w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Health
locus
of
control,
spirituality
and
hope
for
healing
in
individuals
with
intestinal
stoma
Carmelita
Naiara
de
Oliveira
Moreira,
Camila
Barbosa
Marques,
Geraldo
Magela
Salomé
∗,
Diequison
Rite
da
Cunha,
Fernanda
Augusta
Marques
Pinheiro
UniversidadedoValedoSapucaí(UNIVÁS),PousoAlegre,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17July2015 Accepted25April2016 Availableonline30June2016
Keywords:
Intestinalstoma Internal-externalcontrol Spirituality
Religion Hope
a
b
s
t
r
a
c
t
Objective:Toassessthehealthlocusofcontrol,spiritualityandhopeofcureinpatientswith intestinalstoma.
Methods:ThisstudywasconductedatthePoloofOstomizedPeopleinthecityofPouso Ale-gre,MinasGerais.Participantswere52patientswithintestinalstoma.Threequestionnaires wereappliedfordatacollection:aquestionnaireondemographicandstoma-relateddata; theScaleforHealthLocusofControl;theHerthHopeScale,andtheSelf-ratingScalefor Spirituality.
Results:Mostostomizedsubjectswerewomenagedover61years,marriedandretired.Asto thestoma,inthemajorityofcasestheseoperationsweredefinitiveandwerecarriedoutdue toadiagnosisofneoplasia.Mostostomizedsubjectshada20-to40-mmdiametercolostomy, 27showeddermatitisasacomplication,and39(75%)usedatwo-partdevice.Themeantotal scorefortheScaleforHealthLocusofControl,theHerthHopeScale,andtheSelf-rating ScaleforSpiritualitywere62.42,38.27,and23.67,respectively.Regardingthedimensions oftheScaleforHealthLocusofControl,thedimension“completenessofhealth”=22.48, dimension“externality-powerfulothers”=22.48,anddimension“healthexternality”=19.48.
Conclusion:Ostomizedpatients participatingin thestudy believe theycancontrol their healthandthatcaregiversandindividualsinvolvedintheirrehabilitationcancontribute totheirimprovement.Thecureorimprovementhasadivineinfluencethroughreligious practicesorbeliefs.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](G.M.Salomé).
http://dx.doi.org/10.1016/j.jcol.2016.04.013
Locus
de
controle
em
saúde,
Espiritualidade
e
Esperanc¸a
de
cura
nos
indivíduos
com
estoma
intestinal
Palavras-chave:
Estomaintestinal Controleinterno-externo Espiritualidade
Religiosidade Esperanc¸a
R
E
S
U
M
O
Objetivo: Verificarolocusdecontroledasaúde,espiritualidadeeesperanc¸adecuraem indivíduosostomizados.
Métodos:EsteestudofoirealizadonoPolodosostomizadosdacidadedePousoAlegre,Minas Gerais.Fizerampartedoestudo52pacientescomestomaintestinal.Foramutilizadospara coletadedadostrêsquestionários:questionáriosobreosdadosdemográficoserelacionados aoestoma;EscalaparaLocusdecontroledasaúde;EscaladeEsperanc¸adeHertheEscalade auto-classificac¸ãoparaEspiritualidade.
Resultados: Amaioriadosostomizadoseradogênerofemininocomidadeacimade61anos, casadoseaposentados.Comrelac¸ãoaoestoma,amaioriadessesdispositivoseradefinitiva eascausasparaasuaconfecc¸ãododispositivoforam,emsuamaioria,umdiagnósticode neoplasia.Amaioriadosostomizadostinhaumacolostomiacomdiâmetrode20a40mm eapresentavamdermatitecomocomplicac¸ão;e39(75%)utilizavamdispositivosdeduas pec¸as.AmédiadoescoretotaldaescalaparaLocusdecontroledasaúde,EscaladeEsperanc¸a deHerth,eEscaladeAuto-classificac¸ãoparaEspiritualidadefoide,respectivamente,62,42, 38,27e23,67.Comrelac¸ãoàsdimensõesdaEscalaparaLocusdeCcontroledaSaúde,foram obtidososseguintesvalores:dimensãointegralidade“saúde”=22,48,dimensão externali-dade“outrospoderosos”=20,48edimensãoexternalidade“saúde”=19,48.
