ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Prevalence
of
anxiety,
depression
and
kinesiophobia
in
patients
with
low
back
pain
and
their
association
with
the
symptoms
of
low
back
spinal
pain
Tathiana
O.
Trocoli
∗,
Ricardo
V.
Botelho
DepartmentofNeurosurgery,HospitaldoServidorPúblicoEstadualdeSãoPaulo(IAMSPE),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11March2015 Accepted3September2015 Availableonline11March2016
Keywords: Anxiety Depression Kinesiophobia Lowbackpain Somatoformdisorders
a
b
s
t
r
a
c
t
Objective:Toevaluatetheprevalenceofanxiety,depressionandkinesiophobiaandtheir associationwiththesymptomsoflowbackpain.
Methods:Atotalof65patientsweredividedintothreegroups:Organic,AmplifiedOrganic andNon-Organic.TheyansweredtheBeckAnxietyInventory,BeckDepressionInventory andTampaScaleofKinesiophobiaandwereevaluatedaccordingtotheirpainlevelusing theVisualAnalogicScale.
Results:TheaveragekinesiophobiascoresofthepatientsintheOrganic,AmplifiedOrganic andNon-Organicgroupswere36.26,36.21and23.06points,respectively.Patientswhowere classifiedintotheOrganicgroupexperiencedthemostkinesiophobiaoutofallthreegroups (p=0.007).TheaverageanxietyscoresofthepatientsintheOrganic,AmplifiedOrganicand Non-Organicgroupswere33.17,32.79and32.81points,respectively,withnosignificant differenceamongthegroups (p=0.99).Theaveragedepressionscoresofthepatientsin theOrganic,AmplifiedOrganicandNon-Organicgroupswere32.54,28.79and37.69points, respectively,withnosignificantdifferenceamongthegroups(p=0.29).
Conclusion:Therewasnoassociationbetweenthegroupsandanxietyanddepression. How-ever,therewasapositivecorrelationbetweenkinesiophobiaandtheOrganicgroup.Studies ofotherpatientsamplesareneededtoconfirmthereproducibilityandvalidityofthesedata inotherpopulations.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Prevalência
de
ansiedade,
depressão
e
cinesiofobia
em
pacientes
com
lombalgia
e
sua
associac¸ão
com
os
sintomas
da
lombalgia
Palavras-chave: Ansiedade Depressão
r
e
s
u
m
o
Objetivo:Avaliaraprevalênciadeansiedade,depressãoecinesiofobiaesuaassociac¸ãocom ossintomasdalombalgia.
∗ Correspondingauthor.
E-mail:[email protected](T.O.Trocoli).
http://dx.doi.org/10.1016/j.rbre.2016.02.010
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
Cinesiofobia Lombalgia
Transtornossomatoformes
Métodos: Foramdivididos65 pacientesem trêsgrupos:orgânicos,orgânicos amplifica-dosenãoorgânicos.ElesresponderamaoInventáriodeAnsiedadedeBeck,Inventáriode DepressãodeBeckeEscaladeCinesiofobiadeTampaeforamavaliadosdeacordocomseu níveldedorpelaEscalaAnálogo-Numérica.
Resultados: Osescoresmédiosdecinesiofobiadospacientesdosgruposorgânicos, orgâni-cosamplificadosenãoorgânicosforamde36,26,36,21e23,06pontos,respectivamente. Ospacientesqueforamclassificadosnogrupoorgânicosexperimentarammaior cinesiofo-biadentreostrêsgrupos(p=0,007).Osescoresmédiosdeansiedadedospacientesdos gruposorgânicos, orgânicosamplificados enãoorgânicos eram de33,17, 32,79e 32,81 pontos,respectivamente,nãohouvediferenc¸asignificativaentreosgrupos(p=0,99).Os escoresmédiosdedepressãodospacientesdosgruposorgânicos,orgânicosamplificadose nãoorgânicosforamde32,54,28,79e37,69pontos,respectivamente,nãohouvediferenc¸a significativaentreosgrupos(p=0,29).
