w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Special
article
Proposal
for
the
standardization
of
flow
cytometry
protocols
to
detect
minimal
residual
disease
in
acute
lymphoblastic
leukemia
Maura
Rosane
Valério
Ikoma
a,∗,
Miriam
Perlingeiro
Beltrame
b,
Silvia
Inês
Alejandra
Cordoba
Pires
Ferreira
c,
Elizabeth
Xisto
Souto
d,
Mariester
Malvezzi
b,
Mihoko
Yamamoto
e,
on
behalf
of
Minimal
Residual
Disease
Working
Group
of
the
Brazilian
Society
of
Bone
Marrow
Transplantation
(SBTMO)
1aFundac¸ãoAmaralCarvalho(FAC),Jaú,SP,Brazil
bUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
cCentrodeHematologiaeHemoterapiadeSantaCatarina(HEMOSC),Florianópolis,SC,Brazil dDiagnósticosdaAmérica(DASA),SãoPaulo,SP,Brazil
eUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received3May2015 Accepted27July2015
Availableonline28September2015
Keywords:
Minimalresidualdisease
MRDacutelymphoblasticleukemia Flowcytometry
Immunophenotyping
a
b
s
t
r
a
c
t
Minimalresidualdiseaseisthemostpowerfulpredictorofoutcomeinacuteleukemiaandis usefulintherapeuticstratificationforacutelymphoblasticleukemiaprotocols.Nowadays, themostreliablemethodsforstudyingminimalresidualdiseaseinacutelymphoblastic leukemiaaremultiparametricflowcytometryandpolymerasechainreaction.Bothprovide similarresultsataminimalresidualdiseaselevelof0.01%ofnormalcells,thatis, detec-tionofone leukemiccellinupto10,000normalnucleated cells.Currently, therapeutic protocolsestablishthe minimalresidual diseasethresholdvalueat themost informa-tivetimepointsaccordingtotheappropriatemethodologyemployed.Theexpertiseofthe laboratoryinacancercenteroracooperativegroupcouldbethemostimportantfactor indeterminingwhichmethodshouldbeused.InBrazil,multiparametricflowcytometry laboratoriesareavailableinmostleukemiatreatmentcenters,butmultiparametricflow cytometryprocessesmustbestandardizedforminimalresidualdiseaseinvestigationsin ordertoofferreliableandreproducibleresultsthatensurequalityintheclinicalapplication ofthemethod.TheMinimalResidualDiseaseWorkingGroupoftheBrazilianSocietyofBone MarrowTransplantation(SBTMO)wascreatedwiththataim.Thispaperpresents recom-mendationsforthedetectionofminimalresidualdiseaseinacutelymphoblasticleukemia basedontheliteratureandexpertiseofthelaboratorieswhoparticipatedinthisconsensus, includingpre-analyticalandanalyticalmethods.Thispaperalsorecommendsthatboth
∗ Correspondingauthorat:Fundac¸ãoAmaralCarvalho(FAC),RuadasPalmeiras,106,17210-120Jau,SP,Brazil. E-mailaddress:[email protected](M.R.V.Ikoma).
1 MembersofMRDWorkingGroupofSBTMOarelistedinAppendix.
http://dx.doi.org/10.1016/j.bjhh.2015.07.012
multiparametricflowcytometryandpolymerasechainreactionarecomplementary meth-ods,andsomorelaboratorieswithexpertiseinimmunoglobulin/Tcellreceptor(Ig/TCR)gene assaysarenecessaryinBrazil.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Publishedby ElsevierEditoraLtda.Allrightsreserved.
Introduction
Minimalresidualdisease(MRD)istodayconsideredthemost powerful predictor ofoutcome inacute leukemias, includ-ing acutelymphoblastic leukemia (ALL). Althoughclassical factorssuchasage,cytogeneticandmolecularfeatures,and leukocytecountaretakenintoaccounttoestablishtheinitial riskgroupsfortherapeuticpurposes,theevaluationof treat-mentresponsebyMRDdetectionallowsclinicianstoidentify relapseriskcategoriesforALLandstratifythechemotherapy accordingtowell-establishedadultor pediatrictherapeutic protocols.1–7ResultsofMRDstudiescanalsobeusedtoselect treatmentintensityandduration,andestimatetheoptimal timingforhematopoieticstemcelltransplantation(HSCT)in childhoodALL.8
Bothmultiparametricflowcytometry(MFC)andthe ampli-fication of immunoglobulin/T cell receptor (Ig/TCR) genes by polymerasechainreaction(PCR)havesimilarresultsinMRD detectionwitha levelof10−4 cells.Howeverthe besttime pointsfordetectionaredifferentbetweenthetwotechniques.
Clinicalsignificanceofminimalresidualdiseaselevels
ThegoalsofMRDstudiesforclinicalpurposesaretoestablish: (i)thelevelsofMRDthatarerelevanttothetherapeutic deci-sion;(ii)themostinformativetimepointsduringtreatment; and(iii)theclinicalrelevanceofinformationthateachmethod providesatthedifferenttimepoints.
