https://doi.org/10.1590/0004-282X20170035
ARTICLE
Long term follow-up of growth
hormone-secreting pituitary adenomas
submitted to endoscopic endonasal surgery
Seguimento de longo prazo de adenomas hipofisários secretores do hormônio do
crescimento submetidos à cirurgia endoscópica endonasal
Caroline Martins dos Santos Leopoldo1, Felippe Martins dos Santos Leopoldo1, Américo Rubens Leite dos
Santos2, José Carlos Esteves Veiga2, José Viana Lima Junior3, Nilza Maria Scalissi3, Paulo Roberto Lazarini4,
Ricardo Landini Lutaif Dolci4
1 Faculdade de Ciências Médicas, Santa Casa de São Paulo, São Paulo SP, Brasil;
2 Faculdade de Ciências Médicas, Santa Casa de São Paulo, Departamento de Cirurgia, Disciplina de Neurocirurgia, São Paulo SP, Brasil; 3 Faculdade de Ciências Médicas, Santa Casa de São Paulo, Departamento de Medicina, Disciplina de Endocrinologia, São Paulo SP, Brasil; 4 Faculdade de Ciências Médicas, Santa Casa de São Paulo, Departamento de Otorrinolaringologia São Paulo SP, Brasil.
Correspondence: Américo R. L. Santos; Rua Martinico Prado,131 / AP 5; 01224-011 São Paulo SP, Brasil; E-mail: [email protected]
Conflict of interest: There is no conlict of interest to declare.
Received 16 September 2016; Received in inal form 23 December 2016; Accepted 24 January 2017.
ABSTRACT.
Objective: The aim of this study was to evaluate the results of the endoscopic transsphenoidal technique for growth hormone (GH)-secreting adenomas. Methods: A retrospective analysis based on medical records of 23 acromegalic patients submitted to endoscopic transsphenoidal surgery. Biochemical control was deined as basal GH < 1ng/ml, nadir GH < 0.4ng/ml after glucose load and age-adjusted IGF-1 normal at the last follow-up. Results: The overall endocrinological remission rate was 39.1%. While all microademonas achieved a cure, just one third of macroadenomas went into remission. Suprasellar extension, cavernous sinus invasion and high GH levels were associated with lower rates of disease control. The most common complication was diabetes insipidus and the most severe was an ischemic stroke. Conclusion: The endoscopic transsphenoidal approach is a safe and effective technique to control GH-secreting adenomas. The transcavernous approach may increase the risk of complications. Suprasellar and cavernous sinus extensions may preclude gross total resection of these tumors.
Keywords: acromegaly; growth hormone-secreting pituitary adenoma; endoscopy
RESUMO
Objetivo: O objetivo do estudo é analisar os resultados da cirurgia de ressecção endoscópica transesfenoidal para adenomas secretores do hormônio do crescimento (GH). Métodos: Revisão retrospectiva baseada em análise de prontuários de 23 pacientes acromegálicos submetidos à cirurgia endoscópica. Remissão foi deinida por GH < 1ng/ml, nadir de GH ≤ 0,4ng/ml no teste oral de tolerância a glicose e IGF-1 normal para idade. Resultados: A taxa de remissão endocrinológica foi 39,1%. Enquanto todos microadenomas alcançaram controle hormonal, apenas um terço dos macroadenomas obtiveram remissão. Extensão suprasselar, invasão do seio cavernoso e altos níveis de GH foram associados a menores taxas de controle da doença. A complicação mais comum foi diabetes insipidus e a mais grave foi acidente vascular encefálico isquêmico. Conclusão: A abordagem endoscópica transesfenoidal é segura e efetiva para controle de adenomas hipoisários secretores de GH. A abordagem ao seio cavernoso pode aumentar a morbidade da cirurgia. Extensões suprasselares e no seio cavernoso podem diicultar a ressecção completa e o controle da doença.
