w w w . r b o . o r g . b r
Original
article
Rotator
cuff
arthropathy:
what
functional
results
can
be
expected
from
reverse
arthroplasty?
夽
Rodrigo
Caldonazzo
Fávaro,
Michel
Abdulahad
∗,
Salim
Mussi
Filho,
Rafael
Valério,
Mauro
José
Superti
HospitalUniversitárioCajuru,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17September2014 Accepted10November2014 Availableonline20August2015
Keywords:
Rotatorcuff Arthroplasty Shoulder
Evaluationofresults
a
b
s
t
r
a
c
t
Objective:Toevaluatethefunctionalresultsfromreversearthroplastyanditscomplications andrelationshipswithtypesofinjury.
Methods:Twenty-sevenshoulders(26womenandoneman)weretreated.Thepatientswere assessedusingtheUCLAfunctionalscale.TheimplantusedwastheDeltaXtendDepuy®
model.TheinjurieswereclassifiedusingtheSeebauermethodforthedegreeofarthroplasty andtheNerotmethodfornotching.
Result:Themeanagewas77.4years(range:67–89)andthefollow-upwas25.8months(range: 6–51).ThepreoperativeUCLAscorewas10.1(range:6–15)andthepostoperativeUCLAscore was29.8(range:22–35),whichwasastatisticallysignificantimprovement(p<0.001). Accord-ingtotheSeebauerclassification,fivepatientswere1B,19were2Aandthreewere2B.Fifteen casespresentedcomplications(55.5%)andnotchingwasthecommonestofthese,occurring in14patients(ninewithgrade1andfivewithgrade2),butthisdidnotcauseinstabilityin anyofthem.Onlyonepatient(3.7%)hadamajorcomplication,consistingofdislocationin theimmediatepostoperativeperiod.Twopatients(7.4%)saidthattheywouldundergothe procedureagain.Onepatient(3.7%)underwentarevisionprocedure.
Conclusion: Reversearthroplastywasshowntobeanexcellentoptionfortreatingpatients withrotatorcuffarthropathy,withalowrateofmajorcomplications.Notchingwasa fre-quentcomplication,butinthemajorityofthecases,itdidnotpresentclinicalrepercussions. ©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Artropatia
de
manguito:
o
que
esperar
do
resultado
funcional
da
artroplastia
reversa?
Palavras-chave:
Bainharotadora
r
e
s
u
m
o
Objetivo:Avaliaroresultadofuncionaldaartroplastiareversa,suascomplicac¸õeserelac¸ões comostiposdelesões.
夽
WorkperformedbytheShoulderandElbowGroup,OrthopedicsandTraumatology,HospitalUniversitárioCajuru,Curitiba,PR,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](M.Abdulahad).
http://dx.doi.org/10.1016/j.rboe.2015.08.005
Avaliac¸ãoderesultados Depuy®.AslesõesforamclassificadassegundoSeebauerparaograudeartropatiaeNerot
paraonotching.
Resultado: Aidademédiafoide77,4(67-89),oseguimentofoide25,8meses(6-51),oUCLA préerade10,1(6-15)eoUCLApósfoide29,8(22-35),comumamelhoriaestatisticamente significativa(p<0,001).Pelaclassificac¸ãodeSeebauer,cincoeram1B,19eram2Aetrês eram2B.Tivemos15complicac¸ões(55,5%),onotchingfoiomaiscomumeocorreuem14 pacientes,novedelesgrauIecincograuII,masnenhumdelesgerouinstabilidade. Ape-nasumapaciente(3,7%)tevecomplicac¸ãomaior,comluxac¸ãonopós-operatórioimediato. Doispacientes(7,4%)alegaramquenãorepetiriamoprocedimento.Umapaciente(3,7%)foi submetidaarevisão.
Conclusão: Aartroplastiareversamostrou-seumaexcelenteopc¸ãoparaotratamentode pacientescomartropatiadomanguitorotadorcombaixoíndicedecomplicac¸õesmaiores. Onotchingéumacomplicac¸ãofrequente,masquenamaioriadoscasosnãoapresenta repercussãoclínica
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thefirstcasesofglenohumeralarthrosisresultingfrom rota-torcuffinjuriesweredescribedbyAdamsandSmith,in1850,
apudFeeleyetal.,1butitwasNeeretal.,2in1983,whoused
theterm“arthropathyoftherotatorcuff”forthefirsttimeto describeacombinationofmassiverotatorcuffinjurytogether with upward migration and femoralization of the femoral headanderosionoftheacromionwithpossible acetabular-ization.
