REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
The
impact
of
patients
controlled
analgesia
undergoing
orthopedic
surgery
夽
Aluane
Silva
Dias
a,
Tathyana
Rinaldi
a,
Luciana
Gardin
Barbosa
a,b,∗aHospitaldaAssociac¸ãodeAssistênciaàCrianc¸aDeficiente-AACD,SãoPaulo,SP,Brazil
bIntensiveCare,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(HC-FM-USP),SãoPaulo,SP,Brazil
Received10February2013;accepted10June2013
Availableonline17April2015
KEYWORDS
Analgesia; PCA; Pain;
Orthopedicsurgery;
Postsurgical; Rehabilitation
Abstract
Introduction:Thecurrentlycommonmusculoskeletaldisordershavebeenincreasinglytreated surgically,andthepaincanbealimitingfactorinpostoperativerehabilitation.
Rationale: Patientcontrolledanalgesia(PCA)controlspain,butitsadverseeffectscaninterfere withrehabilitationandinthepatientdischargeprocess.Thisstudybecomesimportant,since therearefewstudiesevaluatingthiscorrelation.
Objectives: Tocomparetheoutcomesofpatientswhousedanddidnotusepatientcontrolled analgesiainpostoperativeorthopedicsurgerywithrespecttopain,unscheduledneedforO2
(oxygen),andtimeofimmobilityandin-hospitallengthofstay.
Methods:Thisisanobservational,prospectivestudyconductedatHospitalAbreuSodréfrom MaytoAugust2012.Thedatawasdailyobtainedthroughassessmentsandinterviewsofpatients undergoingtotalhiparthroplasty(THA)andtotalkneearthroplasty(TKA),thoracolumbarspine arthrodesis(longPVA),cervicalspinearthrodesis(cervicalAVA)andlumbarspinearthrodesis (lumbarPVA).
Results:The studyshowedsome differencesbetweengroups,namely:thepainfullevelwas higherinthegroupundergoinglumbarPVAwithoutPCAcompared withthegroupwithPCA (p=0.03) andinthegroup oflongPVAwithoutPCA intheearlypostoperative period.This lattergroupusedO2foralongertime(p=0.09).
Conclusion: Inthisstudy,PCAwasusefulforanalgesiainpatientsundergoinglumbarPVAand probablywouldhaveinfluencedtheusagetimeofO2inthegroupoflongPVAinfaceofalarger
sample.TheuseofPCAdidnotinfluencethetimeofleavingthebedandthein-hospitallength ofstayforthepatientsstudied.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
夽 AstudybytheHospitalAbreuSodré---Associac¸ãodeAssistênciaàCrianc¸aDeficiente,Moema,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](L.G.Barbosa).
http://dx.doi.org/10.1016/j.bjane.2013.06.023
PALAVRAS-CHAVE
Analgesia; PCA; Dor;
Cirurgiaortopédica;
Pós-cirúrgico;
Reabilitac¸ão
Oimpactodaanalgesiacontroladapelospacientessubmetidosacirurgiasortopédicas
Resumo
Introduc¸ão:Asdisfunc¸õesmusculoesqueléticas, comunsatualmente,têmsidocadavezmais tratadascirurgicamente,eadorépodeserumfatorlimitantenareabilitac¸ãopós-operatória.
Justificativa:A AnalgesiaControladapeloPaciente(PCA)controlaador,porémseusefeitos adversospodeminterferirnoprocessodereabilitac¸ãoealtadospacientes.Estapesquisa torna-seimportante,poispoucosestudosavaliamessacorrelac¸ão.
Objetivos: Compararaevoluc¸ãodospacientesqueusaramenãousaramPCAnopós-operatório de cirurgiasortopédicas em relac¸ãoà dor,necessidadede O2 (oxigênio) não programadae
tempoimobilismoeinternac¸ãohospitalar.
Métodos: Estudo observacional, prospectivo, realizado no Hospital Abreu Sodré de maio a agostode2012.Obteve-sedadosdiáriosatravésdeavaliac¸ãoeentrevistadospacientes sub-metidosàartroplastiatotaldequadril(ATQ)ejoelho(ATJ),artrodesedecolunatoracolombar (AVPlonga),colunacervical(AVAcervical)ecolunalombar(AVPlombar).