Palavras-chave: acromegalia; adenoma hipoisário secretor de hormônio do crescimento; endoscopia
Supraphysiological levels of growth hormone (GH) and insulin-like growth factor 1 (IGF-1) are related to acromegaly1,2. his chronic disease is most commonly caused by pituitary tumors3,4. he increase in GH levels can cause cardiovascu -lar and cerebrovascu-lar diseases, which commonly result in death. Acromegaly carries a mortality rate at least twice as high as in the general population4.
he main goal of treatment is the normalization of GH, IGF-1 levels and nadir GH < 0.4ng/ml after an oral glucose load, to reduce symptoms and mortality5,6,7,8. he options for
pituitary surgery for acromegaly was performed by Caton and Paul, under the supervision of Sir Victor Horsley11,12,13, while the irst transnasal resection of a pituitary tumor was performed by Schlofer in 190714. Cushing15 systematically used a
transs-phenoidal approach in sellar lesions and this technique was subsequently reined and popularized by Guiot16 and Hardy17,18. he objectives of the surgical approach are gross tumor resec -tion, relief of mass efect, normalization of hormone levels, reduction of recurrences and avoidance of postoperative com-plications, resulting in reduced morbidity and mortality3,19,20.
he microsurgical transsphenoidal route has been the main approach for this disease. he endoscopic technique is a recent innovation3,21,22 that allows a panoramic wide angle view to efectively reach supra- and parasellar lesions. herefore has been suggested that the endoscopic technique may be preferred over the conventional technique, especially in patients with invasive macroadenomas23,24,25.
he aim of this study was to evaluate the results of the endoscopic transsphenoidal technique for the control of GH-secreting adenomas.
METHODS
Patient population
A retrospective analysis based on medical records of acromegalic patients who underwent endoscopic transsphe-noidal surgery, between February 2005 and April 2015.
he records of 104 patients that had pituitary surgery were reviewed, 26 had GH-secreting adenomas, and three were excluded because of missing data.
his study was approved by the Research Ethics Committee of Santa Casa de Misericórdia de São Paulo (project number 36634114.9.0000.5479).
Endocrinological evaluation
Growth hormone, IGF-1, oral glucose tolerance, and the remaining pituitary hormones were measured preopera-tively, three months postoperapreopera-tively, and at the last follow-up. Hormonal control was deined as GH < 1.0 ng/ml and not higher than 0.4 ng/ml after glucose load, and IGF-1 levels normal for age7.
Neuroimaging examination
Tumors were classiied according to their size (macroad -enomas > 1cm, microad-enomas ≤ 1cm) and extension (sellar, suprasellar, parasellar).
Invasion of the cavernous sinus was considered when the magnetic resonance imaging (MRI) demonstrated Grade 2 or higher in the Knosp classiication26.
Surgical procedure
All the patients were submitted to an endoscopic endo -nasal transsphenoidal approach with a technique described
in our previous publication18. All operations were performed by the same neurosurgeon.
Statistical analysis
Data was analyzed with OpenEpi Software, a web-based epidemiologic and statistical calculator for public health27.
Descriptive statistics, such as mean, standard deviation and range were used to describe continuous variables, and percentages were used to describe categorical variables. Statistical analysis, consisting of the Chi-square test or Fisher exact test, Chi-square for trend and Student’s t test, were per -formed to predict the remission rate based on tumor exten -sion, GH and IGF-1 levels. A p value of less than 0.05 was con-sidered statistically signiicant.