Regarding etiology, Garancis et al.3 proposed the name
“Milwaukee shoulder” for this pathological condition and suggestedthatitmightbecausedthroughaccumulationof hydroxyapatitecrystals insidethe joint,which would then bephagocytizedbysynovialcells,therebyreleasing proteo-lyticenzymes andleading tojointdestruction.Neeret al.2
putforwardthehypothesisthatmechanicalandnutritional alterations would interact in the etiology of the disease. Mechanically,thepresenceofmassiveinjurytotherotatorcuff wouldcauseanimbalanceinthepairsofforcesandwould resultinupwardmigrationofthe headand erosionofthe acromion.Theuncoveringoftheheadwouldleadtounsealing ofthejointwithlossofnegativepressureandextravasation ofthe synovialfluidtothe soft tissues.The qualityofthe remainingfluidwoulddiminishandthiswouldleadto degen-erationofthejointcartilageandosteopeniathroughdisuse.2
Thisdiseaseaffectswomenmoreoften,andparticularly betweenthesixthandseventhdecadesoflife.Thedominant limbismore commonlyaffected and bilaterality occurs in 10–25%ofthecases.Thenaturalevolutionleadstoprogressive chronicpainandlimitationofactivities.Inphysical evalua-tions,supraspinatustestsarepositive.Thesubscapulariscan beevaluatedthroughtheGerberorliftofftest,andpatients maypresentpseudoparalysisandtestpositivelyforthe Horn-blowersign.Nighttimepainandlossofrangeofmotionare common, especially with regard to elevation and external rotation.Recurrentanterioredema(geysersignorfluidsign)
resulting from increasedfluidpressure onthe subacromial bursamayalsobeobserved.1,4
The forms of treatment range from conservative treatment,5,6 which is always indicated initially, to
arthro-scopic debridement,7–9 hemiarthroplasty,10–12 reverse
arthroplasty13–15 and salvage procedures such as
arthrodesis16,17 and resection arthroplasty.18 Currently,
anatomical totalarthroplastyisproscribedfortreating this pathologicalconditionbecauseofthelowsuccessrate,high rate of loosening, high attrition and instability generated throughthephenomenonknownasrockinghorse.19
Recently, the popularity of reverse arthroplasty has increased.Theconceptofthecurrentmodelsisbasedonthe principlesofGrammont,withmedializationand inferioriza-tionofthecenterofrotation,whichbooststheactionofthe deltoid.13,20
Theobjectiveofthepresentstudywastoevaluatethe func-tionalresultfromreversearthroplastyfortreatingarthropathy oftherotatorcuff,thecomplicationsfromthisprocedureand relationshipswithtypesofinjury.
Materials
and
methods
Between January 2010 and November 2013, the Shoulder and Elbow Group of the Department of Orthopedics and Traumatologyofourinstitutionconductedaretrospective epi-demiologicalstudythatinvolvedreviewingthemedicalfiles.
ThisstudywasapprovedbytheEthicsCommitteeofthe institutionatwhichitwasconducted.
Theinclusion criteria were:(1) arthroplasty ofthe rota-tor cuffalready established; (2)imaging examinationsthat demonstrated massive tearing of the rotator cuff; and (3) trophicdeltoidpresentingstrengthgrade5.
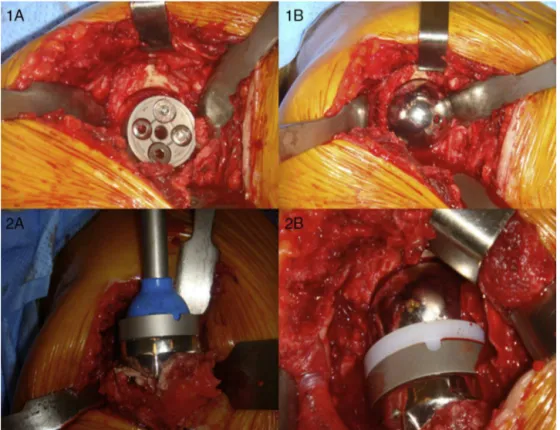
Fig.1–Duringtheoperation:(1A)insertionofbaseplatewithlockingscrewsandcorticalscrews;(1B)fittingofglenosphere; (2A)insertionofcementedhumeralcomponent;(2B)fittingofpolyethylenepieceandreductionofthecomponents.
