www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
The
role
of
uric
acid
in
the
insulin
resistance
in
children
and
adolescents
with
obesity
Josiane
Aparecida
de
Miranda
a,∗,
Guilherme
Gomide
Almeida
b,
Raissa
Isabelle
Leão
Martins
b,
Mariana
Botrel
Cunha
b,
Vanessa
Almeida
Belo
c,
José
Eduardo
Tanus
dos
Santos
c,
Carlos
Alberto
Mourão-Júnior
b,
Carla
Márcia
Moreira
Lanna
baUniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil bUniversidadeFederaldeJuizdeFora(UFJF),JuizdeFora,MG,Brazil cUniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
Received19December2014;accepted29March2015 Availableonline24August2015
KEYWORDS
Childhoodobesity; Insulinresistance; Uricacid
Abstract
Objective: Toinvestigatetheassociationbetweenserumuricacidlevelsandinsulinresistance inchildrenandadolescentswithobesity.
Methods: Cross-sectionalstudywith245childrenandadolescents(134obeseand111controls), aged8---18years.Theanthropometricvariables(weight,heightandwaistcircumference),blood pressureandbiochemicalparameterswerecollected.Theclinicalcharacteristicsofthegroups wereanalyzedbyt-testorchi-squaretest.Toevaluatetheassociationbetweenuricacidlevels andinsulinresistancethePearson’stestandlogisticregressionwereapplied.
Results: Theprevalenceofinsulinresistancewas26.9%.Theanthropometricvariables,systolic anddiastolicbloodpressureandbiochemicalvariablesweresignificantlyhigherintheobese group(p<0.001),exceptforthehigh-density-lipoproteincholesterol.Therewasapositiveand significant correlationbetweenanthropometricvariables anduricacidwithHOMA-IR inthe obeseandinthecontrolgroups,whichwashigherintheobesegroupandinthetotalsample. Thelogisticregressionmodelthatincludedage,genderandobesity,showedanoddsratioof uricacidasavariableassociatedwithinsulinresistanceof1.91(95%CI1.40---2.62;p<−0.001).
Conclusions: The increase inserum uricacid showed apositive statistical correlationwith insulin resistanceanditisassociated withand increasedriskofinsulinresistanceinobese childrenandadolescents.
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-license(https://creativecommons.org/licenses/by/4.0/).
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2015.03.009
∗Correspondingauthor.
E-mail:[email protected](J.A.Miranda).
PALAVRAS-CHAVE
Obesidadepediátrica; Resistênciaàinsulina; Ácidoúrico
Opapeldoácidoúriconaresistênciainsulínicaemcrianc¸aseadolescentescom obesidade
Resumo
Objetivo: Investigaraassociac¸ãoentreosníveisséricosdeácidoúricoeresistênciainsulínica emcrianc¸aseadolescentescomobesidade.
Métodos: Estudotransversal,com245crianc¸aseadolescentes(134obesose111controles), comidadeentreoitoe18anos.Foramcoletadasvariáveisantropométricas(peso,estaturae circunferênciaabdominal),pressãoarterialeparâmetrosbioquímicos.Ascaracterísticas clíni-casdosgruposforamanalisadaspelotestetoupeloqui-quadrado.Paraavaliaraassociac¸ão entreosníveisdeácidoúricoearesistênciainsulínicautilizou-seotestedePearsoneregressão logística,sendoaresistênciainsulínicaavariáveldependentenomodeloderegressão.
Resultados: Aprevalênciaderesistênciainsulínicafoide26,9%.Asvariáveisantropométricas, apressãoarterialsistólicaediastólicaeasvariáveisbioquímicasforammaioresnogrupoobeso (p<0,001),excetoocolesteroldealtadensidade.Foiobservadacorrelac¸ãopositivae significa-tivaentreasvariáveisantropométricaseoácidoúricocomoHOMA-IRnogrupoobesoeno controle,sendoestamaiornogrupoobesoenaamostratotal.Nomodeloderegressão logís-ticaqueincluiuidade,sexoeobesidade,aOddsRatiodoácidoúricocomofatorassociadoà resistênciainsulínicafoi1,91(IC95%1,40---2,62;p<0,001).
Conclusões: Observa-se queoaumento nonível séricode ácido úricoapresenta correlac¸ão estatísticapositivacomaresistênciainsulínicaeestáassociadoàelevac¸ãonoriscodamesma, emcrianc¸aseadolescentesobesos.
