www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Medical
adherence
to
intranasal
corticosteroids
in
adult
patients
夽
Emre
Ocak,
Baran
Acar
∗,
Deniz
Kocaöz
KeciorenTrainingandResearchHospital,DepartmentofOtorhinolaryngology,Ankara,Turkey
Received2May2016;accepted30June2016 Availableonline20July2016
KEYWORDS
Adherence; Allergicrhinitis; Intranasal corticosteroids; Treatment
Abstract
Introduction:Theadherencetomedicaltreatment inallergic rhinitisispoorlyevaluatedin clinicalpractice.
Objectives:Toevaluate adherenceto intranasalcorticosteroidsinthetreatmentofallergic rhinitispatients.
Methods:Thisprospectivestudy wasconductedonadultpatientswhowereadmittedtothe outpatientclinicoftheotolaryngologydepartmenttertiaryhospital.Patientsdiagnosedwith moderatetoseverepersistentARandwhohadnotusedanynasalsprayswereenrolledinthe study.Thepatients wereprovidedwithmometasone furoatenasal sprays.Onthe30th day, allparticipantsfilledoutaquestionnaireregardingthefactorsthatmayhaveinfluencedtheir adherencetothetreatment.Afterwards,eachpatientfilledouttheTurkish-language-validated MoriskyMedicalAdherenceScale(MMAS-8)form.Eachfactorthatmayhaveaffectedadherence totheprescribedmedicationwasevaluatedaccordingtotheMMAS-8scoreandallvariables wereanalyzedstatistically.
Results:Fifty-nine adult patients with amean ageof 32.5years(range 21---52 years)were includedinthestudy.ThemeanoverallMMAS-8scorewas3.64.Twofactorswere significan-tlyrelatedtolowadherence:numberofdependentchildren(p=0.001)andbenefitfromthe medication(p=0.001).Inaddition,patientswithhighereducationlevelsseemedtobemore adherentthantherestofthegroup.
Conclusion:Clinicians must keep inmind the factorsrelated to non-adherencein orderto achievebettertreatmentoutcomes.Therefore,basedonourresults,patientsmustbeinformed thatmedicationsshouldbetakenproperlyregardlessofthebenefit,andthetreatmentshould bescheduledwithrespecttodailyactivities,particularlyforpatientscaringformorethantwo children.
© 2016 Publishedby Elsevier EditoraLtda. on behalf ofAssociac¸˜ao Brasileira de Otorrino-laringologiaeCirurgiaC´ervico-Facial.ThisisanopenaccessarticleundertheCCBYlicense (http://creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:OcakE,AcarB,KocaözD.Medicaladherencetointranasalcorticosteroidsinadultpatients.BrazJ
Otorhino-laryngol.2017;83:558---62.
∗Correspondingauthor.
E-mail:[email protected](B.Acar).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.06.007
PALAVRAS-CHAVE
Adesão; Rinitealérgica; Corticosteroides intranasais; Tratamento
Adesãoclínicaacorticosteroidesintranasaisempacientesadultos
Resumo
Introduc¸ão: Aadesãoaotratamentoclínicoderinitealérgicaémalavaliadanapráticaclínica.
Objetivos: Avaliaraadesãoaoscorticosteroidesintranasaisnotratamentodepacientescom rinitealérgica.
Método: Esteestudoprospectivofoirealizadoempacientesadultosadmitidosnoambulatório dosetordeotorrinolaringologiadeumhospitalterciário.Ospacientesdiagnosticadoscomrinite alérgicamoderadaapersistentegraveequenãohaviamaindausadospraynasalforamincluídos noestudo.Ospacientesreceberamspraysnasaisdefuroatodemometasona.No30◦dia,todos
osparticipantespreencheramumquestionáriosobreosfatoresquepodemterinfluenciadoa suaadesãoaotratamento.Depoisdisso,cadapacientepreencheuoformuláriodaEscalade AdesãoClínicaMoriskyvalidadoparaalínguaturca(MMAS-8).Cadafatorquepodeterafetado aadesão àmedicac¸ãoprescritafoiavaliado deacordocomoescore deMMAS-8e todasas variáveisforamanalisadasestatisticamente.