Using these criteria, 27 shoulders in 24 patients were includedinoursample.
Allthepatientswereoperatedbytheseniorsurgeonofthe group,and all operations were performedwith thepatient inthe deckchairposition. Theapproachusedwas a trans-deltoidsuperolateralaccess(Fig.1).Theimplantmodelused wastheDeltaXtendDepuy®.Theinjurieswereclassifiedin accordancewithSeebauer21forthedegreeofarthropathyand
Valentietal.22forthenotching.
After the procedure, a suction drain was installed and thiswas keptinplacefor24h.Thepatients werereleased onthesecond postoperativeday.Between thetimesofthe surgeryandrelease,thepatientsreceived3gofcefazolin intra-venously,dividedintothreedosesof1geach.
The patients were followed up (Fig. 2) two weeks, six weeks,threemonthsandsixmonthsaftertheoperationand annuallythereafter.Foralloftheconsultations,thepatients underwent traumaseries radiological examinationson the scapulohumeraljoint.Attheconsultations,thepatientswere evaluatedusingtheUCLAscoreandaquestionnaireon com-plicationsandthedegreeofsatisfactionwiththeprocedure wasfilledout.
Statisticalanalysis
Theresultsrelatingtoquantitativevariablesweredescribed using means, medians, minimum values, maximum val-ues and standard deviations. Qualitative variables were described using frequencies and percentages. To compare groups defined using the classifications ofSeebauer21 and
Table1–Arthropathyoftherotatorcuffaccordingto Seebauerclassification.
Seebauer Frequency Percentage
2A 19 70.4
1B 5 18.5
2B 3 11.1
Total 27 100
Valentiet al.,22 inrelationtotheUCLAscore,the
nonpara-metricMann–WhitneyandKruskal–Wallistestswereused.A
p-value<0.05indicatedstatisticalsignificance.Thedatawere analyzedusingtheSPSSv.20.0computersoftware.
Results
Thedataregisteredinrelationto27shouldersin24patients who underwent shoulder surgery were analyzed. These patientswereevaluatedbeforeandaftertheoperationin rela-tiontotheUCLAscore.Theirmeanagewas77.4years(range: 60–89).Themeanlengthoffollow-upamongthepatients ana-lyzedwas25.8months(range:6–51).
Amongthe24patients,onlyone(3.7%)wasmaleandthe other23(96.3%)werefemale.Inrelationtothesideaffected, 14(51.9%)ofthecaseswereontherightsideand13(48.1%) wereontheleftside.
AccordingtotheSeebauer21classificationforarthropathy
Fig.2–Elevationandexternalandinternalrotationinapatient,12monthsaftertheoperation.
Therewere15casesofcomplications,14ofnotchingand oneofdislocationofthecomponentsduringtheimmediate postoperativeperiod,inwhichrevisionwithexchangeofthe polyethylenepiecewasnecessary.Uptothetimeofthemost recentfollow-up,onlythispatienthasundergonerevision.
Inrelationtothe presenceofnotching,13(48.1%)ofthe patientsdidnotpresentthiscomplication,whilenine(33.3%) presentedgrade1 accordingto Nerotand five (18.5%) pre-sentedgrade2(Fig.3).
Fig.3–Notching:reabsorptionofthelowerportionofthe scapularneck.
The preoperative and postoperative UCLA scores were comparedandanalyzed.ThepostoperativeUCLAscoreswere comparedwiththepresenceanddegreeofnotchingandits severityaccordingtoNerot.
ThemeanpreoperativeUCLAscorewas10.1(range:6–15). ThemeanpostoperativeUCLAscorewas29.8(range:20–35).
ThemeanincreaseinUCLAscorefrombeforetoafterthe operationwas19.7(p<0.001),thusshowingthatthepatients attained a statistically significant functional improvement
(Table2).
