RevBrasAnestesiol.2014;64(1):1---15
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
SBA
Recommendations
for
regional
anesthesia
safety
in
patients
taking
anticoagulants
Neuber
Martins
Fonseca,
Rodrigo
Rodrigues
Alves,
João
Paulo
Jordão
Pontes,
Sociedade
Brasileira
de
Anestesiologia
∗SchoolofMedicine,UniversidadeFederaldeUberlândia,Uberlândia,MG,Brazil
Received23April2013;accepted28April2013
Description
of
evidence
collection
method
We conducted searches in multiple databases (Medline
1965-2012; Cochrane Library, Lilacs)and cross-references withthecollectedmaterialtoidentifystudieswithbetter methodologicaldesign,followedbyacriticalevaluationof theircontents andclassificationaccordingtothe strength ofevidence.
We conductedsearchesbetween August andDecember
2012. The following strategies were usedfor searches in
PubMed:
1. ‘‘regional anaesthesia’’ OR ‘‘anesthesia, conduction’’
OR ‘‘anesthesia’’ AND ‘‘conduction’’ OR ‘‘conduction
anesthesia’’ OR ‘‘regional’’ AND ‘‘anesthesia’’ OR
‘‘regionalanesthesia’’AND‘‘antithrombotic’’;
2. ‘‘regional anaesthesia’’ OR ‘‘anesthesia,
conduc-tion’’ [MeSH Terms] AND ‘‘infection’’ [MeSH
Terms] AND ‘‘thromboembolism’’ [MeSH Terms] OR
‘‘thromboembolism’’[AllFields];
3. ‘‘thromboembolism’’ [MeSH Terms] OR
‘‘thromboembolism’’[All Fields]AND‘‘regional anaes-thesia’’[AllFields]OR‘‘anesthesia,conduction’’[MeSH Terms]OR‘‘anesthesia’’[AllFields]AND‘‘conduction’’
∗Correspondingauthor:
E-mail:[email protected]
(SociedadeBrasileiradeAnestesiologia).
[AllFields])OR‘‘conductionanesthesia’’[AllFields]OR ‘‘regional’’ [All Fields] AND ‘‘anesthesia’’ [All Fields] OR‘‘regionalanesthesia’’[AllFields].
In the field of regional anesthesia, we selected stud-iesaddressing managementsof differenttypesofregional anesthesiainindividualstakingdrugsthatmodifytheblood coagulationstatus.Wefocusedonriskfactors,etiology, pre-vention,diagnosis,andtreatment.Wealsoincludedstudies assessingtheriskofcomplicationsinpatientsafterregional blockadeandstudiesthatclarifythemanagementandsafe handlingofdrugstobeadministered.
Level
of
evidence
and
strength
of
recommendation
A:Experimentalorobservationalstudieswithbetter con-sistency.
B:Experimentalorobservationalstudieswithless consis-tency.
C:Casereportsorcaseseries(non-controlledstudies). D:Opinionwithoutcriticalevaluation,basedonconsensus, expertopinions,physiologicalstudies,oranimalmodels.
Objective
To assess the safety aspects of regional anesthesia and analgesia,suchasthepossible technique’s complications;
2 N.M.Fonsecaetal.
risk factors associated with spinal hematoma, prevention strategies,diagnosis,andtreatment; andsafeintervalfor drug suspension and resumption after regional block in patientstakingantithromboticdrugs.
Introduction
Thecurrentincidenceofneurologicaldysfunctionresulting frombleedingcomplicationsassociatedwithneuraxialblock is unknown.1 Its occurrence is estimated to be less than 1:150,000 epiduralpunctures and 1:220,000 subarachnoid punctures.1 After neuraxial anesthesia, the use of anti-coagulants is the risk factor most often associated with spinalhematoma.2Becausespinalhematomaisrare, recom-mendationsregardingregionalanesthesiaandconcomitant useofthromboprophylaxisorantithrombotictherapy,which wouldbeofgreaterpredictivevalueifreportedby prospec-tive randomized studies, are based on case reports and expert recommendations3, which ethically precludes the study.
The number of patients on anticoagulant therapy has been growing due to the aging process, longer life expectancy, and prevalence of cardiovascular disease. Recommendations on safety in regional anesthesia and antithrombotictherapyshouldbeconstantlyupdated,asthe introductionofnewantithromboticdrugstothemarketis doneatregularintervals.2
Thisguidelineaimstoreviewtherisksand recommenda-tionsfor regional anesthesiainsubjects takingdrugs that interfere with coagulation and present safety regulations andguidelinesrequiredforregionalprocedures.
Spinal/epidural
hematoma
Incidence
Althoughtheincidenceof spinal-epiduralhematoma(SEH) issmall,theclinicalseverityofitsconsequences,alongwith litigationcoststhatfollowanadverseevent,makesitcrucial todevelopsoundstrategiesforthemanagementofpatients onanticoagulantsduringneuraxialanesthesia.4
Inaliteraturereview5assessingseveralcasereports,we notedthattheincidenceofSEHwas1:220,000afterspinal anesthesiaand1:150,000afterepiduralpuncture.However, recentindicationssuggestahigherincidence,asthe stud-iesusedin these calculations wereconducted beforethe perioperativethromboprophylaxisroutine.6
Aftertheintroductionofenoxaparin(30mg,twicedaily) for thromboprophylaxis in the United States,an alarming numberofcasesofepiduralhematoma,somewith perma-nentparaplegia,theriskofspinal/epiduralhematomawith twicedailyadministrationofenoxaparinwasreportedand calculatedat1:40,800afterspinalanesthesia,1:6,600after simpleepiduralpuncture,and1:3,100afterepidural punc-turewithepiduralcatheterinsertion.7 InEurope,a single doseadministrationofenoxaparin(40mg)showedalower incidenceof spinalhematoma.In aretrospective Swedish study,8 theauthors found a risk of 1:156,000 after spinal anesthesia and 1:18,000 in epidural anesthesia. Bleeding wasrareintheobstetricpopulation(1:200,000)compared withthatofwomenundergoingkneearthroplasty(1:3,600).
Subsequent studies showed incidences ashigh as 1:2,700 to 1:19,505.9---11 However, Cook et al. presented updated resultsattheThirdNationalAuditProjectoftheRoyal Col-legeofAnaesthetistsinwhichonlyeightcasesofSEHwere seen in 707,405 neuraxial blocks.Of these, onlyfive met theinclusioncriteria,andtheincidencewascalculatedat 1:88,000to1:140,000.12
RiskFactors2,4
TheoccurrenceofSEHismorespontaneousthantheresult of neuraxialanesthesia.Mostspontaneoushematomasare idiopathic;casesrelatedtoanticoagulanttherapyand vas-cularmalformationsarethesecondandthirdmostcommon causes, respectively. Concomitantuse ofanticoagulants is themain riskfactor relatedtoSEH,whenassociatedwith neuraxialblock.2
Risk factors for SEH have been described by several authors8,13---18 and are shown in Table 1. The incidence of SEHvariesaccordingtothetypeofsurgery,ageandgender of patient.For example, the incidence of SEH in obstet-ricsurgeryisestimated at1:200,000,whereasin geriatric agewomenundergoingkneearthroplastyitisestimatedat 1:3,600.8 This may be explained by the higher incidence ofspinalabnormalitiesassociatedwithosteoporosis,useof dualantiplatelet/anticoagulanttherapy,andaccumulation of anticoagulant duetoa decreasein renalexcretion not detectedinthisagegroup.
Among thetype of neuraxialblocks, therisk of SEH is higherwiththeuseofepiduralcatheters,followedbysimple epiduralpuncture,andlessfrequentaftersingle subarach-noid puncture,17,19,20 the latter likely due to the thinner needlesusedinthetechnique.Catheterremovalisas crit-icalasinsertion;therefore,vascularinjurymaystilloccur4 atthesameincidence;thatis,halfthecasesofSEHoccurs duringepiduralcatheterremoval.16
There areindications that epidural hematoma is more common after lumbar puncture compared with thoracic puncture.11
Clinicalcondition,treatment,andprevention
Bleeding into the spinal canal, which causes thecal sac compression,mayresultinirreversibleneurologicaldamage with paraplegia and is a major concern of anesthesiolo-gistsperformingneuraxialblockinpatientsonanticoagulant drugs.4
Clinicalconditionischaracterizedbyslowregressionor absent sensory or motor block, back pain,urinary reten-tion or return of motor or sensory deficit after complete regression oftheprevious block,aloneor incombination, suggestingthedevelopmentofspinalhematoma.2
SBA
R
ecommendations
for
regional
anesthesia
safety
in
patients
taking
anticoagulants
3
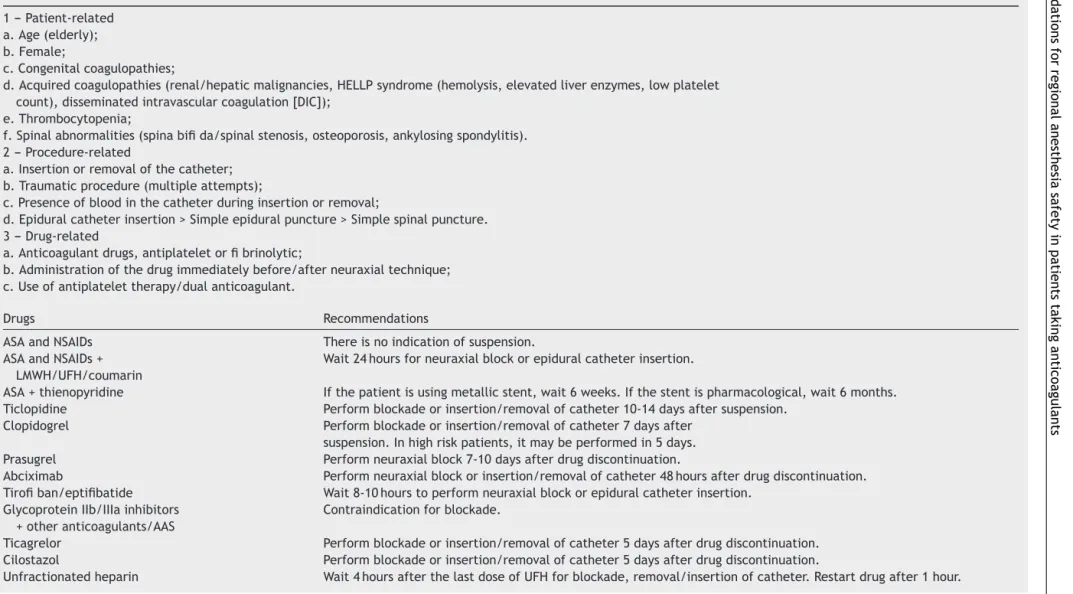
Table1 RiskFactorsAssociatedwithHematomaSpinal/Epidural.