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Uricacidistheendproductofpurinemetabolism,produced bytheliverandexcretedbythekidneys,1withrecognized
antioxidantaction when itsblood levelsarewithin
physi-ologicallimits.2However,theincreaseinitsserumlevels,
calledhyperuricemia,isanindependentriskfactorfor
car-diovasculardiseaseandalsohasaroleinthedevelopment
ofmetabolicdiseases.3---5Moreover,recentprospective
stud-ieswithrepresentative samplesindicatehyperuricemia as
apredictor for the developmentof insulin resistanceand
type 2 diabetes mellitus.4,5 Krishnan et al.5 showed that
hyperuricemiaincreasesby1.87-foldthechanceof
devel-opingtype2diabetesmellitusand1.36-foldthechanceof
developinginsulinresistanceafter15yearsoffollow-up.
Oneofthepathologicalconditionsassociatedwith
hype-ruricemiaisobesity.6,7 Obeseindividualshave lowerrenal
excretion, and may also have increased production of
uric acid.8 In children and adolescents, studies indicate
that the association between hyperuricemia and
obe-sity is positive6 and it is associated with cardiometabolic
complications, such as hypertension, atherosclerosis and
metabolicsyndrome.9---12Yooetal.13studiedtheprevalence
of insulin resistance and metabolic syndrome in patients
withgout, which is a metabolic disease characterized by
hyperuricemiaanddepositionofmonosodiumuratecrystals
inthejointsandtissues.Theauthorsconcludedthatthese
patientshaveahigherprevalenceofinsulinresistanceand
metabolicsyndromewhencomparedtotheirhealthypeers,
andthathyperuricemiainassociationwithinsulinresistance
maybecausedbyabdominalobesity.13
Inthiscontext,inwhichhyperuricemiahasbeen
identi-fiedasanotherlinkbetweenobesityandinsulinresistance,
studies in thepediatric population arescarce. Therefore,
the aim of this study was to investigate the association
between serum uric acid levels and insulin resistance in
obesechildrenandadolescents.
Method
Cross-sectionalstudywithaquantitativeapproach,partof aprojectentitled‘‘Associationofgeneticpolymorphismsof cardiovascular relevance with systemic arterial hyperten-sionandobesityinchildhoodandadolescence’’,approved by theInstitutional Review Boardof UniversidadeFederal deJuizdeFora,processnumber1942.001.2010. Allthose involvedintheresearch,parentsorguardiansandchildren andadolescentswereinformedofthestudyobjectivesand procedures,andthosewhoagreedtoparticipateinthestudy signedtheInformedConsentForm.
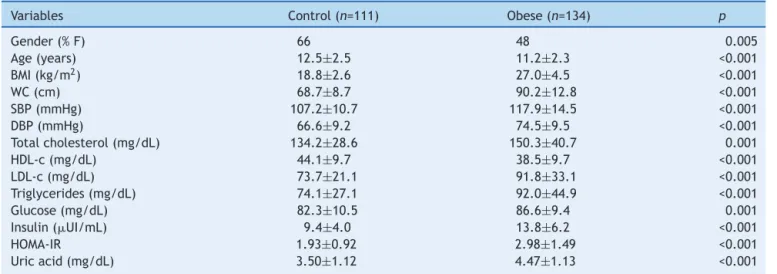
Table1 Clinicalcharacteristicsofthestudygroups.
Variables Control(n=111) Obese(n=134) p
Gender(%F) 66 48 0.005
Age(years) 12.5±2.5 11.2±2.3 <0.001
BMI(kg/m2) 18.8
±2.6 27.0±4.5 <0.001
WC(cm) 68.7±8.7 90.2±12.8 <0.001
SBP(mmHg) 107.2±10.7 117.9±14.5 <0.001
DBP(mmHg) 66.6±9.2 74.5±9.5 <0.001
Totalcholesterol(mg/dL) 134.2±28.6 150.3±40.7 0.001
HDL-c(mg/dL) 44.1±9.7 38.5±9.7 <0.001
LDL-c(mg/dL) 73.7±21.1 91.8±33.1 <0.001
Triglycerides(mg/dL) 74.1±27.1 92.0±44.9 <0.001
Glucose(mg/dL) 82.3±10.5 86.6±9.4 0.001
Insulin(UI/mL) 9.4±4.0 13.8±6.2 <0.001
HOMA-IR 1.93±0.92 2.98±1.49 <0.001
Uricacid(mg/dL) 3.50±1.12 4.47±1.13 <0.001
F,female;M,male;BMI,bodymassindex;WC,waistcircumference;SBP,systolicbloodpressure;DBP,diastolicbloodpressure;HDL, high-densitylipoprotein;LDL,low-densitylipoprotein;HOMA-IR,homeostaticmodelassessmentforinsulinresistance.
infectionandpregnancy.Allchildrenandadolescents under-wentphysicalexamination.