Thenullhypothesisthattherewasnocorrelationbetween thepre-andpostoperativeUCLAscores(correlationcoefficient equalto0)wastestedversusthealternativehypothesisthat a correlation existed (correlation coefficient differing from 0).Spearman’scorrelationcoefficientwasestimatedas0.18, without statistical significance (p=0.360). This meant that althoughtherewasasignificantincreaseinUCLAscore sub-sequenttotheoperation,therewasnorelationshipbetween lower preoperative UCLA scores and postoperative UCLA scoresthatwerealsolower.Thus,wecannotaffirmthatthere wasacorrelationbetweenapoorfunctionalscorebeforethe operationanditspostoperativeresult.
Intheanalysisonthecorrelationbetweenthe postopera-tiveUCLAscoreandthepresenceofnotchinganditsseverity accordingtotheNerotclassification,thenullhypothesisthat the resultswould beequalforthe groups ofpatientswith notchingofgrades0,1and2wastestedversusthe alterna-tivehypothesisthatatleastonegroupwouldhaveresultsthat differedfromthoseoftheothergroups.Inthisanalysis,the nonparametricKruskal–Wallistestwasused.
Table2–UCLAscorebeforeandaftertheoperation.
Variable n Mean Median Minimum Maximum Standarddeviation p-Valuea
UCLAbefore 27 10.1 11 6 15 2.8 <0.001
UCLAafter 27 29.8 31 20 35 4.2
DiffUCLA(after-before) 27 19.7 19 11 29 4.6
a p<0.001andthereforeshowingstatisticalsignificanceforcomparisonofUCLAscoresfrombeforetoaftertheoperation.
Table3–CorrelationofnotchingwithdifferenceinUCLAscorefrombeforetoaftertheoperation.
Notching n DiffUCLA(after-before) Standarddeviation p-Valuea
Mean Median Minimum Maximum
0 13 19.2 17 14 29 4.7 0.225
1 9 21.3 23 11 26 4.6
2 5 18.0 18 12 24 4.3
a p=0.225andthereforeshowingthatthecorrelationofnotchingwithUCLAscoredidnotpresentstatisticalsignificance.
presenceandseverityofnotchingdidnothaveanycorrelation withthefunctionalresultobtained(p=0.446)(Table3).
Onlytwopatientssaidthat theywould notundergothe procedureagain.
Discussion
Althoughtheinitialtreatmentshouldalwaysbeconservative, consisting ofchanges toactivities, oral analgesics, physio-therapy and intra-articular infiltrations, surgical treatment generallybecomesnecessary.Glenohumeralarthrodesishas theaimofpainrelief,butabsenceofthisjointleadsto over-loadingoftheacromioclavicularjointandmaycausepainin thisjoint.However,thistechniqueisalsoasalvagealternative forpatientswhohavealreadyundergoneothersurgical proce-duresandforthosepresentingirreparablerotatorcuffdefects, historiesofinfectionordeficienciesofthedeltoid.16,17
Another salvage procedure that is possible is resection arthroplasty. Thisisindicatedas asalvage optionand last treatmentoptionincasesofchronicinfectionsubsequentto osteosynthesiswithboneloss,orafterinfectedarthroplasty procedures.18
Conventional arthroplasty is atechnique that has been greatlyused,but withoutthe lowercompression force vec-tors,thehumeralheadwouldbecomedisplacedupwardsand wouldleadtoaneccentricloadonthe glenoidcomponent, which isan effect known asthe rocking horse.Thus, this techniqueisproscribedtoday.19,20
Hemiarthroplasty is a viable option with good results, especiallyinpatientswhostillpresentsatisfactory preoper-ativerangeofmotion.Theriskofreabsorptionoftheglenoid andacromion,whichisacomplicationrelatedtothis treat-mentmethod,isassociatedwithpreviousacromioplastyand resectionofthecoracoacromialligament.Studieshaveshown that resection of this ligament and a history of previous acromioplastyarerelatedtoworseresultsbecauseof insta-bilityandupwardmigrationoftheprosthesis.10,11
Thepatients’meanagewas77.4years,whichwasslightly greaterthanthemeanintheworldwideliterature,inwhich the majority of the patients were still completing their