Thecut-off valueto define ALL MRDpositivity is0.01% or10−4 cells,becausethisrepresentsthe limitofdetection
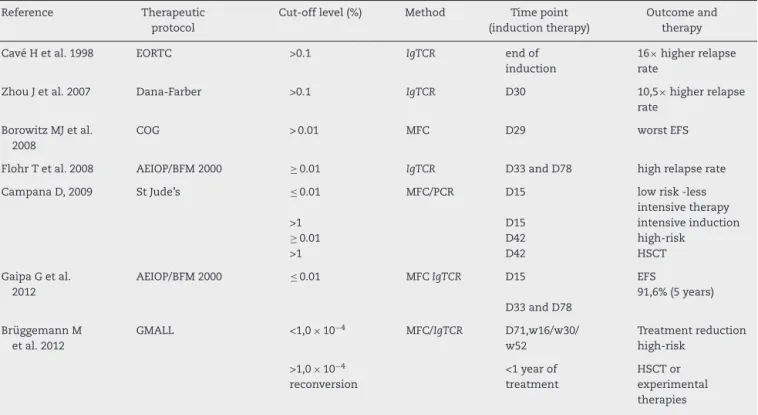
byimmunophenotypingandmolecularassays,althoughitis possibleto achieve ahigher sensitivity (betterthan 0.01%) byPCRtechniques.Moreover,withtherecentimprovements intechnology, this thresholdcan nowbe achievedbyflow cytometry.8,9Currently,therapeuticprotocolsestablisha cut-offpointatthemostinformativetimetopredictdangerof relapseaccordingtotheappropriatemethodologyemployed forMRDdetection(Table1).
The identification of the disease relapse risk allows therapeutic stratification and better clinical management, includingrecognitionofpatientswhorequirelessintensive therapyandthoseeligibleforHSCTatfirstremission.5,10
The level of MRD in pediatric patients prior to condi-tioning for allogeneic HSCT has a significant impact on post-transplantoutcomesanditisthemostimportant pre-dictorofrelapseafterHSCT.Patientswithhigh-levelMRDat thetimeoftransplant(>10−3 or0.1%malignantcells) have
significantlypoorer outcomes than those who entered the transplantationwithnegativeMRD(<10−3cells).11TheAcute
LymphoblasticLeukemiaBerlin-Frankfurt-MünsterStemCell Transplantation Group (ALL-BFM-SCT) 2003 trial assessed MRDinthe bonemarrow(BM) atDays30,60,90,180, and 365 after HSCT and each time point with a MRD ≥10−4 leukemiccellswasconsistentlycorrelatedwithshorterevent freesurvival.12
Two techniques are available for post-transplant mon-itoring of disease remission: MRD detection and the characterization of post-transplant chimerism. The MRD detection techniquessearchforthe malignantclone,while assessments ofchimerism characterize the origin of post-transplanthematopoiesis.11Thesensitivityofinvestigations ofchimerismvarygreatlydependingonthemethodused.13
PatientswithalowMRDlevelafterHSCT(<10−3),can
con-vertmixedchimerismtocompletechimerismbypre-emptive immunotherapy,11,14,15 whichdemonstrates theimportance ofMRDmonitoringafterHSCT.Althoughthereisnota well-establishedmanagementscheduleforthesecases,MRDstatus providesarealperspectiveofrationaltherapeuticintervention afterHSCTtopreventrecurrenceofthedisease.14
Methodsofminimalresidualdiseasedetection
ThemostreliablemethodsofevaluatingMRDareMFCanalysis withtheidentificationofleukemia-associated immunophe-notypes(LAIPs)andamplifyingantigen-receptor(Ig/TCR)gene rearrangementsandfusiontranscriptsbyPCR.BothMFCand amplificationofIg/TCRgenesbyPCRprovidesimilarresultsat aMRDlevelof0.01%,5,16andbothMFCandPCRhave advan-tagesand disadvantages. MFCisarapidmethod, usefulin >95%ofALLcasesandismoreinformativethanPCRduring thefirstphaseofinductiontherapy,whilePCRispreferablefor studiesafterHSCTorattheendoftherapybecauseofitshigh sensitivityinthosemoments.10,17Duringthefirst2–3weeks ofremission-inductiontherapy, BMspecimensdo not con-tainlymphoidprogenitors,andsothedetectionofimmature B-cellsbyMFCcanbeanindicationofresidualdisease.17
ThemostimportantcausesofdiscrepancybetweenMFC andPCRassaysare:(i)samplescontainingalimitedcell num-berforMFCassays;(ii)phenotypevariationsofregenerating precursor B-cells(PBC)inBMduringtherapyandrelatedto age; (iii) druginduced antigenic modulation;(iv) qualityof PCRclonalmarkers;(v)amplificationofnonspecificDNAfrom deadcells;and(vi)oligoclonalityandclonalevolution.6,18–20
Table1–ClinicalsignificanceofMRD,cut-offlevelsandtimepointsofdetectionduringinductiontherapyinacute lymphoblasticleukemia.
Reference Therapeutic
protocol
Cut-offlevel(%) Method Timepoint
(inductiontherapy)
Outcomeand therapy
CavéHetal.1998 EORTC >0.1 IgTCR endof
induction
16×higherrelapse
rate
ZhouJetal.2007 Dana-Farber >0.1 IgTCR D30 10,5×higherrelapse
rate
BorowitzMJetal. 2008
COG >0.01 MFC D29 worstEFS
FlohrTetal.2008 AEIOP/BFM2000 ≥0.01 IgTCR D33andD78 highrelapserate
CampanaD,2009 StJude’s ≤0.01
>1
≥0.01 >1
MFC/PCR D15
D15 D42 D42
lowrisk-less intensivetherapy intensiveinduction high-risk
HSCT
GaipaGetal. 2012
AEIOP/BFM2000 ≤0.01 MFCIgTCR D15
D33andD78
EFS
91,6%(5years)
BrüggemannM etal.2012
GMALL <1,0×10−4 MFC/IgTCR D71,w16/w30/
w52
Treatmentreduction high-risk
>1,0×10−4
reconversion
<1yearof treatment
HSCTor experimental therapies
MRD,minimalresidualdisease;MFC,multiparametricflowcytometry;Ig,immunoglobulin;TCR,T-cellreceptor;PCR,polymerasechainreaction; EFS,eventfreesurvival;HSCT,hematopoieticstemcelltransplantation.