Weight and height were measured while participants werewearinglightclothingandnoshoes.Heightwas mea-suredwitha0.1cm-accuracyusingawallstadiometer.Body weight was measured with a digital scale with a 0.1 kg-accuracy. Obesity was defined as body mass index (BMI) abovethe95thpercentileforage andgender.14 Waist
cir-cumference (WC)wasmeasuredusingan inelastictapeat
midpointbetweenthelastribandtheupperborderofthe
iliaccrest.15Bloodpressurewasmeasuredbyauscultation,
andtheappropriatecuffsizewasconsidered.Afterresting
for10mininaquietenvironment,bloodpressure
measure-ment was taken.16 After the physical examination, blood
collectionwasperformedby venipunctureinthemorning,
after12hoffasting.Thebloodwasimmediatelycentrifuged
atroomtemperature,andplasmaandserumsampleswere
storedat−70◦Cuntiltheywereanalyzed.
Thelevelsofglucose,uricacidandthelipidparameters
(totalcholesterol,triglyceridesandhigh-density-lipoprotein
cholesterol) were measured in serum, withroutine
enzy-maticmethods,usingcommercialkits(LabtestDiagnostics,
AS, Lagoa Santa, Brazil). The level of
low-density-lipoproteincholesterolwasestimatedusingtheFriedewald
formula.17 The insulin level was determined by serum
enzyme immunoassay kit (Genese Produtos Diagnósticos,
São Paulo, Brazil).The estimateof insulin resistance was
obtained through the Homeostasis Model Assessment for
InsulinResistance (HOMA-IR),which is theproductof
fas-tinginsulin (U/mL)andfastingplasmaglucose(mmol/L)
divided by 22.5. Insulin resistance is defined when the
HOMA-IRvaluewasgreaterthanorequalto3.16.18
Dataareshownasmean±standarddeviation.The
clini-calcharacteristicsofthegroupswereanalyzedusingthetor
Chi-squaretests.Toevaluatetheassociationbetweenage,
BMI,WC,systolicbloodpressure,diastolicblood pressure,
HDLanduricacidwithHOMA-IR,we usedPearson’s
corre-lationtest. Alogistic regression modelwasalsoproduced
tomeasuretheassociationbetweenuricacidlevels
(inde-pendentvariable)andinsulinresistance(binarydependent
variable).Otherindependentvariablesandpotentially
con-foundingvariables(age,genderandobesity)wereincluded
in theregression model in order tocontrol their possible
effectoninsulinresistance.Theselectedindependent
varia-bles were included in the model because of the known
associationbetweenthemandinsulinresistance.6The
sig-nificancelevelwassetat5%(p<0.05)foralltests,andthe
statisticalsoftwareusedwasSPSSversion15.0.
Results
Weevaluated245childrenandadolescents(55.9%females) and the prevalence of insulin resistance was 26.9%. The clinicalcharacteristicsoftheassessedgroupsareshownin Table1.As expected,theobesegrouphadhigherBMIand
WCvalues than the control group (p<0.001). The systolic
anddiastolicbloodpressureswerehigherintheobesegroup
whencomparedtothecontrolgroup(p<0.001).Inaddition,
allthebiochemicalcharacteristics,totalcholesterol,LDL,
triglycerides,glucose, uric acid, insulin and HOMA-IRhad
higherlevelsintheobesegroup,exceptfortheHDL,which
waslowerintheobesegroupwhencomparedtothecontrol
group(p<0.001).
