REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SPECIAL
ARTICLE
Perineural
dexmedetomidine
effects
on
sciatic
nerve
in
rat
Abdulkadir
Yektas
¸
a,∗,
Murat
C
¸abalar
b,
Mehmet
Sar
b,
Ays
¸in
Alagöl
c,
Duygu
Sultan
C
¸elik
c,
Vildan
Yayla
b,
Deniz
Tolga
caBagcilarTrainingandResearchHospital,Istanbul,Turkey
bBakırköyDr.Sadikonuke˘gitimvearas¸tırmahastanesi, ˙Istanbul,Turkey
cBagcilarEgitimveArastirmaHastanesi,Istanbul,Turkey
Received20May2015;accepted17August2015 Availableonline28April2016
KEYWORDS Pawwithdrawal latencytesting; Analgesiameter; Sciaticnerve; Electromyography; Dexmedetomidine
Abstract Thepresentstudywasdesignedtotestthehypothesisthathighdose dexmedeto-midinewouldincrease thedurationofantinociceptiontoathermalstimulusinaratmodel of sciaticnerve blockade without causing nervedamage. The rats were anesthetized with isoflurane. Afterelectromyography(EMG)recordings,rightsciaticnerveswereexploredand perineuralinjectionsweredelivered:GroupD(n=7),40ggkg−1dexmedetomidine
admin-istration, Group II (n=6), (0.2mL) saline administration, Group III (n=2), only surgically exploration ofthe rightsciaticnevre. Timeto pawwithdrawal latency(PAW) toa thermal stimulusforbothpawsandanassessmentofmotorfunctionweremeasuredevery30minafter thenerveblockuntilareturntobaseline.Thecompound muscleactionpotential(CMAP)of rightandleftsciaticnerveswererecorded10timespereachnerveoncemoreafterperineural injectionsat14day.AfterEMGrecordings,rightandthepartofleftsciaticnervewereexcised atalengthofatminimum15mmforhistopathologicalexamination.Comparisonofright/left CMAPamplituderatiosbeforeand14daysaftertheprocedureshowedastatistically signifi-cantdifference(p=0.000).Therewerenodifferencesinperineuralinflammationbetweenthe GroupD,GroupS,andGroupEat14days.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeAnestesiologia. ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE Testesdelatênciade retiradadapata; Medidordeanalgesia; Nervociático;
Efeitosdedexmedetomidinaperineuralnonervociáticoemratos
Resumo Opresenteestudofoidesenvolvidoparatestarahipótesedequedexmedetomidina emdosealtaaumentariaadurac¸ãodaantinocicepc¸ãoaumestímulotérmicoemmodelode ratodebloqueiodonervociáticosemcausardanosaonervo.Osratosforamanestesiadoscom
∗Correspondingauthor.
E-mail:[email protected](A.Yektas¸). http://dx.doi.org/10.1016/j.bjane.2015.08.012
significativa(p=0,000).Nãohouvediferenc¸aseminflamac¸ãoperineuralentreosgruposD,Se Eaos14dias.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradeAnestesiologia. Este ´e um artigo Open Access sobuma licenc¸a CC BY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Peripheral nerve blocks are frequently used in surgical procedures targeted at post-operative pain and surgical anesthesia.Long-actinglocalanestheticsmayalsoprovide analgesia per se for 9---14h.1---4 If the block is performed
in the morning and afternoon, patients generally report post-operative pain at night hours. The need for opioid cause’sopioid-relatedpotentialsideeffectsandsuppression ofhealingsleep.5Using opioidsresultsinpotentialairway
obstruction,whichcausessaturationtodecrease.6---8Ideally,
single-timeperipheralnerveblockshouldprovideanalgesia duringthefirstpost-operativenight.
Interventions targetedincreasing thedurationof block inordertohealpost-operative painwithmany additional local anesthetics are under investigation. The efficacy of clonidine has been proven in many regional anesthetic techniques.9 However, long-acting local anesthetics have
producedresultsthatarenotveryimpressive.10,11Insome
studies, nobeneficialeffects of adding clonidine to long-actinganestheticshavebeenfound.11
Dexmedetomidine is a selective alpha-adrenoceptor agonist. A previously performed study showed that dexmedetomidine extends the sensorial and motor block timewhencombinedwithbupivacaine in ratmodelswith sciaticnerveblock.12
Studies indicated that local anesthetics result in myonecrosis;however,itisbelieved thatthedamagemay not be clinically important since the muscles are regen-erated in a normal way.13---16 Local anesthetic doses are
generallyreliableinhealthyhumanbeings;however,there mayreally be neurotoxicity present in patients with sub-clinical neuropathy diabetes or multiple sclerosis.17---19 An
increase ininflammatory mediators wasidentified follow-ingtheadministrationofperineuralclonidine.20---25 Astudy
reportedasignificantdecreaseinperineuralinflammationat 24hwiththeadditionofdexmedetomidinetobupivacaineas comparedwiththeadministrationofbupivacainealone.The samestudyfound thattheperineural inflammation values at 24h were higher as compared with the bupivacaine-only saline control group. The perineural inflammation
values of the group that received both bupivacaine and dexmedetomidine and the group that received only dexmedetomidine were similar to those of the saline group.26
As discussed in previous studies, it is believed that decreased perineural inflammation with the use of dexmedetomidine is due to decreased proinflammatory products of healing immune cells and increased anti-inflammatory cytokines at the wound site.20---25 It is very
important todetermine the functionalstatusesof nerves. Oneofthefunctionalevaluationmethodsforneuralhealing or transmissiondisorderis toperformelectrophysiological measurements. Electromyography is a commonprocedure inclinicalandfundamentalstudiesinthecontextofinvivo and invitro functional nervestudies. Ithas awidespread useintheelectro-diagnosticevaluationofperipheralnerve damageofthesciaticnerveinanimalmodels.Astudy per-formed showed thatthe useof a siliconetube filledwith hyaluronic acid following end-to-end repair of an incised nervecouldhaveapositiveeffectonlatencyandCMAP,and consequentlyonaxonal regeneration.27 CMAPisavaluable
parameter that generallyshows thetime aspect of nerve regeneration and reinnervation.28 A study demonstrated
thatstimulationsinglefiberelectromyography(SSFEMG)was amoresensitiveelectrophysiologicalmethodinthe detec-tionofneuromusculartransmissionblockthatoccursinrats withweakmusclesandacuteorganophosphatepoisoning.29
These electromyographic studies showed that both nerve healingandnervedamagecouldbeshownusing electromyo-graphicmethods.Inourstudy,wedeterminedtheeffectsof dexmedetomidineinjectiononneuraltransmissionbyusing electromyographicmethods.
