REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Prevalence
of
burnout
syndrome
among
anesthesiologists
in
the
Federal
District
夽
Edno
Magalhães
a,∗,
Áurea
Carolina
Machado
de
Sousa
Oliveira
b,
Catia
Sousa
Govêia
a,
Luis
Cláudio
Araújo
Ladeira
a,
Daniel
Moser
Queiroz
b,
Camila
Viana
Vieira
baCentrodeAnestesiologiadaFaculdadedeMedicinadaUniversidadedeBrasília,Brasília,DF,Brazil bHospitalUniversitáriodeBrasília(HUB),Brasília,DF,Brazil
Received11February2013;accepted16July2013
Availableonline22November2014
KEYWORDS
Burnout/epidemiology; Jobsatisfaction; Worker’s
health/statisticsand numericaldata; Anesthesiology
Abstract
Background: Burnoutsyndromeisaresultofchronicstress,characterizedbyemotional exhaus-tion,depersonalization,andasenseoflowprofessionalaccomplishment.Itaffectsworkers underextremeresponsibilityorthosewhocareforindividualsatrisk,including anesthesiolo-gistswhodistancedthemselvesfromthework,patientsandcolleaguesbecausetheyfeelsafer inmaintainingindifference.
Objective:Toevaluatetheprevalenceofburnoutsyndromeandtheintensityofitscomponents andidentify thecharacteristics ofthosewith thesyndromeamong anesthesiologists inthe FederalDistrict.
Method: Across-sectionalstudywascarriedoutwith241anesthesiologistsenrolledinthe Soci-etyofAnesthesiologyoftheFederalDistrict.Aself-administeredquestionnairewasused,which includedtheMaslachBurnoutInventory,demographic,professional,andleisuredata.
Results:Of the 134 completed questionnaires (55.8%), there was a predominance ofmale (65.6%),aged30---50years(67.9%).Significantlowerlevelsofjobsatisfaction(47.7%), deper-sonalization(28.3%),andemotionalexhaustion(23.1%)werefound.Burnoutsyndromeshowed aprevalenceof10.4%,occurringmainlyinmen(64.2%),aged30---50years(64.2%),withover10 yearsofexperience(64.2%),workinginnightshifts(71.4%),sedentary(57.1%),andnottaking coursesunrelatedtomedicine(78.5%).Oftheparticipants,50.7%hadatleastoneofthethree criteriatodevelopthesyndromeandonly8.2%havealowrisktomanifestit.
夽
StudyconductedatCentrodeAnestesiologiaofFaculdadedeMedicinadaUniversidadedeBrasília(UnB).
∗Correspondingauthor.
E-mail:[email protected](E.Magalhães).
http://dx.doi.org/10.1016/j.bjane.2013.07.016
Conclusion: TheprevalenceofburnoutisrelevantamonganesthesiologistsintheFederal Dis-trict.Itisadvisabletoseekstrategiesforlaborrestructuringtoreducestressfactorsandloss ofmotivationandincreasejobsatisfaction.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE Esgotamento profis-sional/epidemiologia; Satisfac¸ãono
emprego; Saúdedo traba-lhador/estatísticae dadosnuméricos; Anestesiologia
PrevalênciadesíndromedeburnoutentreosanestesiologistasdoDistritoFederal
Resumo
Justificativa: A síndrome de burnout (queimar até a exaustão), consequência do estresse crônico, caracteriza-se por exaustão emocional, despersonalizac¸ão e sentimento de baixa realizac¸ãoprofissional.Acometetrabalhadoressobextremaresponsabilidadeouqueassistem indivíduossobrisco,incluindoanestesiologistas.Podemapresentardistanciamentoemrelac¸ão aotrabalho,pacientesecolegas,porsentirem-semaissegurosaomanteraindiferenc¸a.
Objetivo: Avaliaraprevalênciadasíndromedoesgotamentoprofissional,aintensidadedeseus componenteseidentificarcaracterísticasdosseusportadoresentreanestesiologistasdoDistrito Federal.