PCRtargets21;and(iv)therearesubcloneswithdistinctclonal
Ig/TCR generearrangementsthatareundetectedat diagno-sis and that may become predominant during the course ofthe disease(oligoclonality).22 Becauseofthese disadvan-tages,manylaboratoriestrytouseMFCforMRDdetection,21 althoughnewapproachesofsequencingtechnologiesareof greatpotentialforfacilitatingmolecularMRDstudiesinALL andmaywellsupplantthecurrentmethod.23
Immunophenotyping
Detection ofMRD by MFC consists ofsearching for LAIPs, also called aberrant phenotypes, that are absent in nor-mal,reactiveorregeneratingBMandperipheralbloodcells; this is useful to discriminate neoplastic cells from nor-mal hematopoietic cells. LAIPs include the presence of cross-lineageantigenexpression(e.g.expressionofmyeloid antigensinALLcases),asynchronouspatternsofexpressionof maturationmarkers(e.g.surfaceIgexpressiononCD34+cells)
andabnormallevelsofexpressionofindividualmarkers(e.g. antigenoverexpressionorunderexpression).LAIPsare identi-fiedinmorethan95%ofALLcases.5,17Thus,MFCcanbeused tomonitor90–95%ofMRDinALLcasesduringtherapeutic management.ImportantlyMRDcanbeusedwithPBsamples inpatientswithTcellALLgivingsimilarresultstotheuseof MRDtestinginBM.HoweverinpatientswithB-lineageALL, MRDisusuallypresentathigherlevelsinBMthaninPB;8BM ispreferableforMRDdetectioninthissituation.
Thesensitivityofthismethodvariesaccordingtothe num-berofMFCcolorsappliedinMRDassays:10−3to10−4MRDcells
with3–4colorsand10−4to10−5with>6colors.9Newwaysof samplepreparationsuchasbulklysis24,25andimprovements in analysis strategies can also contribute to increase MFC sensitivity.9Althoughtheseimprovementscanbeachievedin MRDdetection,severalstudiesdemonstratedthatMRD mon-itoringbyfour-colorMFCcanstillbeclinicallyinformative.3,26 Theprincipaladvantagesofimmunophenotypingare:(i) the possibility ofevaluatingthe samplecellularity and the degree of hemodilution; (ii) the maturation of normal BM cells,includinglymphoidrecoveryafterimmunosuppressive therapy;(iii)thespeedofobtainingresults;and(iv)its wide-rangingapplicability.
The limitations ofimmunophenotyping in MRD studies are:(i)thelownumberofcellsavailable;(ii)thesimilarityof theimmunophenotypebetweennormalprecursor cellsand leukemiacellshinderstheidentificationofresidualblastcells; (iii)themodulationofantigenexpressionduringtreatment18; (iv)thenecessityofhighexpertisetoperformMRDassays;and (v) thelackofinter-laboratorialstandardizationandquality control.
Immunophenotypic modulation, described in ALL patients,5,19,27interferesintheabilitytoaccuratelydetermine
MRD(Table2).SomemodulationsofBcellantigenexpressions
Table2–Commonmodulationofantigenexpression duringacutelymphoblasticleukemiatreatment.
BprecursorcellALL TcellALL
Inductiontherapy(untilDay33) Down-modulationofCD10and CD34
Up-modulationofCD19,CD20, CD45RAandCD11a
Induction therapy Down-modulationof TdT,CD99,CD34 andCD10 AtDay78ofinduction
ReversionofCD10andCD34to initialexpression
therapy, thereis areversionofCD10 and CD34expression
to initial levels and the CD58 expression stablizes.18,19,28 Significantchangesinforward-anglelightscatter(FSC)and side angle light scatter (SSC) signals associatedwith blast cellsatdiagnosisandatDay15arenotobserved.18
Roshaletal.alsodescribeddown-modulationof immatu-ritymarkerssuchasTdT,CD99,CD34andCD10inT-ALLcells duringinductiontherapy.Theydidnotobserveintensity vari-ationsinCD2,CD3,CD4,CD5,CD7,andCD8,andCD45showed aslightgaininmeanfluorescenceintensitycomparedto nor-malTcells.27
Furthermore immunophenotypic changes have been reportedinrelapsedacuteleukemiabyclonalselectionor lin-eageswitch.26ThechangesinLAIPscanaffecttheaccuracy oftheflowcytometricdetectionofMRDrenderingfalse neg-ativeresults.Theuse ofmultiplemarkercombinationscan minimizefalsenegativeresultssuggestingthat thisshould beastrategyforMRDdetectionbyimmunologicalmethods. Thus,theuseofnewmarkersforoverexpressedor underex-pressedPBCALL comparedtonormal PBCincludingCD24, CD44,CD49f, CD69,CD72,CD73,CD79b,CD86,CD97,CD99, CD102,CD123,CD130,CD164,CD200,CD300a,CD304,BCL2, HSPB1,PBX1,CTNNA1, and ITGB7ispromising toimprove sensitivityofimmunophenotypeMRDstudies.29Inaddition, someofthesemarkersareassociatedtogenetic abnormali-ties,andhavebeenprovedtobestableaftertreatment.29
Detectionofminimalresidualdiseaseinacute lymphoblasticleukemiabymultiparametricflow cytometry–aproposalofstandardization
MFCandamplificationofIg/TCRgenesbyPCRhavesimilar resultsataMRDlevelgreaterthan0.01%cells6,30butthe intro-ductionofMFCwithsixormorecolors,thestandardization ofinstrumentsettingsandimmunophenotypingprotocols,24 theavailabilityofarobustsinglemulticolorantibody combi-nation,andnovel dataanalysisstrategies,9 maycontribute toimprove thepotentialofMFCinthediagnosisofMRD.21 Thetypeoflaboratoryexpertiseavailabletoacancercenter oracooperativegroupcouldbethemostimportantfactorin determiningwhichmethodshouldbeused.8
InBrazil,asinother countries,thereareflowcytometry laboratoriesinmostleukemiatreatmentcenters,makingthis methodmorereadilyavailable.