Weconductedthisstudyinordertoassesstheeffectsof dexmedetomidineonsciaticnervesofratsthrough analges-imetry,histopathologyandelectromyography.
Method
Figure1 Inductionroom(PlexxModel:HNG6).
meeting issue 2012/60, number HADYEK/2012-13 held on 27.02.2012 by the Animal Experiments Local Ethics Com-mitteeofBa˘gcılarTeachingandResearchHospital,Bakırköy SecretariatGeneral oftheAssociation ofPublicHospitals, MinistryofHealthoftheRepublicofTurkey.Thisstudywas conductedinaccordancewiththeguidelinefortheuseand careoflaboratoryanimalsandtheguidelineforuseandcare ofmammalsinbehavioralstudiesconductedinthecontext ofneurologicalsciences.Duringthestudy,15maleratsof theSpragueDawleyspeciesweighing400---500gwereused. Drugpreparation:PrecedexIVvials(Abbott, Dexmedeto-midine hydrochloride 100g/mL) were diluted using
physiologicalsalinesolutionataratioof50g/mL.
Subfascialsciaticnerveinjection
Aftertheratswereweighed,theywereanesthetizedwith isoflurane2.5%intheinductionroom(PlexxModel:HNG6) (Fig.1), they wererested in right lateral decubitus posi-tionandisoflurane2.5%anesthesiacontinuedtobeprovided through a mask (Fig. 1). Lateral incision was performed on the leg to receive the injection. The superficial fas-ciawasseparatedandthesciaticnerve wasexposed at a pointproximaltothebifurcation(Fig.2).Afterthesciatic nerve exposure, dexmedetomidine 40g/kg was injected
in perineural space in Group D (n=7) and physiological salinesolutionat avolumeequal to40g/kg
dexmedeto-midine wasinjected inGroup S (n=6). 30GPPD injectors were used for injection. In Group E (n=2), only the sci-aticnervewasexposedanditwasclosedagain.The time ofinjectionadministrationwasrecorded.Todeterminethe sitewherenervesamplewouldbecollected,thefasciaof
Figure2 Thesuperficialfasciawasseparatedandthesciatic nervewasexposedatapointproximaltothebifurcation.
Figure3 PWLtest.
biceps femorismuscle corresponding tothe injectionsite was marked using non-absorbable sutures under the skin whileworkingontheskinpreparation.Thesutureswerenot placedaroundthenerveanddidnottouchthenerve.After theinjections weremade, theincisionfolds wereclosed. Theisofluraneanesthesiawasinterruptedandthetimeof anesthesiainterruptionwasrecorded;theratswereplaced intheircagesinasupineposition.Then,thetimeswhenrats returnedtopronepositionwererecordedasresumptionof rightingreflex(RoRR).
Pawwithdrawallatency(PWL)testing
Aftertheratsreturnedtoproneposition,aplantaranalgesia meter(Series8model336T,IITCLifeScienceInc.,Woodland Hills,CA)wasplacedintheplantaranalgesiameterchamber inordertoperformthePWLtest(Fig.3).Thesourceoflight wasusedasaheateratanalgesiameter.Afterthesourceof light wasturned on and the temperature at the point to whichtheratclawcorresponded reached 30◦C, awaiting
timeof 5min wasallowed, the rat clawwas moved toa pointcorrespondingthere.Thisprocedurewasrepeatedfor boththerightandleftpaws.
Figure4 Thepeaktopeakcompoundmuscleactionpotential (CMAP)anddistal motorlatency oftherightand left sciatic nerves.