Conclusão: Nãohouveassociac¸ãoentreosgruposeaansiedadeeadepressão.Noentanto, houveumacorrelac¸ãopositivaentreacinesiofobiaeogrupoorgânicos.Sãonecessários estudoscomoutrasamostrasdepacientesparaconfirmarareprodutibilidadeeavalidade dessesdadosemoutraspopulac¸ões.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Lowbackpainisafrequentcauseofphysicallimitationsand absencefrom workand isassociatedwithvarious somato-formdisorders.1–8Studieshaveshownthatthedisabilitythat
iscreditedtothesymptomsoflowbackpainpresentsaweak correlationwithpainintensity.1–3,6,8,9Manyfactorsare
associ-atedwithdisabilitysuchascognitive,affective,environmental andsocialfactorsandtheymayinfluenceapatient’s willing-nesstoquestionthepaintheyexperience2–4,6,8,10,11andthus,
abiopsychosocialapproachcouldofferanalternative under-standingofchronicpainanditsimpactontheabilityofthe patienttofunction.1–3,6,8,9
Thepsychologicalprofilesofpatientswithlowbackpain havebeen considered the most importantprognostic indi-catorforthetherapyofspinaldisorders.1 Anawarenessof
therelationshipofthedisabilitytothepainintensityandto thepatient’scognitive-behavioralprofilemaysupplyvaluable informationthatmaybeusedtopredicttheprognosisandthe treatmentandtohelpchoosethebesttherapeuticapproach.2,8
Themanifestationofa patient’ssymptoms hasoftenbeen consideredapredictivetoolforthatpatient’s psychological profile.12,13Thereareinterestinthedevelopmentof
alterna-tivemethodstoevaluatepsychologicaldistresswithoutusing specificpsychologicaltools.
However,results inthe literature are still conflicting as to whether indirect methods are able to evaluate psycho-logicaldistresstothesameextentasclassicalpsychological instruments.14
InthestudybyJohanssonetal.,5whichcomparedpatients
scheduledforeitherdiscsurgeryorarthroscopickneesurgery, spinepatientswhowereunabletoworkreportedmore dis-satisfaction with their current work activity than patients awaitingarthroscopywhowerealsounabletowork.
Thissuggeststhatpatientswithspinalconditionsaremore intenselyaffectedbysomatoformdisordersthanthosewith otherinjuries.5
Ransford14showedthereareagroupofpatientswithhigh
correlation between symptomsand image findings respec-ting the sensitive and motor radicularpaths, and a group withscattered,amplified,migratoryandnon-anatomicpain withoutcorrelationwiththeimagefindings.However,clinical experienceshowsthatweusuallyhaveathirdgroupwitha transitionbetweenthose groups,withsigns andsymptoms explained bythe images, but associated withamplified or exaggeratedpaths,outoftheanatomicdistribution.
Therefore, we classified the patient’s symptomsas rep-resentative of an organic disease (Organic – ORG), of organicdiseasewithbehavioral-cognitiveexpansion (Ampli-fiedOrganic–AO),orasarepresentativeofpsychosomatic manifestations(Non-Organic–NO)andcorrelated withthe levels of anxiety, depression and kinesiophobia in each of thesesymptomsgroups.
Theobjectiveofthisstudywastoevaluatetheprevalence ofanxiety,depressionandkinesiophobiainpatientswithlow back paininthreegroupsofspinesymptoms, dividedinto Organic,AmplifiedOrganicandNon-Organic.