Resultados: Oestudoevidencioualgumasdiferenc¸asentreosgrupos,sendoelas:onívelálgico foimaiornogruposubmetidoàAVPlombarsemPCAem relac¸ãoao comPCA (p=0,03)eno grupodeAVPlongasemPCAnoprimeiropós-operatório.Nesseúltimogrupo,houveusodeO2
pormaistempo(p=0,09).
Conclusão:Nesseestudo,aPCAmostrou-seútilparaanalgesiaempacientessubmetidosàAVP lombareprovavelmenteteriainfluêncianotempodeusodeO2nogrupodeAVPlonga,casoa
amostrafossemaior.OusodaPCAnãoinfluenciounotempodesaídadoleitoedeinternac¸ão hospitalarnospacientesestudados.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Currently,musculoskeletal disorders have become a
com-monproblem,inpartduetoincreasedlifeexpectancyand
incidenceofobesityintheworldpopulation.Thesedisorders
causefunctionallimitationsthatinvariablyhavea
progres-sivecourseifnotmanagedproperly.1---3
Treatmentmaybeconservativewithcontrolofsymptoms
throughmedication,physicalorsurgicalrehabilitation,with
repairand/orreplacementofdamagedjoints.2
Surgical techniques have been improved rapidlyin the
lastdecades,butitdoesnotalwaysimpactthe
postopera-tiverehabilitationof patients.Pain severityandlengthof
hospitalstay, especially when added to a previous status
oflimitation,in additiontocomplications associatedwith
the anesthetic and surgical procedure,4 result in greater
morbidityandfunctionalloss5andmayaffectprognosis.6---8
Pain is one of the main factors limiting ambulation,
increasing the risk of thromboembolism by immobility
and causing metabolic changes that affect other
sys-tems.Therefore,individualizedpainmanagementwiththe
use of appropriate analgesic techniques is of paramount
importance. Moreover, early intervention of
rehabilita-tion aiming at a better postoperative recovery6,9---11 may
reduce the length of hospital stay and return to daily
activities.12,13
Thereareseveraltechniquesofanalgesia;however,the
use of patient-controlled analgesia (PCA) is increasingly
presentinhospitals.Thismethod,whichisconsideredsafe
andeffectivefortreatingmoderatetoseverepain,6,14,15is
usedsincethe1970s.
PCApumpsareinfusiondevicesthatallowvariousforms
of programming and whose drug administration may be
intravenousorepidural,continuouslyorthroughadeviceto
requestbolusdoses(intermittent).Thepatientoperatesthe
device,ifnecessary.Thisanalgesictechniqueisoftenused
incasesofseverepain,suchasafterorthopedicsurgery,6or
chronicpain,suchaspatientswithadvancedmalignancies
undergoingpalliativecare.
On the other hand, the use of PCA may be associated
withhypotension, urinary retention, andmotor blockade,
which limitsmobilizationand,withhigh doses ofopioids,
itmayresultinsedation,respiratorydepression,
constipa-tion, confusion, urinary retention, nausea, vomiting, and
pruritus.7Itisnoteworthythatrespiratorydepressionisthe
mosttroublingadverseeffect.Itisexpressedbydecreased
peripheral oxygen saturation (SpO2) and respiratory rate,
assuggestedbysomeauthors.Theoxygenrequirementfor
hypoxemiamanagementmayprolong hospitalization,with
consequentdelayinrehabilitation.9,16,17
Brazilian literature is scarce in studies assessing the
impact of PCA in clinical outcome and rehabilitation of
patientsafterorthopedicsurgery.Theaimofthisstudywas
tocomparetheoutcomeofpatientssubmittedto
orthope-dicsurgery, withandwithout PCA,regarding theneedfor
supplementalO2,patientbedtime,lengthofhospitalstay,
andlevelofpain.
Thus,itispossibletoidentifysituationsthatmayaffect thetimeittakesthepatienttoreturntodailyactivities,in
ordertointervenewithprophylacticresourcesandimprove
postoperative rehabilitation. These factors are important
Table1 Samplecharacterization.