seventh decade oflife.Thedominantside wasmoreoften affected (55%) and females were affected in muchgreater numbers(96.3%).Thesedataweresimilartothefindingsof otherstudies.23
The complications from reverse arthroplasty include notching(thecommonestcomplication),infection,instability, hematomas,looseningoftheglenoidcomponent,loosening ofthehumeralcomponent,dissociationofthecomponents, fracturesoftheacromion,otherfracturesandneurovascular lesions.Inthepresentstudy,therewere14casesofscapular notching(51.9%)andoneofdislocationofthecomponents. Therewerenocasesofinfectionorothercomplications.The notchingratewassimilartothatoftheliterature,whilethe generalcomplicationratewaslower.6,23–25
The complication most frequently encountered in the literatureisnotching.Thisischaracterizedasattritionor reab-sorptionintheinferoposteriorportionofthescapularneck.Its severitywasstratifiedandclassifiedbyValentietal.22There
isstillsomecontroversyintheliteratureregardingitsclinical relevance.Inourstudy,notchingwasthecommonest compli-cation.Wefoundthatitsincidencewas51.9%,apercentage thatwaswithintherangeintheliterature,whichhasbeen from 19%to 100%.23,26,27 Thefactors thatcontribute tothe
presenceofthisboneerosionincludethelearningcurve, posi-tionoftheglenoidcomponent,diminishedacromial-humeral spaceand fattyinfiltrationoftheinfraspinatus. Inferioriza-tionofthebaseplateisthefactorthatcontributesmosttoward thiscomplication.27Thepresenceandseverityofnotchingas
classifiedbyNerotdidnotpresentanyrelationshipwiththe functionalresult,i.e.thepresenceorabsenceofthis compli-cationdidnotaffecttheresultfromthereversearthroplasty orthepatient’ssatisfactionwithit.
Therewerenocasesofinfectioninthisgroup.According totheliterature,thisisthesecondmostfrequent complica-tion,witharateofaround5%.23,28Theabsenceofsofttissues
Thismayleadtounsatisfactoryresultsandgreaternumbers ofsubsequentsurgicalproceduresneededtotreatit.
Intheliterature,thereare fewstudies onperiprosthetic fractures in arthroplasty procedures involving the gleno-humeraljoint.29Wewereunabletofindanyspecificarticles
onhumeralfracturesfromreverseprosthesesinoursurvey, andwealsodidnothavethiscomplicationinoursample.
Instabilityofthe“ballandsocket”interfaceofthe com-ponentofthe prosthesisleadstodislocation. Itsincidence rangesfrom0%to14%.23Thelackofcompressiveforces
asso-ciatedwithashallowhumeralcomponentisthefactormost correlatedwithdislocation.Thiscomplicationtendstooccur withinthefirstmonths,andclosedreductionistheimmediate treatment.Whenit isrecurrent,newsurgerybecomes nec-essaryinordertocorrectthepossibletechnicalfailures.We onlyhadonecaseofdislocation(3.7%),whichoccurred dur-ingtheimmediatepostoperativeperiod,whilethepatientwas beingtransferredtoabed.Thehumeralcomponentbecame loosenedandthepatientthenunderwentrevisionsurgeryin whichthepolyethylenecomponentwasexchangedforalarger one.Thispatientevolvedsatisfactorily,withoutrecurrenceof theinstability.
Whenthereisanindicationforreversearthroplasty, ero-sionoftheacromionbythehumeralheadisalreadypresent. Withthisprosthesis,thelengthofthearmincreasesby2.5cm onaverageandthetensiononthedeltoidalsoincreases.In addition,themedializationofthecenterofrotationincreases thetensionontheacromion.Thisleadstotheriskoffracturing theacromion,whichmayoccurinupto3%ofthecasesafter reversearthroplasty.30Inourgroup,wedidnothaveanycases
ofthiscomplication.Preoperativelesionsoftheacromiondo notcontraindicatearthroplasty,butwhenfracturesoccurafter theoperation,thereisacorrelationwithworseprognosisand functionalresultsfromreversearthroplasty.30Their
diagno-sismaygounnoticedandthereneedstobeahighdegreeof suspicionaccordingtotheclinicalconditionthatthepatient presents, with confirmation by means of radiography and tomographywhennecessary.