RESULTS
Patients characteristics
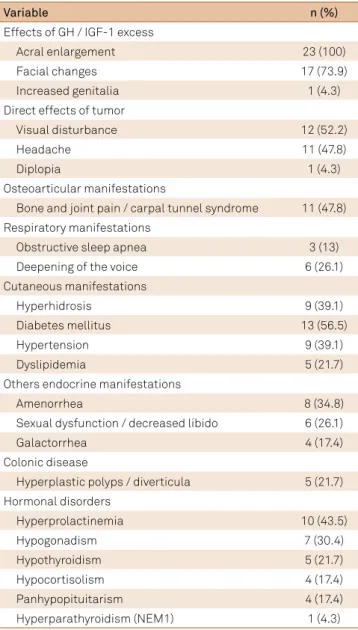
Of the 23 patients evaluated for GH-secreting adeno -mas, nine (39.1%) were male and 14 (60.9%) were female. The mean age was 41.7 ± 11.9 years (range 15-65 years). The clinical manifestations of these patients are pre-sented in Table 1. All the patients prepre-sented with clini -cal signs of acromegaly. Diabetes mellitus was the most common associated disease (56.5%). Approximately half of these patients presented with decreased visual acu-ity or visual fields, headaches, and bone and joint pain. No severe cardiovascular disease was identified and one patient presented with a cardiac valve lesion dur-ing follow-up. The mean preoperative GH values were 28.2 ± 35.6 ng/ml (range 2.4–151 ng/ml) and IGF-1 values were 730.7 ± 212.5 ng/ml (range 268–1178 ng/ml). Mean fol -low-up time was 46.9± 28.2 months (range 8–125 months).
Tumor characteristics
he majority of the tumors were classiied as macroadeno -mas corresponding to 91.3% of the cases (21 patients). From all macroadenomas, 10 (47.6%) showed cavernous sinus invasion and 11 (52.4%) showed suprasellar extension (Table 2).
Table 2. Magnetic resonance imaging characteristics on 23 preoperative patients.
Variable n (%)
Microadenoma (< 1 cm) 2 (8.7)
Macroadenoma (> 1 cm)
S 6 (26.1)
S + CS 4 (17.4)
S + SS 5 (21.7)
S + SS + CS 6 (26.1)
S: sellar; SS: suprasellar; CS: cavernous sinus.
Table 3. Material used to close the sella in the irst approach of 23 patients.
Variable n (%)
Absorbable hemostatic 4 (17.4)
Absorbable hemostatic + ibrin glue 2 (8.7)
Fat graft / fascia lata + ibrin glue 3 (13)
Mucoperiosteal lap + ibrin glue 13 (56.5)
Mucoperiosteal lap + ibrin glue + fat graft / fascia lata 1 (4.3)
After the irst approach, nine patients (39.1%) achieved hor -monal remission, evaluated by serum GH levels < 1 ng/ml, IGF-1 levels normal for age and GH levels suppressed to < 0.4 ng/ml after glucose load. However, one of these patients could not be evaluated with the oral glucose test, because of diabetes. Postoperative MRI showed total tumor resection in eight cases (43.5%) and the presence of a residual lesion in 15 cases (56.5%), one of which had no clinical correlation. All 14 patients (60.9%) with persistent disease after the irst surgery received medical treatment (Octreotide). hree of them were submitted to a sec -ond approach. After the sec-ond surgery, one patient achieved hormonal remission and medical treatment was suspended, the other patient was controlled with permanent medication. Both patients had an MRI demonstrating apparent total tumor resection. he third patient had a subtotal tumor resection and still lives with active disease. Another two patients received ste-reotactic radiotherapy. One of them was controlled with medi -cation and presented with progressive hormonal level reduction over the eight years of follow-up. he other patient lives with persistent disease. Of the nine patients who received only medi -cal treatment, only two achieved biochemi-cal remission.
No recurrence of the GH-secreting adenoma occurred in the follow-up. Seven patients (33.3%) reported signiicant body soft tissue reduction. Of the 12 patients with visual disturbance, ive (41.7%) showed improvement postoperatively. Of the 13 patients with diabetes mellitus, half had glycated hemoglobin reduction and a quarter could reduce their medication. Of the 10 patients with hypertension, two (20%) showed improvement.
Complications
In our study, surgical complications occurred in 13 patients (56.5%). Diabetes insipidus was the most common complica -tion (39.1%). Seven (30.4%) were transient, six patients required treatment for a maximum of three days, and one for one year prior to resolution. Two patients (8.7%) had permanent diabetes
Table 4. Immunohistochemistry investigation of the lesion in 23 patients.