1--- Patient-related a.Age(elderly); b.Female;
c.Congenitalcoagulopathies;
d.Acquiredcoagulopathies(renal/hepaticmalignancies,HELLPsyndrome(hemolysis,elevatedliverenzymes,lowplatelet count),disseminatedintravascularcoagulation[DIC]);
e.Thrombocytopenia;
f.Spinalabnormalities(spinabifida/spinalstenosis,osteoporosis,ankylosingspondylitis). 2--- Procedure-related
a.Insertionorremovalofthecatheter; b.Traumaticprocedure(multipleattempts);
c.Presenceofbloodinthecatheterduringinsertionorremoval;
d.Epiduralcatheterinsertion>Simpleepiduralpuncture>Simplespinalpuncture. 3--- Drug-related
a.Anticoagulantdrugs,antiplateletorfibrinolytic;
b.Administrationofthedrugimmediatelybefore/afterneuraxialtechnique; c.Useofantiplatelettherapy/dualanticoagulant.
Drugs Recommendations
ASAandNSAIDs Thereisnoindicationofsuspension.
ASAandNSAIDs+ LMWH/UFH/coumarin
Wait24hoursforneuraxialblockorepiduralcatheterinsertion.
ASA+thienopyridine Ifthepatientisusingmetallicstent,wait6weeks.Ifthestentispharmacological,wait6months. Ticlopidine Performblockadeorinsertion/removalofcatheter10-14daysaftersuspension.
Clopidogrel Performblockadeorinsertion/removalofcatheter7daysafter
suspension.Inhighriskpatients,itmaybeperformedin5days.
Prasugrel Performneuraxialblock7-10daysafterdrugdiscontinuation.
Abciximab Performneuraxialblockorinsertion/removalofcatheter48hoursafterdrugdiscontinuation. Tirofiban/eptifibatide Wait8-10hourstoperformneuraxialblockorepiduralcatheterinsertion.
GlycoproteinIIb/IIIainhibitors +otheranticoagulants/AAS
Contraindicationforblockade.
Ticagrelor Performblockadeorinsertion/removalofcatheter5daysafterdrugdiscontinuation. Cilostazol Performblockadeorinsertion/removalofcatheter5daysafterdrugdiscontinuation.
4
N.M.
Fonseca
et
al.
Table1 (Continued)
Drugs Recommendations
Lowmolecularweightheparin Prophylacticdoses:wait10-12hourstoperformblockade. Therapeuticdoses:wait24hours.Withdrawalofcatheter10-12 hoursafterlastdose.Restartdrug2hoursaftercatheterremoval.
Coumarin Performblockade4-5daysafterdiscontinuation.INRmonitoring
duringepiduralanalgesia.
Fondaparinux Prophylacticdose(2.5mg):blockademaybeperformed.Ifepidural catheter,removeit36hoursafterthelastdose.Restartdose12
hoursaftercatheterremoval.Therapeuticdose(5-10mg):blockadeiscontraindicated. Rivaroxaban Performneuraxialblockade,insertion/removalofcatheter24hours
afterdrugdiscontinuation.Restart4-6hoursaftercatheterremoval.
Apixaban Performneuraxialblockade,insertion/removalofcatheter20-30
hoursafterdrugdiscontinuation.Restart4-6hoursaftercatheterremoval.
SBARecommendationsforregionalanesthesiasafetyinpatientstakinganticoagulants 5
Thus,patientsshouldbecarefullyevaluatedto investi-gatepossiblesignsindicatingSEH,bothafterneuraxialblock andepiduralcatheterremoval.Thepatientshouldbe mon-itoredatregularintervalsuntilregressionofsensoryblock byatleasttwodermatomesormotorfunctionrecovery2and foratleast24hoursafterepiduralcatheterremoval.21
EuropeanandAmericansocietieshavepublished guide-lines with the goal of increasing security in performing neuraxialblockin patientsonanticoagulants.1,6,22---27 How-ever, most of theserecommendations areexpert opinions based on case series and pharmacological data with anticoagulant drugs involved.27 These recommendations include: (I) minimum timeinterval required between the last dose of anticoagulant and the insertion of neurax-ial needle/catheter or catheter removal; (II) minimum interval required between the insertion of neuraxial needle/catheterorcatheterremovalandnextdoseof anti-coagulant;(III)minimumcoagulationtimerequiredforthe useofneuraxialtechnique(ifavailable forthedrugbeing used).
Duetotherapiddevelopmentofanticoagulantdrugsby thepharmaceuticalindustryandtheirreleaseand increas-ing use in clinical practice, experiments are lacking and it becomesdifficult tomake anystatementonthe useof neuraxialanesthesiainpatientsonnewanticoagulants.
Recently, Rosencheretal.proposed anewstrategyfor managing patients on new anticoagulants.28 According to this strategy, the insertion and subsequent withdrawal of neuraxialneedle/cathetermustbemadeatatimesuperior totwohalf-lives of elimination after thelast dose of the usedanticoagulant.Thebasis forthisproposalisthat30% to40%ofthefunctionofcoagulationfactorsisrequiredfor hemostasis,sothatafter twohalf-lives, thedrug concen-trationin bloodstreamisnear25% oftheinitial.The next anticoagulantdoseshouldbeadministeredwithatime inter-val(dT) obtained by subtractingthe timeneeded for the drugtoreachthepeakplasmalevelandthetimetoproduce stablebloodclot,considered8hours(8h-Tpeak=dT).28
Neuraxialblockanduseofantiplateletagents
Antiplatelet drugs consist of non-steroidal anti-inflammatory drugs (NSAIDs), thienopyridines (ticlopidine, clopidogrel, and prasugrel), and glycoprotein IIb/IIIa inhibitors(abciximab,eptifibatide,andtirofiban).
Acetylsalicylicacid(ASA)andNSAIDs
ASApromotesirreversibleblockadeofplateletfunctionby inhibitingcyclooxygenaseenzymeproductionof thrombox-aneA2(potentplateletactivator).Thiseffectlaststhesame astheplatelets’half-life,usually7-10days.3
OtherNSAIDsalsoinhibitcyclooxygenase-1andplatelet aggregation, but in a reversible manner and proportional to the agent half-life. This process normalizes from 12 to 24hours after NSAIDs discontinuation.29 The selective inhibitors of Type 2 cyclooxygenase (COX-2) are anti-inflammatorydrugsthatdonotcauseplateletdysfunction, asCOX-2isnotexpressedinplatelets.30
The bleedingeffectcausedbyASA appearstobe dose-dependent,withmoremarkedeffectsinpatientsreceiving
doses greater than 100mg.day-1 31 However, prospective studies evaluatingthe safety of neuraxial block with ASA reportednocaseofspinalhematoma.32---34
AlthoughtheisolateduseofASA seemsnottoincrease the probability of spinal hematoma, complications have been observed in both medical and surgical patients, if combinedwithheparin.14,35Thus,inindividualsusingASA, it seems prudent to administer heparin for postopera-tivethrombosisprophylaxis, astheresearchteamdidnot observesuperiorityofthromboprophylaxiswhentheheparin doseisgivenpreoperatively(B).36However,the administra-tionofalow-dosecombinationofASA-dipyridamoleseems nottoincreasetheriskofspinalhematoma.2
In patients with a history of acute coronarysyndrome (ACS),cerebrovascularaccident(CVA)orperipheralarterial occlusive disease, ASA reduces the risk of recurrent car-diovasculareventsby 30%andmortalityby approximately 15%.37 Recent studies suggest that morbidity and mortal-ity,particularlyinpatientswithnewlyimplantedcoronary stentsorunstablecoronarysyndromeismarkedlyincreased if ASA is suspended before a surgical procedure.38---40 Rebound phenomenon hasalsobeen described.41 The risk of late thrombosis is higher in patients with drug-eluting stents.