Surgery nwithPCA---sex(f/m) nwithoutPCA---sex(f/m) Meanage Total THA 4(1/3) 19(12/7) 64 23 TKA 23(20/3) 23(20/3) 67.5 46 LongAVP 22(17/5) 8(8/0) 21.6 30 LumbarAVP 23(14/9) 93(61/32) 46.8 116 CervicalAVA 23(17/6) 50.9 23 Total 72(52/20) 166(118/48) 50.1 238
f,female;m,male;n,numberofpatients.
reductionduetoshorterhospitalstays.Theproposedstudy
results mayalso serve asa guidefor improving care
pro-tocols of physiotherapy service, besides contributingto a
betterunderstandingofPCAeffectsonorthopedicpatients.
Methods
Prospective, observationalstudy conductedthrough
moni-toringofpatientsattheAACDHospitalfromMaytoAugust
2012.
A daily screening in hospital occupancy map was
per-formedtoincludepatients.Allpatientsundergoingtotalhip
arthroplasty(THA),totalkneearthroplasty(TKA),
arthrode-sis via posterior approach of thoracolumbar spine (long
AVP),arthrodesisviaanteriorapproachofthecervicalspine
(cervical AVA), and arthrodesis via posterior approach of
lumbar spine (lumbar AVP) were selected. Subsequently,
thesamplewasdividedintotwogroups:withandwithout
PCA.
Exclusion criteria were patients whowere not able to
quantifypainusingthenumericpainscale(NPS),18---20those
with chronic lung disease (COPD, chronic restrictive
pul-monarydiseaseorofchestorigin,asthma,O2dependency),
andhomeusersofnoninvasivemechanicalventilation.
The study was approved by the institutional Ethics
Research Committee. Selected patients were informed
about the study and signed a written consentform.They
weremonitoreddailybytheinvestigatorsinvolvedwhofilled
outaformwithdatacollectedfrommedicalrecords.When
datawerenotavailableinthemedicalrecords,themissing
datawerecollectedviapatientassessment.
The data collection form was filled once a day, with
thepatientat rest, fromthe firstpostoperativeperiodto
hospital discharge. Data were tabulated in spreadsheets,
using Microsoft Excel 2010®, and analyzed statistically.
Mann---Whitney test wasused to compare age, bodymass
index(BMI),lengthof hospitalstay,timeofgettingoutof bed,useofO2,andpainvariables.Fisherexacttestwasused
toevaluatethedifferenceingenderdistributionofpatients.
Whenpatientswereseparatedbylengthofstayortimefor
gettingoutof bed,the pain,BMI,andagevariables were
evaluatedwiththeKruskal---Wallistest,andDunn’spost-test
wasusedformultiplecomparisons.Foradditionalanalysis,
suchascorrelationsbetweenoxygenuseandBMIandage,
theSpearmancorrelationwasapplied.Thesignificancelevel
wassetatp≤0.05.ThesoftwareusedwasGraphPadPRISM®
version5.
Fordaily patient assessment, the following tools were
used:
(a) Datacollectionform;
(b) Pulse oximeter (noninvasive measurement system of
oxyhemoglobinsaturation);
(c) Numerical pain scale (NPS), which allows quantifying
painseveritywithnumbersfromzeroto10(0represents
nopainand10theworstpossiblepain).Theremaining
numbersquantifyintermediatepain18---20.Inthisstudy,
theNPSwasappliedorally.
Results
Thestudyincluded270patients,ofwhich32wereexcluded
fordatacollectionfailure,leavingasampleof238patients.
Ofthese, 170 werewomen (meanage of 50.2 years)and
68men(meanageof47.6years).Table1showsthesample
characteristics.
Comparing groups undergoing THA and TKA with and
without PCA, there was no statistical difference in pain,
age,BMI, use of supplemental O2, timeof gettingout of
bed,andlengthof hospitalstay.The onlysignificant
find-ing was regarding sex: more men than women used PCA
(p<0.0001).