Electrophysiologystudy
Aftertheratswereanesthetizedwithisoflurane2.5%,the tailsof ratsmadetorest insupinepositionwerefixed on theworking platform.Theneedleelectrodewasplacedin thegastrocnemiusmuscleandthesciaticnervewas stimu-lated10timeswithasurfaceelectrodeinasupramaxillary wayata suitablepoint proximaltothehipjoint(Fig.1). Thepeaktopeakcompoundmuscleactionpotential(CMAP) anddistalmotorlatencyoftherightandleftsciaticnerves wererecorded,respectively(Fig.4).For electrophysiolog-ical study, an electromyography system (Biopac systems, Inc., Model: MP150) was used and the software program LabChart7wasusedfortheassessmentofmeasurements. Thesameprocedurewasperformedafteradministrationof isofluraneanesthesiabeforeinjectiontothesciaticnerve and on Day 14 after the injection into the sciatic nerve beforecollecting asample fromthesciaticnerveandthe resultswerecompared.
Histopathologicalstudy
Onday14aftertheratswereanesthetizedwithisoflurane forthefirstelectrophysiologystudyanddruginjectioninto the sciatic nerve, the rats were anesthetized again with isofluraneandelectrophysiologystudywasperformed.The formerincisionsiteintherearrightextremitywasopened, themarkingsuturewaslocatedandasciaticnervesample of 1.5cm inlength was collectedfrom the corresponding site. The same procedure was repeated for the rear left extremity.Thenervesampleswerefixedfor3daysin glyc-eraldehyde2.5%andthenembeddedinparaffinblocksand cross-sectionsof5mwereprepared.Thesesampleswere
stainedwitheosinandevaluated.Thefollowingwere identi-fied:perineuralinflammationinthesciaticnerve(Figs.5---8) (0=noinflammation, 1=slightedemaand/orinflammation insmallfoci,2=moderateedemaand/orinflammationina locallywidearea,3=moderateedemaand/orinflammation indiffuseareas,localnervedamagefindings)(0=nolesions, 1=damagein1---2%ofaxonsormyelins,2=damagein2---5% ofaxonsormyelins,3=damageinmorethan5%ofaxonsor
Figure5 Microscopicimagesoftheperineuralinflammation level0.
Figure6 Microscopicimagesoftheperineuralinflammation level1.
myelins).After theremovalsciaticnerve, euthanasiawas performedonratsusingthecervicaldislocationmethod.
Statistics
Statistical calculationsweremadeusingthesoftware pro-gram SPSS 11.5 for Windows. Comparison of anesthesia
Figure8 Microscopicimagesoftheperineuralinflammation level3.
durations among groups, comparisons of RoRR values, histopathologicallyperformedinflammationandlocalnerve damagevaluesweremadeviatheNPartestsKruskal---Wallis test.Incaseswheretherewerestatisticallysignificant dif-ferences among groups, they were compared individually using the NPar tests Mann---Whitney U test. The rear and rightleftextremitybasalPWLvaluesandPWLvaluesat30, 60, 90, 120,150, 180, 210min andon days1---14 of each andeverygroupwerecomparedduringNParTestsWilcoxon SignedRankstest.TheCMAPandLatencyvalueswere com-pared using the ANOVA test among all threegroups. The comparison of electromyographic values before the drug administrationandonDay14afterthedrugadministration andthecomparisonofelectromyographicvaluesbeforeand afterdrugadministrationamongthegroupswereperformed usingthepaired-ttest.Thevalueofp<0.05wasconsidered statisticallysignificantforallthedata.
Results
When the durations of anesthesia provided while admin-istering injections torats werecompared,no statistically significantdifferenceswerefound(p=0.823)(Fig.9).
When the RoRR values of rats were compared as per thegroups, statisticallysignificantdifferenceswerefound amonggroups(p=0.005).Whenthegroupswerecompared individually,it was seen that the RoRR valuesin Group D werestatisticallysignificantlydifferentthantheothertwo groups and the RoRR values were longer as compared to the twoother groups (Group D---GroupS: p=0.003,Group D---GroupE:p=0.040)(Fig.10).
28 28.5 29 29.5 30 30.5
Ti
m
e
Group D Group S Group E
Groups
Seri 1
Figure9 Comparisonofdurationofanesthesiainthegroups.
0 20 40 60 80 100 120
RoRR Values
Group E Group S
Group D
Groups
Seri 1
Figure10 ComparisonofRoRRinthegroups.
0 5 10 15 20 25 30 35 40
210.Min 180.Min 150.Min 120.Min 90.Min 60.Min 30.Min Baseline
Time
PW
L
c
h
a
ng
es
Seri 1 Seri 2 Seri 3
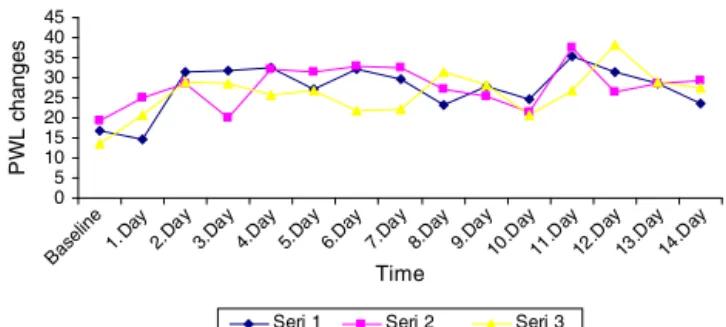
Figure11 Time-PWL changes intheright rear limb inthe groups(Seri1,GroupD;Seri2,GroupS;Seri3,GroupE).