Themean preoperativeUCLAscoreof10.1 showedthat theshouldersevaluatedpresentedpoorfunctional capacity inrelationtodailyactivities,withlimitationoftherangeof motionand presence ofpain. Comparison with the mean postoperative UCLA score of 29.8 shows that there was a statisticallysignificantimprovement(p<0.05), withamean differenceof19.7onthisscale.Amongallthepatients,only oneofthem(3.7%)declaredthathewouldnotundergothis surgeryagain.Thisdemonstratesthattherateofsatisfaction withthesurgerywashighamongthesepatients.Incomparing thepostoperativeUCLAscorewiththepresenceofnotching, itwasnotedthattherewasnocorrelationbetweenthesetwo parameters.
Conclusion
Reverse arthroplasty was shown to bean excellent option for treating patients with arthropathy of the rotator cuff, withsatisfactoryfunctionalresults.Notchingwasafrequent
beenlimitedbyitssmallsamplesize.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FeeleyBT,GalloRA,CraigEV.Cuffteararthropathy:current
trendsindiagnosisandsurgicalmanagement.JShoulder
ElbowSurg.2009;18(3):484–94.
2.NeerCS2nd,CraigEV,FukudaH.Cuff-teararthropathy.J
BoneJointSurgAm.1983;65(9):1232–44.
3.GarancisJC,CheungHS,HalversonPB,McCartyDJ.Milwaukee
shoulder–associationofmicrospheroidscontaining
hydroxyapatitecrystals,activecollagenase,andneutral
proteasewithrotatorcuffdefects.III.Morphologicand
biochemicalstudiesofanexcisedsynoviumshowing
chondromatosis.ArthritisRheum.1981;24(3):484–91.
4.NamD,MaakTG,RaphaelBS,KeplerCK,CrossMB,Warren
RF.Rotatorcuffteararthropathy:evaluation,diagnosis,and
treatment:AAOSexhibitselection.JBoneJointSurgAm.
2012;94(6):e34.
5.JensenKL,WilliamsGRJr,RussellIJ,RockwoodCAJr.Rotator
cuffteararthropathy.JBoneJointSurgAm.
1999;81(9):1312–24.
6.WalchG,WallB,MottierF.Complicationsandrevisionofthe
reverseprosthesis,amulticenterstudyof457cases.In:Walch
G,BoileauP,MoleD,FavardL,LevigneC,SirveauxF,editors.
Reverseshoulderarthroplasty:clinicalresults,complications,
revision.Montpellier,France:SaurampsMedical;2006.p.
335–52.
7.HockmanDE,LucasGL,RothCA.Roleofthecoracoacromial
ligamentasrestraintaftershoulderhemiarthroplasty.Clin
OrthopRelatRes.2004;(419):80–2.
8.BoileauP,BaquéF,ValerioL,AhrensP,ChuinardC,TrojaniC.
Isolatedarthroscopicbicepstenotomyortenodesisimproves
symptomsinpatientswithmassiveirreparablerotatorcuff
tears.JBoneJointSurgAm.2007;89(4):747–57.
9.KlingerHM,SteckelH,ErnstbergerT,BaumsMH.
Arthroscopicdebridementofmassiverotatorcufftears:
negativeprognosticfactors.ArchOrthopTraumaSurg.
2005;125(4):261–6.
10.BrasilFilhoR,RibeiroFR,TenorJuniorAC,FilardiFilhoCS,
CostaGBL,StortiTM,etal.Resultadosdotratamentocirúrgico
daartropatiadegenerativadomanguitorotadorutilizando
hemiartroplastia-CTA®.RevBrasOrtop.2012;47(1):66–72.
11.VisotskyJL,BasamaniaC,SeebauerL,RockwoodCA,Jensen
KL.Cuffteararthropathy:pathogenesis,classification,and
algorithmfortreatment.JBoneJointSurgAm.2004;86Suppl.
2:35–40.
12.WilliamsGRJr,RockwoodCAJr.Hemiarthroplastyinrotator
cuff-deficientshoulders.JShoulderElbowSurg.
1996;5(5):362–7.