InlongAVPgroup,theuseofsupplementalO2was
sta-tisticallysignificant(p=0.09),indicatingatendencyforO2
consumption bypatients whodid notuse PCA (Fig. 1).In
thesamegroup,therewasnostatisticaldifferenceinother analyzes.
AmongpatientsundergoinglumbarAVPtherewas
statis-ticallysignificant differencebetweenthe groupswithand
Without PCA 15
10
5
0
With PCA O2
use
Figure1 RelationshipofO2useinpatientsofAVPlonggroup,
Without PCA
Pain
6
4
2
*
0
With PCA
Figure 2 Relationship of pain with and without PCA in
patientsoflumbarAVPgroup.*Statisticallysignificant
differ-encebetweenthetwogroups.
Pain
1 0 2 4 6 8 10
2 3 4
*
*vs 2
5 6
Hospital stay (days)
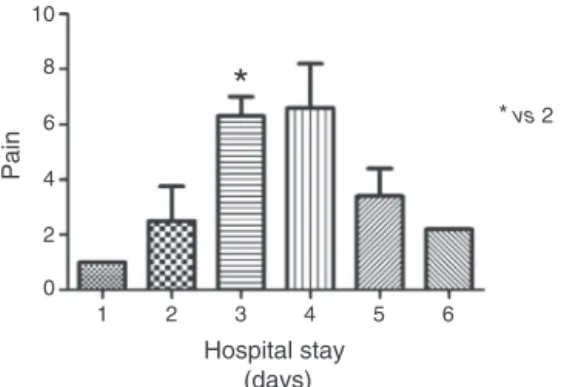
Figure3 Relationshipofpostoperativepainandhospitalstay
inpatientsofcervicalAVAgroup.
withoutPCA(p=0.031).The NPSmeanscorewaslowerin
firstgroup(Fig.2).
PCA wasnotusedby patientsundergoingcervical AVA.
However,when painscale wasassessed, it wasseen that
patients reported more severe pain on the third
postop-erativeday thanonthesecond day(Fig.3).An additional
analysisofdatacomparing BMIvaluewithtimeof getting
outofbedrevealed aclosetosignificant value(p=0.068)
betweenthefirstandsecondpostoperativeperiods,which
indicatesthatthissampleofpatientswithhigherBMItended togetoutofbedlater(Fig.4).
ComparingthemeanNPSofpatientswithPCAwiththose
withoutPCAonthefirstpostoperativeday,analmost
signif-icantdifference(p=0.058)wasfound betweenthegroups
Out of bed time (days)
BMI (kg.m
-2)
1 0 10 20 30 40
2 3
Figure4 RelationshipofBMIandtimeforleavingthebedin
patientsofcervicalAVAgroup.
Without PCA
Long and lumbar AVP pain 1st PO
With PCA 8
6
4
2
0
Figure5 Relationshipofpaininthefirstpostoperativeperiod
betweenpatientswithandwithoutPCAundergoinglumbarand
longAVP.
withandwithoutPCAundergoinglumbarandlongAVP
sur-geries(Fig.5).Therewasnostatisticaldifferencebetween
TKAandTHAsurgeries.
Patients’ pain was analyzed the day after PCA
with-drawal,buttherewasnosignificantdifference.
Table2 shows thedata correlated withthe respective
significantvalues(p-value<0.05)
Discussion
Theresultsofthisstudyshowthattherewasapredominance
ofwomendiagnosedwithosteoarthritis,whichcorroborates
theliterature.21
Moreover, there was no statistical difference in any
of the variables when the groups with and without PCA
submitted tothe THAand TKA surgerieswere compared.
Due to the role of PCA in pain management, it was
expectedthat therewould besome significant difference
regardingpain.Whatcouldbeseenwasthatpatients
asso-ciate pain with the operated limb mobilization periods
and not with rest periods. Because data collection was
notperformed in periodsofactivity,this factormayhave
influenced the results, which causes a limitation in the
study.
The results also showed that the majority of patients
undergoinglongAVPwereyoungwomen.AccordingtoLima
Júnioretal.,22 womentendtohavegreatercurvaturesof
thespine, whichrequired surgicalinterventiontoprevent
progression.
