REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Correlation
between
weekly
working
time
and
burnout
syndrome
among
anesthesiologists
of
Maceió-AL
夽
Fabiano
Timbó
Barbosa
∗,
Raissa
Jardelino
Eloi,
Luciano
Menezes
dos
Santos,
Bruna
Acioly
Leão,
Fernando
José
Camelo
de
Lima,
Célio
Fernando
de
Sousa-Rodrigues
UniversidadeFederaldeAlagoas(Ufal),Maceió,AL,Brazil
Received5June2014;accepted22June2015 Availableonline18January2017
KEYWORDS Burnout; Professional; Workload;
Intensivecareunits; Cross-sectional studies; Diagnosis
Abstract
Backgroundandobjective: Thecurrentjobsareinsufficienttodeterminethecausativeagent, aswellastoidentifycharacteristichighriskprofilesforBS,leavingaclearneedformorestudies tothisend.Thisstudyobjectivewastoevaluatethecorrelationbetweenweeklyworkloadand BSdimensions.
Methods:Anobservational,descriptive,cross-sectionalstudyperformedwith43 anesthesiolo-gistsfromMaceió-AL,withtheapplicationofMaslachBurnoutInventory(MBI)forms.Pearson’s correlationcoefficientrwasusedforthethreedimensionsanda95%confidenceintervalfor theprevalenceofburnoutsyndromeandhighscoresinallthreedimensions.
Results:Among the studied physicians, 51.16% were male and the average age was 49.82±12.05 years.For physicianswho havebeendiagnosedwith BS throughthe MBI,the averageweeklyworkingtime69.27±22.39h.Thehighleveloffrequencyinatleastoneof thethreedimensionswasfoundin67.44%ofphysicians,withthispercentagebeingconsidered diagnosticforburnoutsyndromeinthispopulation.
Conclusion: Thisstudy showednocorrelationbetween theweeklyworkingtimeandtheBS dimensionsinthispopulation.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE Burnout;
Profissional; Cargadetrabalho; Unidadesdecuidados intensivos;
Correlac¸ãoentreacargahoráriasemanaldetrabalhocomasíndromedeburnout
entreosmédicosanestesiologistasdeMaceió-AL
Resumo
Justificativaeobjetivo: Ostrabalhosatuaissãoinsuficientesparadeterminaroagentecausal, assim como identificarperfis característicos dealto riscoparasíndrome deburnout(SB),e
夽 Institution:UniversidadeFederaldeAlagoas,Maceió,AL,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.T.Barbosa). http://dx.doi.org/10.1016/j.bjane.2015.06.001
Estudostransversais; Diagnóstico
deixamevidenteanecessidadedemaispesquisascomesseobjetivo.Opresenteestudoteve comoobjetivoavaliaracorrelac¸ãoentreacargasemanaldetrabalhocomasdimensõesdaSB. Métodos: Estudoobservacionaldescritivoetransversalfeitocom43médicosanestesiologistas deMaceió-AL,pormeiodaaplicac¸ãodeformulárioscomoMaslachBurnoutInventory(MBI).Foi usadootestedecorrelac¸ãoRdePearsonparaastrêsdimensõeseumintervalodeconfianc¸a de95%paraaprevalênciadasíndromedeburnouteparaescoresaltosnastrêsdimensões. Resultados: Entreosmédicosestudados,51,16%pertenciamaogêneromasculinocommédiade 49,82±12,05anos.ParaosmédicosquepormeiodoMBIforamdiagnosticadoscomSB,amédia decargahoráriasemanaldetrabalhofoide69,27±22,39horas.Afrequênciadealtonívelem pelomenos umadastrêsdimensões foiencontradaem67,44%dosmédicos,foiconsiderada essaaporcentagemdediagnósticoparaasíndromedeburnoutnapopulac¸ãoestudada. Conclusão:Opresenteestudodemonstranãohavercorrelac¸ãoentreacargahoráriasemanal detrabalhocomasdimensõesdaSBnapopulac¸ãoestudada.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Burnout syndrome (BS) is closely related to work and it hasbecomeincreasinglypresentinthemedicalroutine,as doctorsareconstantlysubjectedtohighworkloads, accumu-lationoffunctions,poorwages,stressfulworkenvironment, multiple jobs, among other factors.1 Despite occupying a
goodtimeof the daily routine,the workdoes not neces-sarilybringprofessionalsatisfaction.2Itwasinthiscontext
that Freudenberger formulated the staff burnout expres-sion,characterized by physical exhaustioncombined with psychosocialbehavioralchanges.3