Método: Estudotransversal,com241anestesiologistasinscritosnaSociedadedeAnestesiologia doDistritoFederal.Usou-sequestionárioautoaplicávelqueincluiuoInventáriodeBurnoutde Maslach,dadossociodemográficos,profissionaisedelazer.
Resultados: Dos134questionáriosrespondidos(55,8%),forampredominantesospreenchidos porhomens (65,6%),comfaixade30a50anos(67,9%).Foramencontradosníveis significa-tivosdebaixarealizac¸ãoprofissional(47,7%),despersonalizac¸ão(28,3%)eexaustãoemocional (23,1%).Asíndromedeburnoutapresentouprevalênciade10,4%,ocorreuprincipalmenteem homens(64,2%),nafaixade30a50anos(64,2%),commaisdedezanosdeprofissão(64,2%), comatuac¸ãoemplantõesnoturnos(71,4%),sedentários(57,1%)equenãofazemcursosnão relacionadosàmedicina(78,5%).Dosparticipantes,50,7%apresentarampelomenosumdetrês critériosparadesenvolverasíndromeeapenas8,2%têmbaixoriscoparasuamanifestac¸ão.
Conclusão:Aprevalênciadasíndromedeburnoutérelevanteentreosanestesiologistasdo Dis-tritoFederal.Éaconselhávelbuscarestratégiasdereorganizac¸ãolaboralparadiminuirfatores deestresseeperdadamotivac¸ãoeaumentarasatisfac¸ãonoemprego.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
BurnoutsyndromewasfirstdescribedbyFreudenbergerin 1974 as staff burnout.1 Its occurrence becomes the way
found bytheindividualtocope,although inappropriately, withtheoccupationalstress chronicity.Thischronicstress psychologicallyderangestheprofessionalforcinghimtouse extraenergyresourcesandinhibitingtheactionsnecessary todealwiththissetting.2,3Thesyndromeariseswhenother
strategiesfailtodealwithstress.4,5Dependingonthe
inten-sity andduration of thisstatus, theindividual maysuffer serious consequences, both physical and psychological, if hecannotrestoretheprevioussettingordevelopadaptive mechanismstorestorethelostbalance.
Currently, the most widely used definitionis that pro-posed in 1986 by Maslach andJackson, in that emotional exhaustion is referred to as a syndrome consisting of threedimensions: emotional exhaustion, dehumanization, andlow personalaccomplishmentat work.The emotional exhaustion dimension is characterized by the sense of
emotionalandphysicalexhaustion.Itistherealizationthat thereisnoenergylefttocarryoutworkactivities.Thedaily lifeatworkbecomesarduousandpainful.2,3
Depersonalizationisrevealedthroughattitudesof emo-tionaldetachment from people towhom the professional shouldcareforandcoworkers.Thecontactsbecome imper-sonal, devoid of affection, andinhuman. Sometimes, the individualbeginstoshowharsh,cynicalorironicbehaviors. Thisdimensionisconsideredthedefensiveelementofthe syndrome.2,3
Personal achievement in occupational tasks decreases andthe individual loses thesatisfaction andefficiency at work. There is a feelingof personal dissatisfaction, work losesmeaningandbecomesaburden.2,3
Socio-psychologicalconceptionshowstheexistenceof mul-tidimensionalfactors,suchasnegative,cynical,cold,and impersonal interaction with service users, including the declineofidealismandindifferencetowhatmighthappento others.Theorganizationalandsocio-historicalperspectives reflect the labor organization influence on the syndrome development.6---9
Several authors recognize the importance of the role playedbylabor,aswellastheimplicationsofsocialand rela-tionaldimensioninthesyndromedevelopment.Ingeneral, anyactivitycantriggeraprocessofemotionalexhaustion. However, some occupations are more likely to have the peculiarcharacteristicsofthesyndrome.Occupationswhose activities have emotional involvement are considered at higherriskforburnoutsyndrome,especiallythosewhowork directlywithotherpeople,assistingthemorasresponsible for their development and well being. Therefore,people whoarededicatedtoteaching,nursing,medicine, psychol-ogy,and policing areconsidered more predisposedtothe syndrome.4,5,10,11
MaslachandLeiterreportthat‘‘accordingtothenature and functionality of the occupation, there are risk and high-riskoccupations,withfewbeinglow riskfor burnout syndrome’’.Anesthesiology is considered a specialty that promotes high levelsof stress and mayresult in negative consequences for those who practice it. Therefore, it is classifiedashighrisk.3,6,10
TheFederal District,whosecurrent populationisabout 2.5million,has391anesthesiologistsregisteredatthelocal anesthesiologysociety(Sadif).Therearenoreportsofthe burnout syndrome prevalence among anesthesiologists in thatregion.