InthisgroupofpatientsundergoinglongAVPtherewas
a nearlysignificant difference in the use of O2 (p=0.09)
between groups withand without PCA, which couldhave
been defined with a larger sample. Pain can be a very
limitingfactorinthisgroupofpatientsbecauseitisamajor
surgery that involves multiple spinal segments,
includ-ing the accessory muscles of respiration, decreases chest
expansion, and impacts on SpO2 and time restricted to
bed.
Accordingtooursresults,itwasrealizedthattherewas
nostatisticallysignificant value regardingPCA use andO2
supplementationintheothergroups.
Asanadditionalfinding,itwasnoticedthatthe
major-ity of patients using O2 had between 60 and 80 years.
Possiblybecauseelderlypatientshavepreviouslimitations
Table2 Correlationsperformedwithmedian,1stand3rdquartile,andp-value. Data Medianwithout
PCA/withPCA
1stquartile withoutPCA/with PCA
3rdquartile withoutPCA/with PCA
p-value
THAage 66/63.5 50/56 78/72.5 0.8076 THABMI 27/30 23/25.25 32/33.25 0.441 THAt 4/4.5 4/3.25 4/7.25 0.4182 THAO2 0/0.5 0/0 0/1 0.3145
THAoutofbed 02/02 2/0 2/0 Morethan2per groupisneeded THApain 02/02 1/1.255 5/3.5 0.6847
TKAage 70/70 65/59 75/73 0.7333 TKABMI 27/30 24/27 32/33 0.307 TKAt 4/4 4/3 5/5 0.8645 TKAO2 0/0 0/0 1/1 0.6289
TKAoutofbed 2/2 2/2 2/2 0.23 TKApain 3/4 1/2 4/5 0.1136 LongAVPage 14.5/16 14/13.75 16.75/22.25 0.6205 LongAVPBMI 18/21 17/18 26/24.25 0.725 LongAVPt 6/5 4.25/5 8.5/7 0.6804 LongAVPO2 0/0 0/0 3/0 0.0956
LongAVPoutof bed
3/2.5 2/2 3/3 0.4215 LongAVPpain 4/3.5 1.5/1 4/4.25 0.9066 LumbarAVPage 47.5/49 35/42 58.75/61 0.2455 LumbarAVPBMI 27/27 24/25 30/31 0.384 LumbarAVPt 3/3 2/3 4/5 0.4061 LumbarAVPO2 0/0 0/0 0/0 0.2131
LumbarAVPoutof bed
2/2 1/2 2/2 0.273 LumbarAVPpain 3.5/2 2/1 5/4 0.0311 TKAandTHApain
1stPO
2/4 0/2 5/7 0.1071 Longandlumbar
AVPpain1stPO
4/3 2/1 6/5 0.0583 WithPCAand
withoutPCA ---samepatient
3/3 0/1 4.5/5 0.3007
THA,totalhiparthroplasty;TKA,totalkneearthroplasty;LongAVP,arthrodesisviaposteriorapproachofthoracolumbarspine;Lumbar AVP,arthrodesisviaposteriorapproachoflumbarspine;t,lengthofhospitalstay;BMI,bodymassindex;O2,oxygenuse;1stPO,first
postoperativeperiod.
procedure,itmaycomplicaterecoveryandleadto
respira-torycomplications.4
In studies of opioids in PCA pumps, respiratory
depression occurs commonly among the first 12---24h.16
However,in thisstudy,datawere collectedfromthe first
postoperativeday.Perhaps,thiswasthereasonwhythere
wasnocaseofrespiratorydepressioninthissample.
Regarding lumbarAVPsurgery, themostcommoncause
washerniateddisk,whichisinaccordancewiththecurrent
literaturereportingthatthis isthemain reasonforspinal surgeryintheadultpopulation.23Itwasalsothelargest sam-pleamongthesurgeriesanalyzedinthisstudy.Themeanage
ofpatientsundergoinglumbarAVPwas46.8years.
Accord-ingly, Vialle et al.23 reported that disk herniation occurs
mainlybetweenthefourthandfifthdecadesoflife,despite beingdescribedinallagegroups.