Resultados: Foramincluídosnoestudo59pacientesadultoscommédiade32,5anos(variac¸ão de21-52).OescoretotalmédiodeMMAS-8foide3,64.Doisfatoresforamsignificantemente relacionadoscomabaixaadesão:númerodedependentesinfantis(p=0,001)ebenefícioda medicac¸ão(p=0,001).Alémdisso,ospacientescomníveisdeensinomaiselevadospareceram sermaisaderentesdoqueorestantedogrupo.
Conclusão:Osmédicosdevemestarcientesdosfatoresrelacionadosàfaltadeadesão,afim de alcanc¸ar melhores resultados dotratamento. Portanto, com baseem nossosresultados, os pacientes devem ser informados de que os medicamentosdevem ser usados adequada-mente independentementedo benefício,e otratamentodeve serprogramadocomrelac¸ão àsatividadesdiárias,especialmenteparaospacientesquecuidamdemaisdedoisfilhos. © 2016Publicadopor ElsevierEditora Ltda.em nomede Associac¸˜ao Brasileira de Otorrino-laringologia eCirurgiaC´ervico-Facial.Este ´eumartigo Open Accesssob umalicenc¸a CCBY (http://creativecommons.org/licenses/by/4.0/).
Introduction
Adherence is defined as ‘the extent to which a
per-son’sbehavior---takingmedication,followingadiet,and/or
executing lifestyle changes --- corresponds with agreed
recommendations from a health care provider’.1
Non-adherencetoprescribedmedicationshasalwaysattracted
lessattentioninthetreatmentofdisease.Inparticular,
indi-viduals whosuffer from chronic diseases such asasthma,
hypertension, diabetes mellitus, or Chronic Obstructive
PulmonaryDisease(COPD)havecertaindifficultieswith
con-tinuingmedicaltreatment.Thishasbeenstudiedinseveral
papers,andinonestudyregardingasthmapatients,itwas
reportedthatlessthanhalfofprescribedmedicationswere
taken.2Awarenessofproblemswithadherenceisas
impor-tant as setting up the right treatment modality in such
diseases.Itisobviousthatnon-adherencewillhavea
nega-tiveeffectonlong-termtreatmentresultsandobliviousness
aboutthis problemwillleadtounnecessarytherapies and
incorrectdecisions.AnotherstudybyEvansetal.indicated
adiscontinuationrateof39%inhypertension.3The rateis
evenhigherinCOPDpatients,at86%accordingto
Penning-vanBeestetal.4Thesefindingsemphasizetheimportance
ofadherencetomedicaltreatments.
The most commonly used scale for objectively
evaluating adherence is the Morisky Medication
Adher-ence Scale (MMAS), which is a generic, self-reported,
medication-taking-behavior scale that was initially
vali-dated for hypertension but is used for a wide variety of
medicalconditions.5The originalversionconsistedoffour
items,anditwaseventuallyupdatedtoaneight-itemscale
calledtheMMAS-8(Table1).6Accordingtothisscale,more
pointsindicateloweradherencetotreatment.
Intranasal corticosteroids (ICS) are the mainstay
med-ication for allergic rhinitis (AR) in the daily routine of
outpatientotorhinolaryngologyclinics.However,adherence
tothistreatmenthasnotbeenwell-studied.Inthepresent
study,weinvestigatedadherenceratesandfactorsthatmay
leadtonon-adherenceinanadultARpopulation.
Methods
Studydesignandpatientpopulation
Thisprospectivestudywasconductedonadultpatientswho
wereadmittedtotheoutpatientclinicofthe
otolaryngol-ogydepartment at a tertiaryhospital. Patientswhowere
diagnosedwith moderate tosevere persistent AR
accord-ingtotheARIA (allergicrhinitisanditsimpactonasthma)
guidelinesandwhohadnotpreviouslyusedanynasalsprays
were enrolled.7 Informed consent was obtained from all
patientsbefore the study began. The institutional review
Table1 MMAS-8scale.
Yes No
1.Doyousometimesforgettotakeyourpills?
2.Peoplesometimesmisstakingtheirmedicationsforreasonsotherthanforgetting. Thinkingoverthepasttwoweeks,werethereanydayswhenyoudidnottakeyour medicine?
3.Haveyouevercutbackorstoppedtakingmedicinewithouttellingyourdoctor becauseyoufeltworsewhenyoutookit?
