rev bras ortop.2014;49(2):202–205
w w w . r b o . o r g . b r
Case
Report
Fixation
of
an
osteochondral
fragment
after
acute
patellar
dislocation
in
an
immature
skeleton
夽
,
夽夽
Rodrigo
Pires
e
Albuquerque
a,∗,
José
Félix
dos
Santos
Neto
b,
Maria
Isabel
Pires
e
Albuquerque
c,
Vincenzo
Giordano
b,
Ney
Pecegueiro
do
Amaral
b aKneeSurgeryCenter,InstitutoNacionaldeTraumatologiaeOrtopedia,RiodeJaneiro,RJ,BrazilbOrthopedicsService,HospitalMunicipalMiguelCouto,RiodeJaneiro,RJ,Brazil
cInstitutoNacionaldoCâncer,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received1May2013 Accepted12July2013
Availableonline27March2014
Keywords: Osteochondritis Bonefractures Patella Kneejoint
a
b
s
t
r
a
c
t
Fixationofanosteochondralfractureafteracutepatellardislocationisaninfrequentformof treatment.Likewise,thelocationofthisfragmentinthelateralregionofthelateralfemoral condyle,functioningasafreebody,isuncommon.Theaimofthisstudywastopresenta caseofosteochondralfractureofthepatellaatanunusualsite,alongwiththetherapyused andtheclinicalfollow-up.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Fixac¸ão
do
fragmento
osteocondral
após
luxac¸ão
aguda
da
patela
no
esqueleto
imaturo
Palavras-chave: Osteocondrite Fraturasósseas Patela
Articulac¸ãodojoelho
r
e
s
u
m
o
Afixac¸ãodafraturaosteocondralapósaluxac¸ãoagudadapatelaéumtratamento infre-quente,bemcomoalocalizac¸ãodessefragmentonaregiãolateraldocôndilofemorallateral quefuncionacomoumcorpolivre.Oobjetivodestapesquisafoiapresentarumcasode fraturaosteocondraldapatelaemsítionãousual,assimcomoaterapêuticaadotadaeo seguimentoclínico.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽Pleasecitethisarticleas:AlbuquerqueRPe,FélixdosSantosNetoJ,AlbuquerqueMIPe,GiordanoV,PecegueirodoAmaralN.OFixac¸ão
dofragmentoosteocondralapósluxac¸ãoagudadapatelanoesqueletoimaturo.RevBrasOrtop.2014;49:202–205.
夽夽Workperformedatthe“ProfessorNovaMonteiro”OrthopedicsandTraumatologyService,HospitalMunicipalMiguelCouto,Riode
Janeiro,RJ,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](R.P.e.Albuquerque).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
rev bras ortop.2014;49(2):202–205
203
Introduction
Acutedislocationofthepatellainanimmatureskeletonisnot anunusualinjuryintheagegroupbetween13and15years.1 Intra-articularosteochondralfracturesare complications thathavebeenestimatedtooccurinaround5%ofcasesof acutedislocationofthepatellaamongchildren,althoughit shouldbeemphasizedthatitisveryrareforfragmentsofthe patellatofunctionasfreebodiesinthejoint.1
Theaimofthisstudywastopresentacaseoffixationof anosteochondralfragmentsubsequenttoacutedislocation ofthepatella,emphasizingthelocationofthefragmentinan unusualregion,thetherapyusedandtheclinicalfollow-up.
Case
report
Thepatientwasahealthy14-year-oldmalewhosuffered a fallfromastandingpositionthatcauseddirecttraumatothe rightknee,andwastakentotheemergencyserviceofour hos-pital.Thepatient’sconditionevolvedimmediately,withpain, hemarthrosisandincapacitytowalk. Physicalexamination revealededemaintheright kneeand hypermobilityofthe patella,incomparisonwiththecontralateralside.Atthetime ofthetrauma,thepatient’sweightwas60kgandhisheight was1.68m.