Characterized by emotional exhaustion, depersonaliza-tion, and reduced personal accomplishment, BS becomes typical for the health areas that involve human relation-ships, productivity, professional recognition, and energy expenditurethatmaygenerateprofessionalfailure.4
Emo-tionalexhaustionismarkedbyemotionalexhaustion.Thus, professionalscometobelievethattheynolongerhavethe energytodealwithpatients.Regardingdepersonalization,it makeshealthprofessionalsinsensitive,whichleadsthemto treatpatientsandcolleaguesasobjectswithoutvalue.The reductionof professionalachievement,in itsturn,reveals employee dissatisfaction with their performance at work leadingthem tobelievethattheir functionsarenolonger carriedoutduetolackofenergy.5
The impact of professional exhaustion and its conse-quences on physician’s health has aroused national and internationalscientificinterest.In2007,inthestudyAsaúde domédico noBrasil(Thephysician’shealth inBrazil),the FederalCouncilofMedicineidentified,amongotherthings, thatofthe 2364physiciansparticipating inthe work,57% hadsomeworryingdegreeofBS,frommoderatetosevere. InastudyconductedamongBrazilianoncologists, a52.3% prevalence of the syndrome was identified.6 Similarly, in
a study performed in the United States (US), in order to comparetheprevalenceofBSamongphysiciansandtheUS generalpopulation,itwasidentifiedaprevalenceof37.9% and23.5%,respectively.7
Regarding the anesthesiology field, the occupational health ofthismedicalspecialtyhasattractedmore atten-tion.In2011,DuvalNetoetal.drewattentiontotheneed for greater care and concern for the occupational health of Brazilian anesthesiologists, by the doctors themselves, the Stateandthe governmentalorganizations.8 According
tothearticle,inrecentdecades,innovationsand increas-ing changes in the daily activities of the specialty, with changesin thetechnological frameworkandgreater chal-lengeatwork,inadditiontotheincreasinglycomplexcases, caused a strong impactontheoccupational well-being of anesthesiologists.
The current reports are insufficient to determine the causalagent,aswellastoidentifythecharacteristichigh riskprofilesforBS,makingcleartheneedformoreresearch for thispurpose.9,10 The aimofthisstudy wastoevaluate
the correlation between the weekly workload and the BS dimensions.
Material
and
methods
This wasadescriptivecross-sectional observationalstudy, in which data were collected among anesthesiologists of Maceió-AL,fromMarchtillMay2014,inpublicandprivate hospitals.Beforedatacollection, thestudywassubmitted tothePlataformaBrasilforproperapprovalandtheEthics andResearchCommitteeoftheFederalUniversityofAlagoas (Ufal)authorization.
Forselection of physicians, we reviewed a list of 150 anesthesiologists,which was providedby the Anesthesiol-ogySocietyoftheStateofAlagoas(Saeal).Weconducteda drawof43doctors,whoweregiventhesurveyformswith theMaslachBurnoutInventory(MBI).
tothe participant, leavinghim freeto participateor not in the research.This agreement wasmade in accordance withtheUfalEthicsandResearchCommitteemodelandalso in accordancewiththe Resolution 466/12 of theNational HealthCouncil(CNS).
Theinvestigatorscontacteddoctorsinthreepublic hos-pitals and two private hospitals in Maceió-AL. In every visitmadeintheoperatingroomtheinvestigatorsexposed the research and its objectives and showed the need to detect thepresenceof thesyndromeinthe fieldof these professionals.Doctorsansweredtheinventorywithout inter-ferencefrominvestigators.
The inclusioncriteriaweredoctorstrainedin medicine andwithanesthesiologyspecialization,withregular employ-ment and registration in the Alagoas Regional Medical Council (Cremal). The exclusioncriteria were incomplete MBI questionnaires and failure to fill the weekly working hours.