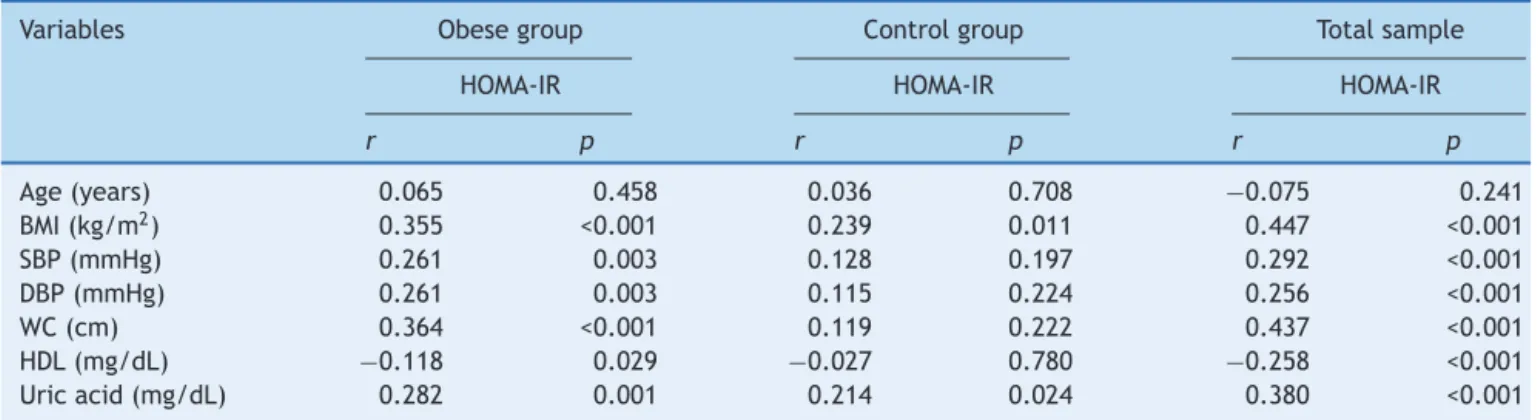
Table 2 shows the results of the correlation analysis
betweenthevariablesage,BMI,WC,systolicbloodpressure,
diastolic blood pressure, HDL and uric acid with
HOMA-IR in obese, control groups and in both groups. In the
obesegrouptherewasapositiveandsignificantcorrelation
between most of the variableswith the HOMA-IR,except
forage,whichwasnotcorrelatedwithHOMA-IR,andHDL,
whichshowedanegativecorrelation.Inthecontrolgroup,
therewasapositiveandsignificantcorrelationbetweenBMI
andHOMA-IR and uricacid and HOMA-IR. When analyzing
the total sample, there is a positive and significant
cor-relationbetween most of the variablesand theHOMA-IR,
except for age, which was not correlated withHOMA-IR,
andHDL,whichshowedanegativecorrelation.The
Table2 CorrelationbetweenHOMA-IRandthevariablesanalyzedbygroups.
Variables Obesegroup Controlgroup Totalsample
HOMA-IR HOMA-IR HOMA-IR
r p r p r p
Age(years) 0.065 0.458 0.036 0.708 −0.075 0.241
BMI(kg/m2) 0.355 <0.001 0.239 0.011 0.447 <0.001
SBP(mmHg) 0.261 0.003 0.128 0.197 0.292 <0.001
DBP(mmHg) 0.261 0.003 0.115 0.224 0.256 <0.001
WC(cm) 0.364 <0.001 0.119 0.222 0.437 <0.001
HDL(mg/dL) −0.118 0.029 −0.027 0.780 −0.258 <0.001 Uricacid(mg/dL) 0.282 0.001 0.214 0.024 0.380 <0.001
BMI,bodymassindex;WC,waistcircumference;SBP,systolicbloodpressure;DBP,diastolicbloodpressure;HDL,high-densitylipoprotein; HOMA-IR,homeostaticmodelassessmentforinsulinresistance.
acidshowedthebestcorrelations withHOMA-IR (r=0.447, r=0.437andr=380;p<0.001respectively).
The associationof insulinresistancewithuricacid lev-elswasalsoassessedinalogisticregressionmodel,which included age, gender and obesity as independent varia-bles.Thelogisticregressionmodelproducedtomeasurethe associationbetweenuricacidlevels(independentvariable) andinsulinresistance(binarydependentvariable)included other independent variables and potentially confounding variables(age,genderandobesity),included inthemodel tocontrol theirpossibleeffects oninsulin resistance.The dependent variable (insulin resistance) was dichotomized accordingtotheHOMA-IRcutoffpoint(3.16).Theoddsratio (OR)ofuricacidwas1.91(95%CI:1.40---2.62;p<0.001), indi-catingthattheincreaseofoneuricacidunitincreasesby 91%thelikelihoodofinsulinresistance.