4.Whenyoutravelorleavehome,doyousometimesforgettobringalongyour medicine?
5.Didyoutakeallyourmedicineyesterday?
6.Whenyoufeellikeyoursymptomsareundercontroldoyousometimesstoptaking yourmedicine?
7.Takingmedicineforeverydayisarealinconvenienceforsomepeople.Doyouever fellhassledaboutstickingtoyourtreatmentplan?
8.Howoftendoyoufelldifficultyrememberingtotakeallyourmedicine?
Never/rarely Onceinawhile Sometimes Usually Allthetime
Afteradetailedclinicalhistoryandexaminationofthe nasalcavity,sinuses,nasopharynx,andchesteitherwitha telescopeorX-rays,thediagnosisofARwasconfirmedwith evidenceofspecificIgEreactivitytoallergens,determined ona Skin-PrickTest(SPT)and/or bythedemonstration of serum-specificIgE.Patientswithasthma,nasalseptal devi-ation,ahistoryofnasalsprayuse,acute/chronicsinusitis,a historyofsinonasalsurgery,orahistoryofsinonasal malig-nancy were excluded. After diagnosis, the patients were providedwithmometasonefuroatenasalsprayatadoseof 256gperday,administeredastwosprayspernostrilonce
dailyinthemorningfor30days.Allpatientsweregiven writ-tenstandardizedinstructionsonhowtousethemedication. Attheendofthetherapy,allparticipantswereseenfora controlexaminationandwereaskedtofilloutan11 item questionnaire regarding the factors that may have influ-encedtheiradherencetothetreatment(Table2).Afterthe
questionnaire,eachpatientfilledoutthe
Turkish-language-validated MMAS-8 form and the scores were calculated
byanother physicianwho wasblind tothe clinical data.8
MMAS-8 is a practical scale comprised of 8 yes/no
ques-tionsregardingpatient’sadherencetomedicaltreatment.
As described abovehigherscores mean less adherence to
treatment.Eachfactor thatmayhaveaffectedadherence
totheprescribedmedicationwasevaluatedaccordingtothe
MMAS-8scoreandallvariableswereanalyzedstatistically.
Statisticalanalysis
StatisticalanalysiswasperformedusingtheStatistical
Pack-agefortheSocialSciencesversion15.0(SPSS,Inc.,Chicago,
IL,USA).Thesignificanceofthedifferencebetweengroups
in terms of median values was determined with the
Kruskal---Wallistest.Ap-valueof<0.05wasconsidered
sig-nificant.
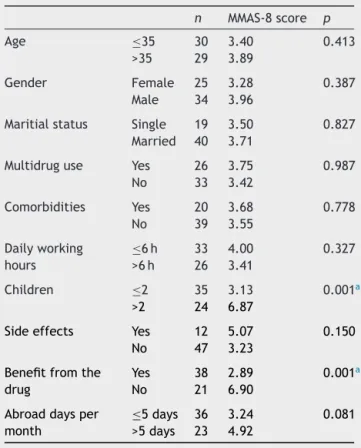
Table2 Factorsrelatedtoadherencelevel.
n MMAS-8score p
Age ≤35 30 3.40 0.413
>35 29 3.89
Gender Female 25 3.28 0.387 Male 34 3.96
Maritialstatus Single 19 3.50 0.827 Married 40 3.71
Multidruguse Yes 26 3.75 0.987 No 33 3.42
Comorbidities Yes 20 3.68 0.778 No 39 3.55
Dailyworking hours
≤6h 33 4.00 0.327 >6h 26 3.41
Children ≤2 35 3.13 0.001a >2 24 6.87
Sideeffects Yes 12 5.07 0.150 No 47 3.23
Benefitfromthe drug
Yes 38 2.89 0.001a
No 21 6.90
Abroaddaysper month
≤5days 36 3.24 0.081
>5days 23 4.92
a Statisticallysignificant.
