Effect of breastfeeding on child and material adiposity 4-5 years after birth: results from the Portuguese birth cohort
Texto
Imagem



Documentos relacionados
Com o conceito da negação determinada, Hegel destacou um elemento que distingue o esclarecimento da desagregação positivista à qual ele o atribui.” (Id.. 59) Em sua relação
A cannabis permanece como a substância ilícita mais consumida no mundo. Defendida por uns e “diabolizada” por outros, constitui uma das substâncias
Quanto à percepção ambiental sobre os impactos causados ao meio ambiente quando da eliminação do lixo gerado no condomínio, dos 54 moradores entrevistados, 88,89%
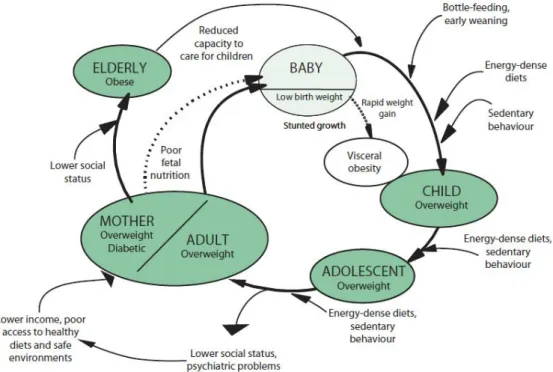
The direct effect of birth weight on adiposity in adult life, adjusted for socioeconomic status at the time of birth and the number of cigarettes smoked by the mother
To analyze the effect of breastfeeding duration on the age of persistence of paciier-sucking habits, the sample was assigned to ive groups by duration, in months,
In the present study, other initial difficulties with breastfeeding technique, such as the inadequate posi- tioning of the binomial mother/child, problems with the latch, mother and
No entanto, mesmo nesse contexto de perdas ela não desiste de ficar com o filho por acreditar que, para a criança, ainda é melhor estar com a mãe, ape-. sar dos desafios e
to promote the bond between mother and child and in the promotion of maternal well-being, but is inserted in a context of social conflicts and losses; Experiencing daily attachment