InGroupD
WhentherearrightextremityPWLvaluesoftheratswere comparedwiththeirbasalvalues,itwasseenthatthePWL valueswerelowerthanthebasalvaluein30minafterdrug administrationandhigherin210min.Therewereno statis-ticallysignificantdifferencesamongvaluesmeasuredin60, 90,120,150and180min(p=0.018---p=0.237---p=0.237 ---p=0.735---p=0.499---p=0.091---p=0.028)(Fig.11).
WhentherearleftextremityPWLvaluesoftheratswere compared with their basal values, no statistically signifi-cant differences were observed in 60, 90, 120, 150, 180 and210min (p=0.044 --- p=0.138--- p=0.067 --- p=0.54 ---p=0.128---p=0.098---p=0.056)(Fig.12).
Whenthe rearrightextremityPWLvaluesofratswere comparedwiththeirbasalvalues,nostatisticallysignificant differenceswereseenonDays 1,8,9and14ascompared to the basal values; however, the PWL values were sta-tistically significantly longer on other days in comparison withthe basal values (1 Day: p=0.735; 2 Day: p=0.028;
0 5 10 15 20 25 30 35 40 45 50
210.Min 180.Min 150.Min 120.Min 90.Min 60.Min 30.Min Baseline
PWL
c
ha
nges
Time
Series 1 Series 2 Series 3
groupsafterinjection(Seri1,GroupD;Seri2,GroupS;Seri3, GroupE).
3Day:p=0.018;4Day:p=0.028; 5Day:p=0.043;6Day: p=0.018;7Day:p=0.028;8Day:p=0.128;9Day:p=0.063; 10Day: p=0.028;11 Day: p=0.018;12 Day:p=0.028; 13 Day:p=0.663;14Day:p=0.128)(Fig.13).
When the rear leftextremity PWL valuesof rats were comparedwith their basal values,it wasseen there was a statistically significant difference in terms of measure-ments taken on Days 4---6, 9---12 throughout 14 days and theywere longerthan the basal values (1Day: p=0.612; 2Day:p=0.018;3Day:p=0.063; 4Day:p=0.018;5Day: p=0.018;6Day:p=0.018;7Day:p=0.091;8Day:p=0.128; 9Day:p=0.028;10Day:p=0.125;11Day:p=0.028;12Day: p=0.018;13Day:p=0.028;14Day:p=0.063)(Fig.14).
Motorblockdidnotdevelop inanyoftheratsinGroup D.
InGroupS
WhentherearrightextremityPWLvaluesofratswere com-pared with their basal values, no statistically significant differenceswereobservedin30,60,90,120,150,180and 210min(Fig.11).
When the rear leftextremity PWL valuesof rats were comparedwiththeirbasalvalues,nostatisticallysignificant differenceswereobservedin30,60,90,120,150,180and 210min(Fig.12).
When therearrightextremityPWLvaluesofratswere compared with their basal values, there were significant differences on Days 4---7, 10, 11 and 14 and they were longerascompared tothe basalvalues (1 Day:p=0.345; 2Day:p=0.116;3Day:p=0.600; 4Day:p=0.046;5Day: p=0.046;6Day:p=0.028;7Day:p=0.028;8Day:p=0.075;
0 10 20 30 40 50 60 70 80 90
4.D ay 1.D
ay 2.D
ay 3.D
ay 5.D
ay 6.D
ay 7.D
ay 8.D
ay 9.D
ay 10.D
ay 11.D
ay 12.D
ay 13.D
ay 14.D
ay
Baseline
Time
PW
L
c
h
a
ng
es
Seri 1 Seri 2 Seri 3
Figure 14 Time-PWL changes in the left rear limb in the groupsafter injection(Seri1, Group D;Seri2, Group S;Seri 3,GroupE).
InGroupE
WhentherearrightextremityPWLvaluesofratswere com-pared with their basal values, no statistically significant differenceswereobservedin30,60,90,120,150,180and 210min(Fig.11).
When the rearleft extremity PWLvalues of rats were comparedwiththeirbasalvalues,nostatisticallysignificant differenceswereobservedin30,60,90,120,150,180and 210min(Fig.12).
Whentherearright extremityPWLvaluesof ratswere comparedwiththeirbasalvalues,nostatisticallysignificant differenceswereobservedonDays1---14(Fig.13).
When the rearleft extremity PWLvalues of rats were comparedwiththeirbasalvalues,nostatisticallysignificant differenceswereobservedonDays1---14(Fig.14).
NoratsdevelopedmotorblocksinGroupE.
Whentherightsciaticnervesofratswere histopathologi-callycompared,nostatisticallysignificantdifferenceswere seenamonggroupswithrespecttoinflammationandlocal nervedamagefindings(p=0.633---p=0.867).
Whentheleftsciaticnervesofgroupswere histopatho-logically compared, nostatistically significant differences wereseenamonggroupsintermsofinflammationandlocal nervedamagefindings(p=0.751---p=0.668).