Methodology
Organic group Amplified organic group Non organic group
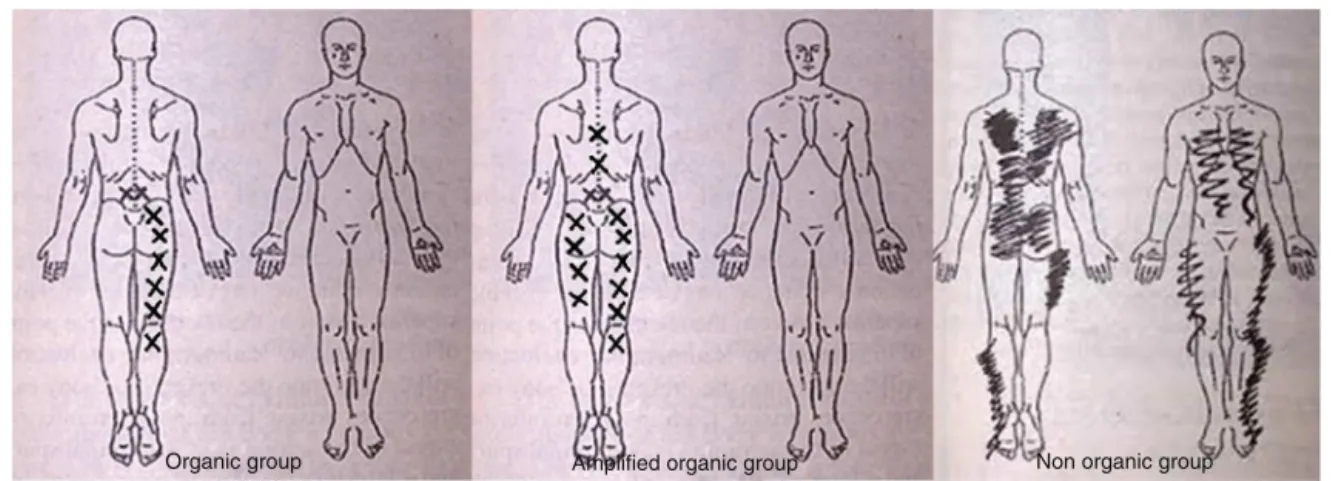
Fig.1–Representationofpatientssymptomsaccordingtothegroups.
oftime duringwhich thesymptomswere experiencedwas measuredinmonthsstartingfromtheonsetofthesymptoms.
Classificationofthesymptoms
Ransfordetal.14demonstratedthatforpatientswithlowback
pain,anabnormalwayofdepictingtheirsymptomsona sil-houetteofthehumanbodyisassociatedwithelevatedscores onotherpsychosomaticscales.14Basedontheevaluationof
thepaindrawings,anamnesisandaphysicalevaluation per-formed bythe patient’s doctor, patients were classified as Organic,AmplifiedOrganicandNon-Organic.
Organicgroup(ORG):patientswhoshowedahigh correla-tionbetweensymptomsandimagefindings.Thesymptoms ofthisgroupsuggestaradicularcomponentwithout amplifi-cations,respectingthesensitiveandmotorpaths.
Amplified Organic group (AO): patients with signs and symptoms explained by the images, but associated with amplifiedorexaggeratedpaths,outoftheanatomic distribu-tion.
Non-Organicgroup(NO):thosepatientswhohadscattered, amplified,migratoryandnon-anatomicpain,without correla-tionwiththeimagefindings.
Anexampleofthepaindrawingsfromeachspecificgroup canbefoundinFig.1.
Anxiety, depression and kinesiophobia assessment: to measureanxious and depressive behaviors, the Beck Anx-ietyInventory15 and the Beck Depression Inventory16 were
used.Inaddition,theBrazilianversionoftheTampaScaleof Kinesiophobia10wasusedtoassesskinesiophobia.Thisscale
consistsofaself-administeredquestionnairecomposedof17 questionsthataddressesthepainandintensityofsymptoms. Scoresrangefromonetofourpoints,andtheanswer“strongly disagree”isequivalenttoonepoint,“partiallydisagree”totwo points,“partiallyagree”tothreepoints,and“stronglyagree”to fourpoints.Toobtainthefinaltotalscoreisrequiredinversion ofscoresforthequestions4,812and16.Thefinalscoremaybe atleast17pointsandmaximum68points,andthehigherthe scorethemostkinesiophobiathepatientpresents.Assessed kinesiophobiawasclassifiedasmild(17–34 points), moder-ate(35–50points)orsevere(51–68points).Assessedanxiety wasclassifiedasmild(0–15points),moderate(16–25points)
orsevere(26–63 points).Assesseddepressionwasclassified asmild(0–18points),moderate(19–29points)orsevere(30–62 points).