Results
From82patients whowerediagnosed asARinour
outpa-tient clinic, 59 patients (32 female and 27 male) with a
meanage of32.5 years(range21---52)whometthe
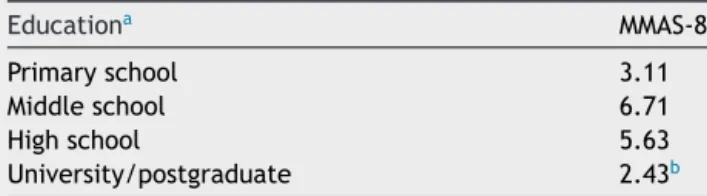
Table3 MMAS-8scoresaccordingtoeducationlevel.
Educationa MMAS-8
Primaryschool 3.11
Middleschool 6.71
Highschool 5.63
University/postgraduate 2.43b a EducationlevelsareshownaccordingtotheTurkish
educa-tionsystem.
b Statisticallysignificantaccordingtononparametrictests.
in the study. The remainder 23 patients were excluded.
Forty-two patients of the study group had a positive SPT
and 23had specific IgE reactivityto allergens (6patients
hadbothpositiveSPTandspecificIgEreactivity).Themean
overallMMAS-8scorewas3.64.Thefactorsthatmayaffect
adherenceandtherelatedMMAS-8scores aresummarized
in Table2. When thescores were evaluated, patients
liv-ing withmore thantwo dependent children, whodid not
benefitfromthemedication,whoexperiencedsideeffects,
or whotraveled more than 5 days per month had higher
scoresforpooradherence(6.87,6.90,5.07,and4.92points,
respectively).Whenallquestionswereevaluatedfromthe
statisticalpointofview,twofactorsseemedtobe
significan-tlyrelatedtolowadherence:numberofdependentchildren
(p=0.001)and benefitfromthemedication (p=0.001). In
our study, patients with more than two dependent
chil-dren and who thought that the medication did not work
weremorelikelytodiscontinuetheirtherapy.Ontheother
hand, patients whobenefited fromthe medication, those
whowerelivingwithlessthantwodependentchildren,and
thosewhohadfewersideeffectsweremoreadherenttothe
therapy according toMMAS-8scores (2.89, 3.13,and 3.23
points,respectively).Education statuswasanother
impor-tantfactor.Patientswithhighereducationlevelsseemedto
bemoreadherentthantherestofthegroup(Table3).
Discussion
Theimportanceofadherencetomedicaltherapyisan
incon-testable element thatmay affect treatment outcomes. It
is beyonddoubt that non-adherencewill cause prolonged
duration of treatment, dissatisfaction of patients, low
qualityoflife,andunnecessaryfinancialburdensfor
govern-ments.Areportstatedthatmorethanhalfofpatientswith
chronic diseases fail to continue prescribed medication.9
Adherence is an underestimated factor in the treatment
protocols for various diseases, but the number of studies
investigating this phenomenon has gradually increased in
thelastdecade.InastudybyChristensen,non-adherenceto
medicaltreatmentregimenswasreportedtorangebetween
20%and40%inacuteillnessand30%---60%inchronicdiseases.
Moreover,discontinuityrateswere ashigh as80%for
pre-ventivetreatments.10Therearenumerousdeterminantsof
adherence.Ingeneral,thesecanbedividedintomodifiable
andnon-modifiablefactors,suchasthetypeofprescribed
medication,thephysician---patientrelationship,thecostand
thediseaseitselfasstatedbyOsterbergetal.11
Although investigations about medical adherence have
attractedmuchattention lately,adherencetoICSin ARis
lesswellstudied. Afewreports werepublishedaboutthe
roleofpatientpreference,knowledgelevelandwillingness
toadheretothetherapy.12---14
Basedonthisbackground,weinvestigatedthevariables
thatmayberelatedtomedicaladherencetoICSinAR.Our
findingssuggestedthatthenumberofchildrendependenton
thepatientandthefeelingofreceivingabenefitfromthe
drugwerethetwomostsignificantfactorsrelevantto
adher-ence.Providingbenefitfromthedrugisasubjectiveterm.
Ourdatademonstratesthatitisanimportantfactorandthe
patientswhowereinthefeelingthatthemedicationis
work-ing,seemedtobemoreadherenttothetreatment.Thus,
wesuggestschedulingthemedicationplanwithrespectto
dailyactivities,particularlyforpatientscaringformorethan
twochildren.Itisalsoimportanttoremindthepatientto
taketheprescribedmedicationsproperly,regardlessofthe
benefit.Inordertoavoidnon-adherenceduetothe
above-mentionedfactors,itisessentialtoreexaminethepatient
atregularintervalsandtochangethemedicineifnecessary.