Conclusão: Ospacientesostomizadosqueparticiparamdoestudoacreditamquepodem controlarsuasaúde,equeaspessoasenvolvidasnocuidadoeemsuareabilitac¸ãopodem contribuirparasuamelhora.Acuraoumelhorateminfluênciadivinapormeiodaspráticas oucrenc¸asreligiosas.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este esunart´ıculoOpenAccessbajolalicenciaCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
An ostomy is an artificial communication between organs orvisceraand theexternalenvironmentforobtainingfood andfordrainageanddisposal.Themakingofanintestinal ostomyisamedical-surgicalprocedureinwhichachangein bowelhabitsoccurs,changinganatomicallythepatient,with externalizationofahollowviscus(inthiscase,theintestine) throughhis/herbody,andwhichisinsertedintotheexternal abdominalwall.Takingintoaccounttheoriginofthedisease, theostomymaybetemporaryordefinitive.1,2
The individual, after being submitted to a stoma, not onlylose a segment ofhis/her body but alsoundergoes a changeinphysicalappearance andgoeson livingwiththe lossofcontrolofeliminationoffecesandgases,whichnow occur through the abdomen, and this type of control is a paramountconditionforlifeinsociety.3,4 Patientsarefaced
withachallenge,whichistheself-care,whichincludesthe exchange of the collector device and skin and peristomal hygiene.
Self-careisaprocessthatispartoftheacceptanceprocess, bythe stomauser, ofhis/her newphysicaland physiolog-icalcondition.Thiscondition mustbeseen asanecessary therapeutictreatmentthataimstoimprovethepathological picture,inordertocurethepatient,wherethepurposeisnotto diminishthequalityoflifeofthoseostomized,buttoprioritize theirhealthinallareas.4–9
Thus,somechangesinthedailylivesoftheseindividuals occur,rangingfromphysiological,anatomicaland gastroin-testinalalterationstotheachievementofself-care.Inaddition tothesephysicalchanges,psychological,emotionalandsocial changes also occur; these individuals may feel incompe-tent,uselesstodevelopday-to-dayactivities,andespecially self-care. Often the patient ends up suffering changes in his/herreligiousness, losingfaithand thehopeofrecovery orimprovement,forfearthathe/shewillnotbeableto per-formself-care(whichconsistsofcleaningtheperistomalskin andofexchangingandcleaningthebag).Consequently,this factpromoteschangesinqualityoflife,self-esteem, spiritu-ality,self-image,sexuality,familyandsociallifeandleisure activitiesoftheindividual.
Spiritualitycanbedefinedasabeliefsystemthatincludes intangibleelementsthatconveyvitalityandmeaningtolife events.Suchabeliefcanmobilizeextremelypositiveenergies andinitiatives,withunlimitedpotentialtoimprovethe per-son’squalityoflife.Religiouspeoplearephysicallyhealthier, havemorehealthfullifestyles andrequire lesshealthcare. Thereisanassociationbetweenspiritualityandhealththatis probablyvalidandpossiblycausal.Itisfullyrecognizedthat thehealthofindividualsisdeterminedbytheinteractionof physical,mental,socialandspiritualfactors.10,11
Hope is a state associated with a positive outlook for the future, a way to cope with the situation that one is experiencing,12,13 inwhichthe individualhasfaithand the
individualtoactandgivesstrengthtosolveproblemsand con-frontations,suchasloss,tragedy,lonelinessandsuffering.14
Healthlocusofcontrolisasetofbeliefsthatindividuals layonthesourceofcontrolofusualbehaviorsoreventsthat occur to themselves or to the environment in which they areinserted,indicatingtheexistenceofacontrolof internal-externalreinforcement,withregardtothedegreetowhichthe individualbelievesthatthereinforcementsarecontingenton his/herconduct.15,16
Theconstruct“healthlocusofcontrol”isdesignedas a multidimensional variable. External beliefs can be divided into random expectations (the reinforcement would be determinedbyluck,byfate)andexpectationsthatthe rein-forcements would bedependent onthe actionofpowerful others(suchasfamily,teachersordoctors).Thesubjectswho believethatpowerfulotherscontroltheirlivescanact differ-ently,incomparisonwiththosewhobelievethattheevents oftheirlivesemergechaoticallyandunpredictably.17,18
Theevaluationofthehealthlocusofcontroland spiritu-alityandhopeofcurecanbecomeanessentialinstrumentin guidinghealthactionsforostomizedpeople,consideringthat thisprovidessubsidiesforabetterunderstandingofthe psy-chosocialandemotionalfactorsinvolvedwiththedifficulties oflivingwiththestomaandintheachievementofself-care.