Variable n (%)
Normal gland tissue 1 (4.3)
Adenoma with immunohistochemistry
expression for GH 9 (39.1)
Adenoma with immunohistochemistry
expression for GH and PRL 8 (34.8)
Adenoma with immunohistochemistry
expression for GH and ACTH 2 (8.7)
Adenoma with immunohistochemistry
expression for GH, PRL and ACTH 1 (4.3)
Adenoma with immunohistochemistry
expression for GH, PRL and TSH 1 (4.3)
Adenoma with immunohistochemistry
expression for GH, ACTH, TSH, FSH and LH 1 (4.3)
GH: growth hormone; PRL: Prolactin, ACTH: Adrenocorticotropic hormone, TSH: thyroid-stimulating hormone, FSH: Follicle-stimulating hormone, LH: Luteinizing hormone
Table 1. Clinical manifestations in 23 patients with acromegaly.
Variable n (%)
Effects of GH / IGF-1 excess
Acral enlargement 23 (100)
Facial changes 17 (73.9)
Increased genitalia 1 (4.3)
Direct effects of tumor
Visual disturbance 12 (52.2)
Headache 11 (47.8)
Diplopia 1 (4.3)
Osteoarticular manifestations
Bone and joint pain / carpal tunnel syndrome 11 (47.8) Respiratory manifestations
Obstructive sleep apnea 3 (13)
Deepening of the voice 6 (26.1)
Cutaneous manifestations
Hyperhidrosis 9 (39.1)
Diabetes mellitus 13 (56.5)
Hypertension 9 (39.1)
Dyslipidemia 5 (21.7)
Others endocrine manifestations
Amenorrhea 8 (34.8)
Sexual dysfunction / decreased libido 6 (26.1)
Galactorrhea 4 (17.4)
Colonic disease
Hyperplastic polyps / diverticula 5 (21.7)
Hormonal disorders
Hyperprolactinemia 10 (43.5)
Hypogonadism 7 (30.4)
Hypothyroidism 5 (21.7)
Hypocortisolism 4 (17.4)
Panhypopituitarism 4 (17.4)
Hyperparathyroidism (NEM1) 1 (4.3)
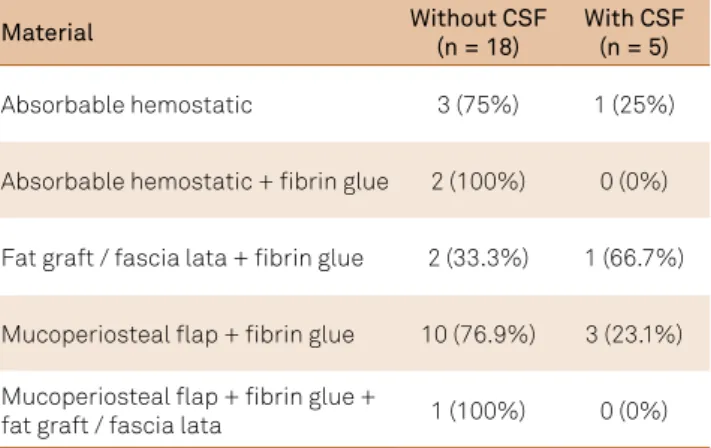
insipidus. Five patients (21.7%) developed cerebrospinal luid (CSF) leaks; three were treated successfully with external lum -bar drainage and two required a new approach to close the sella with a mucoperiostal lap, fat graft, fascia lata and ibrin glue. he correlation of the development of CSF leaks and the mate -rial used to close the sella is shown in Table 5. Four patients (17.4%) had otorhinolaryngologic complications; three of them had epistaxis, two were controlled with only nasal tampons, and one with a nasal catheter and nitroprusside. One patient had transient cacosmia. Two patients (8.7%) developed new panhy-popituitarism. Postoperative meningitis was seen in one patient (4.3%), who had also sufered a CSF leak. he most severe complication was an ischemic stroke of the basal ganglia that occurred in one (4.3%) patient who was submitted to a trans -cavernous sinus approach with extensive manipulation of the carotid artery. his was associated with postoperative pneumo -nia, hemiparesis and dysphagia. here were no mortalities dur -ing the follow-up.