TheMRDWorkingGroupoftheSBTMOwascreatedwith theaimofstandardizingMFCforMRDinvestigationsandto
offerreliableandreproducibleresultsthatensurequalityin clinicalapplicationandpatientcare.
Methods
InitiallyallmembersoftheWorkingGroupreviewedthe lit-eraturedata;theyalsoevaluated20list-modeofnormaland regeneratingBMofadultandpediatricsampleswhichwere providedbyeightparticipatingcentersandavailableonline.
TheproposalstostandardizeMFCpresentedinthisarticle arebasedonreporteddataandrelevantinformationcollected fromtheexpertiseoftheparticipatingcenters.Theyinclude: (i) protocols forsamplepreparation and staining, (ii) stan-dardizationofmonoclonalantibodies(MoAbs)andrespective fluorochromes, combined in four-color marker panels, (iii) standardizationofMFCacquisitionprotocolsand(iv)quality controlissues.
According to the Brazilian Group of Flow Cytometry (GBCFLUX)data, mostBrazilian MFClaboratoriesare today equippedwithcytometerswiththreeandfourfluorescence sets.Recently,GBCFLUXpublisheddiagnosticpanelsforacute leukemiarecommendedtomostBrazilianMFClaboratories.31 ThenextstepswillbetotrainWorkingGroupmembers tosupportthe standardizationprocess andevaluate repro-ducibility through online interchange of MFC data files to analyzeMRDcasesasagroup.Dataanalysisisnotthegoal ofthisworkandshouldbeaddressedinafuturepaper.
Minimalresidualdiseaseworkinggrouprecommendations
Generalrecommendations
Cell morphologyshouldbeassessedvisually using conven-tional optical microscopy. Smears of samples collected in tubescontainingethylenediaminetetraaceticacid(EDTA)are alsoanalyzedtoestimatethehemodilutionparameter.The smearsareinternalcontrolsofthelaboratorytoverifythe cel-lularityofthesampletobeprocessed.Nonetheless,ethically, allsamplesmustbeprocessed,includinghemodiluted sam-ples.BM(1–2mL)orPBsamplesmustbecollectedinK3EDTA (7.5%)forbothMFCandacompletebloodcount.Thestorage ofsamplesshouldnotexceed24haftercollection(Table3).
Recommendationforsamplepreparation
Most laboratories of the MRD Working Group that use MFC prepare samples by the conventional stain-and-then-lyse technique or bulk lysis and stain.25 One laboratory uses mononuclearcells separatedusingthe Ficoll-Hypaque method5accordingtorequirementsofthespecifictreatment protocol.
For theconventional technique,freshBMor PBsamples contain106cells,10–100Lwhite bloodcellsmustbe
Table3–Summaryoftechnicalproceedings.
Generalrecommendations
Cellmorphologyofcorrespondingsample
Evaluationofsamplecellularity/hemodilutionassessedby smearsfromethylenediaminetetraaceticacid(EDTA)tube Bonemarrow(1–2mL)orperipheralbloodsamplesmustbe collectedinK3EDTA7.5%forbothmultiparametricflow cytometryandcompletebloodcount
Theincubationofsamplesshouldnotexceed24hafter collection
Recommendationforsamplepreparation
Stain-and-then-lysetechniqueorbulkylysisandstain Samplesincubatedfor15minatroomtemperatureinthedark withfluorochromeconjugatedmonoclonalantibodies Lyseofnon-nucleatedredcellswithlysingsolution CentrifugeandwashtwicewithPBSor0.2%PBS–BSAor0.2% PBS+BSAplus0.1%sodiumazide
Re-suspendin300–500LofPBSformultiparametricflow
cytometryacquisitionandanalysis
Intracellularstainingmustbeperformedafterstainingforcell surfacemembranemarkers,utilizingpermeabilizingsolutions
Standardoperationalprocedures
Dailycleaningandbeadcalibrationprocedures Compensationmustbedonemonthlyorwhenrequired, accordingtothestabilityofflowcytometerparameters Routinepreventivemaintenancemustbeperformedatleast everysixmonths
PBS:phosphatebuffersolution;BSA:bovineserumalbumin.
Non-nucleatedredcellscanbelysedusingFACSLysing solu-tion(Becton-DickinsonBiosciences-BDBTM,SanJose,CA,USA)
orExcellyseEasy(ExbioTM,Vestec,Czech Republic),
accord-ingtothe manufacturer’sinstructions. Theremainingcells aresequentiallycentrifuged (500g)for5min,washed twice inphosphate bufferedsaline(PBS:pH7.4)or PBSplus0.2% bovineserumalbumin(BSA:pH7.4)orPBSplus0.2%BSAplus
0.1%sodiumazide:pH7.4)andre-suspendedin300–500L
inPBSforMFCacquisitionandanalysis.Intracellularstaining forCD3andTdTisperformedafterstainingforcellsurface membranemarkersusing Fix&Permsolution(InvitrogenTM,
Camarillo, CA, USA or An Der GrubTM, Vienna, Austria) or
theIntraStainkit(DakoTM,Carpinteria,CA,USA)asperthe
instructions ofthe manufacturer.The recommended
solu-tionshavebeentested,appliedandselectedforuseinmost ofthelaboratoriesoftheWorkingGroup.