Thestudyofaspectsofspiritualityandhopeofcurewill providerelevantinformationwhichmay influencethe self-carebytheostomizedindividualand his/heracceptanceof beinganostomizedpatientandinlivingwiththestoma.Thus, thisstudyaimstodeterminethehealthlocusofcontrol, spiri-tuality,andhopeofacureinpatientswithanintestinalstoma.
Methods
Thisisadescriptive,cross-sectionalanalyticalstudy. ThisstudywasconductedatthePoloofOstomized Peo-pleinthecityofPousoAlegre,MinasGerais.52patientswith intestinalstomawereincluded.
Theinclusion criteriawere age ≥18 years and being an
intestinalstomacarrier,andexclusioncriteriawerepatients withdementia syndromesand other conditionsthat could preventthemfromunderstandingandansweringtothe ques-tionnaires.
DatawerecollectedafterapprovalbytheEthics Commit-teeonResearchoftheFaculdadedeCiênciasdaSaúde“Dr. JoseAntonioGarciaCoutinho”andaftertheFreeandInformed Consent Form was signed by the patient or his/her care-giver(opinionnumber:620462). Data werecollected bythe researchersthemselves. Theinclusion ofthepatientinthe studyfollowedtheorderofarrivalattheoutpatientclinic.The samplewasselectedinanon-probabilistic,byconvenience, way.
Fordatacollection,threequestionnaireswereapplied:first, aquestionnaireondemographicandstoma-relateddata;then theScaleforHealthLocusofControl;thethirdquestionnaire wastheHerthHopeScaleand,finally,theSelf-ratingScalefor Spirituality.Eachinterviewlastedapproximately25min.
TheScaleforHealthLocusofControlhasbeentranslated andvalidated forthePortugueselanguage.Theinstrument validation,afterapplicationinfoursamples,wasverifiedas
to the reliability (internal consistency) through Cronbach’s alpha,andthevaluesfoundforthesubscaleswere: Internal-ityforhealth,0.62–0.71;Externality-chanceforhealth,0.51–0.78; andExternality-powerfulothers,0.62–0.67.Thisscaleconsistsof threesubscales,eachcontainingsixitemsregardingthe fol-lowingdimensions:Internalityforhealth(items1,6,8,12,13 and 17),whereinthescoresreflectthedegreetowhichthe subjectbelievesthathe/shehimselfcontrolshis/herstateof health;externality-powerful othersforhealth(items3,5,7,10, 14 and 18), wherein the scoresreflectthe degree towhich the subjectbelievesthatother persons orentities(doctors, nurses,friends,family,God,etc.)cancontrolhis/herhealth; andExternality-chanceforhealth(items2,4,9,11,15and16), in whichthe scoresindicate thedegree towhicha person believes that his/herhealth iscontrolled atrandom, with-outhis/herinterferenceortheinterferencefromotherpeople The scores for each dimension range from 1to 5; for the alternatives“Itotallyagree,”“Ipartiallyagree,”“Iam unde-cided,” “I partiallydisagree,” and “I strongly disagree,” the followingvaluesarerespectivelyadded:5,4,3,2,and1.The score obtained for the dimensions willbe the sum of the itemsofthesubscaleatissue.Thetotalvalueofitems belong-ingtoeachofthethreesubscalesrepresentsthetotalscores withrespecttothedimensionofthehealthlocusin ques-tion.Thetotalamountobtainedfromeachsubscalemayvary between 6and 30 andindicates that the higherthe value, the strongerthe belief inthisdimension.Thescale is pre-sentedinitsentirety,inwhichtheitemsofthesubscalesare interleaved.12,19
The Escala da Esperanc¸a de Herth (EEH),that is, the Por-tuguese version of the Herth Hope Scale, is a tool which consistsof12itemswithatotalscoreof12–48points,with responsesproducedinaLikert-likescale,withscoresfrom1to 4pointsforeachoneoftheseitems.Thehigherthescore,the greaterthehope.Theitems3and6haveaninvertedscore.18,20
Intheassessmentoftheresults, datawere enteredand analyzedusingthestatisticalprogramSPSS v.8.0.Fordata analysis, the following statistical tests were used: for the distributionofabsolute(n)andrelative(%)frequencies, Pear-son’sChi-squaredtestwasused,whichdeterminedwhether thedistributionwasdifferentfrom5%,thatis,p<0.05.The comparisonbetween two groupswas performed using the Mann–Whitney test; and when there were more than two groups,theKruskal–Wallistestwasused.Forthecorrelationof continuouswithsemi-continuousvariables,theSpearman’s correlationtestwasused.