WhentherightandleftnervesinGroupDwerecompared intermsofhistopathologicalresults,therewereno statis-ticallysignificantdifferencesintermsofinflammationand localnervedamage(p=0.891---p=0.705).
Whenthe rightand leftsciaticnerves in GroupS were comparedintermsofhistopathologicalresults,therewere nostatisticallysignificantdifferencesintermsof inflamma-tionandlocalnervedamage(p=0.194---p=0.317).
Whentheright andleftsciaticnerves inGroupE were comparedintermsofhistopathologicalresults,therewere nostatisticallysignificantdifferencesintermsof inflamma-tionandlocalnervedamage(p=1.000---p=0.317).
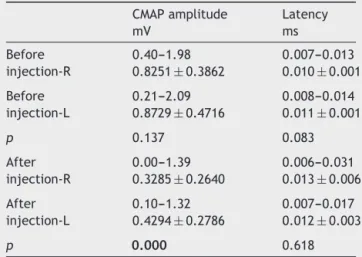
When the Group D, Group S and Group E were com-pared in terms of CMAP and latency values before and aftertheinjection,therewerestatisticallysignificant dif-ferencesintermsofpost-injectionCMAPvalues(p<0.001) (Table1).Therewerenostatisticallysignificantdifferences withrespecttolatencyvalues(p=0.618)(Tables1and2).
The post-injection CMAP measurements were statisti-cally significantlydifferentbetween Group Dand GroupS (p=0.016)
Table1 CMAPamplitudesandlatenciesofrightandleft sciaticnervesbeforeand14daysafterinjection.
CMAPamplitude mV
Latency ms
Before injection-R
0.40---1.98 0.007---0.013
0.8251±0.3862 0.010±0.001
Before injection-L
0.21---2.09 0.008---0.014
0.8729±0.4716 0.011±0.001
p 0.137 0.083
After injection-R
0.00---1.39 0.006---0.031
0.3285±0.2640 0.013±0.006
After injection-L
0.10---1.32 0.007---0.017
0.4294±0.2786 0.012±0.003
p 0.000 0.618
Therewasastatisticallysignificantdifferencebetweenandafter
injectionRCMAPamplitudeandafterinjectionLCMAP
ampli-tude,p=0.000.
When the post-injection CMAPmeasurementsof Group S and Group E were compared,no statisticallysignificant differenceswerefoundbetweenthem(p=0.95).
When the pre-injectionand Latency values were com-paredamongGroupD,GroupSandGroupE,nostatistically significant differences were found (p=0.137 --- p=0.083) (Tables1and2).
When thepre-injectionandpost-injection CMAPvalues of Group D were compared,there was a statistically sig-nificant difference(p<0.001). There wereno statistically significant differences among the pre-injection and post-injectionCMAPvaluesofGroupS andGroup E(p=0.126 ---p=0.548).
Discussion
This study is a placebo-controlled, randomized and blind study.Itwasdemonstratedthathigh-dosedexmedetomidine causedsensorialblockinsciaticnervesofratsanddidnot have any histopathologically toxic effects; however, their effectsonneuraltransmissionwerenotelectromyographic studies.
It wasfound that dexmedetomidine inhibited paraven-tricular nucleus parvocellular neurons by means of Ih
suppressionhypothalamic nucleus neurons which are con-trolled by hyperpolarized-activated flows and in direct
contactwithnoradrenergic neurons are called Ih (H-flow)
andrathypothalamicnucleusneuronsbymeansofthe acti-vationof G-proteinpair,whichinternally regulatestheK+
flow.30 Intheinvitrostudyofratdorsalganglionneurons,
it was found that the combination of both clonidine and dexmedetomidinewithlidocaineproducedanadditivetype ofblockinteractionontetrodotoxin-resistantNaflow.31
Apreviouslyconductedstudyshowedthatincreaseddose of dexmedetomidine added to ropivacaine resulted in a longer sensory motor blockage duration through thermal stimulationinrats.26 Thetimeofintensivesensorialblock
andtimetoreturntonormalsensorialfunctionsincreased inadose-dependentmannerwithgraduallyincreasingdoses of dexmedetomidine.26 Also, another study demonstrated
thatsensorialand motor blockin thesciatic nerve block-age of rats showed a significant increase with high-dose dexmedetomidineaddedtobupivacaine.32 We didnotuse
any local anesthetic drugs in our study. In Group D, we administereddexmedetomidine40g/kg−1onlytothe
per-ineuralspaceoftherightsciaticnerve.In30minfollowing drugadministrationinGroupD,therightPWLvalueswere statistically significantly lower than basal values and the rightPWLvalueswerestatisticallysignificantlyhigherthan basalvalues in 210min. The left PWLvalues were statis-ticallysignificantlylowin 30minin comparisonwithbasal values. The reason why the right and left PWL values in 30minwerelowerthanthebasalvalueswasthattheRoRR reflexwasnotrestoredinanyoftheratsinthemeantime, hence the PWL measurements could not be taken. When bothrightandleftPWLvaluesinGroupSandGroupEwere comparedwithbasalvalues,nostatisticallysignificant dif-ferenceswereseen.WhentherightPWLvaluesonDays1,8, 9and14werecomparedwithbasalvalues,nostatistically significantdifferenceswerefound.However,therewere sta-tisticallysignificantdifferencesintermsofthecomparison ofPWLvaluesontheotherdaysandtheywerelongerthan basalvalues.InGroupD,therewerestatisticallysignificant differencesbetween leftPWL values and basal values on Days 4---6, 9---12 and they were longer than basal values. InGroup S, therewerestatisticallysignificant differences between the right PWL values and basal values on Days 4---7,10,11and14andtheywerelongerthanbasalvalues. Therewerestatisticallysignificantdifferencesbetweenleft PWLvaluesandbasalvaluesonDays 3---6,8---9,11---14and theywerelongerthanbasalvalues.InGroupE,no statisti-callysignificantdifferenceswerefoundwhenthePWLvalues werecomparedwithbasalvaluesonpost-operativedaysin casesthatunderwentsurgicalopeningandclosure.Astudy conductedshowedthattheeffectofdexmedetomidinewas
Table2 CMAPamplituderatiosofrighttoleftsciaticnervesofthegroups.