Discussion
Themainfindingofthisstudywastheassociationbetween serumuricacidlevelsandinsulinresistanceinchildrenand adolescents,evenafteradjustingforage,obesityand gen-der. After adjusting for these variables, it was observed that,for everyincreaseof1mg/dLinserumuricacid lev-els,therewouldbea91%increaseinthechanceofinsulin resistance.Evenwhenanalyzingtheobeseandthecontrol groupsalone,uricacidandBMIshowedacorrelation with HOMA-IR(Table2).
Thisfindingisinagreementwithotherauthors,whoalso
observedanassociationbetweenuricacidlevelsandinsulin
resistance in studies involving children in a more limited
agerange.6,9Gil-Campos etal.6 foundthat inprepubertal
obesechildren,theuricacidlevelsweresignificantlyhigher
whencomparedtothecontrolgroup,afteradjustingfor
gen-der,ageandBMI associatedwithinsulin resistance.These
authorsproposethattheincreaseinserumlevelsofuricacid
maybeanindicatorofearlymetabolicchangesassociated
withother insulin resistancecharacteristics. In our study,
statisticaldifferencewasobservedregardingagebetween
theassessed groups, which was only half of the standard
deviation (50%), and with normal distribution. Thus, this
differencewasnot considered to beclinically significant,
consideringthedegreeofdispersionofthisvariable.
Infact,intheadultpopulation,recentprospective
stud-ies indicate that hyperuricemia is a predictor of insulin
resistanceandtype2diabetesmellitus.4,5,19Aftera
follow-upof15years,Krishnanetal.5showedthathyperuricemia
increases by 1.87-fold the chance of developing type 2
diabetes mellitusandby 1.36-foldthe chanceof
develop-ing insulinresistance. Ina meta-analysis,Kodama etal.19
showedanincreaseof17%intheriskoftype2diabetesfor
everyincreaseof1mg/dLinserumuricacid.
Althoughthephysiopathologicalmechanismsofthe
con-nection betweenhyperuricemia andinsulin resistanceare
not yet clearly established, hyperuricemia is often seen
as the result of the reduction in renal excretion of uric
acidundertheactionofhyperinsulinemia.1,20However,the
aforementionedstudiesopposethisidea,astheyshowthat
hyperuricemiaprecedesinsulinresistance.4,5,19
Inthisstudy,itwasalsonotpossibletoanswerwhatthe
physiopathological mechanisms of serum uric acid
contri-butiononinsulinresistanceareinobesity,but ourwork is
supportedbypreviousresultsofstudieswithanimalmodels
andclinicaltrials,sothatsomespeculationscanbemade.
Obesity is considered a significant risk factor for the
developmentofinsulinresistanceandtype2diabetes
mel-litus, as in obese individuals the adipose tissue releases
substances involved in the development of insulin
resis-tance, such as non-esterified fatty acids, hormones and
proinflammatory cytokines.21,22 Adipose tissue has the
capacitytosecretecytokinesandgrowthfactorsthat
partic-ipateinmanymetabolicprocesses.Someofthesecytokines,
withpro-inflammatorycharacteristicsthatareincreasedin
obesity,aredirectlyassociatedwithinsulinresistance,such
asleptin,TNF-␣andvisfatin,whileadiponectin,acytokine
with anti-inflammatory characteristics, is reduced in the
presenceofobesityandisdescribedasinverselyassociated
withinsulinresistance.21
Anotherfindingofourstudywasthattheobesegrouphad
statisticallyhigherserumuricacidlevelswhencomparedto
thecontrolgroup(4.47±1.13vs.3.50±1.12,p<0.001).This
characteristiccanbeattributedtothefollowingfactors:(1)
obeseindividualshavereducedrenalclearanceofuricacid,
whichcanresultinhigherserumlevels23;(2)adiposetissue,
similartotheliverandintestine,hasabundantactivity of
xanthineoxidase(enzymeresponsibleforcatalyzingpurines
activityofxanthineoxidaseandincreasedproductionofuric
acidbyadiposetissue.8
One of the possible links between hyperuricemia and
insulin resistance seems to be endothelial dysfunction.