Insummary,theperioperativesuspensionofASAis unnec-essaryinmostcasesandassociatedwithanincreasedrisk of acute thrombosis. We recommend that patients with ACSor stentshouldcontinue takingASAthroughout life.42 TheAmericanCollegeofChest Physicians(ACCP) doesnot recommend platelet function evaluation prior to invasive proceduresbecausethereis no apparent correlation with bleeding(D).43
Recommendations
1. NSAIDsappeartorepresentnosignificantadditionalrisk for the onsetofspinal hematomain patients undergo-ingepiduralorspinalanesthesia.NSAIDs(includingASA) havenorisklevelthatinterfereswiththeperformanceof neuraxialblocks.Inpatientsonthesemedications,there is no specific concern regarding the interval between spinal/epidural puncture or catheterinsertion andthe lastdoseofthegivendrug,ortheneedforpostoperative monitoringandintervalforcatheterremovalor postop-erativedrugadministration(A).6,32---34
2. Concomitant use of medications affecting other clot-ting mechanism components, such as oral anticoagu-lants, unfractionated or low molecular weight heparin increasestheriskofbleedingcomplicationsinpatients onNSAIDs.InthesepatientsonASA,theadministrationof heparindosageforpostoperativethromboprophylaxisis recommended(B).36 Inthesepatients,iflowmolecular weightheparin(LMWH) is administeredpreoperatively, thereshouldbea24-hourwaitperiodbeforeperforming blockadeor removing theepiduralcatheterdue tothe increasedriskofbleeding(C).6
6 N.M.Fonsecaetal.
supportingtheeffectontheabilityofplatelet aggrega-tionorincreasedtendencytobleeding(D).1
4. In patients withcoronary stentreceiving dualplatelet therapy (ASA + thienopyridine), needing surgery, and requiring surgical procedure, we recommend postpon-ingsurgeryfor atleast6weeksinthecase ofmetallic stents and at least 6 months in case of drug-eluting stents(D).43Ifpatientsneedsurgerywithin6weeksafter metallicstentor6monthsafterdrug-elutingstent,dual antiplatelettherapyshouldbemaintained,andregional anesthesiaiscontraindicatedvianeuraxialroute(D).43 5. Analgesics,suchasparacetamolanddipyrone,arenota
contraindicationforneuraxialregionalanesthesia, inso-fartherearenocasesrelatedtospinalhematoma(D).3
Thienopyridines
Ticlopidine (Ticlid®),clopidogrel (Plavix®), andprasugrel (Efient®)are platelet inhibitors belonging tothe class of thienopyridines.They are prodrugs cleaved in vivo in the liver to active metabolites that antagonize the platelet receptorofadenosinedinucleotidephosphate(ADP)(P2Y12) andinterferewithplateletactivationandaggregation,an effectthatcannotbeantagonizedandisirreversible.1,2
There is no prospective study assessing the safety of neuraxial techniques in subjects under treatment with thienopyridines.However,cases of spinal hematomahave beenreportedafterneuraxialanesthesiainpatientstaking thesedrugs.44
Ticlopidine
(Ticlid
®)
Ticlopidinehalf-lifeis30to50hours,whichincreasesupto 96hoursifusedroutinelyformorethan14days.2Platelet dysfunctionwiththeuseofticlopidineremainsfor10to14 daysafterdrugdiscontinuation.1Unlikeclopidogrel, ticlo-pidinemayleadtoneutropeniainmorethan1%ofpatients, whichisalimitingfactorofitsuse.3
Recommendations
Neuraxialblock or epiduralcatheterremoval can onlybe performedafter10-14daysofticlopidinesuspension(D).3,6
Clopidogrel
(Plavix
®)
Clopidogrel half-life is 120hours. However, its active metabolitehalf-life isonly 8hours.2The plateletfunction maximuminhibitionoforalclopidogrel(75mg)occurswithin 3-7daysor about12-24hoursafter aninitial loadingdose of 300-600mg. Recovery of platelet function occurs only 6-7 daysafter the end of clopidogrel administration.45 In patientsathighriskforangina,discontinuationforfivedays hasbeensuggestedtopreventcardiovascularmorbidity.46
Recommendations
Neuraxial blockade or removal of epidural catheter in patientsonclopidogrel shouldonlybe performed afterat leastsevendaysofdrugdiscontinuation(D).3Inthecaseof
patientswithhighriskofanginarecurrence,theintervalof fivedayssuspensionhasbeensuggested(D).6
Prasugrel
(Efient
®)
Anovel thienopyridinethat,similartoothers,dependson hepaticconversiontoactivemetabolitetobindtoplatelet P2Y12receptor(whichbindstoADPforplateletactivation) and perform its inhibitory activity. This drug has a rapid onsetofaction(30-60minutes)andis10timesmorepotent thanclopidogrel.47Theantiplateleteffectisequaltothelife ofplatelet,andpretreatmentplateletfunctionisrestored 7-10daysafterdrugdiscontinuation.3
Onestudycomparingprasugrelandclopidogrelin13,608 patients withacutecoronarysyndrome undergoing percu-taneouscoronaryinterventionshowedsignificantreduction ofischemiceventstreatedwithprasugrel,butalsoahigher andoccasionallyfatalriskofbleeding.48
Recommendations
There is no available study assessing the combination of prasugrelandneuraxialanesthesia.However,itseems rea-sonable that treatment withprasugrelbe discontinuedat least7-10daysbeforeneuraxialblockorremovalofepidural catheter(D).3
Glycoprotein
IIb/IIIa
inhibitors
Glycoprotein IIb/IIIa inhibitors include abciximab (Reopro®), eptifibatide (Integrilin®), and tirofiban (Aggrastat®). Currently, these agents are the most effective drugs available for platelet aggregation inhibi-tion, as they block the platelet glycoprotein IIb/IIIa (the siteoffibrinogen bindingbetweenplatelets),whichis the finalcommonpathwayofplateletaggregation.2Thesedrugs areonlyavailableforintravenoususe.Antiplateleteffects are reversible and disappear after the discontinuation of eptifibatide, tirofiban, and abciximab within 8, 24, and 48hours, respectively. The most common sideeffects are thrombocytopenia and bleeding,50 expressed in 0.3-1% with abciximab.49 Abciximab showedbetter efficacy than tirofibanandeptifibatide.51
Recommendations
1. According to the pharmacological properties of these drugs, insertion of epidural/spinal needle/catheter or catheterremovalshouldonlybeperformed after com-plete recovery of platelet aggregation; that is, with discontinuation of 8-10hours for tirofiban/eptifibatide and48hoursforabciximabandexclusionofany throm-bocytopeniathrougharecentplateletcount(D);2 2. GP IIb/IIIa inhibitors are used in acute coronary
SBARecommendationsforregionalanesthesiasafetyinpatientstakinganticoagulants 7
Other
antiplatelet
Ticagrelor(Brilinta®)
Unlike thienopyridines, ticagrelor acts directly on P2Y12 receptoranddoesnotrequireliverbiotransformationinto activemetabolitesbycytochromeP450,although metabo-litesarealsoactive.Similartoprasugrel,ticagrelorprovides a very fast (< 2h), intense (about 70%), and consistent inhibition of P2Y12 receptor, which is greater than that of clopidogrel (30-40%).47 It has a rapid onset of action with reversible binding and short duration (48-72h), and requiresoraladministrationintwodoses.Theinitialeffect on platelet aggregation is seen 30minutes after loading dose. Withtreatment discontinuation,plateletfunctionis restoredwithin4-5days.52
Recommendations
There is no available data regarding the perioperative use of this agent. Theoretically, its short and reversible antiplatelet effect can facilitate perioperative manage-ment.However,neuraxialanesthesiashouldbediscouraged duringtreatmentwithticagrelor,unlessitissuspendedfor atleastfivedaysbeforetheanestheticprocedure,sothat plateletfunctioncanreturntonormal(D).3
Cilostazol
(Vasogard
®,
Cebralat
®,
Pletal
®)
Cilostazolprovidesselectiveinhibitionofphosphodiesterase IIIa (PDEIIIa); thus, it increases the level of intracellu-lar cyclic adenosine monophosphate (cAMP) and leads to weak platelet aggregation inhibition.53,54 Because vascu-larsmoothmusclecontainsPDEIIIa,cilostazolalsoprovides directarterialvasodilation.Nevertheless,cilostazol mech-anismofactionisnotfullyunderstood.Itsuseisindicated forperipheralarterialdiseaseandintermittentclaudication inindividuals whodonotrespondtoexercisetherapy and thosewithlowpossibilityofsurgicalintervention.55
Therouteofadministrationisorallyatadoseof100mg twicedaily,andpeakplasmalevelisachievedwithin2.7to 3.6hours.Drugcompoundis mainlyeliminatedby hepatic metabolism and subsequent urinary excretion of metabo-lites.Theterminaleliminationhalf-lifeofcilostazolandits activemetabolitesisapproximately21hours,andsomeofits metabolitesinhibitplateletaggregationatahigherintensity thantheparentcompound.54
Arecentcasereportfoundspinalhematomaafter epidu-ralcatheterremovalduringtreatmentwithcilostazol,56but, ingeneral,thereisnoprospectivedataonthisdrug’s periop-erativeuseanditseffectonbleedingincidenceisunknown.
Recommendations
Neuraxial block and catheter removal may be performed considering the minimum clearance interval of two half-livesbetweenblockadeandthelastdoseofcilostazol(i.e., 42hours),althoughlaboratoryrecommendationisfivedays ofsuspension.3The nextdose ofcilostazolshouldonly be administered5hoursaftercatheterremoval(D).28,57
Heparins
Unfractionatedheparin(UFH)
The majoranticoagulant effect of heparinis due to pen-tasaccharide present in one third of heparin molecules, whichbindstoantithrombinIII (ATIII).6 Afterthisbinding, UFHcatalysestheinactivationofIIa(thrombin),IXa,andXa, and,toalesserextent,XIaandXIIafactors.4Intheabsence ofheparin,antithrombin IIIhas low affinityfor thrombin. However, when UFH binds to ATIII, the thrombin-binding rateacceleratesfrom100to1,000times,similarlytoother coagulationfactorsinhibitedbyit.UFHalsobindsstrongly toseveralplasmaproteins,endothelialcells,macrophages, andplateletfactor 4 (PF4), whichresults inlow bioavail-ability, inaccuratepharmacokinetics, andheparin-induced thrombocytopenia(HIT).58
The anticoagulantactivity ofUFHdependsonboththe number of heparin molecules with the pentasaccharide chaininitscompositionandthesizeofmoleculescontaining thepentasaccharide. The high molecular weightheparins will catalyze the inhibition of Xa and IIa factors, while thelowmolecularweightheparins willonly inhibittheXa factor.58,59
Intravenousadministrationof UFHresultsin immediate anticoagulation,whilesubcutaneousadministrationresults inonsetofactionwithin1-2hours.Theanticoagulanteffect isboth molecularweightanddosedependent, ina nonlin-earmanner,andincreasesdisproportionatelywithincreased dose.6 The biological half-life of heparin increases from 30minuteswith25UI.kg-1 IVto60minuteswith100UI.kg-1 andto150minuteswith400UI.kg-1.59
When given in therapeutic doses, UFH anticoagulation ismonitored bytheactivatedpartial thromboplastin time (aPTT).Duringcardiopulmonarybypass,coagulation inhibi-tionbyhighdosesofheparinismonitoredbytheactivated clottingtime(ACT).Subcutaneous administrationof small doses(5,000 IU) for prophylaxis of deepvenous thrombo-sis (DVT) usually does not change the aPTT. One of the advantagesofheparinanticoagulationisthereversalby pro-tamine.Eachmilligramofprotaminecanneutralize100IU ofheparin.58
A review study of more than 9,000 patients undergo-ing neuraxial block with prophylactic doses for DVT with heparinshowedno casesof spinal hematoma.60 However, isolated cases have been reported subsequently to that revision.9,16,10,61---63 In patients receiving two- daily dose regimenof subcutaneous UFH(5,000 IU) thereis no con-traindicationfortheuseofneuraxialtechniques.6However, thereareinsufficientdatatoconfirmthesafetyof neurax-ialtechniqueswiththreedailydoses,despitebeingthemost effectivedosageforDVTprevention.64