Results
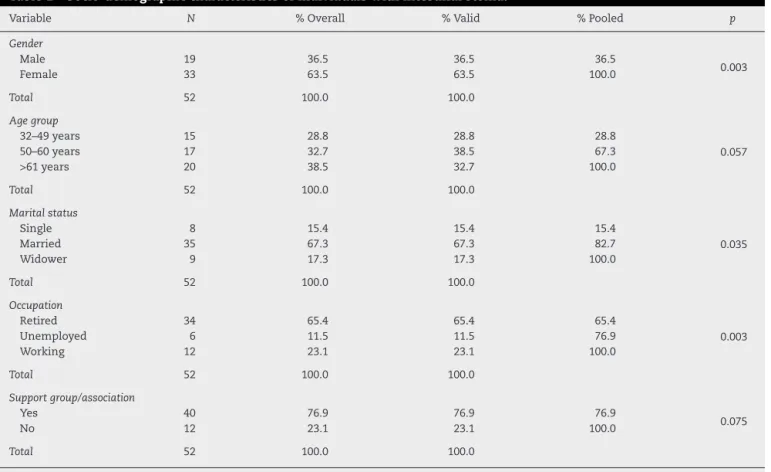
Table1shows that33(63.5%)patientswerefemale, and20
(38.5%)wereagedover61years.36%oftheparticipantsinthis studyweremarried,34(65.4%)wereretired,40(76.9%) partici-patedinasupportgrouporassociation.Thevariablesgender, maritalstatus,andoccupationhadstatisticalsignificance.
Table2showsthatthemaincauseofmakingthestoma
wasthepresenceofaneoplasmin40(76.9%)patients,and40 (76.9%)stomataweredefinitive.44(84.6%)patientsreceiveda colostomy,andin27(51.9%)thestomameasured20–40mm. 31(51.7%)oftheparticipantsshoweddermatitis,and39(75%) usedtwo-piecedevices.Allthesevariableswerestatistically significant.
Table3showsthatthemeantotalscoreoftheScalefor
HealthLocusofControlwas62.42;fortheHerthHopeScale,it was38.27;andfortheSelf-ratingScaleforSpirituality,itwas 23.67.Theseresultswerestatisticallysignificant.
Table4showsthedimensionsoftheScaleforHealthLocus
ofControl:22.48forthedimension“Completenessofhealth”, 20.48 forthe dimension “Externality-powerfulothers”, and 19.48forthedimension“Externality-health”,allwith statis-ticalsignificance.
Discussion
Regardingsociodemographiccharacteristicsofthe52patients withintestinalstomaincludedinthisstudy,mostwereelderly womenagedover 60,retired, married,and participating in asupportorassociation group,whichisinline withother investigationswhosesubjectshadanintestinalstoma.5,9
The gender of the stomized individual can influence his/hersocialadaptation.Womentendtorequirelesstimeto rehabilitationbutshowsignificantdegreesofdespair, depres-sion and fear in the preoperative period. Men, especially thosewhodevelopimpotence,takealongertimetorespond satisfactorilytotheirroutineactivities,andexhibitmore sig-nificantdifficultiesforself-care.23Itisimportanttopointout
that the elderly have unique biological characteristics and thatthisagegroupismorevulnerabletochronicdiseases,for instance,neoplasms.