This study was approved by the institutional Research EthicsCommitteeunderprotocolnumber283.083/2013.
Statisticalanalysis
The demographic and anthropometric characteristics were described bydescriptive statisticswithmean and standard deviation.Thenormalityofthedistributionofthevariables wasperformedusingKolmogorov–Smirnovtest.
Meanofvariables withnonparametric distributions and theirscoreswereevaluatedbyKruskal–Wallisanalysisof vari-ance.
Results
Atotalof80patientswereinvitedtoparticipateinthestudy and15didnotagreetotakepart.
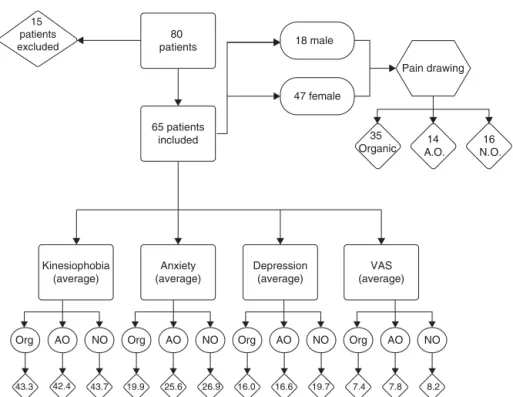
Fig.2isachartthatdemonstratestheresultsofthisstudy.
Resultsforthisgroupofpatients
15 patients excluded
80
patients 18 male
Pain drawing
47 female
35 Organic
Kinesiophobia (average)
Org Org Org
43.3 42.4 43.7 19.9 25.6 26.9 16.0 16.6 19.7 7.4 7.8 8.2
NO NO
AO AO AO NO Org AO NO
Anxiety (average)
Depression (average)
VAS (average)
14 A.O.
16 N.O. 65 patients
included
Fig.2–Flowchartofpatientsincludedandexcludedwiththedistributionineachgroupandthescoresofanxiety, depression,kinesiophobiaandVisualAnalogicScale.
scoresamongallpatientswas43.3points,with16.9%ofcases classifiedasmild,56.9%asmoderateand26.2%assevere.
Classificationofpatientsbytypeofpainbehavior
Concerningthesymptoms,35patientswereplacedintothe Organicgroup, 14into the AmplifiedOrganic groupand 16 patientswereplacedinto theNon-Organicsymptomgroup (Fig. 3).There was nodifference betweenthe averageages ofthethreegroups(one-wayANOVA:F=0.583;p=0.561).The averagelevelofpainmeasuredwas7.37intheOrganicgroup, 7.85 in the Amplified Organic group and 8.31 in the Non-Organicgroup (Kruskal–Wallis;p=0.20). Theaveragelength oftimeofthepatients’ symptomswas40.6months(range: 4–144months).Therewasnosignificantdifferencebetween thesubgroups(Kruskal–Wallis;p=0.39).
Theeducationallevelsandthemanifestationofthethree typesofsymptoms: outofthose whoonlyhadelementary
Organic
Amplified organic
Non-Organic 54%
21% 25%
Fig.3–Distributionofpatientsineachofthethree subgroups:organic,organicamplifiedandnon-organic.
education,fiveparticipantswereclassifiedintothe Organic group,twointotheAmplifiedOrganicgroupandfiveintothe Non-Organic group.Out ofthe individuals who had a sec-ondaryeducation,14patientswereclassifiedintotheOrganic group,sixintotheAmplifiedOrganicgroupandsixintothe Non-Organicgroup.Out ofthosewhohadhighereducation levels,16patientswereclassifiedintotheOrganicgroup,six intotheAmplifiedOrganicgroupandfiveintotheNon-Organic group(p<0.01).