We used the MBI, prepared by Christina Maslach and Susan Jackson, which is a questionnaire formed by three dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment, consisting of 22 ques-tions withfiveoptions for each question (scale from1 to 5).11TheBSindicesareidentifiedfromthevaluesobtained
ineachevaluateddimension.Regardingemotional exhaus-tion,itshighleveldetectionisidentifiedwithascorehigher thanorequalto27,whereasthemoderatelevelisdetected withvaluesbetween19and26,andvaluesbelow19detects a low level of emotional exhaustion.11 For
depersonaliza-tion,thehighlevelisdetectedwithvaluesgreaterthanor equalto10,whereasvaluesbetweensixandninedetecta moderatelevel andsmaller thansixdetect alow levelof depersonalization.11 Converselytootherdimensions
evalu-ated,personal accomplishmentisdetected withasmaller numberofpoints.11 Valuesbetween0and33indicatehigh
level, while valuesbetween 34 and39 indicatemoderate level andvalues greaterthan or equal to40 indicatelow level.11 BS diagnosis was made according tothe Grunfeld
etal.model,whichrequiresthepresenceofonlyone high-levelscore.12
As for the form,itinitially requestedgeneral informa-tion,suchasname(optional),completiondate,gender,and dateofbirth.Inasecondgroup,questionswereaskedabout workandlifehabits,suchasmaritalstatus,havingchildren, havingspecialist title, totalworking time(years)in anes-thesiology,typeofworkingestablishment,weeklyworking hoursonduty,amongothers.Inthethirdgroup,questions wereaskedaboutthephysicianhealthstatus,inwhichallhis healthstatuswasoutlined,specifyingdisordersthathemay have,andfinally,inthefourthgroup,itwasaskedquestions regardingstressintheworkplace.
The primary variables were frequency of BS in anes-thesiologists and the average weekly working hours on duty of respondents. As secondary variables, we high-lightedthetypeofmedicalspecialty,professionalworking timeandgraduation,typeofworkingestablishment,work shifts, number of night shifts, uninterrupted duty time, recreation, number of cigarettes smoked per day and number of days consuming alcohol per week, presence of any chronic disease and which one, symptoms, signs and disorders associated with BS, behavioral and psy-chological symptoms, as well as work factors that are
considered by the participants as stressful or harmful to health.
Symptoms,signs,anddisordersassociatedwithBSwere characterized by progressive and constant fatigue, sleep disorders (sleep apnea, excessive sleepiness, insomnia, and snoring), muscle or musculoskeletal pain, headache, migraine, immunodeficiency, cardiovascular diseases, res-piratorysystemdisorders,sexualdysfunction(impotenceor lossoflibido),ornoneoftheaboveoptions.
The psychological and behavioral symptoms proposed were:lackofattentionandconcentration,memory impair-ment, slower thinking, feeling of alienation, feelings of loneliness, impatience, feeling of inadequacy, increased aggressiveness, inability to relax, difficulty in accepting changes,lossofinitiative,increasedconsumptionofdrugs, tendencytoisolation, feelingsofomnipotence, emotional instability,lossofinterestinworkorpleasure,difficultyin self-acceptance,absenteeism,asthenia,depression,irony, cynicism,distrust,irritability,ornoneoftheaboveoptions. Some factors that may existin the workplace and are stressfulandharmful tothe physician’s health have been proposed,such asexcessive noise in the operatingroom, possibility of complications, relationship with the team duringcare ofpatients, managementof high-risk patient, administrative problems, pressure to discharge patients, dealingwithsufferinganddeath,difficultysleepingatnight shifts,obligationtodealwithseveralissuessimultaneously, workintheoperatingand/or emergencyroom,numberof patients per doctor, rapid pace of professional activities, lackofmaterialresources,andnoneoftheaboveoptions.
For sample size calculation, we used the electronic calculatoravailableathttp://www.lee.dante.br/pesquisa/ amostragem/amostra.html.It was needed 43 anesthesiol-ogists, witha correlation between the scores of MBI and weeklyworkloadof0.3;asignificancelevelof5%and80% test power. A 95% confidence interval was used for both BSprevalenceandhighscoresinthethreedimensions.For thenumberofchildren,weusedmedianandinterquartile range.Pearson’scorrelationinRwasusedforthethreeaxes.