8 N.M.Fonsecaetal.
Recently, twocases of epiduralhematoma were reported associatedwithUFHtherapyandneuraxialblock.65,66
Heparinizationduringsurgery involvestheuse of5,000 to10,000 U of heparinintravenously during surgery, par-ticularlyin vascular surgery toprevent thrombosisduring artery clamping.59 Most published cases series uses the same guidelines for neuraxial anesthesia management in thesepatients,basedontheexclusionofhigh-riskpatients (preexisting coagulopathy) and performing the neuraxial techniqueatleastonehourbeforeheparinadministration.60 Stafford-Smith showed increased incidence of bleeding in patients on ASA associated with intraoperative intra-venousheparin.SEHriskincreasedto1:8,500afterepidural puncture and to 1:12,000 after spinal anesthesia, even when neuraxial anesthesia and subsequent heparinization occurredafterone-hourinterval.35
Incardiacsurgery,thebenefitsofthoracicepidural anes-thesia on pulmonary function and analgesia are evident, with lower intensity for arrhythmia management and no effectonhospitalandICUlengthofstayandmortality.67,68 However, the benefits must be evaluated concerning the high risk of SEH. The probability of spinal hematoma in patients undergoing cardiac surgery with full hepariniza-tion is 1:1,528 with epidural and 1:3,610 with spinal techniques.69,70Expertsrecommendthatneuraxialblockbe performedthedaybeforesurgeryduetocompletesurgical heparinization.22,71,72Becauseneuraxialblockadeincardiac surgerycarriessignificantriskswithoutimprovingmorbidity andmortality,thereisdiscussionwhetherepiduralorspinal anesthesiaisjustified,probablywiththecontraindicationof thetechniqueinthisgroup.72
Recommendations
1. InpatientsontwodailyprophylacticdosesofUFH(5,000 IU)therearenocontraindicationstoneuraxialblock(D);6 2. The safetyof neuraxialblockinpatients receiving pro-phylactic doses of UFH above10,000 IU or above two dailydosesisnotestablished.Althoughdosageofthree daily dosesmay leadtoincreasedsurgical bleeding, it is unclearwhetherthereisan increasedriskfor spinal hematomadevelopment(D);6
3. Because heparin-induced thrombocytopenia (HIT) may occur duringUFHadministration, plateletcountshould bedonebeforeneuraxialtechniqueorcatheterremoval, ifthepatientisonHNFforfiveormoredays(B);3 4. Waitaminimumintervalof4hoursbetweenthelast
pro-phylactic dose of UFHand spinal/epiduralpuncture or epiduralcatheterremoval.Thenextdoseof prophylac-ticUFHshouldbeadministeredatleastonehourafter neuraxialanesthesiaorepiduralcatheterremoval(D);3 5. IfUFHis usedin therapeuticdoses toperform
neurax-ialanesthesia,administrationofcontinuousintravenous heparin therapy should be discontinued for at least 4hoursbeforepuncture or catheterremoval, andit is necessarytocheckthereturnofnormalcoagulationby determiningaPTTorACT(D);3
6. Insituationsofintraoperativeheparinization,the follow-ingrecommendationsshouldbeconsidered:1)minimum intervalofone-hourbetweenpunctureorcatheter place-ment and heparinization;2) donot performneuraxial
block in patients with coagulopathy or on anticoagu-lants;3)wait4hoursbetweenthelastdoseandepidural catheter removal,preferably with laboratory coagula-tiontests;4)aftercatheterremoval,waitonehourfor UFHdoseapplication;5)althoughtheoccurrenceof diffi-cultpunctureorbloodoutputfrompunctureneedlemay increasetheriskofspinalhematoma,therearenodata tojustifysurgerycancellation(A).6
Low
molecular
weight
heparin
(LMWH)
LMWHhasbecomethetreatmentofchoiceforboth preven-tionandtreatmentofDVT,duetothegreaterbioavailability (almost 100%) after subcutaneous administration, which results in higher anticoagulant effect without increasing bleeding tendency and ease of use without the need for bloodcoagulationmonitoring.2
PharmacologyofLMWHdiffersfromUFH.Themain dif-ferences are the highest inhibitory activity against the Xa factor compared with thrombin (IIa), anticoagulant effectdifficultmonitoring(factorXalevels),prolonged half-life, and lack of complete reversibility with protamine.58 Withsubcutaneous administration, peakplasmalevelsare reached in approximately 3-4hours, and the half-life of elimination, with normal renal function, is within 4-6hours.73,74 However, the anti-factor Xa activity remains considerable (50%) after 10-12hours of administration. If creatinine clearancefalls below 30mL.min-1, thehalf-life doubles.74 ComparedtoUFH,theriskofthrombocytopenia (HIT)is10timeslower.However,theyarecontraindicated inHITduetothehighriskofcross-reaction,approximately 90%.75
Ifthromboprophylaxis withLMWH is prescribed in two dailydoses(30mg),comparedtoadailydoseregimen,the riskofspinalhematomamaybeincreased,astheminimum levelsofanti-Xaactivityarehigher.76
TheuseofLMWHinpatientsundergoingneuraxialblock wasadoptedinEuropein1987.Dosagesusedwere20-40mg in a single dose 12hours before surgery. To prevent the occurrence of spinal hematoma, guidelinesrecommended insertion/removalofepiduralcatheterataminimum inter-val of 10-12hours after the last dose of LMWH. The subsequent dose was restarted after 8-12hours.5,16 Thus, reviewsinvolvingdatafrommillionsofpatientsshowedthat theuse ofneuraxialblockinsubjects onLMWHunderthe Europeanregimewassafe,withreportofonlyonecase of spinalhematoma.77,78
SBARecommendationsforregionalanesthesiasafetyinpatientstakinganticoagulants 9
for neuraxial blockand LMWHadministration; (iv) lack of largerseries.19,24
AftertheSecondAmericanSocietyofRegionalAnesthesia (ASRA)resolutionin 2003,studiesin theEnglishliterature reported10casesrelatedtothecombinationofLMWHand spinalhematoma.Fiveadditionalcaseswerereportedbythe RoyalCollegeofAnesthetistsConsensusintheUKin97,925 epiduralblocks,butwithoutprovenevidenceofassociation withanticoagulantdrugs.12
Recommendations
1. Antiplateletdrugsandoralanticoagulantsconcomitantly administered with LMWH increase the risk of spinal hematoma,andinsuchconditionsblockadeis contraindi-cated.InpatientsonASA,itseemsprudenttoadminister thethromboprophylaticdoseofheparinpostoperatively (B).36Inthesepatients,ifLMWHisadministered preop-eratively,wait24hourstoperformblockadeorcatheter removalduetoincreasedriskofbleeding(C);6
2. Bleedingduringneedleorcatheterinsertiondoesnot jus-tifysurgerycancellation.Thebeginningoftherapywith LMWHinthis circumstanceshould occur24hoursafter theendofsurgery(D);6
3. In preoperative patients receiving LMWH thrombopro-phylaxis, neuraxial block is recommended 10-12hours afterthelastdoseofLMWH(D);6
4. InpatientsontherapeuticdosesofLMWH,suchas enoxa-parin 1mg.kg-1 every 12hours, enoxaparin 1.5mg.kg-1 perday,dalteparin120IU.kg-1every12hours,dalteparin 200IU.kg-1perdayortinzaparin175IU.kg-1perday,an intervalofatleast24hoursisrecommendedbetweenthe lastdoseandneuraxialblocktoensurenormal hemosta-sis(D);6
5. Patients under prophylactic regimen of LMWH every 12hours(enoxaparin30mgtwicedaily),onedoseshould beomittedtoenablea24hoursintervalbeforeneuraxial blockorcatheterremoval(A);3
6. RegardingLMWHpostoperativeuse,thefirstdoseshould beadministered6-8hoursaftersurgery.Aseconddoseof LMWHshouldnotbeadministeredbefore24hoursofthe firstdose. Thus,epiduralcathetermaybesafely main-tained.However,epiduralcatheterremovalshouldonly bedone after10-12hoursof thelast dose. The subse-quentdose of LMWHaftercatheterremovalshould be administeredafter2hours.Nodrugsthatalter hemosta-sisshould be given due tothe risk of additive effects (D);6
7. Inpatients undertwice daily dosage regimen,thereis greaterriskofspinalhematoma,andcontinued monitor-ingisrecommended.ThefirstdoseofLMWHshouldbe administered24hoursaftertheendofsurgery,regardless oftheanesthetictechnique,andonlyinthepresenceof adequatesurgical hemostasis.Epiduralcathetershould beremovedbeforerestartingLMWHregimen.Ifthe tech-nique of continuous analgesiais chosen, catheter may be maintained until the morning of the day following surgery,providedthatremovedbeforethefirstdoseof LMWH,whichmaybeadministered2hoursaftercatheter removal(D).6
Vitamin
K
antagonists
(coumarins)
Vitamin K antagonists include acenocoumarol, phenpro-coumon,and warfarinas. These drugs inhibit the gamma-carboxylationsynthesisofvitaminK-dependentfactors(II, VII,IX,X)andCandSproteins,whichmakesthemunable tobind phospholipidin plateletmembranesduring coagu-lation.Prothrombintime(PT)andinternationalnormalized ratio(INR)aretestscommonlyusedtomonitorthesedrugs andreflectthe plasma activityof three(II, VII, andX) of thefourclottingfactors.Clinicalexperiencessuggestthat the40% activity level of each factor is adequate for nor-malhemostasis,or nearnormal.80 INRof 1.5isassociated with the 40% activity of factor VII.81 Because factor VII hasashorter half-life (about 6hours), theinitial increase ofINRwhencoumarinanticoagulantsareusedreflectsthe lossof factor VII activity.However,thesedrugs therapeu-ticeffect is more dependent on the reduction of factors II and X, which have half-lives relatively longer, 60 to 72hoursand24to36hours,respectively.Afterwarfarin dis-continuation, factor II is the latest tonormalize.82 Thus, after drug discontinuation, INR may return to near nor-mal values due to the activity restoration of factor VII. However,factors II and X may not have been restored to normalhemostaticlevels.81Itsanticoagulanteffectcanbe effectivelypreventedbyvitaminK,freshfrozenplasmaor prothrombincomplexconcentrate(II,VII,IX,andXfactors) administration.2
AlthoughtheASRAhasrecommendedepiduralcatheter removalwith INR less than 1.5, this value hasbeen con-sidered as conservative. Reports show epidural catheter removalwithINRhigheranduneventful.83,84 Ifitoccursin thefirst48hoursof medicationuse,it islikelythat there areadequatelevelsofclottingfactorsactivity,particularly IIandXfactors.Beyondthisperiod,allvitaminK-dependent clottingfactorswillbeaffected.Therewasnoreportedcase of spinal hematoma in 11,235 patients receiving epidural analgesia after total knee arthroplasty, and treated with warfarin(5-10mg)startedthenightbeforetheprocedure. Epiduralcatheterswereremoved 48hourspostoperatively. MeanINR at recession timeof was 1.5(0.9-4.3). INR was lessthan 1.5 in approximately40% of cases. These series suggest that notonly the INR value should be considered duringepidural cathetermanagement, but alsothe dura-tionoftherapywithwarfarin,andthataprolongedtimefor morethan48hoursmayrepresentsignificantincreasedrisk ofhematoma.84
Perioperative management of patients on warfarin remainscontroversial.Recommendationsarebasedondrug pharmacology,clinicallyrelevant levels,anddeficiency of vitaminK-dependentclottingfactors,caseseries,andspinal hematomareports.6