Theaimofthisstudywastoevaluatetheprevalenceof burnout syndromeamong anesthesiologistsof the Federal Districtandcharacterizetheintensityofitscomponents.As asecondaryobjective,wedescribethespecific characteris-tics,suchasweeklyworkinghours,agegroup,gender,and timeofpracticeofthestudysample.
Method
A quantitative descriptive cross-sectional study was approved by the Ethics Committee of the Faculdade de MedicinadaUniversidadedeBrasília.The sampleincluded 241of the391anesthetistsregistered withtheSociety of AnesthesiologyoftheFederalDistrict,evaluatedfromMarch toJune,2011.
For data collection, a standardized, self-administered questionnaire wasused, consisting of two parts: the first partconsistedofdemographicdatasuchasage,sex, mari-talstatus,presenceofchildreninthefamily,andacademic training. Professional data were also evaluated, as well asthenumberandtypeof employmentcontracts,weekly workinghours,nightshifts,jobpositions,andvacations,in additiontodataonleisureandpersonalhabits,suchas phys-icalactivity,courses,smokinganddrinkinghabits,andillicit druguse.Thesecondpartofthequestionnaireincludedthe MaslachBurnoutInventory(MBI),astandardtoolfor study-ingthesyndrome.Itisthemostwidelyusedquestionnaire, alreadytranslated,adapted, andvalidated inBrazil, with 22questions.Thequestionsfrom1to9identifythelevelof
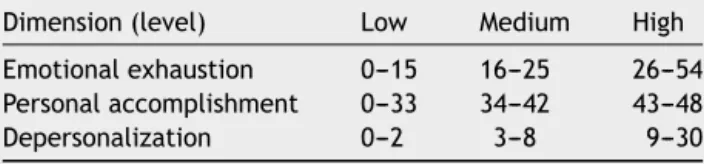
Table 1 Values of the Maslach Burnout Inventory (MBI) scale developed by the Center of Advanced Studies on BurnoutSyndrome.11
Dimension(level) Low Medium High
Emotionalexhaustion 0---15 16---25 26---54
Personalaccomplishment 0---33 34---42 43---48
Depersonalization 0---2 3---8 9---30
emotionalexhaustion,from10to17arerelatedtojob satis-faction,andfrom18to22arerelatedtodepersonalization. ThescoreoftheitemssurveyedbyMBIfollowstheLikert scale,rangingfrom0to6,thatis,from‘‘never’’to‘‘every day’’. For MBI data analysis, the sum of each dimension was performed (emotional exhaustion, depersonalization, and personal accomplishment).The valuesobtained were comparedwiththeCenterforAdvancedStudiesonBurnout Syndrome(Nepasb)11 referencevalues(Table1).
The risk for developing the syndrome was determined afteranalysisofalldimensions.AccordingtoMBI,the prin-cipleforthediagnosisofburnoutistheclassificationofhigh scoresfor theemotionalexhaustionanddepersonalization dimensionsandlowscoresfortheprofessionalachievement dimension. Therefore,the meetingof these three dimen-sional criteria by the professional indicates the burnout syndromemanifestation, andthepresence oftwocriteria determine high risk for itsdevelopment.The other items evaluatedin thefirstpart ofthe questionnairewere ana-lyzedusingpercentages.