Psychosomaticscoresinthedifferentsymptomsubgroups
Kinesiophobia: the average scores of the patients in the Organic, Amplified Organic and Non-Organic groups were 43.6,42.4 and 43.68points, respectively.Patients whowere classifiedintotheOrganicgroupexperiencedthemost kine-siophobiaoutofallthreegroups(p=0.007).
Anxiety:theaverageanxietyscoresofthepatientsinthe Organic,AmplifiedOrganicandNon-Organicgroupswere19.9, 25.6 and 26.9points, respectively. There wasno significant differenceamongthegroups(p=0.99).
Depression:theaveragedepressionscoresofthepatientsin theOrganic,AmplifiedOrganicandNon-Organicgroupswere 16,16.6and19.7points,respectively.Therewasnosignificant differenceamongthegroups(p=0.29).
The kinesiophobia, anxiety and depression scores are showninFig.4andTable1.
Discussion
25
0 5 10
Scores
Severe Moderate
Mild
Kinesiophobia
Anxiety
Organic Amplified organic Non-Organic
Depression
Kinesiophobia
Anxiety
Depression
Kinesiophobia
Anxiety
Depression
15 20
Fig.4–Scoresofkinesiophobia,anxietyanddepressionin eachofthesymptomgroupsclassifiedasmild,moderate andsevere.
factorsand alterationsinbodilyfunctionsaccordingtothe ICF(InternationalClassificationofFunctioning,Disabilityand Health).1 Anxiety and depression often coexist inpatients
withchronic pain,17,18 and hindertheir ability towork, as
wellastofunctionbothsociallyandphysically.Thisalso com-plicatestheabilityofpatientstocontroltheirpainandthus alsoaffectsthequalityoflifeofindividualswithdegenerative diseasesofthelowerback.19
The Beck Anxiety15 and Depression16 Inventories are
widelyusedtoolsintheclassificationofanxiousand depres-sivebehaviorsofpatientsinoutpatientclinicalcaresettings. TheTampaScaleofKinesiophobiahasbeenusedasa power-fulselectorofpatientswithpoorpsychologicalprofilesand, therefore,thosewithapoorprognosisfortherapy.3,10
There are theories that have attempted to explain the originofchroniclowerbackpain. Acommonlyusedmodel forunderstandingchronic lower backpainisbased onthe proportionalityofthe pain inrelation tothe extentofthe tissueinjury.1–4,8,20However,thereisevidencethatthe
persis-tenceofpainmaynotonlybeexplainedbyobjectiveclinical findings,1–4,8,20andsomeauthorshavefoundaweak
associa-tionbetweenpainintensityandthedisabilityofthepatient.10
Table1–Distributionofpatientsbythegroupsandthe
averagescoresofkinesiophobia,anxietyanddepression
ineachgroup.
n Kinesiophobia Anxiety Depression
Organic 35 43.3 19.9 16.0
Amplifiedorganic 14 42.4 25.6 16.0
Non-organic 16 43.7 26.9 19.7
Someresearchsuggeststhatapatient’spsychological pro-fileisthemostimportantpredictorofprognosisafterspine therapy.1 The study by Bair et al.19 has illustrated that a
combinationofchronicmusculoskeletalpainand psychoso-maticfactors(anxietyanddepression)isassociatedwithmore severe painand agreaterinterferencewithdailyactivities, whentheyarecomparedwithpatientswhoexperiencepain exclusively.