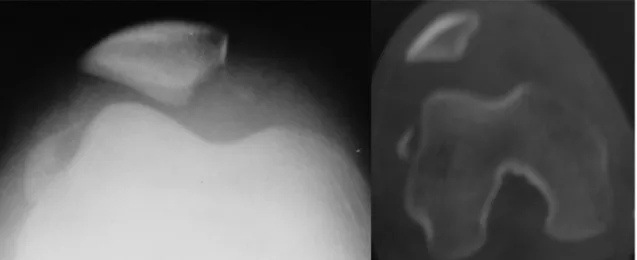
Radiographyontherightkneeshowedamarginalfracture ofthepatellawithanosteochondralfragmentlocatedinthe lateralregionofthelateralfemoralcondyle(Fig.1).Computed tomographywasperformedontherightkneetotryto con-firmthediagnosisandmeasurethesizeoftheosteochondral fragment(Fig.1).
Thephysicalexaminationconductedinconjunctionwith theimagingexaminationsconfirmedthediagnosisofacute dislocationofthepatellaand presenceofafreebodyfrom thejoint,locatedinthelateralregionofthelateralfemoral condyle.
Thesurgerywasperformedtwodaysafterhospital admis-sion,usingatourniquetandastraightmedialincisioninthe right knee. The surgicaltechnique used consisted ofopen reductionand osteosynthesis withthree3-mm cannulated
metalscrews intheosteochondralfragmentofthe patella. Themedialpatellofemoralligamentwasrepairedbymeans ofatransosseoussuture(Fig.2AandB).Theosteosynthesis wastestedbymeansofcarefulflexionofthekneejoint.
Aftertheoperation,thekneewasimmobilizedusingalong kneeimmobilizerforsixweeks.Thiswasremovedforactive rehabilitationexercisesinordertoavoidatrophyofthe quadri-ceps.The programconsistedofisometric exercisesfor the quadricepsduringtheimmobilizationperiodandactive exer-cisesforthequadricepswithprogressiveincreasesinrange ofmotion.Completerangeofmotionandafullyfunctioning kneewereachievedinfivemonths.
Ourpatientwasevaluatedoneweek,15days,onemonth, 45daysandtwomonthsaftertheoperationandthenmonthly untilthesixthmonth,whentheconsultationsbecame three-monthly.Wehavenowfollowedupthispatientfortwoyears andhehasreturnedtohishabitualactivitiesaccompaniedby radiologicalcontrols(Fig.3).Inthefunctionalevaluationson theknee,weusedthemodifiedLysholmsystem.2Weobtained ameanscoreof94pointsintherightknee,whichisconsidered excellentinthisevaluationsystem(Fig.4).
Discussion
Thecasesinthe literaturehavepredominantly occurredin females.1 Our case goes against the data inthe literature, whichemphasizestheimportanceofthepresentcasereport. Webelievethatfemalesaremoreaffectedbecauseofgreater ligament laxity, and also because of hormonal alterations resultingfromthebeginningofthemenstrualcycle.
Themeanageaccordingtotheliteratureis13.3years,and thiswascorroboratedbyourpatient,whowas14yearsofage.1 Hernandezetal.3observedthatosteochondralfragments subsequenttodislocationofthepatellamaygounnoticedon radiographsoftheknee.Wesharedtheirthinkingand,forthis reason,eventhoughwehad madethediagnosis bymeans of radiographs, werequested computed tomography scans inordertounderstandtheinjurybetter.Unfortunately,our servicedoesnothavemagneticresonanceimaging(MRI) avail-able,whichwewouldotherwisehaverequested.Webelieve
204
rev bras ortop.2014;49(2):202–205Fig.2–(AandB)Intraoperativeanalysis.
rev bras ortop.2014;49(2):202–205
205
Fig.4–Postoperativefunctionalevaluation.
thatMRIistheimagingexaminationthatbestassessesthe softtissuesoftheknee.