Results
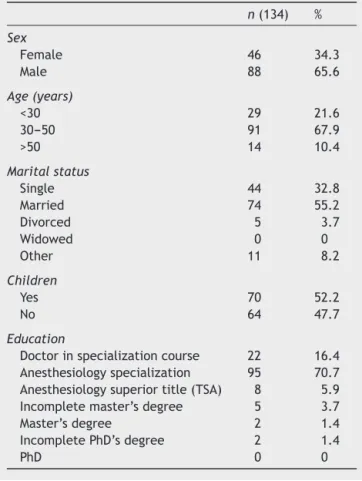
The questionnaire was delivered to 241 professionals enrolled in the Society of Anesthesiology of the Federal District. The final sample consisted of 134 anesthesiolo-gists, corresponding to 55.6% adherence, as 107 did not respondtothequestionnaire.Analysisofdemographicdata showed that there wasa predominance of male (65.6%), aged 30---50 years(67.9%), married (55.2%), with children (52.3%),andmostwiththetitleofspecialistin anesthesi-ology(TEA)(55.9%).Medicalspecialistsrepresented16.1% (Table 2). Regarding the sample professionaldata, it was found that most had fewer than fiveyears of experience in the specialty (41%), up to two centers of professional activity(52.2%),61---84hweeklyworking(44.1%),andnight shift(83.5%).About12%occupyaleadingpositionand88% hadvacationinthepreviousyear(Table3).Dataonleisure revealedregularphysical activityin61.1%andattendance ofcoursesunrelatedtomedicineinonly17.1%.Lowratesof smokingandalcoholconsumption(5.9%and18.6%, respec-tively)werefound.Therewerenoreportsofillicitdruguse (Table4).
Table 2 Sample distribution of DF anesthesiologists accordingtosocio-demographicdata.
n(134) %
Sex
Female 46 34.3
Male 88 65.6
Age(years)
<30 29 21.6
30---50 91 67.9
>50 14 10.4
Maritalstatus
Single 44 32.8
Married 74 55.2
Divorced 5 3.7
Widowed 0 0
Other 11 8.2
Children
Yes 70 52.2
No 64 47.7
Education
Doctorinspecializationcourse 22 16.4 Anesthesiologyspecialization 95 70.7 Anesthesiologysuperiortitle(TSA) 8 5.9 Incompletemaster’sdegree 5 3.7
Master’sdegree 2 1.4
IncompletePhD’sdegree 2 1.4
PhD 0 0
had highlevels of emotional exhaustion;there wasalow ratingofprofessionalachievementin47.7%,andhighlevel of depersonalizationin28.3%, characteristics thatset the diagnosis for the burnout syndrome manifestation or high riskforitsdevelopment(Table5).
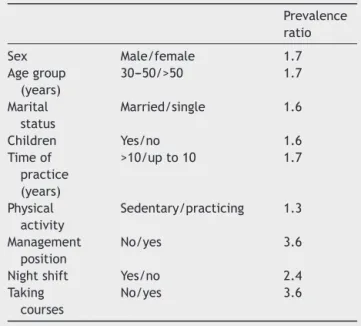
The burnout syndrome prevalence was 10.4% and occurredmainlyinmen(64.2%),aged30---50years(64.2%), with children (57.1%), and the following other features: title of specialist (42.8%), over 10 years in the pro-fession (64.2%), work in night shifts (71.4%), sedentary (57.1%), andnot attendingcoursesor activities unrelated tomedicine(78.5%).Theywerecharacterizedbythe preva-lence ratio (Table 6). There was no difference between married and unmarried (42.8% for both). No doctor in specialization course had burnout syndrome. Of the 134 participants, 50.7% had at least one of three criteria to develop the syndromeand only8.2% have low risk for its manifestation.