Results
Forty-three anesthesiologistsworking in night shifts were included. To achieve this number, three draws using the names present in the Saeal list were needed, as 15 ran-domlyselectedphysicianswereinasituationofexclusion, aswellasnotexercisingtheactivityorhadrefusedto par-ticipate.ThecompletedformswereevaluatedforMBIand othervariables.TheprevalenceofBSinthestudypopulation was67.44%(29/43,53.43---81.45%).
Of the physicians participating in the study, 51.16% (22/43) were male, mean age of 49.82±12.05 years. Regarding marital status, 69.77% (30/43) declared them-selves as married, 16.28% (7/43) as singles, and 13.95% (6/43)asdivorcedorwidowed.Amongthestudied anesthe-siologists,76.74% (33/43)have children, withmedianand interquartilerangeof2(1---3).
workplace,93.04%(40/43)workinbothpublicandprivate institutions,2.32% (1/43) reportedworking only in public institutions,2.32% (1/43) only inprivate institutions,and 2.32%(1/43)declinedtoanswerthisquestion.
The physician’s average weekly working hours onduty inanesthesiologywas63.64±22.39h.Forphysicians diag-nosedwithBSthroughtheMBI,withthediagnosticcriteria asexplainedinthemethodology,theaverageweekly work-inghourswas69.27±22.39h.Forthosewhodidnotreceive a positive diagnosis, the average weekly duty time was 51.08±18.74h. For all participants, the average of the longestweeklydutytimewas27.09±17.18h,whereasfor those diagnosed with BS it was 30.69±16.28h, and for thosewhodidnotreceivethisdiagnosisitwas,onaverage, 19.08±17h.
Life habits, including the harmful ones, were also addressed, such as leisure time, physical activity, smok-ing and alcohol consumption. The average leisure time per week was 28.71±16.32h. Regarding physical activ-ity, 60.47% (26/43) reported engaging in regular physical activity, with bodybuilding and walking being the most citedactivities. The BS prevalence amongthose engaged inphysicalactivitywas61.54%(16/26)and76.47%(13/17) among those not engaged in such activity. None of the assessed physicians reported being a smoker and 72.09% (31/43)reportedalcoholconsumption.Despitethedifficulty inestimating the amount of weekly alcohol consumption, 54.84%(17/31)consumeonetothreeglasses (200mL)per week,22.58%(7/31)lessthanoneglass,and22.58%(7/31) more than three glasses of alcohol per week. Regard-ing the type of alcohol consumed, the most frequently reported were beer, wine, whiskey, sparkling wine and vodka.
Regarding general health conditions, 62.79% (27/43) reportedhavingsomediagnosedchronicdisease,themost frequentlyreportedwerehypertension,sleepdisorders,and allergies.Regardingthepresenceofsignsandsymptomsthat couldbe possible consequences of BS, the most reported were muscle or musculoskeletal pain by 46.51% (20/43), sleep disorders by 41.86% (18/43), headache by 23.25% (10/43),andsteadyandprogressivefatigueby20.93%(9/43) ofphysicians.Only13.95%(6/43)reportednothavinganyof thequestionedsignsandsymptoms.
In the population studied, between the psychologi-cal and behavioral symptoms related to BS, the standing out ones were impatience reported by 55.81% (24/43) and irritability reported by 48.84% (21/43) of physicians. Among other symptoms, the most common were lack of attention and concentration in 27.91% (12/43), memory impairment in 27.91% (12/43), discouragement in 25.58% (11/43), emotional instability in 23.25% (10/43), inability torelax in 20.93% (9/43), in addition to slower thinking, asthenia, and increased aggression, which were reported by 16.28% (7/43). Only 11.63% (5/43) of the physicians reportedhavingnoneofthepsychological symptoms men-tioned.