Total GroupD GroupS GroupE
Before injection-R/L
0.37---2.26 1.0641±0.3965a
After injection-R/L
0.13---3.15 0.13---2.07 0.27---3.15 0.31---1.69
0.8456±0.5016 0.7297±0.3608a,b 0.9744±0.6155b 0.8064±0.4018
SignificantdifferencesbetweenGroupD.
analgesia achievedin rats by dexmedetomidine added to ropivacainefor peripheral nerveblock developsthanks to peripheraleffects.In thisstudy,thegroupof dexmedeto-midinealonedevelopedshortandpartialsensorialblock.35
Ourstudy showedthat dexmedetomidine resulted inPWL prolongation notonly in the right sciatic nerve, where it wasinjectedinperineuralspace,butalsointheleftsciatic nerveon specific daysfollowing drugadministration. The sameeffectwasalsoobservedinGroupS.Thiseffectwasnot observedinGroupE.Forthatreason,itwouldnotbe accu-ratetoattributetheseprolongationstodexmedetomidine; however,theseeffectsmaybeattributedtointerventions ontheperineuralspace.Morestudiesshouldbeperformed onthatsubject. However, thesame PWLprolongations in GroupDandGroupSalsotookplaceinleftsciaticnerves. Asfortheleftsciaticnerves,nosurgicalinterventionswere madeonthem.Thisisoneofthesubjectsthatmeritsfurther investigation.
When high dose dexmedetomidine is added to bupiva-caine for sciaticnerve block in rats, it does enhance the block.36
When dexmedetomidine is intravenouslyadministered, itgeneratessedation andanalgesiawithoutcausing respi-ratory depression.37---40 It may change sensory perception
through centrally effective analgesia and sedation.37---40
Contrary to the result of a previous study where all the rats received a bilateral sciatic nerve block with both bupivacaine alone and bupivacaine enhanced with dexmedetomidine,36 the resultsof thestudy wherea
uni-lateral block was achieved showed that26 the effects of
dexmedetomidine were dominantat the peripheral nerve level.26Dexmedetomidineataveryhighdoseof20
g/kg−1
hasverylarge, systemiceffectsthatfurtherprolongRoRR atasignificantdegree.26 Inourstudy,thedurationofRoRR
reflexinGroupD wasstatisticallysignificantlyhigherthan theothergroups.
Variousinvitroandinvivostudieshavebeenconducted inordertounderstandwhetherdexmedetomidinehastoxic effectsonnervecells.Schoeleretal.41exposedorganotypic
hippocampalslicestodexmedetomidineandcreateafocal, mechanicaltraumainordertoshowthatdexmedetomidine providedaneuron-protectiveeffectinaninvitrotraumatic brainmodel.Sandersetal.42showedthatdexmedetomidine
preventedcorticalapoptosisunderinvitroandinvivo condi-tions.Inanotherstudythatwasconducted,thecombination ofbupivacaineanddexmedetomidinewerecomparedwith bupivacainealone andit wasassociatedwithsignificantly lessperineuralinflammationat24h.36
Astudyobservedfindingsindicatingthat dexmedetomi-dine5or10ginjected intotheepiduralspaceinrabbits
resulted in the demyelination of oligodendrocytes in the
receivingbupivacaineenhancedwithdexmedetomidineand in the group receiving bupivacaine alone.12 This situation
wasattributedtothecapacityofalpha-2agoniststoreduce inflammatoryresponse.20,22,21,23,44,25,45Inthestudythatwe
carried out, there were no statistically significant differ-encesinallthreegroupswithrespecttohistopathological findings of inflammation and local nerve damage in the perineural space ofthe right and leftsciaticnerve cross-sections.
