RevBrasAnestesiol.2015;65(4):240---243
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Use
of
sugammadex
on
burn
patients:
descriptive
study
Eduardo
Rodríguez
Sánchez
M.
∗,
Concepción
Martínez
Torres,
Pablo
Herrera
Calo,
Ignacio
Jiménez
AnesthesiologyandReanimation,HospitalesUniversitariosVirgendelRocío,Sevilla,Spain
Received13August2014;accepted8October2014 Availableonline7June2015
KEYWORDS
Sugammadex; Cyclodextrin; Burninjury; Rocuronium;
Neuromuscularblock; Neostigmine
Abstract
Objectives:Aburnpatientisachallengeforanyanesthesiologist,undergoingseveralsurgeries duringadmission,andrequiringgeneralanesthesiaandmusclerelaxationmostofthetimes. Thevictimmayhaverespiratorysystemimpairmentandaresponsetomusclerelaxantsthat differsfromthehealthypatient,thuspropermonitoringandreversaliscrucial.Weanalyzed sugammadexeffectivenessandsafetyinthispopulation.
Materialsandmethods: Itwasaprospectivelydescriptivestudy,including4patients,andall ofthemwereconsideredmajorburnpatients,whounderwentescharotomywithgeneral anes-thesiaandneuromuscularrelaxation.Themainvariablewasthetimefor recoveryofaTOF higherthan0.9aftertheadministrationofsugammadexbeforeextubation.
Results:MeantimeofrecoveryfromaTOFratiohigherthan0.9followingtheadministration ofSugammadexwasof4.95min95%CI(3.25---6.64,p=.53).
Conclusions:Thereversionofneuromuscularrelaxationwithsugammadexappearstobe effec-tiveandsafeintheburnpatient.Moreanalytical,comparativestudiesoflargerpopulations wouldbenecessarytoconfirmthesedata.
©2015SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Sugammadex; Gama-Ciclodextrinas; Queimaduras; Rocurônio; Bloqueio neuromuscular; Neostigmina
Usodesugamadexnopacientequeimado:estudodescritivo
Resumo
Objetivos: Opacientequeimadorepresentaumdesafioparaoanestesiologista,pois submete-seaváriasintervenc¸õescirúrgicasdurantesuahospitalizac¸ão,necessitandodeanestesiageral erelaxamentomuscularnamaiorpartedelas.Apresentasistemarespiratóriocomprometido eumarespostaaosrelaxantesmuscularesquediferedopacientesadio;portanto,um moni-toramentocorretoereversãotornam-seimprescindíveis.Avaliamosaeficáciaeseguranc¸ado sugamadexnestapopulac¸ão.
∗Correspondingauthor.
E-mail:[email protected](E.RodríguezSánchezM.).
http://dx.doi.org/10.1016/j.bjane.2014.10.001
Sugammadexinthemajorburnpatient:descriptivestudy 241
Materialemétodos: Estudodescritivocomcaráter prospectivoque incluiquatro pacientes, todoselesconsideradosgrandesqueimados,submetidosaescarectomiacomanestesiagerale relaxamentoneuromuscular.Comovariávelprincipaltomou-seotempoderecuperac¸ãodeTOF superiora0,9apósaadministrac¸ãodesugamadexantesdeextubac¸ão.
Resultados: O tempo médio de recuperac¸ão de uma razão TOF superior a 0,9 após a administrac¸ãodesugamadexfoide4,95min(IC95%3,25-6,64;p=0,53).
Conclusões: A reversãodo relaxamentoneuromuscular comsugamadex parece sereficaz e seguranopacientequeimado.Seriamnecessáriosmaisestudosanalíticos,comparativosede maiorpopulac¸ãoparaconfirmaressesdados.
©2015SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Burnsaretissueinjuriesproduced byskinaggression from anysourceofenergy.Theseveritycriteriawouldbe involve-ment of more than 25% of totalbody surface, burns that follow inhalation syndrome, involvement of face, eyes, hands,feetandperineum.1Mortalityofmajorburnpatients is approximately13.9%.2,3 In our unit, 174 patients were attendedintheyearof2012.Thesepatientsunderwent sev-eralsurgicalinterventionsduringtheirstayinthehospital, withmost of them under general anesthesia, orotracheal intubation,andneuromuscularrelaxation.
Sugammadexisamodifiedcyclodextrinusedforreversion of rocuronium- and vecuronium-induced nondepolarizing muscle block.4,5 The dose of sugammadex varies depend-ingonthelevel ofmusclerelaxation,withmeantimefor recoveryof aTOFratiohigherthan 0.9of3min.(min).6,7 Several studies demonstrated the superiority of this drug comparedtoneostigmine8---10 regardingsafetyandtimefor recovery.Itwassuccessfullyusedinthe obesepatient,in the elderly, and also in children older than two years.11 However,its use in the major burn patienthad not been studied.Themainobjectiveofthisworkwastoanalyzethe efficacyofsugammadexinthispatientprofileinwhomthe metabolic-hemodynamicchanges mayalterits pharmacol-ogyandinwhom,duetorespiratorysysteminvolvement(if constant),anappropriatereversalofneuromuscular block-ersiscrucial.Secondaryobjectivesarethemeasurementof neuromuscularrelaxation recovery timeafterits adminis-tration,thecomparisonoftheseresultswiththoseexisting in the literaturein other types of patients, report of the emergenceofadverseeffectsrelatedtoitsadministration, andreportofmainanestheticconsiderationsofmajorburn patient.
