www.jped.com.br
ORIGINAL
ARTICLE
Comparison
of
two
dose
regimens
of
ibuprofen
for
the
closure
of
patent
ductus
arteriosus
in
preterm
newborns
夽
,
夽夽
Laura
Vargas
Dornelles
a,
Andréa
Lúcia
Corso
a,b,
Rita
de
Cássia
Silveira
a,b,
Renato
Soibelmann
Procianoy
a,b,∗aServiceofNeonatology,HospitaldeClínicasdePortoAlegre(HCPA),PortoAlegre,RS,Brazil
bDepartmentofPediatrics,SchoolofMedicine,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
Received27May2015;accepted2September2015 Availableonline3March2016
KEYWORDS
Patentductus arteriosus; Ibuprofen; Preterminfant
Abstract
Objective: Tocomparetheefficacyofintravenousibuprofenathigh(20-10-10mg/kg/dose)and lowdoses(10-5-5mg/kg/dose)theclosureofpatentductusarteriosusinpretermnewborns.
Methods: Acohortstudywithhistoricalcontrolofnewbornsthatreceivedhigh-andlow-dose intravenousibuprofen,from2010to2013inaneonatalintensivecareunit,forclosureofthe patentductusarteriosus,documentedbyechocardiography.Secondaryoutcomesincludedthe numberofibuprofencycles,incidenceofbronchopulmonarydysplasia,necrotizing enterocoli-tis,changesinrenalfunction,anddeath.
Results: Seventy-sevenpatientsreceivedthreedosesofibuprofenforthetreatmentofpatent ductusarteriosus,with33receivinghigh-doseand44low-dosetherapy.Theductusclosedafter thefirstcyclein25(56.8%)low-dosepatientsandin17(51.5%)high-dosepatients(p>0.99). Sixteen patients received asecond cycle ofibuprofen,and the ductus closed in50% after low-doseandin60% after high-dose therapy(p>0.99).Seven patients required surgeryfor ductusclosure,13.6%inthelow-dosegroupand3%inthehigh-dosegroup(p=0.22). Thirty-ninepatientsdevelopedbronchopulmonarydysplasia,50%inthelow-dosegroupand51.5%in thehigh-dosegroup(p>0.99).Twenty-two(50%)low-dosepatientsdiedvs.15(45.5%)high-dose patients(p=0.86).
Conclusions: There was no difference in closureof the ductus arteriosus or occurrence of adverseeffectsbetweenthetwodoseregimens.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
夽 Pleasecitethisarticleas:DornellesLV,CorsoAL,SilveiraRC,ProcianoyRS.Comparisonoftwodoseregimensofibuprofenfortheclosure
ofpatentductusarteriosusinpretermnewborns.JPediatr(RioJ).2016;92:314---8.
夽夽ThestudyisassociatedwiththeNeonatologyService,HospitaldeClínicasdePortoAlegre(HCPA),PortoAlegre,RS,Brazil. ∗Correspondingauthor.
E-mail:[email protected](R.S.Procianoy). http://dx.doi.org/10.1016/j.jped.2015.09.009
PALAVRAS-CHAVE
Permeabilidadedo canalarterial; Ibuprofeno; Recém-nascido prematuro
Comparac¸ãodedoisesquemasposológicosdeibuprofenoparaofechamentodocanal arterialemrecém-nascidospré-termo
Resumo
Objetivo: Comparar a eficácia do ibuprofeno endovenoso em doses altas (20, 10 e 10mg/kg/dose)eemdosesbaixas(10,5e5mg/kg/dose)paraofechamentodocanalarterial emrecém-nascidospré-termo.
Métodos: Estudodecoortecomcontrolehistóricopesquisandorecém-nascidosquereceberam ibuprofenoendovenoso, noperíodo de2010à2013naunidade deinternac¸ãoneonatal, em dosesaltasebaixasparaofechamentodocanalarterial,documentadoporecocardiograma. Comodesfechossecundáriosforamavaliadosonúmerodeciclosdeibuprofenorealizados,a incidênciadedisplasiabroncopulmonar,enterocolitenecrosante,alterac¸ãodefunc¸ãorenale óbito.