Standardoperationalprocedures
Daily cleaning and calibration ofbead procedures are
rec-ommendedandcompensationshouldbedoneeverymonth
or when required according to stability of flow cytometer
parameters. Flowcytometerperformancemust be checked
everydayoraccordingtothe manufacturer’s
recommenda-tionstoensurethatthe evaluationofsamplesalwaysuses
the same parameters and enable an accurate analysis of
theunderexpressionandoverexpressionofmarkerswhichis veryimportantforMRDdetection.Routinepreventive main-tenancemustbeperformedperiodically,thatis,atleastevery sixmonths(Table3).
Table4–Fluorochromeconjugatedantibodypanelsused forminimalresidualdiseasedetectioninBprecursor cell-acutelymphoblasticleukemiabymultiparametric flowcytometry.
Mandatorypanel
Tube1–CD20FITC/CD10PE/CD19PerCPorPEcy5.5/CD34APC Tube2–CD45FITC/CD34PE/CD19PerCPorPEcy5.5/CD38APC Tube3–nTdTFITC/CD10PE/CD19PercporPEcy5.5/CD34APC
Recommendedtubesa
Tube4–CD81FITC/CD66cPE/CD19PerCPorPEcy5.5/CD34APC Tube5–CD45FITC/CD123PE/CD19PerCPorPEcy5.5/CD34APC Tube6–CD15FITCandCD65FITC/NG2PE/CD45PerCP/CD19APC
Optionalmarkersa
CD13and/orCD33PE,CD58FITC,CD9FITC/CD25PE,CD22PE
n:nuclearstaining.
a Accordingtoantigenexpressionatdiagnosis.
Fluorochromeselectionforfour-colorpanels
Theselectionofthemostappropriatecombination of fluo-rochromesforfour-colorpanelsshouldallowsimultaneous usageofbackbonemarkersaimedattheidentificationofthe cellpopulationsofinterestandadditionalantibodymarkers devotedtoamoredetailedcharacterizationoftheleukemic cell populationssuchas maturationmarkers, cross-lineage markers,and markersassociatedwithmolecularlesions.A combination of FITC, PE, PerCP or PECy5.5 and APC were selectedbasedontheliteratureandtheexpertiseofthe Work-ingGroup.
ImmunophenotypicabnormalitiesofleukemicBcell popu-lationsareidentifiedbythedeviationfromnormalpatterns ofB-lymphoiddevelopment9.PBCorhematogoneshave mor-phologic and immunophenotypic similarities to neoplastic lymphoblasts.PBCmaybepresentinlargenumbersinmany situations as early as infancy, or in a variety of diseases both in childhood and in adult life, as in some autoim-mune and congenital cytopenias,neoplasms and acquired immunodeficiency syndrome (AIDS).32 Hematogones also maybeparticularlyprominentinregeneratingBMfollowing chemotherapy or HSCT (Figure 1).32–35 Particularly follow-ing ALLtreatment,hematogonesare oftenexpandedinBM and canpotentiallybemistakenforresidual disease.Some studiesshowedthatthePBCpopulationalwaysexpressesa continuousandcompletematurationspectrumbyfour-color flow cytometry.36 In contrast, casesof PBC ALL frequently show adifferentspectrumtonormalB-lineagematuration. Thesedifferencesinclude:maturationarrest;overexpression, underexpression,and asynchronous expressionofantigens observed in PBC and often the expression of myeloid-associatedantigens.33,37
AccordingtothisMRDWorkingGroupconsensus,residual B-cellALLmustbeinvestigatedinBMandidentifiedbytwo backbonemarkersinafour-colorMoAbpanel,suchasCD19 andCD34.
The mandatory panel for B-cell ALL MRD detection
(Table4)isaddressedtoidentifydeviationsinthematuration
CD 10 PE
CD 20 FITC NG2 PE CD 66 PE CD 20 FITC
A
B
C
D
E
CD 10 PE CD 15+CD 65 FITC CD 58 FITC
1E1
1E1 1
1 1E2
1E2 1E3
1E3 1E4
1E1
–1E2 1E2 1E3 1E4 1E5
–1E2 1E2 1E3 1E4 1E5
1 1E2 1E3 1E4
1E4 1 1E1 1E2 0 1E2 1E3 1E4 1E5 0 1E2 1E3 1E4 1E5 1E2 1E2
1E3 1E3
1E4 1E4
1E5 1E5
0 0
1E3 1E4
Figure1–MinimalresidualdiseaseinprecursorB-cellacutelymphoblasticleukemiausingmaturationtube: CD20FITC/CD10PE/CD19PerCP/CD34APC.(A)Atdiagnosis(77.6%ofblastcells)and(B)thesamepatientonDay15of
inductiontherapywithpositiveminimalresidualdisease(0.03%).(C)MLLAF4precursorB-cellacutelymphoblasticleukemia
withpositiveminimalresidualdisease(0.28%)onDay40afterhematopoieticstemcelltransplantation.(DandE)BCR-ABL
positiveprecursorB-cellacutelymphoblasticleukemiawithpositiveminimalresidualdisease(0.32%)beforeconditioning treatmentforhematopoieticstemcelltransplantation.GateinCD19+cells.Ingreen:matureB-cells(A–C),normalprecursor andmatureB-cells(DandE).Inred:blastcells.Inblue:normalCD34+precursorB-cells.Acquisition:1,000,000oftotal events.Method:bulklysis.
CD19PerCP or PEcy5.5/CD38APC and Tube 3: nTdT-FITC/CD10PE/CD19PerCPorPEcy5.5/CD34APC.
Recommendedtubesareintendedtorecognize:(i)markers thatarefrequently underexpressedinBcellALL compared to normal B-cells such as CD81; (ii) cross-lineage markers suchasCD15, CD65,CD66c,CD123;and (iii)markers asso-ciatedwithmolecularlesionssuchasCD66c[insomecases presenting the breakpoint cluster region-Abelson murine leukemia(BCR-ABL)fusionprotein]andNG2(associatedwith 11q23alterations);thislatteroneisoftenexpressed concomi-tantlytoCD15and/orCD65(Figure1).