Discussion
Burnout is a response to chronic labor stress, involves significant behavioral changes in addition toits aggravat-ing sociodemographic, professional, leisure, and lifestyle habit variables.When the anesthesiologistis affected, he willtake actionsthataffect patients,colleagues,and the work itself, because the coping methods become inade-quate and flawed.4,6 Therefore, it is necessary to clarify
Table 3 Sample distribution of DF anesthesiologists accordingtoprofessionaldata.
n(134) %
Timeofpractice(years)
<5 55 41
5---10 23 17.2
11---15 18 13.4
16---20 14 10.4
>20 24 17.9
Numberofjobs
Upto2 70 52.2
Morethan2 64 47.7
Typeofemployment
Privateservice 9 6.7
Statutorypublic 24 17.9 Temporarypublic 23 17.1 Morethanonetype 78 58.2
Weeklyworkload
Upto60h 47 35.1
60---80h 59 44
Over80h 28 20.9
Nightshift
Yes 112 83.5
No 22 16.4
Managementposition
Yes 16 11.9
No 118 88
Vacationinthepreviousyear
Yes 118 88
No 16 11.9
Table 4 Sample distribution of DF anesthesiologists accordingtoleisureandpersonalhabitdata.
n(134) %
Courses(outsidethemedicalfield)
Yes 23 17.1
No 111 82.8
Physicalactivity
Yes 82 61.1
No 52 38.8
Smokinghabit
Yes 8 5.9
No 126 94
Alcoholism
Yes 25 18.6
No 109 81.3
Illicitdrugs
Yes 0 0
Table5 PrevalenceoftheMaslachBurnoutInventory(MBI) dimensions.
Dimension(level) Low Medium High
Emotionalexhaustion 45.5% 31.3% 23.1% Personalaccomplishment 47.7% 38.8% 13.4% Depersonalization 23.1% 48.5% 28.3%
the emotional exhaustion amonganesthesiologists and its correlations.
The surveywas conducted with 55.6% participation of anesthesiologistsinterviewedattheAnesthesiologySociety ofFederalDistrict(Sadif),asignificant numberof respon-dents, which was 35% higher than the acceptable.12 The
profileofSadifanesthesiologistsisayoung,predominantly malepopulation,withless than 10years ofpractice,and mostlywithatitleofspecialistinanesthesiology.
Earlyresearchonthesyndromebeganfocusingonrelated issues,suchastheemotionthatoccursintheworkplace,and notasemotionalexhaustion.Thesetofsubsequentresearch wasmore systematic in evaluatingpsychological burnout, partofaresearchprogramtodevelopapsychometrictoolof standardizedmeasure.Thus,theMBIthatevaluatesallthree dimensionsofthesyndromeandisconsideredthestandard investigationtoolwasdeveloped.6,11
The most affected dimension in the sample was pro-fessionalachievement, whichwaslowin 47.7%,similarto theAustralianstudy byKluger etal., inwhich the preva-lenceof low jobsatisfaction was36%.13 This may bedue
tothefeelingofoverloadbytheindividualfor performing activitiesthatgobeyondhisability.Sometimesthestaffis reducedcomparedtothedemandfor activitiesand work-load.Thisrelationshipmaybeinfluencedbythehealthcare modeladopted in surgical centers,which generates over-headmovement and occupationalstress. Consideringthat
Table6 Associationmeasuredbythemainvariable preva-lenceratioinanesthesiologistsdiagnosedwithburnout.
Prevalence ratio
Sex Male/female 1.7
Agegroup (years)
30---50/>50 1.7
Marital status
Married/single 1.6
Children Yes/no 1.6
Timeof practice (years)
>10/upto10 1.7
Physical activity
Sedentary/practicing 1.3
Management position
No/yes 3.6
Nightshift Yes/no 2.4 Taking
courses
No/yes 3.6
theneedtotakeimmediateandeffectivedecisionsis con-stant,thismayleaveanesthesiologistswiththefeelingthat theworkisnotrewarding.7,14
Inthepresentstudy,10.4%ofrespondentsinFederal Dis-trict hadburnout,aprevalencesimilartootherclasses of professionals also considered at high risk, but with some differences between the evaluated variables. According to some authors, the lower tendency for burnout among physicians in intensive care and oncology is attributed to the marriage or stable union and the fact of having children.12,15Inthissample,thesyndromewasmore
preva-lent in men (64.2%) with children (55.6%) and there was nodifference betweenthe maritalstatuses. We observed a higher prevalence (78.5%) in professionals who do not take courses outside the medical field, which suggests that the practice of this activity can promote stress relief.
