USEFULNESS OF ADDITIONAL NERVE CONDUCTION
TECHNIQUES IN M ILD CARPAL TUNNEL SYNDROM E
João Aris Kouyoumdjian
1, M aria P. A. M orit a
2, Amalia F. P. M olina
3ABSTRACT - This st udy w as done t o assess t he percent age of abnormalit y in addit ional nerve conduct ion t echniques aft er normal median dist al lat ency (rout ine) in mild carpal t unnel syndrome (CTS). Bilat eral nerve conduct ion st udies w ere carried out in 116 consecut ive sympt omat ic CTS pat ient s (153 hands). M ild cases w ere based on normal rout ine (< 3.7 ms, peak-measured, 14 cm) and at least one t echnique abnormal of t he follow ing: sensory radial difference (M R); sensory ulnar difference (M U4); mixed palm medianulnar difference (M UP); median palm lat ency (PW); and mot or median dist al lat ency (M DL). Aft er normal cut -off values for rout ine, 3.1 t o 3.6 ms (< 3.7 ms), w e found an abnormal M R, ranging from 86.6 t o 93.4%, follow ed by M U4 (40 t o 81.7%), M UP (20 t o 71.2%), PW (0 t o 41.1%), and M DL (0 t o 19.6%). The most frequent abnormal associat ion w ere M R plus M U4 in 90.1%, follow ed by M R plus M UP and M U4 plus M UP. The most frequent abnormal addit ional nerve conduct ion t echnique for mild CTS elect rodiagnosis w as M R, follow ed by M U4 and M UP. Percent age of M R abnormalit y w as very high regardless of t he median rout ine lat ency cut -off (< 3.1 t o < 3.6 ms).
KEY WORDS: carpal tunnel syndrome, median nerve, entrapment neuropathy, electrodiagnosis, nerve conduction.
Utilidade de técnicas adicionais de condução nervosa para o dignóstico de síndrome do túnel do carpo leve
RESUM O - Est e est udo foi realizado para avaliação da percent agem de anormalidade de t écnicas adicionais de condução nervosa no síndrome do t únel do carpo (STC) leve quando o valor de lat ência dist al sensit iva do nervo mediano (rot ina) est á dent ro dos limit es normais. Condução nervosa bilat eral foi realizada em 116 pacient es consecut ivos com STC sint omát ico (153 mãos). A seleção foi feit a baseada na rot ina normal (< 3,7 ms, medida no pico, 14 cm) e, pelo menos uma técnica anormal entre as seguintes: diferença sensitiva mediano-radial (M R); diferença sensit iva mediano-ulnar (M U4); diferença mediano-ulnar palmar (M UP); lat ência palmar do mediano (PW); e lat ência dist al mot ora do mediano (M DL). Os valores normais da rot ina foram separados em grupos desde 3,1 at é 3,6 ms (< 3,7 ms), obt endo-se valores anormais ent re 86,6 e 93,4% (M R), 40 e 81.7% (M U4), 20 e 71,2% (M UP), 0 e 41,1% (PW) e 0 e 19,6% (M DL). A associação anormal mais frequent e foi M R com M U4 em 90,1%, seguido de M R com M UP e M U4 com M UP. A t écnica adicional isolada anormal mais frequent e foi M R seguida de M U4 e M UP. O percent ual de anormalidade da t écnica M R foi muit o elevada, independent ement e do valor de cort e na condução rot ina (3,1 a 3,6 ms).
PALAVRAS-CHAVE: síndrome do túnel do carpo, nervo mediano, neuropatia compressiva, eletroneuromiografia, condução nervosa.
Elect romyography Laborat ory, Clinical Neurophysiology, Depart ment of Neurological Sciences, St at e M edical School, São Jose do Rio Pret o SP, Brazil: 1Associat e-Professor (M D, PhD); 2Assist ent -Professor (M D, M Sc); 3Post graduat e St udent (M D).
Received 19 April 2002, received in final form 14 June 2002. Accept ed 22 June 2002.