Optionalmarkersare:CD9andCD22thatareexpressedin Bnormalcells andoftenunderexpressedintheir leukemic counterparts; CD58 that has been shown to be overex-pressedinleukemicblastswhencomparedtotheirnormal counterparts,28CD13andCD33(myeloidmarkers) as cross-lineagemarkersandCD25(interleukin2receptor)canalsobe associatedwiththepresenceofBCR-ABLpositivePBCALL.It mustbeemphasizedthatrecommendedandoptionalmarkers shouldbechosenaccordingtotheirexpressionatdiagnosis.
MRDdetectionofT-ALLinthe PBor BMistheoretically easier asmost stagesof normalT lymphocyte maturation occur inthe thymus.Therefore the presenceofan imma-ture T cell subset in the PB or BM should be considered
Table5–Fluorochromeconjugatedantibodypanelsused forminimalresidualdiseasedetectioninTcell-acute lymphoblasticleukemiabymultiparametricflow cytometry.
Mandatorypanel
Tube1–cyCD3FITC/mCD3PE/CD45PerCP/CD7APC Tube2–nTdTFITC/CD2PE/CD5PerCP/CD7APC
Recommendedtube
Tube3–CD1aFITC/CD99PE/mCD3PerCP/CD7APC
Optionalmarkersa
CD10PE,CD13PE,CD33PE,CD34PE,CD44PE,CD117PE
cy: cytoplasmic staining; n: nuclear staining; m: membrane staining.
a Accordingtoantigenexpressionatdiagnosis.
aberrant. For the investigation of MRD in T-cell ALL, CD3 and CD7are recommended asbackbonemarkers(Table5). Mandatoryandrecommendedtubesare addressedto iden-tifymaturation stageofblastcells and includeimmaturity markerssuchasTdT,CD34,CD1a,andCD99(Figure2). Dif-ficultiesinMRDdetectioninT-ALLlargelystemfromtheloss ofimmaturitymarkersontheabnormalblastpopulation fol-lowinginductionchemotherapy.OptionalmarkersforT-ALL
CD 99 PE mCD 3 PE CD 117 PE CD 34 PE
CD 7 APC
CD 45Per CP
–1E2
1E2 0 1E2
1E3 1E3
1E4 1E4
1E5
–1E2 1E2 1E3 1E4 1E5
1E5 1E2 1E3
1E3
1E4 1E4
1E5 1E5
0 0 1E2 1E3 1E4 1E5 0 1E2 1E3 1E4 1E5
0
1E3 1E4 1E5
0
MRDaimtorecognizecross-lineagemarkerssuchasCD13and CD33;amarkerthatisunderexpressedoroverexpressedin 81%ofT-ALLcasessuchasCD44,29andCD117,expressedin earlyT-ALL.ThesemarkersmaybeusefulforMRDdetection whentheyareexpressedatdiagnosis.
Dataacquisition
Data acquisition must be performed in sequence immedi-atelyaftersamplepreparationiscompleted.Foreachsample aliquot,a minimumof500,000 and maximum of1,000,000 eventsmustbeacquired.Optionally,laboratoriesthatperform bulklysisareabletoacquire5,000,000events.Acriterionfor quantifiableMRDpositivitywasestablishedusingadetection limitofabsoluteMRDcellcountsof10cellsormoreineach tube.38
Conclusion
MFC is a powerful method for MRD investigations of hematology malignancies, but it is fundamental to have good standardization of the pre-analytical, analytical and post-analyticalprocesses. TheMRDWorkingGroup recom-mendationsmeetthisrequirementwiththemaingoalbeing thepatients’safetyandcare.Forthispurpose,italsoshouldbe stressedthattheMFCandPCRtechniquesarecomplementary, andsoitisnecessarythatmoremolecularbiologylaboratories withexpertiseinIg/TCRassaysareavailableinBrazil.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthorsthankthecolleagueswhocontributedtothiswork bysendingdatafrom theirlaboratories:Alex FreireSandes (DivisãodeHematologiadoGrupoFleury,SãoPaulo,SP); Eliz-abeth Delbuono (GRAAC, São Paulo, SP); Leandro S Thiago (InstitutoNacionaldoCancer,RiodeJaneiro,RJ);MariaMirtes Sales(LaboratóriodeCitometriadeFluxodoHospitaldas Clin-icas,FaculdadedeMedicinaUniversidadedeSãoPaulo,SP).
Theauthors especiallythankDrLuciaSilla,presidentof SBTMO,DrNelsonHamerschlakcoordinatorofSBTMO work-inggroupsandDr.VergilioARensiColturato,whoconceived thegroup,forsupportingthedevelopmentofthegroup.
Appendix.
Members
of
MRD
Working
Group
of
SBTMO
AdrianaSeber,AnaPaulaAlegretti,AnaPauladeAzambuja, CintiaGFMachado, ElaineSobralda Costa,ElizabethXisto Souto,IreneGHLorand-Metze,MariaLuizaMenezesCortez, Mariester Malvezzi, Maura Rosane Valério Ikoma, Mihoko Yamamoto,MíriamPerlingeiroBeltrame,NormaLucena-Silva, NydiaStrachmanBacal,SilviaInesAlejandraCórdobaPires Ferreira,VergílioAntonioRensiColturato,VirginiaPires.
r
e
f
e
r
e
n
c
e
s
1.CaveH,vanderWerfftenBoschJ,SuciuS,GuidalC,
WaterkeynC,etal.Clinicalsignificanceofminimalresidual
diseaseinchildhoodacutelymphoblasticleukemia.European
OrganizationforResearchandTreatmentof
Cancer-ChildhoodLeukemiaCooperativeGroup.NEnglJMed.