Wehave not encountered anystudies in the literature whereelectromyographicvalueswerecomparedbeforeand aftertheinjectionofdexmedetomidineinthesciaticnerve. Theassessmentoflatencyisanindicationofthefunctional axons,numberandqualityofvalidaxonsandthereforethe functionalstatusofmotorneuronsthatarestudied.46There
were no statistically significant differences in any of the groupsintermsofpre-injectionandpost-injectionLatency values inour study.In ourstudy,the post-injection CMAP values inGroup D were statisticallysignificantly different ascomparedto theother groups and theyhaddecreased followinginjection.InGroupD,thepre-injectionand post-injection CMAP values were also statistically significantly differentanddecreasedfollowingtheinjection.WithCMAP, 3valuesarerecordedonthebasisofthemusclethatis stud-ied:1---sizeofthemotorunitinnervatedbyaxons,2---size ofthemotornervefibersthatrespondtothestimulusand 3---synchronizationoftheirresponses.47
Inconclusion,theinjectionofperineural dexmedetomi-dine tothesciatic nervein ratsprolonged thePWL value in210minandprolongedthepost-injectionPWLvalueson Days2---7,10---13.ThedurationofRoRRreflexhadbeen pro-longedatastatisticallysignificantlevelinratsthatreceived perineuraldexmedetomidineinjection.Perineuralinjection ofdexmedetomidineintothesciaticnervedidnotresultin a statisticallysignificant perineuralinflammation increase orlocalnervedamage;however,theCMAPvaluesonDay14 followingtheperineuralinjectionofdexmedetomidineinto thesciaticnervewerefoundtobestatisticallysignificantly lower.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.HickeyR, Hoffman J,Ramamurthy S. A comparisonof ropi-vacaine0.5%andbupivacaine0.5%for brachialplexusblock. Anesthesiology.1991;74:639---42[PubMed:2008942].
3.HickeyR,RowleyCL,CandidoKD,etal.Acomparativestudy of0.25%ropivacaineand0.25%bupivacaineforbrachialplexus block.AnesthAnalg.1992;75:602---6[PubMed:1530173]. 4.Vaghadia H,Chan V, Ganapathy S,et al. Amulticentre trial
ofropivacaine 7.5mg×ml−1 vsbupivacaine 5mg×ml−1 for
supra clavicular brachial plexus anesthesia. Can J Anaesth. 1999;46:946---51[PubMed:10522581].
5.LydicR,BaghdoyanHA.Neurochemicalmechanismsmediating opioid-inducedREMsleepdisruption.In:LavigneG,SessleBJ, ChoinireM,SojaPJ,editors.Sleepandpain.Seattle: Interna-tionalAssociationfortheStudyofPain(IASP)Press;2007. p. 99---122.
6.Bonafide CP, Aucutt-Walter N, Divittore N, et al. Remifen-tanilinhibitsrapideyemovementsleepbutnotthenocturnal melatoninsurgein humans.Anesthesiology.2008;108:627---33 [PubMed:18362594].
7.BowdleTA.Nocturnalarterialoxygendesaturationandepisodic airway obstruction after ambulatory surgery. Anesth Analg. 2004;99:70---6[PubMed:15281506].
8.RosenbergJ, Rosenberg-AdamsenS,Kehlet H.Post-operative sleepdisturbance:causes,factorsandeffectsonoutcome.Eur JAnaesthesiol.1995;10:28---30[PubMed:7641640].
9.Eisenach JC, De Kock M, Klimscha W. Alpha(2)-adrenergic agonists for regional anesthesia. A clinical review of cloni-dine (1984---1995). Anesthesiology. 1996;85:655---74 [PubMed: 8853097].
10.MurphyDB,McCartneyCJ,ChanVW.Novelanalgesicadjuncts forbrachialplexusblock:asystematicreview.AnesthAnalg. 2000;90:1122---8[PubMed:10781465].
11.McCartney CJ, DugganE, Apatu E. Should we add clonidine tolocalanestheticfor peripheral nevreblockade?A qualita-tivesystematicreviewoftheliterature.RegAnesthPainMed. 2007;32:330---8[PubMed:17720118].
12.Brummett CM, Norat MA, Palmisano JM, et al. Perineural administrationofdexmedetomidineincombinationwith bupi-vacaineenhancessensoryandmotorblockadeinsciaticnerve block without inducing neurotoxicity in rat. Anesthesiology. 2008;109:502---11[PubMed:18719449].
13.BenoitPW,BeltWD.Destructionandregenerationofskeletal muscleaftertreatmentwithalocalanaesthetic,bupivacaine (Marcaine).JAnat.1970;107:547---56[PubMed:5492943]. 14.Yagiela JA, Benoit PW, Buoncristiani RD, et al.
Compari-son of myotoxic effects of lidocaine with epinephrine in rats and humans. Anesth Analg. 1981;60:471---80 [PubMed: 7195662].
15.ZinkW,GrafBM.Localanestheticmyotoxicity.RegAnesthPain Med.2004;29:333---40[PubMed:15305253].
16.ZinkW,SeifC,BohlJR,etal.Theacutemyotoxiceffectsof bupivacaineandropivacaineaftercontinuousperipheralnerve blockades.AnesthAnalg.2003;97:1173---9[PubMed:14500177]. 17.HeblJR. Ultrasound-guided regionalanesthesia and the pre-ventionof neurologic injury: fact or fiction? Anesthesiology. 2008;108:186---8[PubMed:18212562].
18.Koff MD, Cohen JA, McIntyre JJ, et al. Severe brachial plexopathy after an ultrasoundguided single-injection nerve block for total shoulder arthroplasty in a patient with multiple sclerosis. Anesthesiology. 2008;108:325---8 [PubMed: 18212578].