Theoccurrenceofstomacomplicationsismultifactorial, involvingfromthemakingofthestomatillitslocation, obe-sity,andinfluenceoftheagefactor.Thus,whenthesefactors areassociatedwiththephysiological changesofaging,the expectedoutcomeisagreatervulnerabilityoftheelderlywith respecttotheincidenceofcomplicationsinthestoma.24
Inthisstudy,mostparticipantswereilliterateandretirees. Thisresultrevealsadisturbing profile,whenonethinksin termsofcitizenshipandrespectforindividualrights,taking intoaccountthatitisknownthatthelowertheeducational level,themoreunfavorableisthelinguisticcapitalofthe indi-vidualtothequestioningofprofessionalsand leaderswith respecttohis/herhealthproblems,thecaretobeoffered,and therightsthatareinherenttoeachperson.Itisimportantto notethatthissituationdoesnotaffecttheperformancewith these peoplebecause theinteraction betweenuser, service andhealthprofessionalshavemadepossibletoovercomethe difficultiesimposedbythisvariable.
Datarelatingtothestomaindicatethat,inmostofthe par-ticipants,neoplasiawasthemaincausalfactortothestoma; thetypeofostomyperformedwascolostomy,andtheostomy wasofthedefinitivetype;theuserswereprovidedwitha 2-piecebag,andmosthaddermatitisasacomplication.With respecttothe stomasize, mostaveraged20–40mm. These findingsagreewithseveralstudiespublished.7,25–28
Itisworthnotingthatthetimespentwiththestomawill dependonthecausativefactorandontheclinicaloutcome afterits making.Thus,anoriginallytemporary stomamay becomepermanent,dependingontheimpeditivefactorsto the reconstructionofintestinaltransit,takinginto account thatinmanycasesthediseasesofthegastrointestinaltract lead toaradical surgery,resulting inatemporary, oreven definitive,ostomy.24
Anotherstudyexaminedtheknowledgeoftheostomized individual regardingthe properself-care afterhospital dis-charge and the incidence of complications related to the stoma. This is a qualitative, exploratory, field study with quantitative data contribution. In our study, we applied a semi-structuredinterviewasatechniquefordatacollection. Tenpatientswithanintestinalstoma(colostomy/ileostomy) participatedinthisstudy,andtheresultsdemonstratedthat mostpatientshaddifficultywithself-care,thankstoalack ofproperguidanceand/orthehelpofprofessionalstrainedto workinthisphaseoftreatment.29
Oneshouldalsoconsiderthatsomecomplicationsincrease with age and alsoin patients without demarcation of the stoma.Consideringthatnostomademarcationwascarried out in the study population (predominantly composed of elderly),itcanbesaidthatthisfactwasoneofthefactorsthat mayhavecontributedtothedevelopmentofcomplications, suchthoseaforementioned,thusconfirmingthefindingsin otherstudies.
Generally, dermatitis in an injury resulting from an improperuseofcollectorequipment,morepreciselyby exces-sivecuttingoftheholeintheprotectivebarrierrelativetothe stoma(thus,theskinisexposedtotheactionoftheeffluent), orbyinadequateindicationofequipmentwithrespecttothe typeofstomaatissue.Collectorsandadjuvantsonthemarket shouldbepresentedindetailtoostomizedpatients.Insome services,theequipmentusedisrecommendedbasedonthe resultsoftheassessmentmadeatthetime;butovertime,the devicecanbereplaced.Thus,acontinuousassessmentisin order.30
Table1–Socio-demographiccharacteristicsofindividualswithintestinalstoma.
Variable N %Overall %Valid %Pooled p
Gender
Male 19 36.5 36.5 36.5
0.003
Female 33 63.5 63.5 100.0
Total 52 100.0 100.0
Agegroup
32–49years 15 28.8 28.8 28.8
0.057
50–60years 17 32.7 38.5 67.3
>61years 20 38.5 32.7 100.0
Total 52 100.0 100.0
Maritalstatus
Single 8 15.4 15.4 15.4
0.035
Married 35 67.3 67.3 82.7
Widower 9 17.3 17.3 100.0
Total 52 100.0 100.0
Occupation
Retired 34 65.4 65.4 65.4
0.003
Unemployed 6 11.5 11.5 76.9
Working 12 23.1 23.1 100.0
Total 52 100.0 100.0
Supportgroup/association
Yes 40 76.9 76.9 76.9
0.075
No 12 23.1 23.1 100.0
Total 52 100.0 100.0
Pearson’sChi-squaredtestandp≤ 0.05.