Materials
and
methods
Aprospectivedescriptivestudyoffourcaseswasconducted overtwomonths.Inclusioncriteriawereasfollows:major burn patient who underwent escharotomy under general anesthesia and orotracheal intubation. Exclusion criteria were: allergy to sugammadex, severe renal impairment
(creatinine clearance below 30mLmin−1, intraoperative
hemodynamicinstabilityrequiringadministrationofamines, or the need for blood transfusions. All patients were monitoredwithelectrocardiogram,oxygensaturation, non-invasive blood pressure and monitoring of neuromuscular blockadebyaccelerometry(TOFwatch).Inductionwas con-ductedwithpropofol(2.5mgkg−1),fentanyl(2gkg−1)and
rocuronium(0.6mgkg−1).Maintenancewasperformedwith
sevofluraneat1CAM,withtheadministrationofabooster doseofrelaxant(30%theinitialdose)onthosewhoshowed recoveryfromblock(emergenceof2responsesinTOF).At theendofthesurgery,andbeforeextubation,sugammadex wasadministeredin allcases,withthe dose according to thelevelneuromuscularblock(deepblock4mgkg−1,
moder-ateblock2mgkg−1,recoveryphasewith4responsestoTOF
ratio1mgkg−1).Thepatientswereextubatedafterrecovery
ofTOF higherthan0.9.The variableconsidered wastime in minutes since the administration of sugammadexuntil recoveryofTOFhigherthan0.9.Allthetimewefollowedthe ethicalstandardsofthehumanexperimentationcommittee ofourcenter.Fordataanalysis,weusedthesoftwareIBM SPSSStatistics22.0.
Results
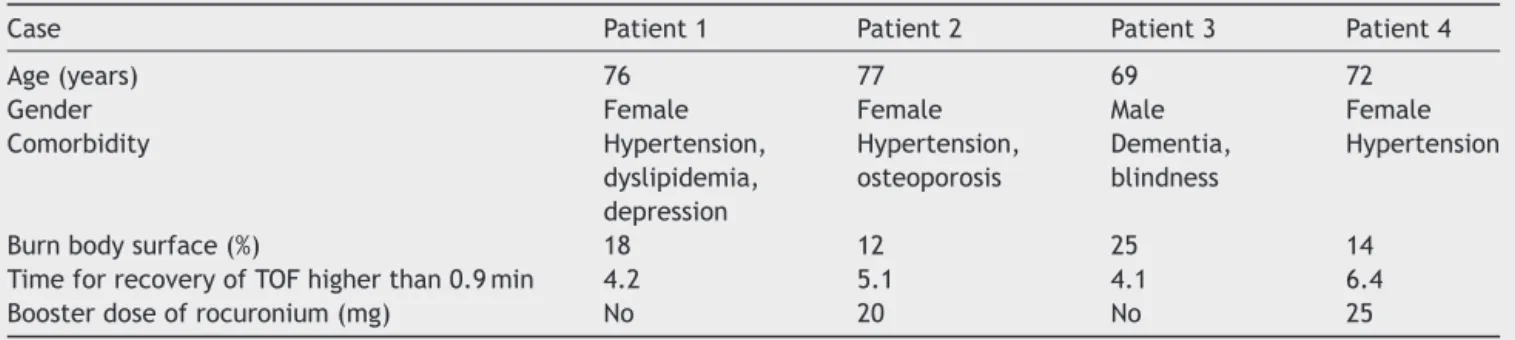
Four patients with ages between 69 and 76 years were included. The clinical characteristics of the patients are summarizedinTable1,andFig.1showsoneofthepatients includedinthestudy.Theaveragepercentageofbody sur-faceareaburnedwas17.25%.Twoofthepatientsreceived aboosterdoseofrocuronium(20and25mgrespectively). The averagerecovery timefrom aTOF ratiogreater than 0.9 after sugammadex administration before extubation was4.95min witha 95% confidence intervalof 3.25---6.64 (p=0.53).Themedianofthesamevariablewasof4.65min. Typicaldeviationwasof1.06.
Discussion
242 E.RodríguezSánchezM.etal.
Table1 Patients’clinicalcharacteristics.