Another feature seen in this study was the predomi-nant age group for burnout syndrome, between 30 and 50 years (64.2%). This may suggest that the profession-als withlowerriskforburnout arethosewithprofessional maturity and greater control of their emotions in stress-ful situations.14,16 The syndrome’s higher prevalence in
professionals who do not exercise management positions (78.5%)alsodrawsattention.Theseelementssuggest that authority, support from colleagues, and job satisfaction may be protective factors, which corroborates a study conducted in Austria.17 Furthermore, the higher
preva-lence of the syndrome in professionals with exclusively statutory publicemployment (50%)may indicatethe pub-lic service lack of working conditions as a potential risk factor.
Apeculiarity of the Federal District, notalways found in other Brazilian regions, should be emphasized. Over 95% of anesthesiologists in the region work exclusively in anesthesiology,becauseofthelargenumberofposts avail-able for this specialty in regional public hospitals. Many professionals work in more than one hospital, but always in the same specialty. Thus, we can assume that in this sample, theelementsrelatedtootheroccupational activ-itiesdidnotaffecttheoccurrenceofsymptomsrelatedto burnout.
Among anesthesiologists, certain factors may be deci-sive in the development of burnout syndrome. Limitation oftimeisreportedasoneofthemostcommonreasonsfor stressamonganesthesiologists,duetotheconstantpressure tomeetschedules, performproceduresquickly,and move betweenhospitals.8,9Thefactorsthatcontributetothe
professionalonthepartofhealthplansmayalsocontribute asadeterminant.18
There is also the physical stress that results from exhaustingfactorsofsurgicalenvironment,includingnoise pollution, exposure to anesthetic gases, radiation, latex, infections, excessive cold or heat, use of uncomfortable chairs, and even the limited space. Noise overload leads to sympathoadrenal activation in normal people and this response is increased in individuals with chronic anxiety and/or hypertension.7 The noise in the operating rooms
maybe enough tocausehyperactivity ofthe sympathetic nervous system and cognitive and psychological effects. Another important factor is sleep deprivation, because anesthesiology is a specialty that has to provide con-tinuous services to patients. There is also the need to be available 24h a day throughout the year and the need to work in night shifts for appropriate coverage of scales on duty. All these factors result in fatigue and exhaustion.7,13,16,19
As in previous studies, the syndromewas more preva-lent in professionals who work in night shifts, because the sleepand fatigue resulting fromnight work generate lack of agility and attention, slowness of cognitive func-tion and reflexes, in addition to making the individual more impatient witheveryday activities. Thus, adequate rest is an additional factor of safety and well being in anesthesiology, whose priority is safety. The personal characteristics mentioned above are not individual trigg-ers of the phenomenon, but facilitators of the action of stressors.4,14
Thisstudyisthefirsttoprovideaprofileof anesthesiol-ogistsin theFederal Districtandtoassesstheprevalence ofburnoutinthiscohort.However,ithassomelimitations. It is a cross-sectional study that examines the exposure-disease relationship in a given population or sample at a particular moment. It provides a picture of how the variablesarerelatedinthatparticular moment,but with-outestablishingacausalconnection.Multivariateanalyzes were also not carried out, which are important to reach definitiveconclusions.20 Thecharacterizationofalcoholism
was flawed because the weekly frequency and the num-berof dosesper day werenotadequately detailedin the questionnaire.Furthermore,theuseofaself-administered questionnairecangeneratedifferencesininterpretationof thequestions.