Hyperuricemia induction in animals resulted in reduced
nitricoxidebioavailability,vasoconstrictionandthe
devel-opmentof microvascular disease24 and, accordingto Park
et al.,25 uric acid is responsible for attenuating the
pro-ductionofnitricoxidebyreducingtheinteractionbetween
eNOS (endothelial nitric oxide synthase enzyme), and
calmodulin. In fact, clinical studies have shown that
ele-vated levels of uric acid are associated with impaired
vascular function in children and adolescents.12,26 Thus,
thehyperuricemia-mediatedendothelialdysfunctioncould
result in lower insulin uptake by reduced blood flow in
peripheraltissues(lessnitricoxidesupply).1
In addition tointerfering withnitric oxide production,
uric acid may also be responsible for its degradation.
Although, at physiological concentrations, uric acid has
antioxidant effects, thus being an endothelial protective
factor,theincreaseinserumlevelscausesittoplaya
pro-oxidant role, as its formation pathway through xanthine
oxidaseproducesreactiveoxygenspeciesandhydrogen
per-oxide, which, in excess, will react with the endothelial
nitricoxideandcreateperoxynitrite,animportantoxidizing
agent.27
Eventhoughtheobservedmeanserumuricacidlevelin
ourstudywassignificantlyhigherintheobesegroup,when
compared withcontrols, there is no consensusin the
lit-eratureonthe referencevaluesofthismarkerinchildren
andadolescents,whichpreventscomparisons.However,we
believethattheserumuricacidlevelisagoodalternativeto
assesscardiometabolicriskevenatayoungage,asitcanbe
seeninourresults.Forthispurpose,itbecomesnecessary
tocarryoutstudiesaimedatestablishingreferencevalues
tohelpinclinicaldiagnosis.
This study has some limitations and, amongthem, we
indicatetheuseofHOMA-IRtoassessinsulinresistance.This
indicator,although itis notthegold standard, isawidely
usedmethodbecauseofitsviability.Theabsenceof
puber-talstatusassessmentisanotherlimitation,consideringthe
agerangeused(8---18years).Thecross-sectionalnatureof
thestudydoesnotallowustoestablishacausalassociation
betweenthevariables.
Basedontheobservedresults,itcanbeconcludedthat
theincreaseinserumuricacidlevelshasapositive
statis-ticalcorrelationwithinsulinresistanceanditisassociated
withthe risk increaseof this resistancein obesechildren
andadolescents.
Funding
ThisstudywasfundedbytheFundac¸ãodeAmparoàPesquisa do Estado de São Paulo (FAPESP) and Coordenac¸ão de Aperfeic¸oamentodePessoaldeNívelSuperior(CAPES).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WethanktheNucleoInterdisciplinardeEstudosePesquisas emNefrologia(NIEPEN)andDr.DéboraCristineSouza-Costa.
References
1.LiC,HsiehMC,ChangSJ.Metabolicsyndrome,diabetes,and hyperuricemia.CurrOpinRheumatol.2013;25:210---6. 2.GlantzounisGK,TsimoyiannisEC,KappasAM,GalarisDA.Uric
acidandoxidativestress.CurrPharmDes.2005;11:4145---51. 3.Fang J, Alderman MH. Serum uric acid and
cardiovascu-lar mortality the NHANES I epidemiologic follow-up study, 1971---1992.NationalHealthandNutritionExaminationSurvey. JAMA.2000;283:2404---10.
4.JuraschekSP,McAdams-DemarcoM,MillerER,GelberAC, May-nardJW,PankowJS,etal.Temporalrelationshipbetweenuric acidconcentrationandriskofdiabetesinacommunity-based studypopulation.AmJEpidemiol.2014;179:684---91.
5.KrishnanE,PandyaBJ,ChungL, HaririA, DabbousO. Hype-ruricemia in young adults and risk of insulin resistance, prediabetes, and diabetes: a 15-year follow-up study.Am J Epidemiol.2012;176:108---16.
6.Gil-CamposM,AguileraCM,Ca˜neteR,GilA.Uricacidis asso-ciatedwithfeatures ofinsulinresistance syndrome inobese childrenatprepubertalstage.NutrHosp.2009;24:607---13. 7.FordES,LiC,CookS,ChoiHK.Serumconcentrationsofuric
acidandthemetabolicsyndromeamongUSchildrenand ado-lescents.Circulation.2007;115:2526---32.
8.TsushimaY,NishizawaH,TochinoY,NakatsujiH,SekimotoR, NagaoH,etal.Uricacidsecretionfromadiposetissueandits increaseinobesity.JBiolChem.2013;288:27138---49.