he postoperative complications of three patients submit -ted to a second transsphenoidal surgery was one case (33.3%) of meningitis and one (33.3%) of permanent diabetes insipidus. Panhypopituitarism persist in two of these patients.
Remission rate based on tumor extension and preoperative hormonal levels
he endocrinological remission rate was 39.1% for all tumors. he best results were achieved for microadenomas, with 100% of disease control. For macroadenomas, remission was obtained in seven patients (33.3%). he postoperative MRI showed total tumor resection in eight patients (34.8%) and residual tumor was identiied in 15 patients (65.2%), one of which had no cor -relation with biochemical levels. Remission and non-remis -sion groups are compared according to adenoma character-istics in Table 6. For statistical analysis, tumors were grouped into non-invasive (microadenomas and sellar macroadenoma), invasive in only one compartment (sellar macroadenoma with suprasellar extension or invasion of the cavernous sinus), and invasive in more than one compartment (sellar macroade-noma with suprasellar extension and cavernous sinus invasion). A meaningful statistical correlation was found between the tumor extension and persistent disease. he highest degrees of invasion tend to be associated with a lower biochemical remis -sion rate (p = 0.015). It was also observed that the noninvasive tumors were associated with an increased probability of disease control when compared to invasive tumors (p = 0.017).
While preoperative IGF-1 serum levels did not show a statistically signiicant diference between patients who demonstrated remission and those who did not (respec-tively 622.3 ± 252.7 ng/ml [range 268–1178ng/ml] and 800.3 ± 154.2 ng/ml [range 607–1047 ng/ml]; p =0.08), preop -erative serum GH levels revealed a meaningful statistical dif-ference between biochemical remission and non-remission groups (respectively 8.6 ± 7.9 ng/ml [range 2.4–25.6 ng/ml] and 40.7 ± 41 ng/ml [range 2.7–151 ng/ml]; p = 0.01).
DISCUSSION
Serum GH excess is associated with high morbidity and mortality rates3,4,19,20. he current irst-line therapy for
acromegaly is gross total resection of the adenoma. It aims to reduce symptoms, relieve compressive efects, improve acromegalic features, reverse cardiovascular risk and restore life expectancy5,28.
he advantages ofered by the endoscopic technique3,21,22,28, which enables the use of diferent angles to operate, may facilitate resection of invasive lesions and, consequently, increase remission rate. However, the resection of adenomas in the cavernous sinus should be carefully considered due to the risk of neurovascular complications.
Long-term results of acromegalic patients submitted to endoscopic endonasal surgery are rarely reported in the lit-erature. In this study, the patients were followed on average for 46.9 months, much longer than published in recent stud -ies1,3,4,5,27. Only Wagenmakers et al.23 presented long term
fol-low-ups with a mean time of 56 months.
Remission rates after endoscopic endonasal transs -phenoidal surgery for GH-secreting pituitary adenomas vary broadly, from 28.8% to 74.6%1,3,5,11,18,23,28. he highest
Table 5. Correlation between the complication of CSF and material used to close the sella.
Material Without CSF
(n = 18)
With CSF (n = 5)
Absorbable hemostatic 3 (75%) 1 (25%)
Absorbable hemostatic + ibrin glue 2 (100%) 0 (0%)
Fat graft / fascia lata + ibrin glue 2 (33.3%) 1 (66.7%)
Mucoperiosteal lap + ibrin glue 10 (76.9%) 3 (23.1%)
Mucoperiosteal lap + ibrin glue +
fat graft / fascia lata 1 (100%) 0 (0%)
CSF: cerebrospinal luid.