Inaddition, thelinkbetweenchronicpainandits affec-tivecomponentsiswellknown.Inarepresentativesample, McWilliamset al.21 foundthatanxiety waspresent in35%
ofpeoplewithchronicpaincomparedto18%ofthegeneral population.19Depressionratesinthegeneralpopulationare
alsoapproximately18%,whereasamongpatientswithchronic pain,thedepressionratemaybeashighas58%.22
Toclassifythepatients’symptoms,theevaluator consid-eredthepatientsthatdemonstrateahighcorrelationbetween symptomsandimagefindingsaspartoftheOrganicgroup; withintheAmplifiedOrganic group,thesymptomsare rel-atively amplified to the underlying condition; within the Non-Organicgroup,thereislittlecorrelationbetween symp-tomsandclinicalfindings.14
Intheory,patientswithaninadequatepsychological pro-file,withsomatoformamplifications,anxietyanddepression, wouldtendtopresentwithsymptomswithintheNon-Organic orAmplifiedOrganicgroups.Patientswithspinalconditions who have adequate psychologicalprofiles without somato-formdisorderswouldtendtopresentwithsymptomswithin theOrganicgroup.Thus,wetestedthisassociation.
However,wefoundnosignificantdifferences inthe dis-tribution of somatoform disorders, except in relation to kinesiophobia,forwhichtherewasasignificantdifferencein theOrganicgroupcomparedtotheothergroups.Webelieve this happenedbecause anxietyand depression inmajority ofthepatientswithspineorspinesuggestedsymptomsare veryprevalentandkinesiophobiarepresentsanillness behav-iormoreassociatedtoorganicspinedisease.Inthis sense, kinesiophobiacouldbeaprotectivemechanismoflocomotor system.
ThestudyofSiqueiraetal.10showedthatindividualswith
high scores in the Tampa Scale of Kinesiophobia perform worse on physical tests, which supports the premise that patientswithawell-definedorganicinjurymaypresentafear ofperformingmovementsthatareknowntocausemorepain. Thekinesiophobiamodelsuggeststhatpatientsfear move-ments because ofpain, toavoidworsening their condition or avoid causing a new problem. This fear leads to two responses:thepatientmayconfrontoravoidtheactivity. Dur-ingconfrontation,theindividualperformsamovement,which graduallyreducestheirfearofthatmovement.Inavoidance, theindividualdoesnotperformthemovementandbecomes increasinglylessactive,whichresultsinaviciouscyclethat leadstophysicaldisability.23
Asaconfirmationofthismodel,astudyonpatientswith chroniclowbackpainfoundthatthosewiththehighestlevel ofkinesiophobiahada41%higherriskofdevelopingaphysical disability.24
Picovetetal.25foundthatkinesiophobiapredictspainand
Kinesiophobiaarevaluableinthattheycanpredictthelevel ofanindividual’sdisabilitycomparedwithclinicalsignsand symptoms,intensityanddurationofpainandanxiety.
Thisstudywasinitiallydesignedtoevaluate30patientsin eachgrouptofittoanormaldistributionofprevalencesamong thegroups.However,aftereachevaluationofdata,theextent towhichthesamplegrewinsubsequentanalysis,morerobust thetrendtoidentifydifferencesinorganicgroupwasrevealed. Theauthorsdecidedtoevaluatethisnumberofpatientsdue tothestabilityofresults.
The average length of time that patients experienced symptomsofpaininthisstudywasalittleoverthreeyears, whichmay bean aggravatingfactor forsomatoform disor-ders,as shown byvander Windt et al.26 They foundthat
patients with lower back pain have a greater tendency to developchronicbackpainandtocatastrophizeit,compared withpatientswithshoulderinjuries(characterizedbyacute painwithaninjurythatisoftenwelllocated).