Recommendations
10 N.M.Fonsecaetal.
VIIactivity).AppropriatelevelsoffactorsII,VII,IX,and X maynotbepresent untilINR iswithinthereference range(B);6
2. Ifwarfarinthromboprophylaxiswasinitiated postopera-tively,removeneuraxialcatheterwithanINRlessthan 1.5.Thisvaluewasobtainedfromstudiesthatcorrelated hemostasis with clotting factor activity levels greater than40%.Inthese,neurologicalmonitoringmustbekept forleast24hoursaftercatheterremoval(D);6
3. When replacing coumarin by LMWH or UFH preopera-tively,considertheUFHandLMWHrecommendationsfor neuraxialblock(D);2
4. If patient is on low doses of warfarin during epidural analgesia,INRmonitoringshouldbedonedaily(D).6
Factor
Xa
inhibitors
Fondaparinux(Arixtra®)
Fondaparinuxisasyntheticselectivepentasaccharidethat indirectly inhibits factor Xa. Unlike the LMWH, it has no effect on factor IIa (thrombin). Platelet aggregation is unaffected.3 This compound has approximately 100% bioavailabilityaftersubcutaneousadministrationand half-lifeofeliminationof18-21hours,primarilybythekidneys. Half-lifeisprolongedto36-42hourswhencreatinine clear-ance is less than 50mL.min-1, and is contraindicated in patientswithclearancelessthan30mL.min-1.85 Prophylac-ticdoseis2.5mgviasubcutaneousroutoncedaily.
Fondaparinux is usually administered 6-12hours after surgery,asitspreoperativeusemayincreasetheriskof sur-gicalbleedingwithoutimprovingantithromboticefficacy.86 Becauseit is usedpostoperatively,thereare noproblems withsinglepunctureneuraxialanesthesia.However,ifthe catheter is inserted, it should be removed only in the absence of fondaparinux plasma levels. The recommen-dations for epidural catheter management in patients on fondaparinuxarebasedontheconditionsusedinthestudy bySingelynetal.87Thisstudyevaluated5,387patients,of whom1,428underwentregionalanesthesia,andthesingle doseoffondaparinuxthenightbeforecatheterremovalwas omitted.Thus, the research team ensured an interval of 36hoursbetween thelast dose andcatheterremovaland 12hoursbetweencatheterremovalandthesubsequentdose offondaparinux.Therewasnocaseofspinalhematomaand noincreasedriskofDVT.87
According tothe American Collegeof Chest Physicians (ACCP), evenwithtwo reportedcases of HIT with fonda-parinux,itsuseinpatientswithahistoryofHITissuggested asanoptiontoUFHorLMWH.88
Recommendations
1. Atprophylacticdose(2.5mg)fondaparinuxmaybeused in postoperative withatraumaticneuraxial anesthesia. Ifused,epiduralcathetershouldberemovedonlyafter 36hoursofthelastdoseandthesubsequentdose admin-isteredonlyafter12hoursofremoval(D);3
2. Neuraxial aneshesia is contraindicated when fonda-parinux(5-10mg.day-1)isusedintherapeuticdosesdue
totherisk ofunpredictableresidualeffectinthebody (D).3
Rivaroxaban
(Xarelto
®)
RivaroxabanisaselectiveinhibitoroffactorXa.Itisorally administeredandapproved forDVTprevention aftertotal knee and hip replacement surgery. Treatment is initiated 6-8hours aftersurgery; withasingle dose of10mg,peak plasmalevelsareachievedin2-4hours.Studiesshowbetter efficacycomparedtoenoxaparinforthromboprophylaxis,89 aswellascomparedtoheparinsandvitaminKantagonists fortreatingDVT.90
Rivaroxabanhasa half-lifeof 5-9hours,ispoorly influ-encedbyrenalfunction(33%clearanceoccursviakidneys), asitalsohashepaticclearance.However,intheelderly,the half-lifemaybeprolongedto11-13hours.3
RivaroxabanprolongsaPTTandHepTest,butthesetests arenot recommendedto evaluatethe drug anticoagulant effect.91 Prothrombin time (PT) is influenced by rivarox-aban in a dose dependent manner, with closecorrelation withplasma concentrations,92 andshould bemeasured in secondsandnotbyIRN.However,routinemonitoringisnot considered necessary.Similartomostnewanticoagulants, rivaroxabancannotbeantagonized.2
Recommendations
1. Due to the lack of prospective studies, an interval greater than two half-lives of elimination is recom-mended(24hours)toperformneuraxialblockorepidural catheterremoval;28
2. Becausepeakplasma leveloccurswithin2-4hours,the subsequentdoseshouldbegiven4-6hoursaftercatheter removal(D);28
3. Ifthereistraumaticpuncturewithbleeding,rivaroxaban shouldbedelayedfor24hours(D).91
Apixaban
(Eliquis
®)
ApixabanisadirectfactorXainhibitor,administeredorally. It has 60% bioavailability and does not require biotrans-formation for activation.93 In contrast with vitamin K antagonists, apixaban does not interact with food. Peak plasma levels are reached in 3hours, half-life is about 12hours(10-15hours),andtwodailydosesarerequired.93,94 Thereisnoneedforroutinecoagulationmonitoring.Kidneys eliminateonly25%andthehepaticandbiliarymetabolisms eliminate75%,excretedviathebowel.
SBARecommendationsforregionalanesthesiasafetyinpatientstakinganticoagulants 11
Recommendations
1. Usethesamerulesfornewanticoagulants;i.e.,interval oftwohalf-livesofelimination(20-30hours)toperform neuraxialblockorremoveepiduralcatheter(D);3 2. Aftercatheterremoval,restartapixabanwithin4-6hours
(D).3
Thrombin
inhibitors
Dabigatran(Pradaxa®)
Dabigatran is a new thrombin reversible inhibitor orally administered and recently approved for DVT prophylaxis in patientsundergoinghipor knee replacementsurgery.99 Dabigatranisadministeredastheprodrug(dabigatran etex-ilate),whichisconvertedtodabigatranbyplasmaesterases. This compound has a half-life of 12-17hours, eliminated mainly by the kidney, and cannot be antagonized. After administration,peakplasmalevelsarereachedin2-4hours. Effectsofcontinuoususemaypersistfor5-7days,depending onrenalfunction.1
Treatment is initiated 1-4hoursafter surgery at doses ranging from 75mg (creatinine clearance 30-50mL.min-1) to 110mg (normal renal function). Dosage is escalated to150mgto 220mg onsubsequent days.Dabigatran pro-longs aPTT without linear effect. Thrombin time (TT) is particularly sensitive and reference for anticoagula-tion management, with linearity between dose-response intherapeutic concentrations.1 Anticoagulationreversalis theoreticallypossiblebyadministrationofrecombinant fac-torVIIa,althoughnotclinicallytested.100
The effectiveness of dabigatran(220mg) for DVT pre-vention is compared to that of enoxaparin (40mg.day-1) and without increased bleeding.101 Preliminary studies of dabigatranandneuraxialblockwereconductedwith epidu-ralcatheterremoval4-6hoursbeforethefirstdose. There is nostudy of patients on dabigatranand use of epidural catheters.