Resultados: 77pacientesreceberam3dosesdeibuprofenoparatratamentodocanalarterial, sendoque33dosealtae44dosebaixa.25(56.8%)dosquereceberamdosebaixafecharamo canalapóso1◦cicloe17(51,5%)fecharamapósreceberemdosealta(p>0.99).16pacientes receberamo2◦ ciclo,destes50%fecharamocanalapósusodedosebaixae60%apósouso dedosealta(p>0.99).7pacientesforamàcirurgiaparafechamentodocanal,sendo13,6%do grupoquerecebeudosebaixae3%dosealta(p=0.22).39pacientesdesenvolveramdisplasia broncopulmonar,50%dogrupodedosebaixae51,5%dogrupodedosealta(p>0.99).22(50%) dospacientesdogrupodosebaixaevoluiuaóbitoversus15(45,5%)dospacientesdogrupode dosealta(p=0.86).
Conclusão: Nãoencontramosdiferenc¸aemrelac¸ãoaofechamentodocanalarterial,assimcomo ocorrênciadeefeitosadversos,quandocomparamososdoisesquemasposológicos.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Patent ductus arteriosus (PDA) is the most common car-diac abnormality in preterm newborns, especially those under 28 weeks old of gestational age.1 This alteration
causes a left-right shunt through the ductus arteriosus andcan become clinically evident.When symptomatic,it increases the need for ventilatory support, increases the risk of peri-intraventricular hemorrhage,2 of
bronchopul-monary dysplasia (BPD)3,4 and necrotizing enterocolitis,5
and reduces survival rates.6 However, there is no clear
evidence of the long-term results of PDA treatment.7
Several randomized controlled trials have failed to show any benefit from treatment on survival and long-term outcomes.1,8,9
Amoreconservativeapproachhasbeenincreasingly sug-gested,especiallyinpatientswithgoodclinicalevolution. Thisisduetothehighchanceofspontaneousclosure,more commoninnewbornsweighing>800g,withouttheneedfor mechanicalventilationandwithnosignsofheartfailureor pulmonarycongestion.10,11
In patients whose patent ductus arteriosus becomes clinically relevant and symptomatic, its constriction can be induced with cyclooxygenase inhibitors, such as indomethacinandibuprofen,withpermanentclosurerates ofaround60---80%.12---14Bothhavesideeffects,butibuprofen
seemstohave fewernegativeeffects onthecerebral and renalbloodflowandalsopossiblyfewergastrointestinalside effects.15---17
Therecommendedstandarddoseofintravenous ibupro-fenfor patent ductusarteriosus closure is 10mg/kg/dose onthefirstdayand5mg/kg/doseonthesecondandthird days.18,19However,Danietal.16demonstratedthattheuse
of ibuprofen at high doses (20-10-10mg/kg/day) is more effectivethanthestandardregimenforPDAinpreterm new-bornswithagestationalage<29weeks,withoutincreasing therateofadverseeffects.
Fromthe year 2012, aimingto achievehigher rates of PDAclosureinpretermnewborns,ibuprofendoseregimens werechangedforthedrugtreatmentofPDAintheNeonatal IntensiveCareUnitofHospitaldeClínicasdePortoAlegre (HCPA).Higher doses of ibuprofen started to be utilized, ratherthanthepreviously usedstandard dose.Therefore, the doses changed to 20mg/kg of ibuprofen for the first intravenousinfusiononday1,followedby10mg/kgondays 2and3,whennewbornsshowedahemodynamically signifi-cantductusarteriosusconfirmedbytheechocardiography.
Thisstudyaimstocomparethetherapeuticeffectiveness andtheimpactofthetwoibuprofendosesonPDAclosure ratesinpretermnewborns,aswellasothermorbiditiessuch asBPD,renalimpairment,needforsurgeryforPDAclosure, anddeath.
Methods
ibuprofenintheperiodofJanuary2010toDecember2013 forthetreatmentofpatentductusarteriosusinthe Neona-tology Service of HCPA. The HCPAis a university tertiary referralhospitalwiththecapacitytoadmitupto50 new-borns.Ithas 20neonatalintensive care unit(NICU) beds, whichencompasslesscomplexcasestoextremelypreterm newborns and those with rare diseases. The study was approvedbytheethicscommitteeoftheinstitution.