When asked about the work environment, the study physicianspointedoutmanyfactorsthatarestressfuland harmful to health and contribute to the development of SB. Only 6.98% (3/43) said not being affected by these factors.Themainelementshighlightedwerelackof mate-rial resources by 67.44% (29/43) and the possibility of
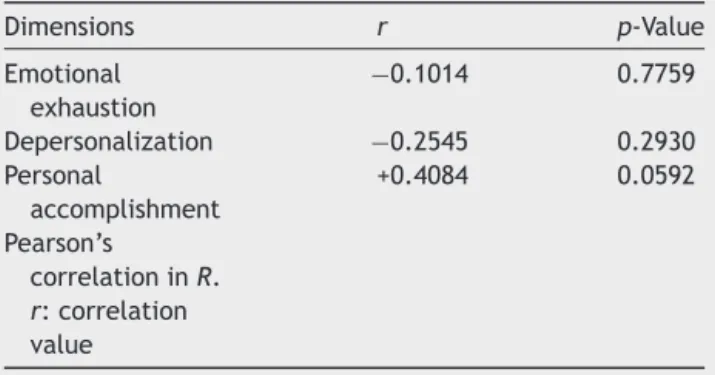
Table 1 Correlation between weekly workinghours and
eachofthethreeburnoutsyndromedimensions.
Dimensions r p-Value
Emotional exhaustion
−0.1014 0.7759
Depersonalization −0.2545 0.2930 Personal
accomplishment
+0.4084 0.0592
Pearson’s
correlationinR. r:correlation value
complications in the management of their patients by 53.49%(23/43).Thepresenceofbothexcessivenoiseinthe workplaceand the occurrenceof administrativeproblems werementionedby46.51%(20/43),troublesleepinginnight shifts were reported by 41.86% (18/43), and the number of patientsper doctorby 34.88%(15/43). Other elements alsoconsideredstressfulandpossiblyinterferingwithhealth appeared less frequently, suchasfast-pace work environ-ment, requirement to handle multiple concurrent issues, andstafflowcommitment,whichwerereportedby27.91% (12/43).
Still regarding the work environment, 23.25% (10/43) reportedfeelinguncomfortablewiththeestablishment fre-quentchangesofrulesandregulations,20.93%(9/43)feel prevented fromactingaccordingtotheir principlesin the workplace, 18.6% (8/43) feel they have communication problems withtheorganizers,and16.28%(7/43)feelthat productionishamperedbythelowqualityofthework atmo-sphere.
In the MBI assessment, the high frequency level in at least one of the threedimensions (emotional exhaustion, depersonalization,andpersonalaccomplishment)wasfound in67.44%(29/43,53.43%to81.45%).Thus,thispercentage wasconsidereddiagnosticforBSinthepopulationstudied. The frequency of high levelscores onthe threeaxeswas only found in 9.3% (4/43, 0.62%to 17.98%).In evaluating each dimension separately, we found high level of emo-tionalexhaustionin25.58%(11/43,12.54%to38.62%),high levelofpersonalaccomplishmentin51.16%(22/43;36.22% to66.10%)anddepersonalizationin44.19%(19/43;29.35% to59.03%).
Pearson’scorrelationcoefficientRwasusedtocorrelate the three dimensions of BS with the weekly workload. Only the data from physicians diagnosed with IBS were usedforthetest.Noneofthethreedimensionscorrelated significantlywiththeweeklyworkinghours(Table1).