Dr. João Aris Kouyoumdjian - Avenida Bady Bassit t 3896 - 15025-000 São José do Rio Pret o SP - Brasil. FAX: 55 17 232-7757. E-mail: jaris@t erra.com.br
Carpal t unnel syndrome (CTS) is t he most com-mon ent rapment neuropat hy in upper limbs. Elec-trodiagnosis is very sensitive and specific for the diag-nosis and several st udies have report ed sensit ivit y in t he range of 80 t o 92%1. Comparison of t he
sensi-t ivisensi-t ies of sensi-t he various nerve conducsensi-t ion sensi-t echniques for CTS diagnosis had demonst rat ed t hat sensory conduct ion is bet t er t han mot or conduct ion and t he median sensory dist al lat ency in w rist -digit segment
(13 or 14 cm) is less sensit ive t han t echniques w hich evaluat e median mixed palm lat ency (8 cm) eit her absolut e or comparat ive t o ulnar, or sensory lat en-cies differences from median-ulnar (14 cm) or me-dian-radial (10 cm) in t he same hand2.
distal sensory latency (wrist-index finger; 14 cm) is found to be below the upper limit of normality (ULN).
M ETHODS
Pat ient s
From June 1998 t o Sept ember 2000, 116 consecut ive pat ient s w it h a clinically confirmed diagnosis of CTS w ere st udied, including hand paraest hesia, numbness, and pain mainly at night ; isolat ed pain w as not considered. Pat ient s w it h diabet es mellit us but no elect rophysiological evidence o f p o lyn eu ro p at h y w ere in clu d ed . Cases w it h o n ly unilat eral nerve conduct ion st udies, or previous CTS sur-gery, asympt omat ic subject s, t hose w it h clinical or elect ro-physiological evidence of polyneuropat hy, and t hose w it h w rist t rauma relat ed t o CTS side w ere excluded.
Elect rophysiology (nerve conduct ion st udies)
All patients had bilateral nerve conduction studies using Cant at a (Dant ec, Skovlunde, Denmark) elet romyography machine. Palmar t emperat ures w ere maint ained above 31 C (digit al t herm om et er, Braile Biom edica, São Jose Rio Pret o, SP, Brazil). Elect rophysiological t echniques are des-cribed as follow s; all lat encies except mot or dist al lat ency, w ere measured t o t he negat ive peak; abnormal cut -offs w ere obt ained from t he most described dat a on lit erat ure2.
1. M edian dist al sensory lat ency (rout ine). The st imu-lat ion delivered on median nerve at w rist act ivat e ant i-dromic sensory act ion pot ent ials at t he second digit ; w e used a fixed 14 cm dist ance from t he ring recording elec-t rodes elec-t haelec-t w ere placed around elec-t he proximal (recording, cat hode) and dist al (ref erence, anode) int erphalangeal joint s. The absolut e lat ency value w as defined as abnormal w hen equal or great er t han 3.7 ms.
2. Sensory median-radial difference (M R). M edian nerve st im ulat ion w as delivered at w rist in order t o act ivat e antidromic sensory action potentials at the thumb; w e used an approximat ely 10 cm dist ance from t he ring recording elect rodes around t he t humb. Radial nerve st imulat ion w as delivered at t he lat eral edge of t he radius in t he dist al forearm at t he same line used for median nerve st imu-lat ion; t he recording ring elect rodes around t he t humb w ere t he same. The lat ency difference w as defined as ab-normal w hen equal or great er t han 0.50 ms.
3. Sensory m edian-ulnar dif f erence (M U4). M edian nerve st imulat ion w as delivered at w rist in order t o act ivat e ant idromic sensory act ion pot ent ials at t he fourt h digit ; w e used a fixed 14 cm dist ance from t he ring recording el ect r o d es t h at w er e p l aced ar o u n d t h e p r o xi m al (recording, cat hode) and dist al (reference, anode) int er-phalangeal joint s. Wrist ulnar nerve st im ulat ion w as d el i ver ed at t h e sam e l i n e u sed f o r m ed i an n er ve st imulat ion. The lat ency difference w as defined as abnor-mal w hen equal or great er t han 0.40 ms.