Thepopulationwasdividedintotwogroups,one receiv-ing low-dose ibuprofen (10-5-5mg/kg/day --- single daily dose),treatedbeforethechangeindoseregimensandthose receivinghigh-doseibuprofen(20-10-10mg/kg/day---single dailydose)for threedays,treatedafterthechangeinthe careprotocol.
Allpatientsunderwentechocardiographyforthe diagno-sisofPDA.Treatmentwasindicatedforthosewithsignificant clinical signs and presence of respiratory symptoms, and with echocardiography findings showing left-right shunt throughtheductusarteriosus withleftatrium/aorticroot ratio≥1.5mm.
Newborns with congenital heart malformation, those without an echocardiogram toconfirm the diagnosis, and thosewhodidnotcomplete thetreatment duetoclinical instabilityordeathwereexcluded.
The collected demographic data included gestational age,birthweight,daysoflifeatthebeginningoftreatment, needforotheribuprofentreatmentcycles,needforsurgical closure, death, and neonatal morbidities, such as bron-chopulmonarydysplasia(definedasneed forsupplemental oxygenorventilatorysupportat28daysoflife),necrotizing enterocolitis(presenceofpneumatosisorintestinal perfo-ration), need for ventilatory support (continuous positive airwaypressure[CPAP],noninvasivemechanicalventilation [NIMV], mechanical ventilation [MV], and high-frequency ventilation[HFV]),presenceofchorioamnionitis,sepsiswith positive blood cultures, and peri-intraventricular hemor-rhagegradesIIIandIV.Serumcreatinineandurealevels48h beforeandaftercompletionofeachtreatmentcyclewere alsorecorded.
Theclosureofthepatentductusarteriosus,theprimary outcome,wasdefinedascompletePDAclosureobservedon echocardiography.
This study compared the clinical outcome of patients receiving higherdoses of ibuprofen withthose previously treatedwithlowerdoses.
Statistical
analysis
Samplesizecalculation
Todetectadifferenceof30percentagepoints(from40%to 10%ofductusarteriosusclosurefailure),consideringpower of 80% and ˛=0.05, 32 patients were necessary in each
group.
Statisticaltests
Datawerestoredinadatabase createdwiththesoftware SPSS®version18.0(SPSSInc.Released2009.PASWStatistics forWindows,Version18.0IL,USA),whichwasalsousedfor
statisticalanalyses.Categoricalvariablesweredescribedas absoluteandrelativefrequencies,continuousvariableswith symmetrical distributionasmean and standard deviation, andtheasymmetricalvariablesasmedianandinterquartile range.Categorical variableswerecomparedusingFisher’s exacttest,thequantitativevariableswithsymmetrical dis-tributionbyStudent’st-test,andthosewithasymmetrical distribution by the Mann---Whitney test. The significance levelwassetat0.05.
The study was approved by the institutional research committee, and all researchers signed a consent form in ordertoobtainaccesstopatients’medicalrecords,inwhich theysworetomaintaincompleteconfidentiality.
Results
A total of 84patients received ibuprofen for PDA closure intheabovementionedperiod;sevenwereexcluded,three because they received five ibuprofen doses rather than one or two cycles of three doses, and four patients due to the incomplete treatment because of death or major clinical instability. There were no losses due to cardiac malformations or lack of diagnosis on echocardiography. The percentageof losseswas 8.3%. The study population consistedof77patients,ofwhom33(42.8%)received high-doseand44(57.1%)low-doseibuprofen.