Table 6. Tumor characteristics on MRI in remission and non-remission groups.
Variable Remission
(n = 9)
Non-remission (n =14)
Microadenoma 2 (100%) 0 (0%)
Macroadenoma
S 4 (66.7%) 2 (33.3%)
S + CS 2 (50%) 2 (50%)
S + SS 1 (20%) 4 (80%)
S + SS + CS 0 (0%) 6 (100%)
values were achieved using old criteria to deine a cure1,3,23. As shown in recent papers, the best results were achieved in microadenomas (56–100%) compared to macroadenomas (27–71.7%)1,4,18,28. he worst outcomes were related to supra -sellar and para-sellar lesions. herefore, the overall remission rate of 39.1% found in this study and the better remission rate for the microadenomas (100%) rather than macroadenomas (33.3%) were expected.
Recent literature has suggested some helpful predic -tors for tumor gross resection and endocrine remission are tumor size3,4,5,11,28, extension of the lesion1,3,4,5,11,28 and
hormonal levels4,23,28.
Concerning tumor extension, Campbell et al.3 and
Buliman et al.4 evidenced that Knosp grades 3 or 4 were
less likely to achieve remission. Univariate analysis of Sarkar et al.28 demonstrated that absence of cavernous
sinus invasion and suprasellar extension were prognos-tic factors. While Gondim et al.1 associated higher levels
of suprasellar/parasellar extension and sella floor erosion with lower disease control (p = 0.01 and p = 0.02, respec-tively), Bunderen et al11.analysis reached borderline sig
-nificance levels, suggesting that parasellar and infrasellar extension tend to be independent predictors of persistent disease. On the other hand, in the study by Wagenmakers et al.23, an invasive tumor did not have significant influ-ence on the remission rate. It was observed in this study that the absence of suprasellar or cavernous sinus inva -sion were signs of a good prognosis, and there was a ten-dency for a lower rate of remission, the higher the degree of tumor invasion.
Additionally, a significant correlation was observed between preoperative GH serum levels and the endocri -nological outcome. Univariate analysis of Sarkar et al.28 established that preoperative GH levels below 40 ng/ml are independent prognostic factors. Buliman et al.4 also
noticed lower GH levels among patients with complete hormonal remission rates. However, there are other stud-ies that indicate no significant difference in preopera-tive GH levels between patients who achieved remission
and those who did not3,5. Our results are comparable to
Sarkar et al.28 and Buliman et al.4, revealing a
statisti-cally meaningful influence in this hormone level and the remission rate (p = 0.01). In our study, preoperative IGF-1 serum levels did not differ significantly between remis -sion and non-remis-sion groups (p = 0.08), which is in con-cordance with Buliman et al.4, Wangenmakers et al. 23 and
Sarkar et al.28.
In this study, the postoperative complication rate was 56.5%, including one major complication (ischemic stroke). his result is signiicantly higher than observed in recent papers1,3,4,5,11,18,23,28, probably due to the greater prevalence of
macroadenomas with extrasellar extension (65.2%) in our cohort (Figure 1). Large suprasellar and parasellar extensions with invasion of cavernous sinus may add a signiicant risk of complications to the procedure.
Transient diabetes insipidus occurred in seven patients (30.4%), which is just comparable with the 37.5% rate of Wangenmakers et al.23; in others studies this percent
-age varied from 3.3% to 9.1%1,3,4,18,28. Permanent diabetes
insipidus occurred in two patients (8.7%), which is a little higher than the 6.7% found by Bunderen et al.11 and our
own previous experience18. Five patients (21.7%) devel-oped CSF leak and two (8.7%) develdevel-oped panhypopituita -rism, which is in concordance with a variation of 0% to 34.8%1,3,4,5,11,18,23,28 and 8.3% to 18.2%5,28, respectively, shown
in recent literature. Wangenmakers et al.23 described sim
-ilar epistaxis rates to our study (13% and 10%, respec-tively). No patient experienced decreased visual fields or acuity after surgery, while five (41.7%) patients presented with improvement.