ostomizedpatient.Thesedifficultiesconcerntheacceptance ofchangesinbodyimage,lifestyle,socialrelationshipsand
sexualperformance– whichcan leadtopsychologicaland
socialdisorders,oftendifficulttoovercome.29
Inrecentyears,the increaseinlifeexpectancyhas con-tributed to the worldwide increase in the incidence and prevalenceofchronicdiseases,especiallydiseasesinwhich peoplereceivestomata.Thus,theneedsofpeoplewhohave toliveinthisconditionaresignificantandaffectmanyaspects oftheirlives,withtheincorporationofnewhabits,aswellas, ofnecessity,areviewandadaptationofsocialroles.
Inthis study,the resultsrelatedto theScaleforHealth LocusofControlrevealedthatostomizedindividuals partic-ipatinginthestudybelievethattheycancontroltheirhealth, andthatthepeopleinvolvedintheircareandrehabilitation cancontributetotheirimprovement.Butthisimprovement andthecurehavenodirectinterferenceinpeopleinvolvedin thetreatment.
Oftentheadaptationofostomizedindividualsoccurswith theadjustmentoflifeinanewcontext,inwhichimportant factorssuchasthewayoflife,sociallifeandfeedinghabits havetobeabandoned,replacedordiminishedinagreat num-berofcases.Thus,thisisanindividualprocessthatdevelops overtimeandthatinvolvesanumberofaspects,rangingfrom the help provided, tothe way the person gets involved in his/herowncare.31
With an intestinal stoma, the patient experiences momentsofconflict,concernsanddifficultiesindealingwith this new situation. This leads the individual to visualize
his/herlimitationsand tofacethe changesinhis/herdaily life.32Thus,itisimportantthatthepatientreceivessupport
fromfamily,friendsandevenfromthoseprofessionalswho arehelping.Withthissupport,thepatientwillfindstrength toovercomethedifficultiesandbarriersrelatedtoself-care andthechangesthatarebeingexperiencedinhis/herdaily live.
The health locus of control is a model that questions whetherthebeliefsoftheindividual,thatis,motivation (inter-nal and external), determine the action to be taken. The individualwhobelievesthattheresults,atleastinpart,are dependentontheactionstaken,isconsideredasinternally oriented;ontheotherhand,thosewithanexternalorientation generallydonotbelieve,orscarcelybelieve,intheexternal relationoftheoutcome,andintheindividualaction.33The
beliefsinfluencetheindividualwithastomaontheperception andexpressionofhopeandfaithinhis/hercureor improve-ment,andonhowtohandlethesevaluesintheinteraction withastomizedhumanbeing.
Table2–Characteristicsofintestinalstoma.
Variable N %Overall %Valid %Pooled p
Causeofostomy
Neoplasia 40 76.9 17.3 76.9
0.003
Inflammatoryboweldisease 9 17.3 17.3 94.2
Trauma 2 3.8 3.8 98.1
Other 1 1.9 1.9 100.0
Total 52 100.0 100.0
Stomatype
Colostomy 44 84.6 84.6 84.6
0.007
Ileostomy 8 15.4 15.4 100.0
Total 52 100.0 100.0
Stomadiameter
0–20mm 12 23.1 23.1 23.1
0.056
20–40mm 27 51.9 51.9 75
40–60mm 10 19.2 19.2 94.2
60–80mm 3 5.8 5.8 100.0
Total 52 100.0 100.0
Complicationtype
Dermatitis 31 51.7 51.7 51.7
0.0023
Fistula 2 3.3 3.3 55
Granuloma 2 3.3 3.3 58.3
Bleeding 2 3.3 3.3 61.7
Peristomalhernia 6 10.0 10.0 71.7
Pseudo-verrucouslesions 5 8.3 8.3 80.0
Allergicreaction 9 15.0 15.0 95.0
Allergy 3 5.0 5.0 100.0
Total 60 100.0 100.0
Typeofdevice
One-piecesystem 13 25 25 25
0.043
Two-piecesystem 39 75 75 100.0
Total 52 100.0 100.0
Stomacharacter
Temporary 12 23.1 23.1 23.1
0.003
Definitive 40 76.9 76.9 100.0
Total 52 100.0 100.0
Pearson’sChi-squaredtestandp≤0.05.