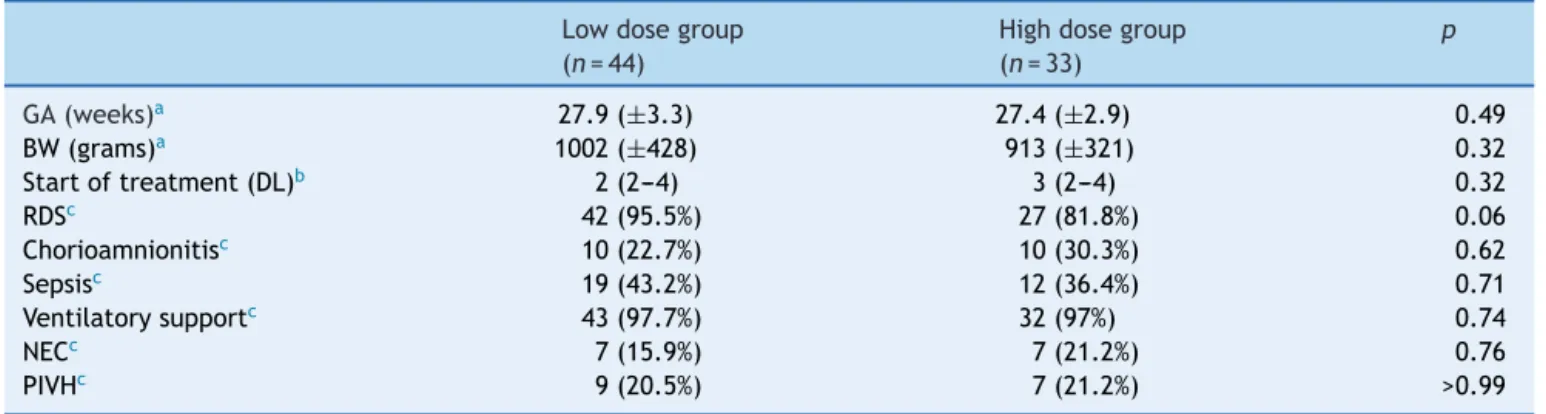
There was no significant difference between the two groups regarding birth weight (p=0.32), gestational age (p=0.49), days of life at the beginning of the treatment withibuprofen(p=0.32),chorioamnionitis(p=0.62),need formechanicalventilation(p=0.74),necrotizing enterocol-itis (p=0.76), peri-intraventricular hemorrhage (p>0.99), hyalinemembrane disease(p=0.06),and infectionwitha positiveculture(p=0.71)(Table1).
Among those who received low-dose treatment, 25 (56.8%)hadPDAclosureafterthefirstcycleofibuprofenand 17(51.5%)afterreceivinghigh-dosetreatment(p>0.99).A totalof22.7%ofthepatientsinthelow-dosegroupreceived asecondcyclevs.18.2%ofpatientsinthehigh-dosegroup (p=0.63).
Sixteenpatientsreceivedasecondibuprofencycle,but only 13 weresubmitted toan echocardiogram at the end of treatment;eightpatients fromthe low-dosegroupand fivefromthehigh-dosegroup.Fourpatients(50%)hadPDA closureafterthelow-doseandthree(60%)afterthe high-dosetreatment(p>0.99).
Table1 Characteristicsofthestudiedpatients.
Lowdosegroup Highdosegroup p
(n=44) (n=33)
GA(weeks)a 27.9(±3.3) 27.4(±2.9) 0.49
BW(grams)a 1002(±428) 913(±321) 0.32
Startoftreatment(DL)b 2(2---4) 3(2---4) 0.32
RDSc 42(95.5%) 27(81.8%) 0.06
Chorioamnionitisc 10(22.7%) 10(30.3%) 0.62
Sepsisc 19(43.2%) 12(36.4%) 0.71
Ventilatorysupportc 43(97.7%) 32(97%) 0.74
NECc 7(15.9%) 7(21.2%) 0.76
PIVHc 9(20.5%) 7(21.2%) >0.99
GA,gestationalage;BW,birthweight;DL,daysoflife;RDS,respiratorydistresssyndrome;sepsis,presenceofpositivebloodculture; NEC,necrotizingenterocolitis;PIVH,peri-intraventricularhemorrhage.
a Student’st-test(meanandstandarddeviation). b Mann---Whitneytest(medianandinterquartilerange). c Fisher’sexacttest(frequencyandpercentage).
Table2 Treatmentoutcomes.
Low-dosegroup High-dosegroup p
(n=44) (n=33)
PDAclosedafter1stcyclea 25(56.8%) 17(51.5%) >0.99
Received2ndcyclea 10(22.7%) 6(18.2%) 0.63
PDAclosedafter2ndcyclea 4(50%) 3(60%) >0.99
Ureab 84.2±40.2 77.8±48.9 0.62
Creatinineb 0.86±0.44 0.74±0.32 0.29
Oliguriaa 1(2.3%) 0(0%) >0.99
Surgerya 6(13.6%) 1(3%) 0.22
BPDa 22(50%) 17(51.5%) >0.99
Deatha 22(50%) 15(45.5%) 0.86
PDA,patentductusarteriosus;BPD,bronchopulmonarydysplasia. a Fisher’sexacttest(frequencyandpercentage).
b Student’st-test(meanandstandarddeviation).