Identifyingindividualswithagoodorapoorprognosisis thegoalofmostoftheresearchonthetreatmentofanyspinal disease.Theabilitytopredicttheprognosisduringaninitial evaluationmayleadtomorerealisticexpectationsof recov-eryaswellastheuseofmoreefficienttreatmentstoprevent orcombatchronicpain.3,10,25 ThestudybyHelmhoutetal.3
exemplifiesthisimportancewhentheydemonstratedthatthe decisiveprognosticfactorwasdisabilityfollowedbyafearor movementasassessedbytheTampaScaleofKinesiophobia. Althoughourresultsdidnotrevealsignificantdifferences in terms of the prevalence of anxiety and depression in anyparticularsymptomgroup,theseconditionswerehighly prevalentandwerenotassociatedwithanysingletypeofpain behaviorinallthreegroupsstudied;however,patientswith higherkinesiophobiascoresweremorelikelytopresentwith organicsymptoms.Wedeliberatelydidnotevaluatethe preex-istenceofpsychiatricconditionsinanyofthepatientsstudied. Oneintuitiveprevioushypothesiswasthatourquestionnaires wouldidentifydifferencesamongthethreeselectedgroups. In fact, anxiety and depression were very prevalent in all groups.
This study reinforces the data that patients with lum-bar spine signs and symptoms have a high prevalence of anxiety and depression and, any professional who treats thosepatientsshouldtakeitinconsiderations. Kinesiopho-biashouldberelatedtoamoreorganicpatientsinselection oftreatments.
Limitationsofthisstudy:furtherstudieswithlargersample andmulticenterstudiesareneededtoverifywhetherthese patientsshowadifferenceinprognosisaccordingtothetype oftreatmenttheyreceived.
Ourresultswereobtainedfromasampleofpatientswho arecivilservantsofthestateofSãoPaulo(Brazil).We can-notassureextrapolation(externalvalidity)ofthesedatafor differentpopulations.
Conclusion
Therewasnoassociationbetweenthesymptomsofanxiety anddepression.However,patientswhowereclassifiedinthe Organicgroupweremorelikelytoexperiencekinesiophobia.
Studiesofotherpatientsamplesare neededtoconfirmthe reproducibilityandvalidityofthesedatainotherpopulations.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LaiC,PuaYH,LimKC.Correlatesofself-reporteddisabilityin
patientswithlowbackpain:theroleoffear-avoidance
beliefs.AnnAcadMedSingap.2007;36:1013–20.
2.MaughanEF,LewisJS.Outcomemeasuresinchroniclowback
pain.EurSpineJ.2010;19:1484–94.
3.HelmhoutPH,StaalJB,HeymansMW,HartsCC,HendriksEJM,
BieRA.Prognosticfactorsforperceivedrecoveryorfunctional
improvementinnon-specificlowbackpain:secondary
analysesofthreerandomizedclinicaltrials.EurSpineJ.
2010;19:650–9.
4.WaddellG.Lowbackdisability:asyndromeofwestern
civilization.NeurosurgClinNAm.1991;2:719–37.
5.JohanssonAC,CornefjordM,BergkvistL,ÖhrvikJ,LintonSJ.
Psychosocialstressfactorsamongpatientswithlumbardisc
herniation,scheduledfordiscsurgeryincomparisonwith
patientsscheduledforarthroscopickneesurgery.EurSpineJ.
2007;16:961–70.
6.RenemanMF,SchiphortsPreuperHR,KleenM,GeertzenJHB,
DijkstraPU.Arepainintensityandpainrelatedfearrelatedto
functionalcapacityofevaluationperformancesofpatients
withchroniclowbackpain.JOccupRehabil.2007;17:247–58.
7.SinikallioS,AaltoT,AiraksinenO,HernoA,KrögerH,
SavolainenS,etal.Depressionisassociatedwithpoorer
outcomeoflumbarspinalstenosissurgery.EurSpineJ.
2007;16:905–12.
8.SmeetsRJEM,MaherCG,NicholasMK,RefshaugeKM,Herbert
RD.Dopsychologicalcharacteristicspredictresponseto
exerciseandadviceforsubacutelowbackpain?Arthritis
Rheum.2009;61:1202–9.
9.WaddellG,NewtonM,HendersonI,SomervilleD,MainCJ.A
fear-avoidancebeliefsquestionnaire(FABQ)andtheroleof
fear-avoidancebeliefsinchroniclowbackpainanddisability.
Pain.1993;52:157–68.