Giventheseverityofburnoutconsequences,thehealth ofanesthesiologistsrequiresmoreattention.Fromthe orga-nizational standpoint, the work in the operating room generates an overload of movement and occupational stress. Aperiodic monitoringof theseprofessionals’ men-tal andphysicalhealth is recommendedtoreorganizethe work processand reduce the stress sources.Forthis pur-pose, thereareseveral strategiesall withthesame goal. The individual’s response to stress should be improved througheducation,seekingtolearnmethods todealwith the triggering factors.The occupational context improve-ment with a focus on management strategies is also recommended.Finally, theinteraction betweenthe occu-pational context and the individual and the combination of educational and administrative changes through psy-chological counseling in multidisciplinary teams is also important.5,17,19
Conclusion
Thehighprevalenceofburnout,aswellasthehighriskforits developmentamonganesthesiologistsoftheFederalDistrict wasdisclosed.The implementationof measurestomodify theseprofessionals’workconditionsandmotivationshould beconsidered.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WethankCristinaSousaGoveiafor herhelpintranslating themanuscript.Wealsothanktheparticipating anesthesi-ologistswhosharedtheirexperienceswithus.
References
1.FreudenbergerH.Staffburnout.JSocIssues.1974;30:159---65.
2.Maslach C, Jackson E. The measurement of experienced burnout.JOccupBehav.1981;2:99---113.
3.MaslachC,SchaufeliB,LeiterP.Jobburnout.AnnuRevPsychol. 2001;52:397---422.
4.NyssenA,HansezI.Stressandburnoutinanaesthesia.CurrOpin Anaesthesiol.2008;21:406---11.
5.GarrosaE,Benevides-PereiraAMT,JiménezBM,etal.Prevenc¸ão e intervenc¸ão na síndrome de burnout. In: Como prevenir (ouremediar)oprocessodeburnout.Benevides-PereiraAMT.
Burnout:quandootrabalhoameac¸aobem-estardotrabalhador. 4a
ed.SãoPaulo:CasadoPsicólogo;2002.p.227---72.
6.ShanafeltT,SloanJ,HabermannT.Thewell-beingofphysicians. AmJMed.2003;114:513---59.
7.SvensenE,ArnetzBB, UrsinH, etal. Healthcomplaints and satisfied withthejob?A cross-sectionalstudy onwork envi-ronment,jobsatisfaction,andsubjectivehealthcomplaints.J OccupEnvironMed.2007;49:32---41.
8.LarssonJ,RosenqvistI,HolmstromI.Enjoyingworkorburdened by it? How anaesthetists experience and handle difficul-ties at work: a qualitative study. Br J Anaesth. 2007;99: 493---9.
9.Pilau MM, Bagatini A, Bondan LG, et al. O anestesiolo-gista no Rio Grande do Sul. Rev Bras Anestesiol. 2000;50: 309---16.
10.ShanafeltT.Burnoutinanesthesiology---acalltoaction. Anes-thesiology.2011;114:1---2.
11.Tamayo M, Tróccoli B. Construc¸ão e validac¸ão fatorial da Escala de Caracterizac¸ão do Burnout (ECB). Estud Psicol. 2009;14:213---21.
12.SobrinhoCLN,BarrosDS,TironiMOS,etal.MédicosdeUTI ---prevalênciadasíndromedeburnout,características sociode-mográficas e condic¸ões de trabalho. Rev Bras Educ Méd. 2010;34:106---15.
13.Kluger MT, Townend K, Laidlaw T. Job satisfaction, stress, andburnoutinAustralianspecialistanaesthetists.Anaesthesia. 2003;58:339---45.
14.Ramirez AJ,GrahamJ, RichardsMA,et al. Mentalhealthof hospital consultants:theeffectsofstress andsatisfactionat work.Lancet.1996;347:724---8.
16.Fernández TB, Roldán PLM, Guerra VA, et al. Prevalence of burnout among anesthesiologists at Hospital Universitario Virgen Macarena de Sevilla. Rev Esp Anestesiol Reanim. 2006;53:359---62.
17.LedererW, KinzlJF, TrefaltE,et al.Significance ofworking conditionsonburnoutinanesthetists.ActaAnaesthesiolScand. 2006;50:58---63.
18.CarneiroAF. Síndrome de burnout em anestesia. Anest Rev. 2011;5:16---7.
19.CalumbiRA,AmorimJA,MacielCMC,etal.Avaliac¸ãoda quali-dadedevidadosanestesiologistasdacidadedoRecife.RevBras Anestesiol.2010;60:42---51.