Discussion
This studydidnotshow greaterefficiencyof higherdoses of intravenous ibuprofen over the standard dose for PDA closure in preterm newborns. In addition, no differences werefoundregardingtheoccurrenceofshort-termadverse effectsorneonatalmorbiditieswhenthetworegimenswere compared.
The optimal dose of ibuprofen for PDA treatment remains controversial. The standard regimen is based on limited and scarce pharmacokinetic data.19---21 Desfrere
etal.22 suggestedthatahigher-doseregimen,with20,10,
10mg/kg/dayfor threedays,couldattainhigherPDA clo-sureratesinnewbornswithlessthan27weeksofgestational age;however,thetolerabilityandsafetyshouldbecarefully assessed in further studies before being routinely recom-mended.
Meißneretal.10 foundacleartrendtowardhigherrates
ofPDAclosurewithhigherdoseswithnoincreaseinadverse effects,butwithoutstatisticalsignificance.
Hirt et al. demonstrated that, with the increase in postnatalage, plasmaibuprofenclearancealsoincreased, resulting in a reduction of half-life (42.2h at three days
vs.17.7h at fivedays),19 probably dueto thematuration
ofcytochromeP450,whichmetabolizesibuprofen.23 These
authorsconcludedthattheibuprofendose regimenshould beprospectivelytested.
Consideringthehypothesis thatthe increasein ibupro-fen doses for PDA closure would be more effective than the standard dose, with no increase in adverse events, Danietal.designedarandomizedcontrolledstudy,which assessed70 newborns, of whom35 receivedthe standard dose,and35,thedoubledose.The authorsobservedthat thehigh-doseregimenwasmoreeffectiveforPDAclosure inpretermnewbornsyoungerthan27weeksofgestational age,withnoincreaseofadverseeventsrates.16
In disagreement with the results of the study by Dani etal.,16 theuseof highdosesof ibuprofeninthe present
Thisstudyshowednostatisticallysignificantdifferences regarding neonatal morbimortality, such as the presence ofbronchopulmonarydysplasia, peri-intraventricular hem-orrhage,necrotizingenterocolitis,anddeathbetweenthe groupsthatreceiveddifferentdosesofibuprofen.
Renal failure or oliguria has been reported in 5---7% of patients treatedwith ibuprofen for PDAclosure, but it is reversible.1 Among thepatientsinthe presentstudy,only
onehadoliguriaandthispatientbelongedtothelow-dose group.The administrationof higher doseswaswell toler-atedandpatientsshowednoadverseeffects.Therewasno significant differencerelated toserumlevels of ureaand creatinineaftertreatmentwithibuprofenbetweenthetwo groups.Thesefindingsareinagreementwiththedata pre-viouslypublishedintheliterature,whichreportedonlymild adverseeffects.22
Toguaranteethesafetyandefficacyofdifferent ibupro-fendoseregimens,theauthorsemphasizethesmallnumber ofassessedpatientsasalimitationofthisstudy,inaddition toits retrospective design. However, although it appears reasonable to consider higher doses when treatment is startedafterthe5thdayoflife,duetothedrug pharma-cokinetics,itwasnotpossibletoanalyzethisinthepresent studydue tothe smallnumberof assessedpatients. Ran-domized prospective studies could further elucidate this issue.
Thisstudyshowednobenefitinchangingtheibuprofen dose regimentodoubledoses for thetreatment of symp-tomaticPDAinpretermnewborns.Therewasnosignificant differencewhen comparing the twotreatment dose regi-mens.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Hamrick SE, Hansmann G. Patent ductus arteriosus of the preterminfant.Pediatrics.2010;125:1020---30.
2.EvansN,KluckowM.Earlyductalshuntingandintraventricular haemorrhageinventilatedpreterminfants.ArchDisChildFetal NeonatalEd.1996;75:F183---6.
3.MarshallDD,KotelchuckM,YoungTE,BoseCL,KruyerL,O’Shea TM.Riskfactorsforchroniclungdiseaseinthesurfactantera:a NorthCarolinapopulation-basedstudyofverylowbirthweight infants.NorthCarolinaNeonatologistsAssociation.Pediatrics. 1999;104:1345---50.