4. M ixed median palm lat ency (PW). M edian nerve st i-mulat ion w as delivered at t he palm (mixed nerve) in order t o act ivat e ort hodromically mainly sensory act ion pot en-t ials aen-t en-t he w risen-t ; w e used a fixed 8 cm disen-t ance from en-t he
bar recording elect rode t hat w ere placed at t he w rist (cat hode dist al). The absolut e lat ency value w as defined as abnormal w hen equal or great er t han 2.30 ms.
5. M ixed median-ulnar palm difference (M UP). M edian nerve st imulat ion w as delivered at t he palm (mixed nerve) in order t o act ivat e ort hodromically mainly sensory act ion pot ent ials at t he w rist ; w e used a fixed 8 cm dist ance from t he bar recording elect rode t hat w ere placed at t he w rist (cat hode dist al). In t he same w ay, ulnar nerve st imulat ion w as done at t he palm (ulnar edge) and recording on w rist (ulnar edge). The lat ency difference w as defined as ab-normal w hen equal or great er t han 0.40 ms.
6. M edian mot or dist al lat ency (M DL). M edian nerve st imulat ion w as delivered at w rist in order t o act ivat e t he compound muscular act ion pot ent ial at t he t henar emi-nence; w e used a fixed 8 cm dist ance from t he disc recor-ding elect rodes t hat w ere placed over t he belly of t he
Abduct or Pollicis Brevis muscle (recording, cat hode) and just dist al t o t he met acarpophalangeal joint (reference, anode). The absolut e lat ency value w as defined as abnor-mal w hen equal or great er t han 4.40 ms.
M ild CTS cases w ere defined w hen rout ine median sen-sory dist al lat ency (w rist t o index finger; 14 cm) w as below 3.7 ms (group 1), below 3.6 ms (group 2), below 3.5 ms (group 3), below 3.4 ms (group 4), below 3.3 ms (group 5), below 3.2 ms (group 6), and, below 3.1 ms (group 7) since t he ULN described for t he rout ine median sensory dist al lat ency could vary among different aut hors. In t hese groups, at least one addit ional nerve conduct ion t echnique performed, as described above, w as found to be abnormal. All t est s w ere done by t he aut hors using t he same EM G inst rument (DANTEC, Cant at a); percut aneous st imuli w ere delivered unt il supram axim al response obt ained; pulse durat ion w ere 0.05/0.1 ms for sensory and mixed nerve st imulat ion and 0.2/0.5 ms for mot or nerve st imulat ion; filt ers w ere set at 20 Hz and 2 kHz; t he sw eep speed w as set at 1 ms per division; bar elect rodes or one-cent imet er disc recording, eit her plat inum or disposable elect rodes, w ere used for mixed nerve st udies and ring elect rodes for sensory st udies; eit her disposable or velcro around t he forearm w ere used as ground.