9.CardosoAS,GonzagaNC,MedeirosCC,CarvalhoDF.Association ofuricacidlevelswithcomponentsofmetabolicsyndromeand non-alcoholicfattyliverdiseaseinoverweightorobesechildren andadolescents.JPediatr(RioJ).2013;89:412---8.
10.ViazziF,AntoliniL,GiussaniM,BrambillaP,GalbiatiS, Mastri-aniS,etal.Serumuricacidandbloodpressureinchildrenat cardiovascularrisk.Pediatrics.2013;132:e93---9.
11.CivantosModinoS,GuijarrodeArmasMG,MonereoMejiasS, MontanoMartinezJM,IglesiasBolanosP,MerinoViverosM,etal. Hyperuricemiaandmetabolicsyndromeinchildrenwith over-weightandobesity.EndocrinolNutr.2012;59:533---8.
12.PacificoL, CantisaniV,AnaniaC,Bonaiuto E,Martino F, Pas-coneR,etal.Serumuricacidanditsassociationwithmetabolic syndromeandcarotidatherosclerosisinobesechildren.EurJ Endocrinol.2009;160:45---52.
13.YooHG,LeeSI,ChaeHJ,ParkSJ,LeeYC,YooWH.Prevalence ofinsulinresistanceandmetabolicsyndromeinpatientswith goutyarthritis.RheumatolInt.2011;31:485---91.
14.KuczmarskiRJ,OgdenCL,Grummer-StrawnLM,FlegalKM,Guo SS,WeiR,etal.CDCgrowthcharts:UnitedStates.AdvData. 2000:1---27.
15.FernandezJR,ReddenDT,PietrobelliA,AllisonDB.Waist cir-cumferencepercentilesinnationallyrepresentativesamplesof African-American,European-American,andMexican-American childrenandadolescents.JPediatr.2004;145:439---44. 16.Sociedade Brasileira de Cardiologia, Sociedade Brasileira de
Hipertensão,SociedadeBrasileirade,Nefrologia.VIDiretrizes BrasileirasdeHipertensão.ArqBrasCardiol.2010;95:1---51. 17.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the
concentrationoflow-densitylipoproteincholesterolinplasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499---502.
glucose/insulinratioandquantitativeinsulinsensitivitycheck indexforassessinginsulinresistanceamongobesechildrenand adolescents.Pediatrics.2005;115:e500---3.
19.KodamaS,SaitoK,YachiY,AsumiM,SugawaraA,TotsukaK, etal.Associationbetweenserumuricacidanddevelopmentof type2diabetes.DiabetesCare.2009;32:1737---42.
20.FeigDI,KangDH,JohnsonRJ.Uricacidandcardiovascularrisk. NEnglJMed.2008;359:1811---21.
21.VanGaalLF,MertensIL,DeBlockCE.Mechanismslinkingobesity withcardiovasculardisease.Nature.2006;444:875---80. 22.BalagopalPB,deFerrantiSD,CookS,DanielsSR,GiddingSS,
HaymanLL,etal.Nontraditionalriskfactorsandbiomarkersfor cardiovasculardisease:mechanistic,research,andclinical con-siderationsforyouth:ascientificstatementfromtheAmerican HeartAssociation.Circulation.2011;123:2749---69.
23.YamashitaS,MatsuzawaY,TokunagaK,FujiokaS,TaruiS. Stud-iesontheimpairedmetabolismofuricacidinobesesubjects: markedreductionofrenalurateexcretionanditsimprovement byalow-caloriediet.IntJObes.1986;10:255---64.
24.KhoslaUM,ZharikovS,FinchJL,NakagawaT,RoncalC,MuW, etal.Hyperuricemia inducesendothelialdysfunction.Kidney Int.2005;67:1739---42.
25.ParkJH,JinYM,HwangS,Cho DH,KangDH,JoI.Uricacid attenuatesnitricoxideproductionbydecreasingtheinteraction between endothelialnitricoxidesynthase and calmodulinin humanumbilicalveinendothelialcells:amechanismforuric acid-inducedcardiovasculardiseasedevelopment.NitricOxide. 2013;32:36---42.
26.Ishiro M, Takaya R, Mori Y, Takitani K, Kono Y, Okasora K, etal.Associationofuricacidwithobesityandendothelial dys-function inchildren and earlyadolescents. Ann NutrMetab. 2013;62:169---76.