13.BoileauP,WatkinsonDJ,HatzidakisAM,BalgF.Grammont
reverseprosthesis:design,rationale,andbiomechanics.J
ShoulderElbowSurg.2005;141Suppl.S:147S–61S.
14.FrankleM,LevyJC,PupelloD,SiegalS,SaleemA,MighellM,
etal.Thereverseshoulderprosthesisforglenohumeral
arthritisassociatedwithsevererotatorcuffdeficiency.A
minimumtwo-yearfollow-upstudyofsixtypatientssurgical
15.SirveauxF,FavardL,OudetD,HuquetD,WalchG,MoléD.
Grammontinvertedtotalshoulderarthroplastyinthe
treatmentofglenohumeralosteoarthritiswithmassive
ruptureofthecuff.Resultsofamulticentrestudyof80
shoulders.JBoneJointSurgBr.2004;86(3):388–95.
16.ScaliseJJ,IannottiJP.Glenohumeralarthrodesisafterfailed
prostheticshoulderarthroplasty.JBoneJointSurgAm.
2008;90(1):70–7.
17.CofieldRH,BriggsBT.Glenohumeralarthrodesis.Operative
andlong-termfunctionalresults.JBoneJointSurgAm.
1979;61(5):668–77.
18.GodinhoGG,FreitasJMA,FrancaFO,Franc¸aFO,Fernandes
LFD,CarvalhoB.Artroplastiaderessecc¸ãodacabec¸aumeral
comoprocedimentodesalvac¸ãoemcomplicac¸ões
pós-cirúrgicas.RevBrasOrtop.2006;41(9):361–5.
19.FranklinJL,BarrettWP,JackinsSE,MatsenFA3rd.Glenoid
looseningintotalshoulderarthroplasty.Associationwith
rotatorcuffdeficiency.JArthroplasty.1988;3(1):39–46.
20.GrammontPM,BaulotE.Deltashoulderprosthesisforrotator
cuffrupture.Orthopedics.1993;16(1):65–8.
21.SeebauerL.Totalreverseshoulderarthroplasty:European
lessonsandfuturetrends.AmJOrthop(BelleMeadNJ).
2007;3612Suppl.1:22–8.
22.ValentiPH,BoutensD,NerotC.Delta3reversedprosthesisfor
osteoarthritiswithmassiverotatorcufftear:long-term
results(5years).In:WalchG,BoileauP,MoleD,editors.
Shoulderprosthesis:twototenyearfollow-up.Montpellier,
France:SaurampsMedical;2001.p.253–9.
23.FarshadM,GerberC.Reversetotalshoulderarthroplasty–
fromthemosttotheleastcommoncomplication.IntOrthop.
2010;34(8):1075–82.
24.WierksC,SkolaskyRL,JiJH,McFarlandEG.Reversetotal
shoulderreplacement:intraoperativeandearlypostoperative
complications.ClinOrthopRelatRes.2009;467(1):
225–34.
25.SimovitchRW,ZumsteinMA,LohriE,HelmyN,GerberC.
Predictorsofscapularnotchinginpatientsmanagedwiththe
DeltaIIIreversetotalshoulderreplacement.JBoneJointSurg
Am.2007;89(3):588–600.
26.LevigneC,BoileauP,FavardL.Scapularnotching.In:WalchG,
BoileauP,MoléD,editors.Reverseshoulderarthroplasty:
clinicalresults,complications,revision.Montpellier,France:
SaurampsMedical;2006.p.353–72.
27.LévigneC,BoileauP,FavardL,GaraudP,MoléD,SirveauxF,
etal.Scapularnotchinginreverseshoulderarthroplasty.J
ShoulderElbowSurg.2008;17(6):925–35.
28.ZellerV,GhorbaniA,StradyC,LeonardP,MamoudyP,
DesplacesN.Propionibacteriumacnes:anagentofprosthetic
jointinfectionandcolonization.JInfect.2007;55(2):
119–24.
29.AndersenJR,WilliamsCD,CainR,MighellM,FrankleM.
Surgicallytreatedhumeralshaftfracturesfollowingshoulder
arthroplasty.JBoneJointSurgAm.2013;95(1):9–18.
30.WalchG,MottierF,WallB,BoileauP,MoléD,FavardL.
Acromialinsufficiencyinreverseshoulderarthroplasties.J