In conclusion, the endoscopic transsphenoidal approach is a safe and effective technique to con-trol GH-secreting pituitary adenomas as seen after a long-term follow-up. The transcavernous approach may add a higher risk of complications to the procedure. Tumors with suprasellar extension associated with cav-ernous sinus invasion may impair the total resection of these tumors and disease control.
A
B
References
1. Gondim JA, Almeida JP, Albuquerque LAF, Gomes E, Schops M, Ferraz T. Pure endoscopic transsphenoidal surgery for treatment of acromegaly: results of 67 cases treated in a pituitary center. Neurosurg Focus. 2010;29(4):E7. https://doi.org/10.3171/2010.7.FOCUS10167 2. Melmed S. Acromegaly pathogenesis and treatment. J Clin Invest.
2009;119(11):3189-202. https://doi.org/10.1172/JCI39375 3. Campbell PG, Kenning E, Andrews DW, Yadla S, Rosen M, Evans JJ.
Outcomes after a purely endoscopic transsphenoidal resection of growth hormone-secreting pituitary adenomas. Neurosurg Focus. 2010;29(4):E5. https://doi.org/10.3171/2010.7.FOCUS10153
4. Buliman A, Tataranu LG, Ciubotaru V, Cazac TL, Dumitrache C. The multimodal management of GH-secreting pituitary adenomas: predictive factors, strategies and outcomes. J Med Life. 2016;9(2):187-92. 5. Hofstetter CP, Mannaa RH, Mubita L, Anand VK, Kennedy JW,
Dehdashti AR et al. Endoscopic endonasal transsphenoidal surgery for growth hormone-secreting pituitary adenomas. Neurosurg Focus. 2010;29(4):E6. https://doi.org/10.3171/2010.7.FOCUS10173 6. Giustina A, Barkan A, Casanueva FF, Cavagnini F, Frohman
L, Ho K et al. Criteria for cure of acromegaly: a consensus statement. J Clin Endocrinol Metab. 2009;85(2):526-9. https://doi.org/10.1210/jcem.85.2.6363
7. Giustina A, Chanson P, Bronstein MD, Klibanski A, Lamberts S, Casanueva FF et al. A consensus on criteria for cure of acromegaly. J Clin Endocrinol Metab. 2010;95(7):3141-8. https://doi.org/10.1210/jc.2009-2670
8. Melmed S, Colao A, Barkan A, Molitch M, Grossman AB, Kleinberg D et al. Guidelines for acromegaly management: an update. J Clin Endocrinol Metab. 2009;94(5):1509-17. https://doi.org/10.1210/jc.2008-2421 9. Gondim JA, Ferraz T, Mota I, Studart D, Almeida JP, Gomes E et al.
Outcome of surgical intrasellar growth hormone tumor performed by a pituitary specialist surgeon in a developing country. Surg Neurol; 2009;72(1):15-9. https://doi.org/10.1016/j.surneu.2008.02.012 10. Gondim JA, Schops M, Almeida JP, Albuquerque LA,
Gomes E, Ferraz T et al. Endoscopic endonasal transsphenoidal surgery: surgical results of 228 pituitary adenomas
treated in a pituitary center. Pituitary. 2010;13(1):68-77. https://doi.org/10.1007/s11102-009-0195-x
11. Bunderen CC, Varsseveld NC, Baayen JC, Furth WR, Aliaga ES, Hazewinkel MJ et al. Predictors of endoscopic transsphenoidal surgery outcome in acromegaly: patient and tumor characteristics evaluated by magnetic resonance imaging. Pituitary.