Itisimportanttonotethatneitherefficiencynorbenefit
fromthetreatmentwasevaluatedinthisstudy.Therefore,
ahomogenousstudygroupwasformed intermsofgender,
age,andseverityofdisease.
Limitations of this study may be the number of
parti-cipants,thepossibilityofinteractionbetweenthefactors,
and the follow-up period. However,as mentioned above,
meticulouseffortwasmadetopreventheterogeneityinthe
studypopulation. On the other hand, a precise and
inde-pendentevaluationof eachfactor requires an excessively
homogenous studygroup, which in practicewould reduce
thenumberofpatients.Anotherfactoristhelack of
mul-tivariatestatistical analysesdue tothe limitednumberof
participants.Thus, furtherstudies with largergroups and
longerfollow-upperiodsareneededtoperformamore
accu-rateevaluationofadherenceinAR.
Conclusion
Thetreatmentofadiseaseisamultifactorialprocess
involv-ing the appropriate drugs, timing, the patient’s general
status, and the healthcare system. After the diagnosis is
made andwhile the clinicianis setting up the treatment
regime,it must bekept in mindthat non-adherence will
frustrateallefforts.Therefore,wesuggestkeepinginmind
thefactorsrelatedtonon-adherencewhenproviding
infor-mationaboutprescribedmedications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.SorensenTD,PestkaDL,BrummelAR,RehrauerDJ,EkstrandMJ. Seeingtheforestthroughthetrees:improvingadherencealone willnotoptimizemedicationuse. JManagCareSpecPharm. 2016;22:598---604.
3.EvansCD,EurichDT,RemillardAJ,ShevchukYM,BlackburnD. First-fillmedicationdiscontinuationsandnonadherenceto anti-hypertensivetherapy:anobservationalstudy.AmJHypertens. 2012;25:195---203.
4.Penning-vanBeestF,vanHerk-SukelM,GaleR,LammersJW, Herings R. Three-year dispensing patterns with long-acting inhaled drugs in COPD: a database analysis. Respir Med. 2011;105:259---65.
5.MoriskyDE,GreenLW, LevineDM. Concurrentand predictive validityofaself-reported measureofmedicationadherence. MedCare.1986;24:67---74.
6.MoriskyDE,AngA,Krousel-WoodM,WardHJ.Predictivevalidity ofamedicationadherencemeasureinanoutpatientsetting.J ClinHypertens.2008;10:348---54.
7.Scadding GK, Durham SR, Mirakian R, Jones NS, Leech SC, FarooqueS,etal.BASCIguidelinesforthemanagementof aller-gicandnon-allergicrhinitis.ClinExpAllergy.2008;38:19---42. 8.O˘guzülgenIK,KöktürkN,Is¸ikdo˘ganZ.Turkishvalidationstudy
ofMorisky8-itemmedicationadherencequestionnaire (MMAS-8)inpatientswithasthmaandchronicobstructivepulmonary disease.TuberkToraks.2014;62:101---7.
9.DeGeestS,SabateE.Adherencetolong-termtherapies: evi-denceforaction.EurJCardiovascNurs.2003;2:323.
10.ChristensenAJ.Patientadherencetomedicaltreatment reg-imens: bridging the gap between behavioral science and biomedicine.Currentperspectives inpsychology series. New Haven,USA:YaleUniversityPress;2004.
11.OstergbergL, BlaschkeT.Adherencetomedication.NEnglJ Med.2005;353:487---97.
12.MahadeviaP,ShahS,LeibmanC,KleinmanL,O’dowdL.Patient preferencesforsensoryattributesofintranasalcorticosteroids and willingness to adhere to prescribed therapy for aller-gicrhinitis:aconjointanalysis.AnnAllergyAsthmaImmunol. 2001;93:345---50.
13.HellingsPW,DobbelsF,DenhaerynckK,PiessensM,Ceuppens JL,DeGeestS.Explorativestudyonpatient’sperceived knowl-edgelevel,expectations,preferencesandfearofsideeffects fortreatmentforallergicrhinitis.ClinTranslAllergy.2012;29: 9.