Nomuraetal.4observedintheirseriesthatthemedialfacet ofthepatella wasthe mostfrequentsite ofosteochondral fractures.However,theydidnotobserveanyfragmentinthe lateralregionofthelateralfemoralcondyle.Forthisreason,we believethatitwasimportantforourrarecasetobepublished. ConradandStanitski5 concludedthattreatmentsuccess dependson early diagnosis ofthe osteochondralfragment andarapidlyimplementedsurgicalapproach.Wecorroborate thisthinkingandemphasizethatawell-performedimaging studyfavorssurgicalplanning.FelusandKowalczyk6andBitar etal.7statedthatthesizeoftheosteochondralfragmentwould determinewhetherfixationorremovalwastobeperformed. HintonandSharma8observedthatosteochondralfragments generallydonotpresentsufficientsizeforreductionand fixa-tionandnormallyareremoved.Nietosvaaraetal.1onlyused fixationinthreecasesoftheirsample.Inthislight,ourcaseis relevantbecauseofthegoodfunctionalresultandthetherapy adopted.
Conradand Stanitski5 alsoshowedthatmany materials are available forfixation of osteochondralfragments after acutedislocationofthe patella.Weusedcannulated metal screwsbecausetheseweretheonlyfixationdevicesthatwere availabletousinourhospitalatthatmoment.Kramerand Pace9 observedthatinthepediatricpopulation, becauseof thelackofstudiesorinvestigationswithlong-termfollow-up, itwasnotpossibletostatethatoneimplantwassuperiorto another.
In our opinion, medial arthrotomy was the best surgi-calapproach because of the location of the osteochondral fragment and because of the ability to view the medial patellofemoralligament.KramerandPace9agreedthat frag-ments of the patella should be dealt with through this access.
Hinton and Sharma8 advocated early exercise with goodguidance,progressivelyimplementedaccordingtothe patient’s level of pain. They reported that through this approach,theatrophyofthequadricepswasdiminishedand thejointcartilagewaskepthealthy.Weagreewiththis think-ing.
Conclusion
Fixationofthe osteochondralfragment ofthe patellaafter acutedislocationusingmetalscrewswasagoodtherapeutic approach.Theunusuallocationofthisfragment,which func-tionedasafreebodyinthejoint,madethisarareinjury.Our patienthasbeenfollowedupfortwoyearssincethe opera-tion,withanexcellentresultaccordingtothescoringsystem used.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.NietosvaaraY,AaltoK,KallioPE.Acutepatellardislocationin children:incidenceandassociatedosteochondralfractures.J PediatrOrthop.1994;14(4):513–5.
2.TegnerY,LysholmJ.Ratingsystemsintheevaluationofknee ligamentinjuries.ClinOrthopRelatRes.1985;(198):43–9. 3.HernandezAJ,FavaroE,LarayaMH.Luxac¸ãoagudadapatela.
RevBrasOrtop.2004;39(3):65–74.
4.NomuraE,InoueM,KurimuraM.Chondralandosteochondral injuriesassociatedwithacutepatellardislocation.
Arthroscopy.2003;19(7):717–21.
5.ConradJM,StanitskiCL.Adolescentacutepatellardislocation. OperTechSportsMed.2001;9(3):190–3.
6.FelusJ,KowalczykB.Age-relateddifferencesinmedial patellofemoralligamentinjurypatternsintraumaticpatellar dislocation:caseseriesof50surgicallytreatedchildrenand adolescents.AmJSportsMed.2012;40(10):2357–64. 7.BitarAC,D’EliaCO,DemangeMK,ViegasAC,CamanhoGL.
Estudoprospectivorandomizadosobrealuxac¸ãotraumática dapatela:tratamentoconservadorversusreconstruc¸ãodo ligamentofemoropatelarmedialcomtendãopatelar–mínimo dedoisanosdeseguimento.RevBrasOrtop.2011;46(6):675–83. 8.HintonRY,SharmaKM.Acuteandrecurrentpatellarinstability
intheyoungathlete.OrthopClinNorthAm.2003;34(3):385–96. 9.KramerDE,PaceJL.Acutetraumaticandsports-related