RESULTS
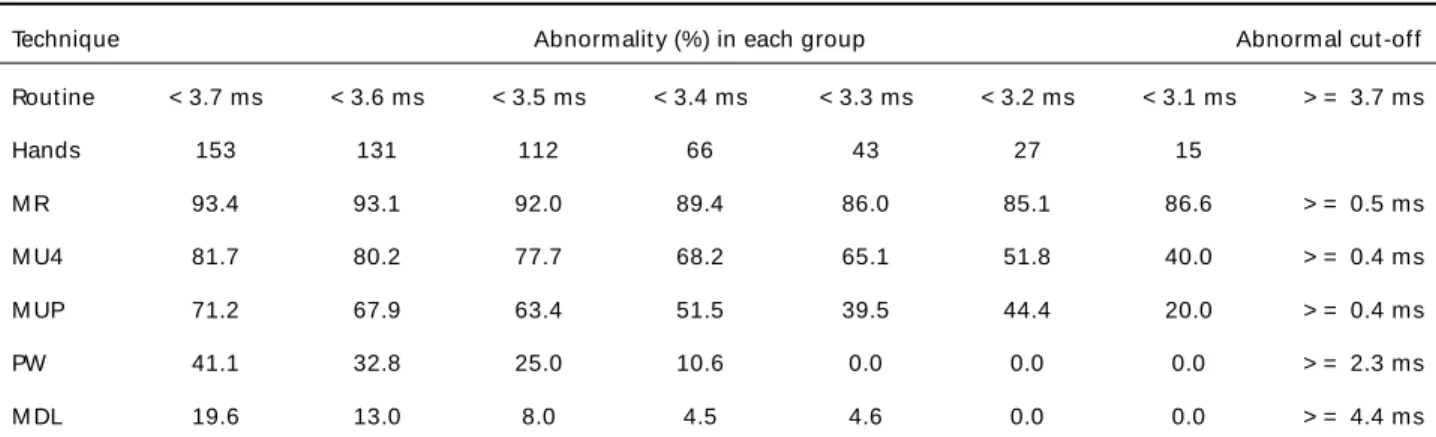
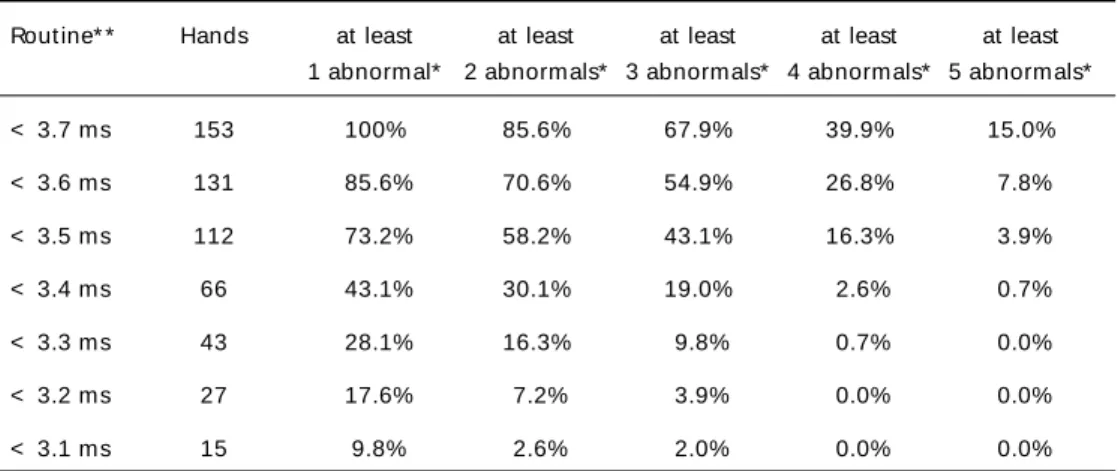
highest value regardless t he seven cut -off rout ine lat ency values, ranging from 93.4 t o 86.6%. The per-cent age of abnormalit y of M U4 reaches t he second highest value regardless t he seven cut -off rout ine lat ency values, ranging from 81.7 t o 40%. The per-cent age of abnormalit y of M UP reaches t he t hird highest value w it h a broader variat ion aft er t he seven cut -off rout ine lat ency values (71.2 t o 20%). The per-cent age of abnormalit y of PW and M DL reached t he smallest value, and, as t he cut -off rout ine lat encies drop from less t han 3.7 t o less t han 3.1 ms, t hey ranged from 41.1 t o 0%, and from 19.6 t o 0%, res-pectively. We also evaluated the percentage of abnor-mality w hen more than one additional technique w e-re found t o be abnormal aft er normal rout ine me-dian sensory dist al lat ency (less t han 3.7 ms) in 131 hands. Abnormalit y of bot h M R and M U4 w as found in 118/131 hands (90.1%), follow ed by M R and M UP in 8/131 hands (6.1%) and M U4 and M UP in 2/131 hands (1.5%). Only in 3 hands out of 131 (2.3%), one of t he 2 abnormal t echniques w ere ot her t han M R, M U4 and M UP. Table 2 show s t he percent age of abnormalit y from all 153 hands w hen at least 1, 2, 3, 4 or 5 additional techniques w ere found abnormal.