Patients who used PCA pump after lumbar AVP seem
to have been those who have benefited most from this
resource. They reported lower levels of pain during
hos-pitalstay thanthosewhodidnotusePCA. Perhapsthisis
justifiedbythefactthatspinalsurgerypatientsare
encour-agedtofrequent change ofposition, which mobilizesthe
surgicalsiteandcausepain.However,PCAmayhavea
bet-ter impactin controlling this symptom although it is not
possibletoassertitbasedontheseresults,consideringthat
analgesicsandanti-inflammatorydrugsusedincombination
withPCAwerenotmonitoredinthisstudy.Thisisanother
limitationfound.
AfteranalyzingthelumbarandlongAVPgroupsregarding
painonlyinthefirstpostoperativeperiod,thecomparisonof
patientswithandwithoutPCArevealedthatpatients
performedwithabsolutevalues.Thus,theresultreinforced thebenefitofPCAinthisgroup.
Inthissample,patientsundergoingcervicalAVAdidnot
use PCA pump after surgery and could not be allocated
intotwogroups,asintheother.Therefore,additional
cor-relationswere made and, although not part of the study
objective,wechosetoquotethemhere.BMIwascorrelated
withthetimeofgettingoutofbed,painwiththetimeof
gettingoutofbed,andfinally,painwiththelengthof
hos-pitalstay.Itwasfound thatthe painwasmoresevere on
thethirddayaftersurgery,withstatisticalsignificance
com-paredtothesecondday.Thismaybeduetotheincreased
levelofactivitiesorthetransitionfromintravenoustooral
analgesia,byproximitytodischarge.
The symptoms reported by patients could have an
impact on the time of getting out of bed. However,
it was not deemed necessary to make this
correla-tion. That is because when analyzing the results of all
groups it was noted that most patients tend to get out
of bed on pre-scheduled days, if they have no clinical
complications, which follows an institutional protocol for
eachsurgery,regardlessofPCAuse.Rehabilitationprotocols areincreasingly present inclinical practice,withthegoal
ofreducingfunctionalloss,inadditiontoshorten hospital
stay.24
Asanadditionalfindingofthestudy,itwasnoticedthat
patientswithhigherBMIwereoutofbedearliercompared
withthosewithlowerBMI(p=0.02).Thismaybeexplained
bythe presenceof other institutionalprotocol, indicating
thatpatients withBMI >25 areconsidered high-risk group
forthedevelopmentofrespiratoryfailurewhenrestricted
tobedforlongerthan48h.Thus,thereisadifferentiated carebytheteamtopreventrespiratorycomplicationsinthis groupofpatients.
Accordingtothelimitationsfoundinthiswork,itis
rec-ommendedthat futurestudies perform the analysis from
the early postoperative period. The control of analgesics
used,inadditiontoPCA,aswellastheapplicationofSNPat restandduringactivityperiodsmayalsocontributetomore concreteresults.
Conclusion
PCAprovedtobeusefulforpainreliefofpatientsundergoing
lumbarAVP. It wasalsoimportantfor patients undergoing
longAVP,whichmayhavereduceddeuseofsupplemental
O2,althoughnotstatisticallysignificantprobablyduetothe
smallsample size. The use of PCA did not correlate with
thetimeofgettingoutofbedandlengthofhospitalstayin eithergroupofpatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PianoLPA,GolmiaRP,ScheinbergM.Artroplastiatotaldequadril e joelho: aspectos clínicos na fase perioperatória.Einstein. 2010;8:350---3.
2.Krauss I, Steinhilber B, Haupt G, et al. Efficacy of conser-vativetreatment regimesfor hip osteoarthritis --- evaluation ofthetherapeutic exerciseregime‘‘HipSchool’’:aprotocol forarandomised,controlledtrial.BMCMusculoskeletDisord. 2011;12:270---82.
3.HootmanJM,HelmickCG,BradyTJ.Apublichealthapproach toaddressingarthritisinolderadults:themostcommoncause ofdisability.AmJPublicHealth.2012;102:426---33.