19.Horlocker TT, O’Driscoll SW, Dinapoli RP. Recurring brachial plexus neuropathy in a diabetic patient after shoulder surgery and continuous interscalene block. Anesth Analg. 2000;91:688---90[PubMed:10960400].
20.Lavand’homme PM, Eisenach JC. Perioperative administra-tion of the alpha2-adrenoceptor agonist clonidine at the site ofnerve injury reducesthedevelopmentof mechanical
hypersensitivityandmodulateslocalcytokineexpression.Pain. 2003;105:247---54[PubMed:14499442].
21.Lavand’homme PM, Ma W, De Kock M, et al. Perineu-ral alpha(2A)-adrenoceptor activation inhibits spinal cord neuroplasticityandtactileallodyniaafternerveinjury. Anes-thesiology.2002;97:972---80[PubMed:12357167].
22.LiuB,EisenachJC.Perineuralclonidinereducesp38 mitogen-activated protein kinase activation in sensory neurons. Neuroreport.2006;17:1313---7[PubMed:16951576].
23.Romero-SandovalA,EisenachJC.Perineuralclonidinereduces mechanicalhypersensitivityandcytokineproductionin estab-lishednerveinjury.Anesthesiology.2006;104:351---5[PubMed: 16436856].
24.Romero-SandovalA,EisenachJC.Clonidinereduces hypersen-sitivity and altersthe balanceof proand anti-inflammatory leukocytesafterlocalinjectionatthesiteofinflammatory neu-ritis.BrainBehavImmun.2007;21:569---80[PubMed:17079113]. 25.Romero-Sandoval EA, McCall C, Eisenach JC. Alpha2-adrenoceptor stimulation transforms immune responses in neuritis and blocks neuritis-induced pain. J Neurosci. 2005;25:8988---94[PubMed:16192389].
26.Brummett CM, Norat MA, Palmisano JM, et al. Perineural administrationofdexmedetomidineincombinationwith bupi-vacaineenhancessensoryandmotorblockadeinsciaticnerve blockwithoutinducingneurotoxicityintherat.Anesthesiology. 2008;109:502---11.
27.Huseyıno˘gluN,OzaydınI,YaylaS, etal.Electrophysiological assessmentoftheeffectsofsiliconetubesandhyaluronicacid onnerveregenerationinratswithsciaticneurorrhaphy.Kafkas UnivVetFakDerg.2012;18:917---22.
28.WangH,SorensonEJ,SpinnerRJ,etal.Electrophysiologic find-ingsandgripstrengthafternerveinjuriesintheratforelimb. MuscleNerve.2008;38:1254---65.
29.Dongren Y, Tao L, Fengsheng H. Electroneurophysiological studies in ratsof acute dimethoate poisoning. Toxicol Lett. 1999;30:249---54.
30.ShirasakaT,KannanH,TakasakiM.ActivationofaG protein-coupled inwardly rectifying K+ current and suppression of Ih contribute to dexmedetomidine-induced inhibition of rat hypothalamicparaventricularnucleusneurons.Anesthesiology. 2007;107:605---15[PubMed:17893457].
31.OdaA,IidaH,TanahashiS,etal.Effectsofalpha2-adrenoceptor agonists on tetrodotoxin-resistant Na+ channels in rat dor-salrootganglionneurons.EurJAnaesthesiol.2007;24:934---41 [PubMed:17568475].
32.Brummett CM, Padda AK, Amodeo FS, et al. Perineural dexmedetomidine added to ropivacaine causes a dose-dependentincreaseinthedurationofthermalantinociception in sciatic nerve block in rat. Anesthesiology. 2009;111: 1111---9.
33.SiaS,LepriA.Clonidineadministeredasanaxillaryblockdoes notaffectpostoperativepainwhengivenasthesoleanalgesic. AnesthAnalg.1999;88:1109---12[PubMed:10320179].
34.SwamiSS,KeniyaVM,LadiSD,etal.Comparisonof dexmedeto-midine and clonidine (␣2 agonist drugs) as an adjuvant to local anaesthesiain supraclavicular brachial plexus block: a randomiseddouble-blindprospectivestudy.IndianJAnaesth. 2012;56:243---9.
35.Brummett CM, Amodeo FS, Janda AM, et al. Perineural dexmedetomidineprovidesanincreaseddurationofanalgesia toathermalstimuluswhencomparedwithasystemiccontrol in a ratsciatic nerveblock. Reg Anesth Pain Med. 2010;35: 427---31.
eral nerve block by lidocaine:prilocaine 1:1 mixture in a lipid depot formulation: comparison of in vitro, in vivo, andeffectkinetics.Anesthesiology.2006;104:110---21[PubMed: 16394697].
41.SchoelerM,LoetscherPD,RossaintR,etal.Dexmedetomidineis neuroprotectiveinaninvitromodelfortraumaticbraininjury. BMCNeurol.2012;11:12---20.
42.Sanders RD, Sun P, Patel S, et al. Dexmedetomidine pro-videscorticalneuroprotection:impactonanaesthetic-induced
46.KorteN,SchenkHC,GrotheC,etal.Evaluationofperiodic elec-trodiagnosticmeasurementstomonitormotor recoveryafter different peripheral nerve lesions in the rat. Muscle Nerve. 2011;44:63---73.