DISCUSSION
Our result s clearly show ed t hat t he lat ency diffe-rences aft er sensory radial, sensory median-ulnar and mixed palm median-median-ulnar t echniques are bet t er t han t he rout ine median sensory lat ency, w rist t o index finger, 14 cm, for CTS elect rodiagnosis, as st at ed by AAEM Qualit y Assurance Com m it t ee2.
These t hree t echniques are above 71.2% of abnor-malit y w hen rout ine sensory conduct ion is st ill below t he ULN, considered as 3.7 ms3,4. The absolut e mixed
median palm lat ency w as abnormal in 41.1% and
t he median mot or dist al lat ency in just 19.6% poin-t ing oupoin-t poin-t hapoin-t poin-t he mospoin-t sensipoin-t ive poin-t echniques are poin-t he comparat ive ones. When w e considered t he ULN for rout ine sensory as less t han 3.6 ms, less t han 3.5 ms, less t han 3.4 ms, less t han 3.3 ms, less t han 3.2 ms or even less t han 3.1 ms, t he percent age of ab-norm alit y in com parat ive t echnique M R w as very high, ranging from 93.4 t o 86.6%. M U4 and M UP show ed less dramat ic posit ivit y ranging from 40 t o 81.7% (M U4) and from 20 t o 71.2% (M UP). This w as just ified because of in some EM G labs t he ULN used for sensory routine could be different. In our previous sim ilar st udy5, w e f ound M R t o be abnorm al in
97.8%, M UP in 88.4% and M U4 in 72.6%, but w e w orked on onset -measured lat ency and t he ULN for rout ine sensory median dist al lat ency w as 3.5 ms (40 m/s). The use of just one abnormal addit ional t echnique aft er normal rout ine median sensory dist al lat ency should be avoided because of t he possible decrease of specificit y in CTS elect rodiagnosis. Our result s show ed t hat w hen at least 2 addit ional t ech-niques w ere abnormal, t he most common associa-t ion w as M R plus M U4 (90.1%) and, in a less exassocia-t enassocia-t , M R plus M UP and M U4 plus M UP.
Som e consid erat ions should b e em p hasized about t he ideal ULN t hat w e could use t o have a correct CTS elect rodiagnosis. The cut -off lat encies for CTS elect rodiagnosis or t o define normal values could increase or decrease the sensitivity or specificity leading to false-positive or false-negative electrodiag-nosis. The abnormal percent age and t he cut -off la-t encies described in la-t he lila-t erala-t ure for la-t he la-t echniques have a w ide variat ion and t here is no consensus about w hich one is t he best or gold st andard and in t his st udy w e use a broad range, f rom a m ore conservat ive 3.7 ms t o a less specific 3.1 ms. Because
Table 1. M ild carpal t unnel syndrome and percent age of abnormalit y of 5 nerve conduct ion t echniques.
Technique Abnormalit y (%) in each group Abnormal cut -off
Rout ine < 3.7 ms < 3.6 ms < 3.5 ms < 3.4 ms < 3.3 ms < 3.2 ms < 3.1 ms > = 3.7 ms
Hands 153 131 112 66 43 27 15
M R 93.4 93.1 92.0 89.4 86.0 85.1 86.6 > = 0.5 ms
M U4 81.7 80.2 77.7 68.2 65.1 51.8 40.0 > = 0.4 ms
M UP 71.2 67.9 63.4 51.5 39.5 44.4 20.0 > = 0.4 ms
PW 41.1 32.8 25.0 10.6 0.0 0.0 0.0 > = 2.3 ms
M DL 19.6 13.0 8.0 4.5 4.6 0.0 0.0 > = 4.4 ms
of median and radial nerve st imulat ion w as delivered at t he same line (w rist for median and lat eral edge of t he radius for radial nerve) inst ead of 1 cm above on radial nerve st imulat ion, w e considered abnormal lat ency difference as > = 0.5 ms and not as 0.4 ms, as described in several papers2.
