”position, soastorelaxthesaphenousnerve.However,others19 have
reportedthatnerveinjuriesoccurredevenwiththisharvesting technique.
Preservationofoneoftheflexortendons(gracilis)inACL reconstructionsmayleadtolowerincidenceofnerveinjuries andlesslossofmusclestrength,whichmaybebeneficialfor therehabilitation.
Conclusion
Harvestingofthesemitendinosusalone,foruseintripleform inACLreconstruction,maybeaviablegraftingoptionwith lowerriskofinjurytobranchesofthesaphenousnervein com-parisonwithusinggraftsfromboththesemitendinosusand thegracilis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BrayRC,DandyDJ.Meniscallesionsandchronicanterior cruciateligamentdeficiency.Meniscaltearsoccurringbefore andafterreconstruction.JBoneJointSurgBr.
1989;71(1):128–30.
2. MirzatolooeiF,PisoodehK.Impactofexplorationofsensory branchesofsaphenousnerveinanteriorcruciateligament reconstructivesurgery.ArchIranMed.2012;15(4):219–22.
3. HarilainenA,LinkoE,SandelinJ.Randomizedprospective studyofACLreconstructionwithinterferencescrewfixation inpatellartendonautograftsversusfemoralmetalplate suspensionandtibialpostfixationinhamstringtendon autografts:5-yearclinicalandradiologicalfollow-upresults. KneeSurgSportsTraumatolArthrosc.2006;14(6):517–28.
4. PinczewskiLA,LymanJ,SalmonLJ,RussellVJ,RoeJ,Linklater J.A10-yearcomparisonofanteriorcruciateligament reconstructionswithhamstringtendonandpatellartendon autograft:acontrolled,prospectivetrial.AmJSportsMed. 2007;35(4):564–74.
5.JanssonKA,LinkoE,SandelinJ,HarilainenA.Aprospective randomizedstudyofpatellarversushamstringtendon autograftsforanteriorcruciateligamentreconstruction.AmJ SportsMed.2003;31(1):12–8.
6.PáduaVBC,MaldonadoH,VilelaJCR,ProvenzaAR,Monteiro C,OliveiraNetoHC.Estudocomparativodareconstruc¸ãodo LCAcomoposicionamentoanatômicodostúneisentreo tendãopatelareostendõesflexores.RevBrasOrtop. 2012;47(1):50–6.
7.BiauDJ,TournouxC,KatsahianS,SchranzPJ,NizardRS. Bone-patellartendon-boneautograftsversushamstring autograftsforreconstructionofanteriorcruciateligament: meta-analysis.BMJ.2006;332(7548):995–1001.
8.SgaglioneNA,WarrenRF,WickiewiczTL,GoldDA,Panariello RA.Primaryrepairwithsemitendinosustendon
augmentationofacuteanteriorcruciateligamentinjuries. AmJSportsMed.1990;18(1):64–73.
9.AgliettiP,GironF,BuzziR,BiddauF,SassoF.Anteriorcruciate ligamentreconstruction:bone-patellartendon-bone comparedwithdoublesemitendinosusandgracilistendon grafts.Aprospective,randomizedclinicaltrial.JBoneJoint SurgAm.2004;86(10):2143–55.
10.LuoH,YuJK,AoYF,YuCL,PengLB,LinCY,etal.Relationship betweendifferentskinincisionsandtheinjuryofthe infrapatellarbranchofthesaphenousnerveduringanterior cruciateligamentreconstruction.ChinMedJ(Engl). 2007;120(13):1127–30.
11.GarofaloR,MouhsineE,ChambatP,SiegristO.Anatomic anteriorcruciateligamentreconstruction:thetwo-incision technique.KneeSurgSportsTraumatolArthrosc.
2006;14(6):510–6.
12.LöcherbachC,ZayniR,ChambatP,Sonnery-CottetB. BiologicallyenhancedACLreconstruction.OrthopTraumatol SurgRes.2010;96(7):810–5.
13.SPSS.IBMSPSSStatisticsBase20Manual,SPSS.Chicago,IL: SPSSInc.;2011.
14.EbraheimNA,MekhailAO.Theinfrapatellarbranchofthe saphenousnerve:ananatomicstudy.JOrthopTrauma. 1997;11(3):195–9.
15.KartusJ,MovinT,KarlssonJ.Donor-sitemorbidityand anteriorkneeproblemsafteranteriorcruciateligament reconstructionusingautografts.Arthroscopy.
2001;17(9):971–80.
16.PapastergiouSG,VoulgaropoulosH,MikalefP,ZiogasE, PappisG,GiannakopoulosI.Injuriestotheinfrapatellar branch(es)ofthesaphenousnerveinanteriorcruciate ligamentreconstructionwithfour-strandhamstringtendon autograft:verticalversushorizontalincisionforharvest. KneeSurgSportsTraumatolArthrosc.2006;14(8):789–93.
17.MochizukiT,MunetaT,YagishitaK,ShinomiyaK,SekiyaI. Skinsensorychangeafterarthroscopically-assistedanterior cruciateligamentreconstructionusingmedialhamstring tendonswithaverticalincision.KneeSurgSportsTraumatol Arthrosc.2004;12(3):198–202.
18.WijdicksCA,WesterhausBD,BrandEJ,JohansenS,
EngebretsenL,LaPradeRF.Sartorialbranchofthesaphenous nerveinrelationtoamedialkneeligamentrepairor reconstruction.KneeSurgSportsTraumatolArthrosc. 2010;18(8):1105–9.
19.SandersB,RolfR,McClellandW,XerogeanesJ.Prevalenceof saphenousnerveinjuryafterautogenoushamstringharvest: ananatomicandclinicalstudyofsartorialbranchinjury. Arthroscopy.2007;23(9):956–63.