2013;16(2):158-67. https://doi.org/10.1007/s11102-012-0395-7 12. Laws ER. Surgery for acromegaly: evolution of the techniques
and outcomes. Rev Endocr Metab Disord. 2008;9(1):67-70. https://doi.org/10.1007/s11154-007-9064-y
13. Schmidt RF, Choudhry OJ, Takkellapati R, Eloy JA, Couldwell WT, LIU JK. Hermann Schloffer and the origin of transsphenoidal pituitary surgery. Neurosurg Focus. 2012;2:E5.
https://doi.org/10.3171/2012.5.FOCUS12129
14. Landolt AM. History of transsphenoidal pituitary surgery. In: Landolt AM, Vance ML, Reilly PL, editors. Pituitary adenomas. London: Churchill Livingstone; 1996. p. 307-14.
15. Rosegay H. Cushing’s legacy to transsphenoidal surgery. J Neurosurg. 1981;54(4):448-54. https://doi.org/10.3171/jns.1981.54.4.0448 16. Guiot A. Transsphenoidal approach in surgical treatment of pituitary
adenomas: general principles and indications in nonfunctioning adenomas. In: Kohler PO, Ross GT, editors. Diagnosis and treatment of pituitary tumors. Amsterdam: ExcerptaMedica, 1973. (International congress series, vol 303). p. 159-78.
17. Hardy J. Transphenoidal microsurgery of the normal and pathological pituitary. Clin Neurosurg. 1969;16:185-217.
18. Santos ARL, Fonseca Neto RM, Veiga JC,
Viana Junior J, Scaliassi NM, Lancellotti CL et al. Endoscopic endonasal transsphenoidal approach for pituitary adenomas. Arq Neuropsiquiatr. 2010;68(4):608-12. https://doi.org/10.1590/S0004-282X2010000400024 19. Melmed S, Casanueva F, Cavagnini F, Chanson P, Frohman LA,
Gaillard R et al. Consensus statement: medical management of acromegaly. Eur J Endocrinol. 2005;153(6):737-40. https://doi.org/10.1530/eje.1.02036
20. Trepp R, Stettler C, Zwahlen M, Seiler R, Diem P, Christ ER. Treatment outcomes and mortality of 94 patients with acromegaly. Acta Neurochir (Wien). 2005;147(3):243-51. https://doi.org/10.1007/s00701-004-0466-2
21. Dehdashti AR, Ganna A, Karabatsou K, Gentili F. Pure endoscopic endonasal approach for pituitary adenomas: early surgical results in 200 patients and comparison with previous microsurgical series. Neurosurgery. 2008;62(5):1006–15. https://doi.org/10.1227/01.neu.0000325862.83961
22. Nomikos P, Buchfelder M, Fahlbusch R. The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical ‘cure’. Eur J Endocrinol. 2005;152:379-87.
23. Wagenmakers MA, Netea-Maier RT, Lindert EJ, Pieters GF, Grotenhuis AJ, Hermus AR. Results of endoscopic transsphenoidal pituitary surgery in 40 patients with a growth hormone-secreting macroadenoma. Acta Neurochir (Wien). 2011;153 (7):1391-9. https://doi.org/10.1007/s00701-011-0959-8
24. Divitiis E, Cappabianca P, Cavallo LM. Endoscopic transsphenoidal approach: adaptability of the procedure to different sellar lesions. Neurosurgery. 2002;51(3):699-705.
25. Sheppard MC. Primary medical therapy for acromegaly. Clin Endocrinol. 2003;58(4):387-99. https://doi.org/10.1046/j.1365-2265.2003.01734.x 26. Micko ASG, Wöhrer A, Wolfsberger S, Knosp E. Invasion
of the cavernous sinus space in pituitary adenomas: endoscopic veriication and its correlation with an MRI-based classiication. J Neurosurg. 2015;122(4):803-11. https://doi.org/10.3171/2014.12.JNS141083
27. Sullivan KM, Dean A, Soe MM. OpenEpi: a web-based epidemiologic and statistical calculator for public health. Public Health Rep. 2009;124(3):471-4. https://doi.org/10.1177/003335490912400320