Discussion
dimensionsofBSareemotionalexhaustion, depersonaliza-tionandreducedpersonalaccomplishment.13 Occupational
demands can depletethe individual,leading him to emo-tional exhaustion.13 Despite being the most studied and
evaluateddimension,it shouldnotbeviewedalone, asit failstocapturethecriticalaspectsoftherelationshipwith work.13Depersonalizationisanattempttodetachfromlabor
activities,inwhichthequalityofinterpersonalrelationship is lost.13 Withthe feelingof inefficiencyand indifference
at work, the individual begins to develop a low personal accomplishment.13Thethreedimensionsmaybedeveloped
sequentiallyorinparallel.13
AccordingtoMurofuseetal.,theBSonsetistriggeredby progressivelevelsofstress,whichcanbediagnosedbasedon perspectives: clinical, socio-psychological, organizational, and socio-historical.4 Freudenberger proposed theclinical
perspective,statingthatemotionalexhaustionleadstothe denialofone’sownneeds.3MaslachandJacksonproposed
that chronic emotional stress related tocaring for others wouldberesponsibleforprofessionalburnoutandBSwould bethesocio-psychologicalapproach.11 Intheorganization,
astressfulandfrustratingor monotonousworkleadstoBS andcausesimpossibilityofcarryingoutthework.4Finally,
inthesocio-historicalperspective,socialconditionswould beresponsibleforthelossofinterpersonalrelationships.14
Although BS is notinherent to anesthesiology or other specialties,thereisagreater susceptibilityofhealth pro-fessionals,asthearduoussearchforknowledge,combined withthehealthsystemfailures,requirestheadaptationof theprofessional.15Inamorecurrentpicture,thistrendwas
demonstratedinan Americanstudy thatcomparing physi-cianswiththegeneralpopulationfoundanincreasedriskin themedicalpopulationfordevelopingemotionalexhaustion anddepersonalization.7
Complaintsrelatedtoexcessivededicationtoworkand lack oftimewithfamilyhavebeen increasingly more fre-quentamongphysicians.16Thus,thetimededicatedtowork
hasbeen identifiedasan importantstressorbythese pro-fessionals and, therefore, an important risk factor to be investigated.It was preciselythis factor that the current studyaimedtoinvestigate.Weinvestigateanycorrelation betweentheweeklyworkinghoursofMaceió anesthesiolo-gistsandBSdimensions.However,nosignificantcorrelation wasfound in the studied sample, a result similarto that foundinastudywithotherdoctorsofMaceió,17but
differ-entfromthatofShanafeltetal.inwhichtheweeklyworking hourswereassociatedwiththeriskofdevelopingBSinUS physicians.7
For BS measurement, the Maslach questionnaire (MBI) wasused,chosenforbeingthemostusedforthispurpose and having the strongest psychometric properties,13,18 in
additiontoenabling thedescriptionandevaluationof the threedimensionsseparately.
AllstudiedphysicianscompletedtheMBIproperly. How-ever,thepresentstudyhassomelimitations,whichshould beaddressedinfuturework.Themainlimitationswerethe physician’sapproachathisworkplace,whichmeantthatthe questionnaire wasanswered quickly;the factthat not all MaceióanesthesiologistsareregisteredinSaeal,whichdid notgivethesamechancetootherdoctorsofMaceióand pre-cludedthepossibilityofotherSBdiagnostics;thestudywas restrictedtoMaceió,makingit impossibletoevaluatethe
conditionsoftheothermunicipalitiesofAlagoasregarding theprevalenceofBS.
Althoughthereisnostandardizationforaproperformof BSdiagnosis withtheuseofMBI,inthisstudyitwas diag-nosedaccordingtoGrunfeldetal.thatdefineprofessional burnout in the presence of at least one high level,12 and
thus itis a verysensitive method, but littlespecific. The frequencyBSfoundinthesamplewas67.44%,slightlybelow thatfoundforthegroupofintensivists,whichwas70.14%,17
butabovethatfoundinasampleofoncologists,whichwas 52.3%.6 Abroader comparisonis hampered bythe lack of
standardizationindiagnosis.IfthecriterionofRamirezetal. wasfollowed, whichdefinesburnout asthepresence ofa highlevelscoreinthreedimensions,19 onlyfouroutof19
ofthe43physicianswould bediagnosed withBS.The low prevalenceofBSwhenthelattercriterionisusedisfound intheliterature.6,20Thislastdiagnosticformhasthe
disad-vantageofbeingmorespecificandlesssensitive,andmay failtodiagnosepositivecasesforSB.