10.SiqueiraFB,Teixeira-SalmelaLF,MagalhãesLC.Análisedas
propriedadespsicométricasdaversãobrasileiradaEscala
TampadeCinesiofobia.ActaOrtopBras.2007;15:19–24.
11.FosterNE,ThomasE,BishopA,DunnKM,MainCJ.
Distinctivenessofpsychologicalobstaclestorecoveryinlow
backpainpatientsinprimarycare.Pain.2010;148:398–406.
12.VonBaeyerCL,BergstromKJ,BrodwinMG,BrodwinSK.
Invaliduseofpaindrawingsinpsychologicalscreeningof
backpainpatients.Pain.1983;16:103–7.
13.BertilsonBC,BrosjöE,BillingH,StrenderLE.Assessmentof
nerveinvolvementinthelumbarspine:agreementbetween
magneticresonanceimaging,physicalexaminationandpain
drawingfindings.BMCMusculoskeletDis.2010;11:1–13.
14.DahlB,GehrchenPM,KiaerT,BlymeP,TondevoldE,BendixT.
Nonorganicpaindrawingsareassociatedwithlow
psychologicalscoresonthepreoperativeSF-36questionnaire
inpatientswithchroniclowbackpain.EurSpineJ.
2001;10:211–4.
15.OsórioFL,CrippaJA,LoureiroSR.Furtherpsychometricstudy
oftheBeckAnxietyInventoryincludingfactorialanalysisand
socialanxietydisorderscreening.IntJPsychiatryClinPract.
16.Gomes-OliveiraMH,GorensteinC,LotufoNetoF,AndradeLH,
WangYP.ValidationoftheBrazilianPortugueseversionofthe
BeckDepressionInventory-IIinacommunitysample.Rev
BrasPsiquiatr.2012;34(4):389–94.
17.BeckTA,RushJA,ShawFB,EmeryG.Terapiacognitivada
depressão.RiodeJaneiro:Zahar;1982.p.250.
18.KeenanK,FengX,HipwellA,KlostermannS.Depression
begetsdepression:comparingthepredictiveutilityof
depressionandanxietysymptomsoflaterdepression.JChild
PsycholPsychiatry.2009;50:1167–75.
19.BairMJ,WuJ,DamushTM,SutherlandJM,KroenkeK.
Associationofdepressionandanxietyaloneandin
combinationwithchronicmusculoskeletalpaininprimary
carepatients.PsychosomMed.2008;70:890–7.
20.PincusT,VogelS,BurtonAK,SantosR,FieldAP.Fear
avoidanceandprognosisinbackpain:asystematicreview
andsynthesisofcurrentevidence.ArthritisRheum.
2006;54:3999–4010.
21.McWilliamsLA,CoxBJ,EnnsMW.Moodandanxietydisorders
associatedwithchronicpain:anexaminationinanationally
representativesample.Pain.2003;106:127–33.
22.BanksSM,KernsRD.Explaininghighratesofdepressionin
chronicpain:adiathesis–stressframework.PsycholBull.
1996;119(1):95–110.
23.MoraesVieiraEB,SalvettiMG,DamianiLP,PimentaCAM.
Self-efficacyandfearavoidancebeliefsinchroniclowback
painpatients:coexistenceandassociatedfactors.PainManag
Nurs.2014;15(3):593–602.
24.SalvettiMG,PimentaCAM,BragaPE,CorreaCF.Disability
relatedtochroniclowbackpain:prevalenceandassociated
factors.RevEscEnfermUSP.2013;46:16–23.
25.PicavetHSJ,VlaeyenJWS,SchoutenJSAG.Pain
catastrophisingandkinesiophobia:predictorsofchroniclow
backpain.AmJEpidemiol.2002;156:1028–34.
26.vanderWindtDAWM,KuijpersT,JellemaP,vanderHeijden
GJMG,BouterLM.Dopsychologicalfactorspredictoutcomein
bothlow-backpainandshoulderpain.AnnRheumDis.