Report s of abnormal percent age for M R are des-cribed as 44%6,7, 58%7, 59.6%8, 87.2%9, 89%10,
90%11, and 100%12. Report s of abnormal percent age
for M U4 are described as 42%11, 44%6, 78%13, 87%14,
88.6%9, 93%15, 99.2%10, and 100%16,17. Report s of
abnormal percentage for M UP are described as 30%6,
57%18, 60%19 and 61%11. The possible cause of
variabilit y in t he result s could be mainly due t o t he cut -off lat ency value for rout ine median sensory nerve conduct ion t hat , in our opinion, should alw ays be below ULN. If t he purpose of t he st udy is t o find out w hich t echnique is t he most useful, w e should est a-blish t he ULN of each one and aft er t hat include in t he result s at least one abnormal value. It could be argued t hat some pat ient s w ere false posit ive be-cause t he ULN used in t his st udy could be found in some normal individuals according t o populat ion se-lect ion1. In addit ion, it is import ant t o include just
hands in w hich rout ine median sensory dist al lat ency is below t he ULN in order t o select only mild cases an d p reven t s h ig h p ercen t ag e o f ab n o rm alit y. Probably all cases could show abnormalit y in com-parative techniques (more sensitive techniques) if the rout ine m edian dist al sensory lat ency is equal or higher t han 3.7 ms, peak-measured.
As st at ed before, a very int erest ing and puzzling finding of our result s w as t he fact t hat even aft er t he rout ine median sensory dist al lat ency decreased from 3.7 t o 3.1 ms, t he percent age M R abnormalit y w ent dow n just a lit t le (93.4 t o 86.6%) w hen
com-pared t o M U4 (81.7 t o 40%) or M UP (71.2 t o 20%). Why t he median-radial lat ency difference maint ains a high percent age of abnormalit y w hereas t he ot her t echniques diminished more proport ionally in accor-dance t o t he reduct ion of rout ine median sensory distal latency? Should w e consider the ULN more than 0.5 ms for M R or it is just a matter of a greater sus-ceptibility of the median fascicle for thumb?
It should be emphasized that our results do not represent the real sensitivity of the electrodiagnosis tests in CTS because w e alw ays include hands w ith at least one abnormal technique; the purpose w as to compare the most sensitive among them. Also, w e believed that w hen only one abnormal comparative t echnique is f ound t oget her w it h norm al rout ine median sensory distal latency it should be considered possible or incipient CTS; nerve conduction studies follow -up should be further required. Redmond and Rivner20 emphasized the increment of false-positive
CTS elect rodiagnosis af t er t he use of addit ional t echniques. M ore t han one abnorm al addit ional technique could be found to keep a high specificity1.
If more t han one comparat ive t echnique is found above ULN even w ith normal routine median sensory distal latency the CTS electrodiagnosis is more reliable.
REFERENCES
1. Andary MT, Werner RA. Electrodiagnosis in clinical decision making: carpal tunnel syndrome. 1997 AAEM Course B: Using electrodiagnosis in clinical decision making. AAEM 20th Annual Continuing Education Courses 1997, San Diego, USA.
2. Jablecki CK, Andary MT, So YT, Wilkins DE, Willians FH. Literature review o f the usefulness o f nerve co nd uctio n stud ies and elec-tro myo graphy fo r the evaluatio n o f patients w ith carpal tunnel syndrome. Muscle Nerve 1993;16:1392-1414.
3. Johnson EW, Melvin JL. Sensory conduction studies of median and ulnar nerves. Arch Phys Med Rehabil 1967;48:25-30.
4. Di Benedetto M, Mitz M, Klingbeil GE, Davidoff D. New criteria for sensory nerve conduction especially useful in diagnosing carpal tunnel syndrome. Arch Phys Med Rehabil 1986;67:586-589.