Case Patient1 Patient2 Patient3 Patient4
Age(years) 76 77 69 72
Gender Female Female Male Female
Comorbidity Hypertension,
dyslipidemia, depression
Hypertension, osteoporosis
Dementia, blindness
Hypertension
Burnbodysurface(%) 18 12 25 14
TimeforrecoveryofTOFhigherthan0.9min 4.2 5.1 4.1 6.4
Boosterdoseofrocuronium(mg) No 20 No 25
lung capillaries,12 and therefore thecontrol of lung func-tionshallbeourpriority.Insevere burnpatients,thereis aproliferationofimmatureacetylcholinereceptorsonboth neuromuscularplateandextra-synapticsites.Thisleadsto anincreasedsensitivitytodepolarizingrelaxants (succinyl-choline),withriskofseverehyperkalemiaandaresistance tonon-depolarizingneuromuscularblockingagents, increas-inginstaurationlatency,andreducingthetimeofaction13; this,alongwithapossiblerenalimpairmentmayresultin itsaccumulationafterreadministration,withriskofresidual curarization.Theuseofmusclerelaxationreversionagents, anditsmonitoringareeffectivemeasurestoprevent pare-sis;thepresenceofTOFratiogreaterthan0.9isconsidered safetoperformextubation.14 Theanticholinesterasedrugs (neostigmine,edrophonium)areroutinelyusedforreversal ofneuromuscular relaxationin burn patients; thesedrugs produceadverseeffectsderivedfromtheincreaseof acetyl-cholineanditsinteractionwithmuscarinicreceptorsoutof intersynapticsite.Theaverage timetoreacha TOFvalue higherthan0.9afterthereappearanceofthe2responses toTOFisof18.5minafterneostigmineadministration.15Itis shownineffectivetoreversedeepblock.Theemergenceof sugammadexassumedtobearevolutioninthisregard,but ithasnotbeenstudiedinburnpatients,withamorerapid andpredictablebeginningofactionbeingdemonstratedin severalstudies,comparedtoneostigmine,andbeing effec-tive in a deep block.8---11 In our study the mean time to recoveryof TOF ratiogreater than 0.9after sugammadex
Figure1 Apatientincludedinthestudy.
administrationwas4.95min, timethat is lowerthan that of neostigminein other populations.None ofthe patients showedcomplicationsrelatedtotheadministrationof sug-ammadex. These data, although preliminary, have shown thatsugammadexcanbeusedinthesepatients,with recov-erytimesformuscleactivitysimilartothatinother types ofpatients.Moreprospectivecomparativeanalytical stud-ieswithmorepatientsarenecessarytoconfirmtheresults ofthiswork.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LatenserBA.Criticalcareoftheburnpatient:thefirst48hours. CritCareMed.2009;37:2819---26.
2.SteinvallI,FredriksonM,BakZ,etal.Mortalityafterthermal injury:nosex-relateddifference.JTrauma.2011;70:959---64. 3.BrusselaersN,MonstreyS,VogelaersD,etal.Severeburninjury
inEurope:asystematicreviewoftheincidence,etiology, mor-bidity,andmortality.CritCare.2010;14:R188.
4.ZhangMQ.Drug-specificcyclodextrins:thefutureofrapid neu-romuscularblockreversal?DrugsFuture.2003;99:632---7. 5.BomA,BradleyM,CameronK,etal.Anovelconceptof
revers-ingneuromuscularblock:chemicalencapsulationofrocuronium bromidebyacyclodextrin-basedsynthetichost.AngewChem IntEdEngl.2002;41:266---70.
6.DuvldestinP,KuizengaK,SaldienV,etal.Arandomized, dose-responsestudyofsugammadexgivenforthereversalofdeep rocuronium- or vecuronium induced neuromuscular blockade undersevofluraneanesthesia.AnesthAnalg.2010;110:74---82. 7.SuyK,MoriasK, CammuG, etal.Effective reversalof
mod-eraterocuroniumorvecuronium-inducedneuromuscularblock whitsugammadex,aselectiverelaxantbindingagent. Anesthe-siology.2007;106:283---8.
8.Jones RK, Caldwell F E, Brull SJ, et al. Reversal of profound rocuronium-induced blockade at extubation: a randomized comparison whit neostigmine. Anesthesiology. 2008;109:816---24.
9.Khuenl-BradyKS,WattwilM,VanackerBF,etal.Sugammadex providesfasterreversalofvecuronium-inducedneuromuscular blockadecomparedwithneostigmine:amulticenter, random-ized,controlledtrial.AnesthAnalg.2010;110:64---73.
Sugammadexinthemajorburnpatient:descriptivestudy 243
11.Plaud B, Meretoja O, Hofmockel R, et al. Reversal of rocuronium-inducedneuromuscularblockadewithsugammadex in pediatric and adult surgical patients. Anesthesiology. 2009;110:284---94.
12.CantalE,GouturbeP,AsencioY,etal.Reanimationetanesthesie dubrulel´adulte.Paris:EMC;2008.
13.GascaPJD.Anestesiaenelpacientequemado.RevMexAnest. 2013;36:327---30.
14.Plaud B, Debaene B, Donati F, et al. Residual paraly-sis after emergence from anesthesia. Anesthesiology. 2010;112:1013---22.