1998;339(9):591–8.
2.ZhouJ,GoldwasserMA,LiA,DahlbergSE,NeubergD,Wang
H,etal.Quantitativeanalysisofminimalresidualdisease
predictsrelapseinchildrenwithB-lineageacute
lymphoblasticleukemiainDFCIALLConsortiumProtocol
95-01.Blood.2007;110(5):1607–11.
3.BorowitzMJ,DevidasM,HungerSP,BowmanWP,CarrollAJ,
CarrollWL,etal.Clinicalsignificanceofminimalresidual
diseaseinchildhoodacutelymphoblasticleukemiaandits
relationshiptootherprognosticfactors:aChildren’s
OncologyGroupstudy.Blood.2008;111(12):5477–85.
4.FlohrT,SchrauderA,CazzanigaG,Panzer-GrümayerR,van
derVeldenV,FischerS,etal.Minimalresidual
disease-directedriskstratificationusingreal-time
quantitativePCRanalysisofimmunoglobulinandT-cell
receptorgenerearrangementsintheinternational
multicentertrial.AIEOP-BFMALL2000forchildhoodacute
lymphoblasticleukemia.Leukemia.2008;22:771–82.
5.CampanaD.Roleofminimalresidualdiseasemonitoringin
adultandpediatricacutelymphoblastic.LeukemiaHematol
OncolClinNAm.2009;23:1083–98.
6.GaipaG,CazzanigaG,ValsecchiMG,Panzer-GrümayerR,
BuldiniB,SilvestriD,etal.Timepoint-dependent
concordanceofflowcytometryandreal-timequantitative
polymerasechainreactionforminimalresidualdisease
detectioninchildhoodacutelymphoblasticleukemia.
Haematologica.2012;97(10):1582–93.
7.BrüggemannM,SchrauderA,RaffT,PfeiferH,DworzakM,
OttmannOG,etal.StandardizedMRDquantificationin
EuropeanALLtrials:ProceedingsoftheSecondInternational
SymposiumonMRDassessmentinKiel,Germany,18–20
September2008.Leukemia.2010;24(3):521–35.
8.CampanaD.Minimalresidualdiseaseinacutelymphoblastic
leukemia.SeminHematol.2009;46(1):100–6.
9.OrfaoA,Flores-MonteroJ,LopezA,BarrenaS,CiudadJ,
VidrialesB,etal.FlowcytometryforMRDdetection:stateof
theart.In:AbstractBook.MRDTechniques:StateoftheArt.
InternationalSymposiumonMinimalResidualDiseasein
HematologicalMalignancies.ESLHO;2012.p.21–3.
10.ScrhrappeM.Minimalresidualdisease:optimalmethods,
timing,andclinicalrelevanceforanindividualpatient.
HematolAmSocHematolEducProgram.2012;2012:137–42.
11.BaderP,WillaschA,KlingebielT.Monitoringof
post-transplantremissionofchildhoodmalignancies:isthere
astandard?BoneMarrowTransplant.2008;42Suppl2:S31–4.
12.BaderP,KreyenbergH,vonStackelbergA,EckertC,
Salzmann-ManriqueE,MeiselR,etal.Monitoringofminimal
residualdiseaseafterallogeneicstem-celltransplantationin
relapsedchildhoodacutelymphoblasticleukemiaallowsfor
theidentificationofimpendingrelapse:resultsofthe
ALL-BFM-SCT2003trial.JClinOncol.2015;33(11):1275–84.
13.ClarkJR,ScottSD,JackAL,LeeH,MasonJ,CarterGI,etal.
Monitoringofchimerismfollowingallogeneichaematopoietic
stemcelltransplantation(HSCT):technicalrecommendations
fortheuseofShortTandemRepeat(STR)basedtechniques,
onbehalfoftheUnitedKingdomNationalExternalQuality
AssessmentServiceforLeucocyteImmunophenotyping
ChimerismWorkingGroup.BrJHaematol.2015;168(1):26–37.
14.SánchezJ,SerranoJ,GómezP,MartínezF,MartínC,MaderoL,
residualdiseaseinacutelymphoblasticleukaemiaafter
allogeneictransplantation.BrJHaematol.2002;116(3):686–94.
15.SchilhamMW,BalduzziA,BaderP.Istherearoleforminimal
residualdiseaselevelsinthetreatmentofALLpatientswho
receiveallogeneicstemcells?BoneMarrowTransplant.
2005;35Suppl1:S49–52.
16.IrvingJ,JessonJ,VirgoP,CaseM,MintoL,EyreL,etal.
Establishmentandvalidationofastandardprotocolforthe
detectionofminimalresidualdiseaseinBlineagechildhood
acutelymphoblasticleukemiabyflowcytometryina
multi-centersetting.Haematologica.2009;94(6):870–4.
17.GaipaG,BassoG,BiondiA,CampanaD.Detectionofminimal
residualdiseaseinpediatricacutelymphoblasticleukemia.
CytometryBClinCytom.2013;84(6):359–69.
18.GaipaG,BassoG,MagliaO,LeoniV,FainiA,CazzanigaG,
etal.Drug-inducedimmunophenotypicmodulationin
childhoodALL:implicationsforminimalresidualdisease
detection.Leukemia.2005;19(1):49–56.
19.DworzakMN,GaipaG,SchumichA,MagliaO,RateiR,Veltroni
M,etal.ModulationofantigenexpressioninB-cellprecursor
acutelymphoblasticleukemiaduringinductiontherapyis
partlytransient:evidenceforadrug-inducedregulatory
phenomenon.Resultsofthe
AIEOP-BFM-ALLFLOW-MRD-studygroup.CytometryBClin
Cytom.2010;78(3):147–53.