In the population studied, the dimension that had the highest frequency of high scorewas personal accomplish-ment, indicating reduced personal accomplishment in 22 ofthephysicians,followedbydepersonalizationin19,and emotionalexhaustionwastheleastfrequent,presentinonly 11.Thereducedpersonalaccomplishmentasthemost fre-quentdimensioninthestudypopulationisparalleltothat foundin asimilarstudyperformed inMaceio,17 but
oppo-sitetothatfound by Tucunduva etal.,whoreportedthis dimensionastheleastfrequent.6Reducedpersonal
accom-plishment is considered by Maslach asthe last one tobe developed,being influencedby emotional exhaustionand depersonalizationintheindividualwithBS.13
The inventoryusedasatoolin thestudy wasnotonly theMBI,butmanyotherdataandvariablesthatallowedus abetterunderstanding ofthe personallifeandwork con-ditionsof each physician.However,unlikethe MBI,which wascompletelyfilledbyallparticipants,whichallowedthe inclusioninthework,notallphysiciansrespondedtoother datawiththesamecareandattention,whichhamperedits standardizationandinterpretation ina fewpoints.This is probablyduetothephysicians’approachintheirworkplace. The anesthesiologists’ profile consisted of an adult populationwithmeanageof 49.82yearsandaslight pre-dominance of male. Of the 29 physicianswith BS, 16 are men.Thisgreaterprevalencecounteractstheonefoundin theliterature,inwhichfemaleisregardedasmore suscep-tibletoBS.6Ofthephysicianssurveyed,69.77%and76.74%
aremarried,havechildrenand,althoughthereisnogeneral agreementontheimpactofmaritalstatusinthe develop-mentofBS,21amajorstudyfoundcorrelationbetweenlack
offamilysupportonadailybasisandhigherincidenceofBS.6
Therefore,a stablefamily life is an important protective factor.
beenreportedasapresentrealityinthedailylivesofsome ofthestudiedphysicians.
Regardingthetitleofspecialistinanesthesiology,97.68% respondedaffirmatively,ahigherproportionthanthatfound inasimilarstudy.22Appropriatemedicalspecialization,
fol-lowedbyconstantupdateallowstheprofessionaltobesure ofhislabor activities.Insecurity wasreportedbyMaslach etal.,alongwithworkoverload,asafactorrelatedtothe developmentof BS.13 However, despitethe safer practice
regardingspecialization,thepracticeofnightshiftsinthe activityleavestheanesthesiologistinvulnerablecondition, asshift work is considered a factor relatedto the devel-opmentoftheBS,withindividualswhoalternatenightand daytimeactivities withchangesinperiodsof twotothree daysbeingthemostsusceptible.23Troublesleepingonnight
shiftswasmentionedasastressfactorby41.86%ofthestudy physicians.
Among thestudysample, 60.47% havehealthylifestyle habitsrelatedtoregularphysicalactivity,prevalencehigher than that found in the study with anesthesiologists from theABCSchoolofMedicine.24Thesamestudyrevealedthat
physicalactivityallowsbetteradaptation,causesa reduc-tioninthedegreeofdepersonalization,24 strengthenedthe
present study results, in which ahigher prevalence of BS occurred among doctors who do not exercise. Regarding alcohol consumption, despite being a habit confirmed by 72.09%ofthedoctors,itwasnotpossibletodetermineitas anexcessiveandharmfulhabittohealthorwithreflection ofastressfulworkactivity.
ExhaustioninducedbyBScancausemanydamagestothe physicalandmentalhealthoftheindividual.21Amongthose
alreadyreportedin theliterature,21 themost frequent in
thestudyphysiciansweremuscleandmusculoskeletalpain, sleepdisorders,headache,andfatigue.Asfor the psycho-logical and behavioral symptoms related to BS, the most reportedwereimpatienceandirritability,aswellaslackof attentionandconcentration,memorychanges,depression, emotional instability, inability to relax, slower thinking, asthenia,andincreasedaggressiveness.
Although it was not found any significant correlation between the weekly working hoursand BS in the studied sample, it does not mean that a heavy workload is not harmful.Excessivededicationtoworkandlackoftimewith thefamily,16which,togetherwithotherworkingconditions,
constituteanunwholesomeenvironmentforhealth. The implications for futureresearch are: avoiding the approach of volunteers in their workplace; the need to assesscorrelationwithothervariables,suchasnoiselevels, level of satisfaction, coexisting diseases. For sample size calculationusingthepresent studyparameters(95% confi-denceinterval,5%˛,and20%ˇ),143participants willbe requiredandadiagnosticcriterionwiththepresenceofat leastonedimensionwithhighscore(prevalenceof70%for BS)or61participantsifusingadiagnosticcriterionrequiring thepresenceofhighscoresforthethreedimensionsofBS (prevalenceof10%forBS).