4.MoscaF,BrayM,LattanzioM,FumagalliM,TosettoC. Compar-ativeevaluationoftheeffectsofindomethacinandibuprofen oncerebralperfusionandoxygenationinpreterminfantswith patentductusarteriosus.JPediatr.1997;131:549---54.
5.Ryder RW, Shelton JD, Guinan ME. Necrotizing enterocoli-tis: aprospectivemulticenterinvestigation.AmJEpidemiol. 1980;112:113---23.
6.NooriS,McCoyM,FriedlichP,BrightB,GottipatiV,SeriI,etal. Failureofductusarteriosusclosureisassociatedwithincreased mortalityinpreterminfants.Pediatrics.2009;123:e138---44.
7.Evans N. Preterm patent ductus arteriosus: a continuing conundrumfor theneonatologist?SeminFetalNeonatalMed. 2015;20:272---7.
8.HeuchanAM,ClymanRI.Managingthepatentductusarteriosus: currenttreatmentoptions.ArchDisChildFetalNeonatalEd. 2014;99:F431---6.
9.Rozé JC, Cambonie G, Marchand-Martin L, Gournay V, Dur-rmeyerX,DuroxM,etal.Associationbetweenearlyscreening for patentductus arteriosusand in-hospitalmortalityamong extremelypreterminfants.JAMA.2015;313:2441---8.
10.MeißnerU, Chakrabarty R, Topf HG, Rascher W, Schroth M. Improvedclosureofpatentductusarteriosuswithhigh doses ofibuprofen.PediatrCardiol.2012;33:586---90.
11.IbrahimTK,HaiumAA,ChandranS,RajaduraiVS.Current con-troversies inthemanagement ofpatent ductus arteriosusin preterminfants.IndianPediatr.2014;51:289---94.
12.ItabashiK,OhnoT,NishidaH.Indomethacinresponsivenessof patent ductus arteriosusand renal abnormalities inpreterm infantstreatedwithindomethacin.JPediatr.2003;143:203---7.
13.OhlssonA, WaliaR, ShahSS.Ibuprofenfor thetreatmentof patentductus arteriosusinpretermand/orlowbirth weight infants.CochraneDatabaseSystRev.2010;(4):CD003481.
14.GournayV,RozeJC,KusterA,DaoudP,CambonieG,HascoetJM, etal.Prophylacticibuprofenversusplaceboinverypremature infants:arandomised,double-blind,placebo-controlledtrial. Lancet.2004;364:1939---44.
15.OncelMY,ErdeveO.Safetyoftherapeuticsusedinmanagement ofpatentductusarteriosusinpreterminfants.CurrDrugSaf. 2015;10:106---12.
16.DaniC,Vangi V,BertiniG, PratesiS, LoriI,Favelli F,et al. High-doseibuprofenforpatentductusarteriosusinextremely preterminfants:arandomizedcontrolledstudy.ClinPharmacol Ther.2012;91:590---6.
17.BenitzWE.Patentductusarteriosus:totreatornottotreat? ArchDisChildFetalNeonatalEd.2012;97:F80---2.
18.ArandaJV,ThomasR.Systematicreview:intravenousibuprofen inpretermnewborns.SeminPerinatol.2006;30:114---20.
19.HirtD,VanOvermeireB, TreluyerJM,LanghendriesJP, Mar-guglio A, Eisinger MJ, et al. Anoptimized ibuprofen dosing schemefor pretermneonates withpatent ductus arteriosus, basedonapopulationpharmacokineticandpharmacodynamic study.BrJClinPharmacol.2008;65:629---36.
20.VanOvermeireB, Touw D,SchepensPJ,Kearns GL,vanden AnkerJN.Ibuprofenpharmacokineticsinpreterminfantswith patentductusarteriosus.ClinPharmacolTher.2001;70:336---43.
21.Aranda JV, Varvarigou A, Beharry K, Bansal R, Bardin C, ModanlouH, et al. Pharmacokinetics and protein binding of intravenousibuprofenintheprematurenewborninfant.Acta Paediatr.1997;86:289---93.
22.DesfrereL,ZoharS,MorvilleP,BrunhesA,ChevretS,PonsG, etal.Dose-findingstudyofibuprofeninpatentductusarteriosus usingthecontinualreassessmentmethod.JClinPharmTher. 2005;30:121---32.