4.Leme EGL, Sitta MC, Toledo M, et al. Cirurgia ortopédica em idosos: aspectos clínicos. Rev Bras Ortop. 2011;46: 238---46.
5.Courtney MD, Edwards HE, Chang AM, et al. A randomised controlledtrial to prevent hospital readmissions and lossof functionalability inhigh riskolder adults:a studyprotocol. BMCHealthServRes.2011;11:202---9.
6.BarrosGAM, LemonicaL.Considerac¸õessobreanalgesia con-trolada pelo paciente em hospital universitário. Rev Bras Anestesiol.2003;53:69---82.
7.Fonseca NM, Ruzi RA, Ferreira FX, et al. Analgesia pós-operatóriaemcirurgiaortopédica:estudocomparativoentre obloqueiodoplexolombarporviaperivascularinguinal(3em 1)comropivacaínaeaanalgesiasubaracnóideacommorfina. RevBrasAnestesiol.2003;53:188---97.
8.Almeida MCS, Locks GF, Gomes HP, et al. Analgesia pós-operatória:comparac¸ãoentreinfusão contínuadeanestésico local e opioide via cateter peridural e infusão contínua de anestésico local via cateter na ferida operatória. Rev Bras Anestesiol.2011;61:298---303.
9.Nett MP. Postoperative pain management. Orthopedic. 2010;33:23---6.
10.PaulaGR,ReisVS,RibeiroFA,etal.Assistênciadeenfermagem edorempacientesortopédicosnarecuperac¸ãoanestésicano Brasil.RevistaDor.2011;12:265---9.
11.Lee HK, Lee JH, Chon SS,et al. The effectof transdermal scopolamineplusintravenousdexamethasoneforthe preven-tion of postoperative nausea and vomiting in patients with epiduralPCAaftermajororthopedicsurgery.Korean J Anes-thesiol.2010;58:50---5.
12.TaylorJM,GropperMA.Criticalcarechallengesinorthopedic surgerypatients.CritCareMed.2006;34:191---9.
13.Kauppila AM,Sintonen H, AronenP,et al. Economic evalua-tionofmultidisciplinaryrehabilitationafterprimarytotalknee arthroplasty based on a randomizedcontrolled trial. Arthrit CareRes.2011;63:335---41.
14.Walder B, Schafer M, Henzi I, et al. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain.ActaAnaesthesiolScand.2001;45:795---804.
15.StillerCO,LundbladH,WeidenhielmL,etal.Theadditionof tramadoltomorphineviapatient-controlledanalgesiadoesnot leadtobetterpost-operativepainreliefaftertotalknee arthro-plasty.ActaAnaesthesiolScand.2007;51:322---30.
16.Duarte LT, Fernandes MdoC, Costa VV, et al. Incidência de depressãorespiratórianopós-operatórioempacientes submeti-dosà analgesiavenosa ou peridural com opioides. RevBras Anestesiol.2009;59:409---20.
17.Kopka A, Wallace E, Reilly G, et al. Observational study of perioperative PtcCO2 and SpO2 in nonventilated patients
receivingepiduralinfusionorpatient-controlledanalgesiausing a single earlobe monitor (Tosca). Br J Anaesth. 2007;99: 567---71.
18.HuskissonEC.Measurementofpain.Lancet.1974;92:1127---31.
19.AndradeFA,PereiraLV,SousaFAEF.Mensurac¸ãodadornoidoso: umarevisão.RevLatino-AmEnfermagem.2006;14:271---6.
20.Pereira LV, Sousa FAEF. Mensurac¸ão e avaliac¸ão da dor pós-operatória: uma breve revisão. RevLatino-Am Enfermagem. 1998;6:77---84.
22.LimaJúniorPCde,LandimE,AvanziO,etal.Escolioseidiopática doadolescente (EIA):perfilclínico eradiográficodalistade esperaparatratamentocirúrgicoemhospitalterciáriodealta complexidade do Sistema Público de Saúde Brasileiro. Col-una/Columna.2011;10:111---5.
23.VialleLR,VialleEN,HenaoJES,etal.Hérniadiscallombar.Rev BrasOrtop.2010;45:17---22.