20.SedekL,BulsaJ,SonsalaA,TwardochM,WieczorekM,
MalinowskaI,etal.Theimmunophenotypesofblastscellsin
b-cellprecursoracutelymphoblasticleukemia:howdifferent
aretheyfromtheirnormalcounterparts?CytometryBClin
Cytom.2014;86(5):329–39.
21.vanDongenJJ.MRDdetectionbyIg/TCRtargets:stateofthe
art.In:AbstractBook.MRDTechniques:StateoftheArt.
InternationalSymposiumonMinimalResidualDiseasein
HematologicalMalignancies.ESLHO;2012.p.11–5.
22.vanderVeldenVH,BrüggemannM,HoogeveenPG,deBieM,
HartPG,RaffT,etal.TCRBgenerearrangementsinchildhood
andadultprecursor-BALL:frequency,applicabilityasMRD
PCRtarget,andstabilitybetweendiagnosisandrelapse.
Leukemia.2004;18(12):1971–80.
23.CampanaD.Minimalresidualdiseasemonitoringin
childhoodacutelymphoblasticleukemia.CurrOpinHematol.
2012;19(4):313–8.
24.KalinaT,Flores-MonteroJ,vanderVeldenVH,Martin-Ayuso
M,BöttcherS,RitgenM,etal.EuroFlowstandardizationof
flowcytometerinstrumentsettingsandimmunophenotyping
protocols.Leukemia.2012;26(9):1986–2010.
25.BulkErythrocyteLysingwithAmmoniumChlorideforFlow CytometryImmunophenotyping.Technicalprotocol. Availablefrom:https://www.bdbiosciences.com/documents/
Multicolor-Bulk-Erythrocyte-Lysing-Protocol.pdf[citedJuly
2014].
26.BassoG,VeltroniM,ValsecchiMG,DworzakMN,RateiR,
SilvestriD,etal.Riskofrelapseofchildhoodacute
lymphoblasticleukemiaispredictedbyflowcytometric
measurementofresidualdiseaseonday15bonemarrow.J
ClinOncol.2009;27(31):5168–74.
27.RoshalM,FrommJR,WinterS,DunsmoreK,WoodB.
Immaturityassociatedantigensarelostduringinductionfor
Tcelllymphoblasticleukemia:implicationsforminimal
residualdiseasedetection.CytometryBClinCytom.
2010;78(3):139–46.
28.VeltroniM,ZenL,SanzariMC,MagliaO,DworzakMN,RateiR,
etal.ExpressionofCD58innormal,regeneratingand
leukemicbonemarrowB-cells:implicationsforthedetection
ofminimalresidualdiseaseinacutelymphocyticleukemia.
Haematologica.2003;88(11):1245–52.
29.Coustan-SmithE,SongG,ClarkC,KeyL,LiuP,MehrpooyaM,
etal.Newmarkersforminimalresidualdiseasedetectionin
acutelymphoblasticleukemia.Blood.2011;117(23):6267–77.
30.GarandR,BeldjordK,CavéH,FossatC,ArnouxI,AsnafiV,
etal.FlowcytometryandIG/TCRquantitativePCRfor
minimalresidualdiseasequantitationinacutelymphoblastic
leukemia:aFrenchmulticenterprospectivestudyonbehalfof
theFRALLE,EORTCandGRAALL.Leukemia.2013;27(2):370–6.
31.IkomaMR,SandesAF,ThiagoLS,JuniorGB,Lorand-MetzeIG,
CostaES,etal.Firstproposedpanelsonacuteleukemiafor
four-colorimmunophenotypingbyflowcytometryfromthe
Braziliangroupofflowcytometry-GBCFLUX.CytometryBClin
Cytom.2015;88(3):194–203.
32.DworzakMN,FritschG,FleischerC,PrintzD,FröschlG,
BuchingerP,etal.Multiparameterphenotypemappingof
normalandpost-chemotherapyBlymphopoiesisinpediatric
bonemarrow.Leukemia.1997;11:1266–73.
33.vanWeringER,vanderLinden-SchreverBE,Szczepa ´nskiT,
WillemseMJ,BaarsEA,vanWijngaarde-SchmitzHM,etal.
RegeneratingnormalB-cellprecursorsduringandafter
treatmentofacutelymphoblasticleukaemia:implicationsfor
monitoringofminimalresidualdisease.BrJHaematol.
2000;110(1):139–46.
34.BabusíkováO,ZelezníkováT,KirschnerováG,KankuriE.
Hematogonesinacuteleukemiaduringandaftertherapy.
LeukLymphoma.2008;49(10):1935–44.
35.McKennaRW,AsplundSL,KroftSH.Immunophenotypic
analysisofhematogones(B-lymphocyteprecursors)and
neoplasticlymphoblastsby4-colorflowcytometry.Leuk
Lymphoma.2004;45(2):277–85.
36.vanLochemEG,vanderVeldenVHJ,WindHK,teMarveldeJG,
WesterdaalNAC,vanDongenJJ.Immunophenotypic
differentiationpatternsofnormalhematopoiesisinhuman
bonemarrow:referencepatternsforage-relatedchangesand
disease-inducedshifts.CytometryBClinCytom.
2004;60(1):1–13.
37.McKennaRW,LaBaronTW,AquinoDB,PickerLJ,KroftSH.
Immunophenotypicanalysisofhematogones(B-lymphocyte
precursors)in662consecutivebonemarrowspecimensby
4-colorflowcytometry.Blood.2001;98(8):2498–507.
38.KarawajewL,DworzakM,RateiR,RheinP,GaipaG,BuldiniB,
etal.Minimalresidualdiseaseanalysisbyeight-colorflow
cytometryinrelapsedchildhoodacutelymphoblastic