Conclusion
Thestudyresultsshownocorrelationbetweentheweekly workinghoursandBSdimensionsinthepopulationstudied.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BarbosaGA,AndradeEO,CarneiroMB,etal.Asaúdedos médi-cosnoBrasil.ConselhoFederaldeMedicina.2007.
2.DejoursC.Aloucuradotrabalho.Oboré.1992.
3.Freudenberger H. Staff burnout. J Soc Issues. 1974;30: 159---65.
4.Murofuse NT, Abranches SS, Napoleão AA. Reflexões sobre estresseeburnoutearelac¸ãocomaenfermagem.RevLatAm Enferm.2005;13:255---61.
5.RosaC,CarlottoMS.Síndromedeburnoutesatisfac¸ãono tra-balhoemprofissionaisdeumainstituic¸ãohospitalar.RevSBPH. 2005;8:1---15.
6.TucunduvaLTCM,GarciaAP,PrudenteFVB,etal.Asíndromeda estafaprofissionalemmédicoscancerologistasbrasileiros.Rev AssocMedBras.2006;52:108---12.
7.Shanafelt TD, Boone S, Tan L, et al. Burnout and satis-faction withwork-life balance among us physicians relative to the general us population. Arch Intern Med. 2012;172: 1377---85.
8.DuvalNetoGF,BonetF,HowardS,etal.Professional wellbe-ingworkpartydaWFSA:éhoraderefletireagiremrelac¸ão àsaúdeocupacionaldoanestesiologista.RevBrasAnestesiol. 2011;61:393---6.
9.LimaFD,BuunkAP,AraújoMBJ,etal.Síndromedeburnoutem residentesdaUniversidadeFederaldeUberlândia---2004.Rev BrasEducMéd.2007;31:137---46.
10.ThomasNK.Residentburnout.JAMA.2004;292:2880---9. 11.MaslachC,JacksonSE,LeiterMP.Maslachburnoutinventory,
manual.PaloAlto:UniversityofCalifornia.Consulting Psychol-ogists;1999.
12.Grunfeld E, Whelan TJ, Zitzelsberger L, et al. Cancer care workersinOntario:prevalenceofburnout,jobstress,andjob satisfaction.CMAJ.2000;163:166---9.
13.MaslachC,ShaufeliWB,LeiterMP.Jobburnout.AnnuRev Psy-chol.2001;52:397---422.
14.ChernissC.Staffburnout:jobstressinthehumanservices.Sage Publications;1980.
15.DelgadoAC,FuentesJMB,QuevedoMPA,etal.Revisiónteórica delburnoutodesgasteprofesionalentrabajadoresdela docen-cia.Caesura.1993;2:47---65.
16.Bogue RJ, Guarneri JG, Reed M, et al. Secrets of physi-ciansatisfaction.Studyidentifiespressurepointsand reveals lifepracticesofhighlysatisfied doctors.PhysExec.2006;32: 30---9.
17.BarbosaFT,LeãoBA,TavaresGM,etal.Burnoutsyndromeand weekly workloadof on-callphysicians:cross-sectional study. SãoPauloMed.2012;130:282---8.
18.Tamayo MR, Tróccoli BT. Construc¸ão e validac¸ão fatorial da EscaladeCaracterizac¸ãodoBurnout(ECB).Estudosde Psicolo-gia.2009;14:213---21.
19.Ramirez AJ, Graham J, Richards MA, et al. Burnout and psychiatric disorder among cancer clinicians. Br J Cancer. 1995;71:1263---9.
20.MoreiraDS,MagnanoRF, SakaeTM,etal.Prevalênciada sín-drome de burnout em trabalhadores de enfermagem de um hospitalde grandeportedaRegião SuldoBrasil. CadSaúde Pública.2009:25.
22.CalumbiRA,AmorimJA,MacielCMC,etal.Avaliac¸ãoda quali-dadedevidadosanestesiologistasdacidadedoRecife.RevBras Anestesiol.2010:60.
23.PeiróJ.Desencadeantesdoestréslaboral.Pirâmide.1999.