Table 2. M ild carpal t unnel syndrome and percent age of abnormalit y f or addit ional t echniques.
Rout ine* * Hands at least at least at least at least at least 1 abnormal* 2 abnormals* 3 abnormals* 4 abnormals* 5 abnormals*
< 3.7 ms 153 100% 85.6% 67.9% 39.9% 15.0%
< 3.6 ms 131 85.6% 70.6% 54.9% 26.8% 7.8%
< 3.5 ms 112 73.2% 58.2% 43.1% 16.3% 3.9%
< 3.4 ms 66 43.1% 30.1% 19.0% 2.6% 0.7%
< 3.3 ms 43 28.1% 16.3% 9.8% 0.7% 0.0%
< 3.2 ms 27 17.6% 7.2% 3.9% 0.0% 0.0%
< 3.1 ms 15 9.8% 2.6% 2.0% 0.0% 0.0%
5. Kouyoumdjian JA , Morita MPA . Comparison of nerve conduction techniques in 95 mild carpal tunnel hand s. A rq Neuro psquiatr 1999;57:195-197.
6. Jackson D, Clifford JC. Electrodiagnosis of mild carpal tunnel syndrome. Arch Phys Med Rehabil 1989;70:199-204.
7. White JC, Hansen SR, Johnson RK. A comparison of EMG procedures in the carpal tunnel syndrome with clinical-EMG correlations. Muscle Nerve 1988;11:1177-1182.
8. Carrol G. Comparison of the median and radial sensory latencies in the electro p hysio lo gical d iagno sis o f carp al tunnel synd ro me. Electroencephalogr Clin Neurophysiol 1987;68:101-106.
9. Pease WS, Cannell CD, Johnson EW. Median to radial latency difference test in mild carpal tunnel syndrome. Muscle Nerve1989;12:905-909. 10. Cioni R, Passero S, Paradiso C, Giannini F, Battistini N, Rushworth G.
Diagnostic specificity of sensory and motor nerve conduction variables in early detection of carpal tunnel syndrome. J Neurol 1989;236:208-213. 11. Andary MT, Fankhauser MJ, Ritson JL, et al. Comparison of sensory mid-palm studies to other techniques in carpal tunnel syndrome. Electromyogr Clin Neurophysiol 1996;36:279-285.
12. Johnson EW, Sipski M, Lammertse T. Median and radial sensory latencies to digit I: normal values and usefulness in carpal tunnel syndrome. Arch Phys Med Rehabil 1987;68:140-141.
13. Uncini A, Lange DJ, Solomon M, Soliven B, Meer J, Lovelace RE. Ring finger testing in carpal tunnel syndrome: a comparative study of diagnostic utility. Muscle Nerve 1989;12:735-741.
14. Lauritzen M, Liguori R, Trojaborg W. Orthodromic sensory conduction along the ring finger in normal subjects and in patients with a carpal tunnel syndrome. Electroencephalogr Clin Neurophysiol 1991;81:18-23. 15. Monga TN, Laidlow DM. Carpal tunnel syndrome measurement of sensory potentials using ring and index fingers. A m J Phys Med 1982;61:123-129.
16. Johnson EW, Kukla RD, Wongsam PE, Piedmont A. Sensory latencies to the ring finger: normal values and relation to carpal tunnel syndrome. Arch Phys Med Rehabil 1981;62:206-208.
17. Charles N, Vial C, Chauplannaz G, Bady B. Clinical validation of antidromic stimulation of the ring finger in early electrodiagnosis of mild carpal tunnel syndrome. Electroencephalogr Clin Neurophysiol 1990;76:142-147. 18. Kim LYS. Palmar d igital stimulatio n to d iagno se carpal tunnel
syndrome. Orthop Rev1983;(6):59-63.
19. Mills KR. Ortho d ro mic senso ry actio n p o tentials fro m p almar stimulation in the diagnosis of carpal tunnel syndrome. J Neurol Neurosurg Psychiatry 1985;48:250-255.