Recommendations
1. Because DVT prophylaxis with dabigatran is initiated postoperatively,thereisnolimitationtosimpleneuraxial block(D);3
2. Dabigatrandiscontinuationshouldbeatleastsevendays beforeneuraxialblocktoallowreturntonormal coagu-lation(D);1
3. The half-live of 12-17hours suggests a 34hours inter-valbetweenthelastdoseandcathetermanagementor removal.However,themanufacturer’s102 recommenda-tionistoavoidepiduralcatheterinpatientsonthisdrug andthatthefirstdose shouldbeadministeredatleast 2hoursaftercatheterremoval(D);3
4. However,becauseplasmalevelcanbereachedin2hours, itis prudenttoobserve aminimum intervalof 6hours aftercatheterremovaltostartdrugadministration(D).2
Argatroban
(Argatra
®)
Argatroban is a direct thrombin reversible inhibitor that bindstothedifferentformsofthrombin.103,104Itisindicated for patients with thrombosis associated with heparin-inducedthrombocytopenia(HIT)bythelack ofinteraction withplateletfactor4(PF4).2
ArgatrobanisadministeredbycontinuousIVinfusionand eliminatedexclusivelybytheliver,andmaybeusedinrenal failure.Thedoseof0.5-2g.kg.min-1isadjustedtomaintain aPTTwithin1.5to3ofthenormalvalue. Inpatientswith good liver function, aPTT normalization occurs 2-4hours fromthe end of infusion due tothe shorthalf-life of 35-45minutes.105
Recommendations
1. Theinsertionofspinal/epiduralneedle/cathetershould bemadeatleast4hoursafterdrugdiscontinuation.The drugreintroductiontimeaftertheblockadeorcatheter removalis2hoursandalwaysexcludedresidual coagu-lanteffectbyaPTTandACTmeasurements(D);2 2. Ifthepatientisunderargatrobantherapydueto
diag-nosisofacuteHIT,treatmentshouldnotbediscontinued becauseoftheriskofthromboembolismand,therefore, blockadeiscontraindicated(D).2
Desirudin
(Iprivask
®)
e
lepirudin
(Refludan
®)
Recombinant hirudins (lepirudin and desirudin) are from the firstgeneration of direct thrombin inhibitors and are parenterallyadministered. They have nointeraction with platelet factor 4 (PF4) and, therefore, do not trigger heparin-inducedthrombocytopenia(HIT).Desirudinis indi-catedforDVTprophylaxisandlepirudinforDVTtreatment ofpatientswithhistoryofHIT.3
Both lepirudin and desirudin have half-lives of 1.3-2hours,but it increasessignificantly inrenal failure.Due tothepotentialriskofbleeding,theanticoagulanteffectof hirudinshouldberoutinely monitoredwithaPTTor ecarin clottingtime(ECT).106
Recommendations
1. In patientswithnormalrenalfunction, wait8-10hours fromlastdosetoperformneuraxialblockwithorwithout epiduralcatheterinstallation(D);3
2. In patientswithnormalrenalfunction, wait8-10hours fromlastdosetoremovecatheter(A);3
3. Wait 2-4hourstorestartthesedrugs afterpuncture or epiduralcatheterremoval(D);3
4. Absenceof residualanticoagulant effectshouldalways beconfirmedbydeterminingaPTTandECT(D).3
Neuraxial
block
and
laboratory
tests
12 N.M.Fonsecaetal.
Platelet function appears to be more important than theisolatednumberof, platelet.107 Researcherssuggest a platelet count greater than 50,000.mm-3 with preserved functionasacceptable,whileaplateletcountgreaterthan 100,000.mm-3isacceptablewithoutconsideringevaluation testofplateletfunction.108,109
A recent study reported that in the absence of risk factors, platelet count > 80,000.mm-3 is considered safe to perform spinal/epidural blocks and platelet count > 40,000.mm-3toperformsimplelumbarpuncture.110
Regarding secondary hemostasis,the40% activity level of each factor is adequate or near normal for normal hemostasis.80INRof1.5isassociatedwiththe40%activityof factorVII.Bleedingmayoccurifthelevelofanycoagulation factorisreducedto20-40%ofitsnormalvalue.81
Recommendations
1. Epiduralorspinalblocks,intheabsenceofriskfactorsfor bleeding, maybeperformedwithplateletcountabove 80,000.mm-3(D);110
2. INR<1.5isconsidered safetoperformneuraxialblocks (D).6
Peripheral
nerve
blocks
and
anticoagulants
Although spinal hematoma is the most important hemor-rhagiccomplicationof regionalanesthesiabecause ofthe catastrophicnatureof bleedingintoarestrictedand non-compressible space, the associated risk after plexus and peripheralnerveblocksremainsundefined.
Thepresenceofhematomamayincreasemorbidityand mortality,andtherearereportedcasesinvolving retroperi-toneal hematomaafter lumbar plexus block withthe use ofenoxaparinor clopidogrel. Inone ofthese reports,the catheter inserted into the lumbar plexus was removed 1.5hoursafterthelastdoseofheparin.111,112
Althoughmostofthecaseshaveevolvedwithout neuro-logical damage, therewasextension of the hospitalstay, with injury and patient dissatisfaction, as well as need for transfusion of packed red blood cells. Some showed deficitsengines andsensitives,renal failureanddeathby bleeding.111---113
The German Society of Anesthesiology and Intensive CareMedicine adoptsthesamerecommendationsfor neu-raxial,peripheral nerve, andplexus blocksin patients on antithrombotic drugs.114 The Austrian Society differenti-ates neuraxial blocks from deep or superficial peripheral blocks.115 Theselatter, similarto axillary brachialplexus, femoralnerve,anddistalsciaticblocks,maybeperformed withtheuseofASAandanticoagulants.115
Withtheincreasinguse ofultrasoundtoaid peripheral nerveandplexusblocks,thenumberofcomplications,such as vascular puncture, decreased because of the dynamic visualization of structures adjacent to the nerve to be blocked.116 Thus, evidenceprobably willdemonstrate the actual decreasein complicationrates with thistechnique and,therefore,recommendtherelativelysafeuseof periph-eral nerve blocks guided by ultrasound in anticoagulated patients.
Recommendations
1. RespecttheintervalbetweenLMWHadministrationand insertion/removalofcatheterssimilartothoseusedfor neuraxialblocks(D);3
2. Donotremoveanycatheterintheperiodof anticoagu-lantgreatestactivity(D);3
3. Because morbidity is associated with retroperitoneal hematoma,paravertebral orlumbarplexusblockshave the same recommendations used in neuraxial blocks (D).111
4. Superficialblocks,suchasaxillary,femoralordistal sci-atic,maybeperformedwiththeuseofanticoagulation orantiplatelettherapy(D).111
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Horlocker TT. Regional anaesthesia in the patient receiv-ing antithrombotic and antiplatelet therapy. Br J Anaesth. 2011;107:96---106.
2.Vandermeulen E. Regional anaesthesiaand anticoagulation. BestPractResClinAnaesthesiol.2010;24:121---31.
3.Gogarten W, Vandermeulen E,Van Aken H, et al. Regional anaesthesiaandantithromboticagents:recommendationsof theEuropeanSocietyofAnaesthesiology.EurJAnaesthesiol. 2010;27:999---1015.
4.GreenL,MachinSJ.Managinganticoagulatedpatientsduring neuraxialanaesthesia.BrJHaematol.2010;149:195---208. 5.TrybaM.Epiduralregionalanesthesiaandlowmolecular
hep-arin: Pro.Anasthesiol IntensivmedNotfallmed Schmerzther. 1993;28:179---81.
6.HorlockerTT,BirnbachDJ,ConnisRT,etal.Practiceadvisory fortheprevention,diagnosis,andmanagementofinfectious complicationsassociatedwithneuraxialtechniques:areport bytheAmerican Societyof AnesthesiologistsTask Forceon infectiouscomplicationsassociatedwithneuraxialtechniques. Anesthesiology.2010;112:530---45.
7.SchroederDR.Statistics:detectingarareadversedrug reac-tion using spontaneous reports. Reg Anesthesia Pain Med. 1998;23:183---9.
8.Moen V, Dahlgren N, Irestedt L. Severe neurological complications after central neuraxial blockades in Sweden 1990-1999.Anesthesiology.2004;101:950---9.
9.Cameron CM, Scott DA, McDonald WM, et al. A review of neuraxial epidural morbidity: experience of more than 8000 cases at a single teaching hospital. Anesthesiology. 2007;106:997---1002.
10.ChristieIW,McCabeS.Majorcomplicationsofepidural anal-gesiaaftersurgery:resultsofasix-yearsurvey.Anaesthesia. 2007;62:335---41.
11.PoppingDM,ZahnPK,VanAkenHK,etal.Effectivenessand safetyofpostoperativepainmanagement:asurveyof18925 consecutivepatientsbetween1998and2006(2ndrevision):a databaseanalysisofprospectivelyraiseddata.BrJAnaesth. 2008;101:832---40.
SBARecommendationsforregionalanesthesiasafetyinpatientstakinganticoagulants 13
13.BremSS,HaflerDA,VanUitertRL,etal.Spinalsubarachnoid hematoma:ahazardoflumbarpunctureresultinginreversible paraplegia.NEngJMed.1981;304:1020---1.
14.RuffRL,DoughertyJrJH.Complicationsoflumbarpuncture followedbyanticoagulation.Stroke.1981;12:879---81. 15.Owens EL, Kasten GW, Hessel EA. Spinal subarachnoid
hematomaafterlumbarpunctureandheparinization:acase report,reviewoftheliterature,anddiscussionofanesthetic implications.AnesthAnalg.1986;65:1201---7.
16.Vandermeulen EP, Van AH, Vermylen J. Anticoagulants and spinal-epiduralanesthesia.AnesthAnalg.1994;79:1165---77. 17.Wulf H Epidural anaesthesia and spinal haematoma. Can J
Anaesth.1996;43:1260---71.
18.HorlockerTT,WedelDJ.Neuraxialblockand low-molecular-weight heparin: balancing perioperative analgesia and thromboprophylaxis.RegAnesthPainMed.1998;23:164---77. 19.TrybaM,WedelDJ.Centralneuraxialblockandlowmolecular
weightheparin(enoxaparine):lessonslearnedfromdifferent dosageregimesintwocontinents.ActaAnaesthesiolScand. 1997;111:100---4.
20.LawtonMT,PorterRW,Heiserman JE. Surgicalmanagement ofspinal epiduralhematoma: relationship betweensurgical timingandneuro-logicaloutcome.JNeurosurg.1995;83:1---7. 21.Meikle J,Bird S, NightingaleJJ,etal. Detection and man-agement ofepidural haematomasrelated toanaesthesia in theUK:anationalsurveyofcurrentpractice.BrJAnaesth. 2008;101:400---4.
22.Tryba M. European practice guidelines: thromboembolism prophylaxis and regional anesthesia. Reg Anesth Pain Med. 1998;23:178---82.
23.Gogarten W, Van Aken H, Buttner J, et al. Neuraxial blockade and thromboembolism prophylaxis/antithrombotic therapy:revisedrecommendationsoftheGermanSocietyof AnaesthesiologyandIntensiveCare.AnasthesiolIntensivmed NotfallmedSchmerzth.2003;44:218---30.
24.HorlockerTT,WedelDJ,BenzonH,etal.Regionalanesthesia intheanticoagulatedpatient:definingtherisks(thesecond ASRAConsensusConferenceonNeuraxialAnesthesiaand Anti-coagulation).RegAnesthPainMed.2003;28:172---97. 25.LlauPitarchJV,DeAndresIbanezJ,GomarSanchoC.
Guide-linesofhemostasisinhibitingdrugsandneuraxialanaesthesia (Spanish).RevEspAnestesiolReanim.2005;52:413---20. 26.Vandermeulen E, Singelyn F, Vercauteren M, et al. Belgian
guidelinesconcerningcentralneuralblockadeinpatientswith drug-inducedalterationofcoagulation:anupdate.Acta Anaes-thesiolBelg.2005;56:139---46.
27.LlauJV,DeAJ,GomarC.Anticlottingdrugsandregional anaes-theticandanalgesictechniques:comparativeupdateofthe safetyrecommendations.EurJAnaesthesiol.2007;24:387---98. 28.Rosencher N, Bonnet MP, Sessler DI. Selected new antithrombotic agents and neuraxialanaesthesia for major orthopaedic surgery: management strategies. Anaesthesia. 2007;62:1154---60.
29.CronbergS,WallmarkE,SoderbergI.Effectonplatelet aggre-gationoforaladministrationof10non-steroidalanalgesicsto humans.ScandJHaematol.1984;33:155---9.
30.LeesePT,HubbardRC, KarimA,etal.Effects ofcelecoxib, a novel cyclooxygenase-2 inhibitor, on platelet function in healthyadults:arandomized,controlledtrial.JClin Pharma-col.2000;40:124---32.
31.SerebruanyVL,SteinhublSR,BergerPB,etal.Analysisofrisk ofbleedingcomplicationsafterdifferentdosesofaspirinin 192.036patientsenrolledin31randomizedcontrolledtrials. AmJCardiol.2005;95:1218---22.
32.Clasp(CollaborativeLow-doseAspirinStudyinPregnancy) Col-laborativeGroupClasp:arandomisedtrialoflow-doseaspirin forthepreventionandtreatmentofpre-eclampsiaamong9364 pregnantwomen.Lancet.1994;343:619---29.
33.Horlocker TT, Wedel DJ, SchroederDR, et al. Preoperative antiplatelet therapy does not increase the risk of spinal hematomaassociatedwithregionalanesthesia.AnesthAnalge. 1995;80:303---9.
34.Horlocker TT, Bajwa ZH, Ashraf Z, et al. Risk assessment of hemorrhagic complications associated with nonsteroidal antiinflammatory medications in ambulatory pain clinic patientsundergoingepiduralsteroidinjection.AnesthAnalge. 2002;95:1691---7.
35.Stafford-SmithM.Impaired haemostasisand regional anaes-thesia.CanJAnaesth.1996;43:129---41.
36.Hull R, Pineo G, MacIsaac S. Low-molecular-weight hep-arinprophylaxis:preoperativeversuspostoperativeinitiation in patients undergoing elective hip surgery. Thromb Res. 2000;101:155---62.
37.Patrono C, Baigent C, Hirsh J, et al. Antiplatelet drugs: AmericanCollegeofChestPhysiciansEvidence-BasedClinical PracticeGuidelines.8thed.Chest.2008;133:199---233. 38.BurgerW,ChemnitiusJM,KneisslGD,etal.Low-doseaspirin
forsecondarycardiovascularprevention:cardiovascularrisks afteritsperioperativewithdrawalversusbleedingriskswith its continuation: review and meta-analysis. J Intern Med. 2005;257:399---414.
39.Ferrari E,Benhamou M, CerboniP, MarcelB. Coronary syn-dromes followingaspirin withdrawal:a special riskfor late stentthrombosis.JAmCollCardiol.2005;45:456---9. 40.Collet J,Montalescot G, BlanchetB, et al. Impactofprior
useorrecentwithdrawaloforalantiplateletagentsonacute coronarysyndromes.Circulation.2004;110:2361---7.
41.HerrenT,StrickerH,HaeberliA,etal.Fibrinformationand degradationinpatientswitharterioscleroticdisease. Circula-tion.1994;90:2679---86.
42.Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and CareforNoncardiacSurgery:ExecutiveSummary.Circulation. 2007;116:1971---96.
43.Douketis JD, SpyropoulosAC,Spencer FA, et al. Periopera-tivemanagementof antithrombotictherapy andprevention of thrombosis. 9th ed. American College of Chest Physi-cians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:S326---50.
44.Vandermeulen E. Is anticoagulation and central neural blockade a safe combination? Curr Opin Anaesthesiol. 1999;12:539---43.
45.DenningerMH,NecciariJ,Serre-LacroixE,SissmannJ. Clopid-ogrelantiplateletactivityisindependentofageandpresence ofatherosclerosis.SeminThrombHemost.1999;25(S2):41---5. 46.Fox KA, Mehta SR, Peters R, et al. Benefits and risks of thecombinationofclopidogrelandaspirininpatients under-going surgical revascularization for non ST-elevation acute coronary syndrome: the clopidogrel in unstable angina to prevent recurrent ischemic events(Cure) trial.Circulation. 2004;110:1202---8.
47.Angiolillo DJ, Bhatt DL, Gurbel PA, et al. Advances in antiplatelet therapy:agents in clinicaldevelopment. AmJ Cardiol.2009;103:40---51.
48.WiviottSD,BraunwaldE,McCabeCH,etal.Prasugrelversus clopidogrelinpatientswithacutecoronarysyndromes.NEng JMed.2007;357:2001---15.
49.CollerBS.Anti-GPIIb/IIIadrugs:currentstrategiesandfuture directions.ThrombHaemost.2001;86:427---43.
50.Harrington RA, Armstrong PW, Graffagnino C,et al. Dose-finding, safety, and tolerability study of an oral platelet glycoprotein IIb/IIIa inhibitor, lotrafiban, in patients with coronary or cerebral atherosclerotic disease. Circulation. 2000;102:728---35.
14 N.M.Fonsecaetal.
tirofibaninpercutaneouscoronaryintervention.AmJCardiol. 2001;87:537---41.
52.GurbelPA,BlidenKP,ButlerK,etal.Randomizeddouble-blind assessmentoftheonsetandoffsetoftheantiplateleteffects ofticagrelorversusclopidogrelinpatientswithstablecoronary arterydisease.Circulation.2009;120:2577---85.
53.Schror K. The pharmacology of cilostazol. Diabetes Obes Metab.2002;4:S14---9.
54.Woo SK, Kang WK, Kwon KI.Pharmacokinetic and pharma-codynamic modeling of the antiplatelet and cardiovascular effectsofcilostazolinhealthyhumans.ClinPharmacolTherap. 2002;71:246---52.
55.SobelM,VerhaegheR.Antithrombotictherapyforperipheral arteryocclusivedisease:AmericanCollegeofChestPhysicians Evidence-Based Clinical PracticeGuidelines. 8th ed. Chest. 2008;133:S815---43.
56.KanedaT,UrimotoG,SuzukiT.Spinalepiduralhematoma fol-lowingepiduralcatheterremovalduringantiplatelettherapy withcilostazol.JAnesth.2008;22:290---3.
57.LlauJV,FerrandisR.Newanticoagulantsandregional anesthe-sia.CurrOpinAnaesthesiol.2009;22:661---6.
58.HirshJ,BauerKA,DonatiMB,etal.Parenteralanticoagulants: AmericanCollegeofChestPhysiciansEvidence-BasedClinical PracticeGuidelines.8thed.Chest.2008;133:141---59. 59.HirshJ,RaschkeR,WarkentinTE,etal.Heparin:mechanismof
action,pharmacokinetics,dosingconsiderations,monitoring, efficacy,andsafety.Chest.1995;108:S258---75.
60.Liu SS, Mulroy MF. Neuraxial anesthesia and analgesia in the presence of standard heparin. Reg Anesth Pain Med. 1998;23:157---63.
61.SandhuH,Morley-ForsterP,SpadaforaS.Epiduralhematoma followingepiduralanalgesiainapatientreceiving unfraction-ated heparinforthromboprophylaxis.RegAnesth PainMed. 2000;25:72---5.
62.PayLL,ChiuJW,ThomasE.Postoperativeepiduralhematoma orcerebrovascularaccident?Adilemmaindifferential diagno-sis.ActaAnaesthesiolScand.2002;46:217---20.
63.SchwarzSK, WongCL,McDonald WN.Spontaneous recovery fromaspinalepiduralhematomawithatypicalpresentation inanonagenarian.CanJAnaesth.2004;51:557---61.
64.King CS, Holley AB, Jackson JL, et al. Twice vs three timesdailyheparindosingforthromboembolismprophylaxis in the general medical population: a metaanalysis. Chest. 2007;131:507---16.
65.Rosen DA, Hawkinberry DW, Rosen KR, et al. An epidural hematoma in an adolescent patient after cardiac surgery. AnesthAnalg.2004;98:966---9.
66.DavignonKR,MaslowA,ChaudreyA,etal.Epiduralhematoma: whenisitsafetoheparinizeaftertheremovalofanepidural catheter?JCardiothorVascAnesth.2008;22:774---8.
67.Liu SS, Block BM, Wu CL. Effects of perioperative cen-tral neuraxial analgesia on outcome after coronary artery bypass surgery: a meta-analysis. Anesthesiology. 2004;101: 153---61.
68.RoedigerL,Larbuisson R,LamyM.Newapproachesand old controversiestopostoperativepaincontrolfollowingcardiac surgery.EurJAnaesthesiol.2006;23:539---50.
69.Ho AM, Chung DC, Joynt GM. Neuraxial blockade and hematoma in cardiac surgery: estimating the risk of a rare adverse event that has not (yet) occurred. Chest. 2000;117:551---5.
70.ChaneyMA.Intrathecalandepiduralanesthesiaandanalgesia forcardiacsurgery.AnesthAnalg.1997;84:1211---21.
71.GogartenW,VanAkenH,ButtnerJ,etal.Regionalanaesthesia and thromboembolism prophylaxis/anticoagulation. Revised recommendations of the German Society of Anaesthesi-ology and Intensive Care Medicine. Anaesth Intensivmed. 2007;48:S109---24.
72.Chaney MA. Cardiac surgery and intrathecal/epidural tech-niques:atthecrossroads?CanJAnaesth.2005;52:783---8. 73.Weitz JI. Low-molecular-weight heparins. N Eng J Med.
1997;337:688---98.
74.SanderinkG-JCM,GuimartCG,OzouxML,etal. Pharmacoki-netics and pharmacodynamics of the prophylactic dose of enoxaparinoncedailyover4daysinpatientswithrenal impair-ment.ThrombRes.2002;105:225---31.
75.Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced thrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin. N Eng J Med. 1995;332:1330---5.
76.Douketis JD, Kinnon K, Crowther MA. Anticoagulant effect atthetimeofepiduralcatheterremovalinpatients receiv-ing twice-daily or once-daily low-molecular-weight heparin and continuousepidural analgesiaafterorthopedic surgery. ThrombHaemost.2002;88:37---40.
77.BergqvistD,LindbladB,MatzschT.Lowmolecularweight hep-arinforthromboprophylaxisandepidural/spinalanaesthesia ---istherearisk?ActaAnaesthesiolScand.1992;36:605---9. 78.Bergqvist D, Lindblad B, Matzsch T. Risk of combining
low molecular weight heparin for thromboprophylaxis and epidural or spinal anesthesia.Seminars inThromb Hemost. 1993;19:147---51.
79.WysowskiDK,TalaricoL,BacsanyiJ,etal.Spinalandepidural hematomaand low-molecular-weightheparin.NEngJMed. 1998;338:1774---5.
80.XiM,BeguinS,HemkerHC. Therelativeimportanceofthe factors II, VII, IX and X for the prothrombinase activity in plasma of orally anticoagulated patients. Thromb Haemos. 1989;62:788---91.
81.EnnekingFK,BenzonH.Oralanticoagulantsandregional anes-thesia:aperspective.RegAnesthPainMed.1998;23:140---5. 82.AnsellJ,HirshJ,HylekE,etal.Pharmacologyand
manage-mentofthevitaminKantagonists:AmericanCollegeofChest PhysiciansEvidence-Based vClinicalPracticeGuidelines.8th ed.Chest.2008;133:S160---98.
83.Buvanendran A, Lubenow T, Majewski M, et al. The INR values at removal of epidural catheter in 4013 patients receiving warfarin. ASA Annual Meeting, Available at: http://www.asaabstracts.com/strands/asaabstracts/search Article.htm,2008.Acesso:dez.2012.
84.ParviziJ,ViscusiER,FrankHG,etal.Canepidural anesthe-siaand warfarin becoadministered? ClinOrthop RelatRes. 2007;456:133---7.
85.Sanofi-Synthelabo&OrganonNV.ClinicalInvestigatorBrochure Org31540/SR90107A.10aed.Apr.2001.
86.Kwong LM,Muntz JE. Thromboprophylaxis dosing: the rela-tionshipbetweentimingoffirstadministration,efficacy,and safety.AmJOrthop.2002;31:16---20.
87.SingelynFJ,VerheyenCCPM,PiovellaF,etal.Thesafetyand efficacyof extended thromboprophylaxiswithfondaparinux aftermajororthopedicsurgeryofthelowerlimbwithor with-out a neuraxial or deep peripheral nerve catheter. Anesth Analg.2007;105:1540---7.
88.Linkins L, Dans AL, Moores LK, et al. Treatment and pre-ventionofheparin-inducedthrombocytopeniaantithrombotic therapyand preventionof Ttrombosis.American Collegeof ChestPhysiciansEvidence-BasedClinicalPracticeGuidelines. 9thed.Chest.2012;141:495---530.
89.ErikssonBI,BorrisLC,FriedmanRJ,etal.Rivaroxabanversus enoxaparinfor thromboprophylaxisafterhiparthroplasty.N EngJMed.2008;358:2765---75.
SBARecommendationsforregionalanesthesiasafetyinpatientstakinganticoagulants 15
91.BayerXarelto.SummaryofProductCharacteristics.Available from: http://www.emea.europa.eu/humandocs/PDFs/EPAR/ xarelto/H-944-PI-en.pdf;2009.
92.KubitzaD,BeckaM,WensingG, et al.Safety, pharmacody-namics,andpharmacokineticsofBAY59-7939---Anoral,direct factorXainhibitoraftermultipledosinginhealthymale sub-jects.EurJClinPharmacol.2005;61:873---80.
93.Eikelboom JW, Weitz JI. New anticoagulants. Circulation. 2010;121:1523---32.
94.GarciaD,LibbyE,CrowtherMA.Theneworalanticoagulants. Blood.2010;115:15---20.
95.LassenMR,RaskobGE,GallusA,etal.Apixabanorenoxaparin forthromboprophylaxisafterkneereplacement.NEngJMed. 2009;361:594---604.
96.Lassen MR, Raskob GE, Gallus A, et al. Apixaban versus enoxaparinfor thromboprophylaxisafterkneereplacement: arandomizeddouble-blindtrial.Lancet.2010;375:807---15. 97.LassenMR,GallusA,RaskobGE,etal.Apixabanversus
enoxa-parinforthromboprophylaxisafterhipreplacement.NEngJ Med.2010;363:2487---98.
98.GrangerCB,AlexanderJH,McMurrayJJ,etal.Apixaban ver-suswarfarininpatientswithatrialfibrillation.NEngJMed. 2011;365:981---92.
99.Weitz JI, Eikelboom JW, Samama MM. New antithrombotic drugsantithrombotic therapyandpreventionofthrombosis. AmericanCollegeofChestPhysiciansEvidence-BasedClinical PracticeGuidelines9thed.Chest.2012;141:120---51.
100.Eriksson BI, Quinlan DJ, Weitz JI. Comparative pharmaco-dynamicsand pharmacokineticsoforaldirectthrombinand factor Xa inhibitors in development. Clin Pharmacokinet. 2009;48:1---22.
101.ErikssonB,DahlO,RosencherN,etal.Oraldabigatran Etexi-latevs.subcutaneousenoxaparinforthepreventionofvenous thromboembolismaftertotalkneereplacement:theremodel randomizedtrial.JThrombHaemost.2007;5:2178---85. 102.Boehringer-Ingelheim Pradaxa. Summary of Product
Char-acteristics. Available from: http://www.emea.europa.eu/ humandocs/PDFs/EPAR/pradaxa/H-829-PI-en.pdf,2009. 103.KaplanKL. Directthrombininhibitors.ExpertOpin
Pharma-cother.2003;4:653---66.
104.Kathiresan S, Shiomura J, Jang IK. Argatroban. J Thromb Thrombol.2002;13:41---7.
105.YehRW,JangI-K.Argatroban:update.AmHeartJ.2006;151: 1131---8.
106.GreinacherA.Lepirudin:abivalentdirectthrombininhibitor for anticoagulation therapy. Expert Rev Cardiovasc Ther. 2004;2:339---57.
107.Abramovitz S, Beilin Y. Thrombocytopenia, low molecular weightheparin,andobstetricanesthesia.AnesthesiolClinN Am.2003;21:99---109.
108.DouglasMJ.Coagulationabnormalitiesandobstetric anaesthe-sia.CanJAnaesth.1991;38:17---25.
109.Schindler M, Gatt S, Isert P, et al. Thrombocytopenia and plateletfunctionaldefectsinpre-eclampsia:implicationsfor regionalanaesthesia.AnaesthIntensCare.1990;18:169---74. 110.VanVeenJJ,NokesTJ,MakrisM.Theriskofspinalhaematoma
followingneuraxialanaesthesiaorlumbarpuncturein throm-bocytopenicindividuals.BrJHaematol.2010;148:15---25. 111.AvelineC,BonnetF.Delayedretroperitonealhaematomaafter
failedlumbarplexusblock.BrJAnaesthesia.2004;93:589---91. 112.MaierC,GleimM,WeissT,etal.Severebleedingfollowing lum-barsympatheticblockadeintwo patientsundermedication withirreversibleplateletaggregationinhibitors. Anesthesiol-ogy.2002;97:740---3.
113.WellerRS,GerancherJC,CrewsJC,etal.Extensive retroperi-tonealhematomawithoutneurologicdeficitintwopatients whounderwentlumbarplexusblockandwerelater anticoag-ulated.Anesthesiology.2003;98:581---5.
114.ButtnerJ,BurkleH,GogartenW,etal.Thromboembolism pro-phylaxisandperipheralnerveblocksforregionalanaesthesia. GuidelineoftheGermanSocietyofAnaesthesiologyand Inten-siveCareMedicine.AnaesthIntensivMed.2005;46:319---22. 115.Kozek-LangeneckerSA,FriesD,GuM,etal.Locoregional
anes-thesia and coagulation inhibitors. Recommendations of the TaskForceonPerioperativeCoagulationoftheAustrianSociety forAnesthesiologyandIntensiveCareMedicine.Anaesthesist. 2005;54:476---84.