Table3–ResultsobtainedinthemeanscorefortheScaleforHealthLocusofControl,HerthHopeScaleandSelf-rating ScaleforSpiritualityinpatientswithintestinalstoma.
Descriptivelevel ScaleforHealthLocusofControl HerthHopeScale Self-ratingScaleforSpirituality
Mean 62.42 38.27 23.67
Median 63 38 24.5
Standarddeviation 7.944 3.515 5.279
Minimum 45 32 11
Maximum 81 47 30
P-Value 0.023
Mann–Whitneytest,Kruskal–Wallistestandp≤ 0.05.
Inthese studies related to the dimensionsof the Scale
forHealthLocusofControl, thepatients respondedas fol-lows:(22.48)relatedtothedimension“Completeness-health,” (20.48) related to the dimension“Externality-powerful oth-ers,” and (19.48) related to the dimension “Externality to health,”withstatisticalsignificance,thuscharacterizingthat theostomizedindividualsparticipatinginthestudybelieve
that they can control their health and that the people
involvedintheircareandrehabilitationcancontributetotheir improvement.However,thisimprovementandthecuredonot interferedirectlyinthepeopleinvolvedintheirtreatment.
Table4–ResultsobtainedinthemeanscorefortheScaleforHealthLocusofControl,HerthHopeScaleandSelf-rating ScaleforSpiritualityinpatientswithintestinalstoma.
Descriptive level
Dimensions
Internalityforhealth Externality–“powerfulothers” Externalityforhealth
Mean 22.48 20.48 19.48
Median 22.5 20 20
Standarddeviation 2.646 4.444 4.881
Minimum 16 12 10
Maximum 28 19 30
p-Value 0.031
Mann–Whitneytest,Kruskal–Wallistestandp<0.05.
caredependsmoreonothersthanonhimself.Itwasfound
thatthedimension“Internality”andthatoftheindex“Total internality”influencetheadherencetotreatmentandto self-careandrehabilitationofostomizedpeople,thatis,ostomized individualswithmore“Internality”adheredlesstotheir treat-ment.Theseresultsdemonstratetheimportanceofbeliefsin
thetherapeuticmanagement,andintherehabilitationand
self-care;andthatspecificinterventions,aimedatincreasing theadherence,shouldbetested.
Thediseasedpersoncanexperiencesituationsof
power-lessnessstemmedfromseveralfactors,rangingfromchanges relatedtothediseasetotheinteractionwiththehealthteam. Thelocusofcontrolinfluencesthepatient’sbehaviorinthe faceofthehealthproblem,bydirectingtheawarenessto fac-torsdependenton him/herselfor onother externalforces. Knowingtheorientationofthepatient’s locusofcontrolis important,inordertoforeseethe changesthatthepatient willneedtopromote,withaviewtoabettercontrolofhis/her treatment.35
Inthis study,assessed ostomizedpatients showedtotal meansof38.27and23.67forSelf-RatingScalefor Spiritual-ityandHerthHopeScale,respectively.Thesefindingsshow thattheseindividualshavehopeandfaithinGodthatthey willimproveandthattheypraytoGodforobtaininghelpto facethedifficultsituationstheyareexperiencing.
Spirituality and religion are related to each other, but althoughtheseconceptsareoftenusedinterchangeably,they donotshare thesame characteristics.Spiritualityis some-thingbroaderandmorepersonal,andisrelatedtoasetof innervalues,innerwholeness,harmony,andconnectionwith others;itstimulatesaninterestinothersandinourselvesand looksforaunitywithlife,nature,andtheuniverse.Spirituality iswhatgivesmeaningtolife,regardlessofone’sreligion,and thus,generatesthe capacitytoendure debilitating feelings ofguilt,angerandanxiety;furthermore,spiritualistaspects can mobilize positive energies and improve the quality of life.10Whenitcomestoostomizedpeople,spiritualitycanbe
contemplatedasoneofthecopingresourcesinperforming self-careandrehabilitation.
Inonestudy,theauthorsreportthatoneofthewaysof copingwiththediseaseandwithdeathisdirectlylinkedto theintensityoffaithandreligious beliefs-thatis,waysof expressingspirituality.Theauthorsconcludedthatoneofthe waysofcopingwithadverseandfavorablesituationsisinthe feelingoffaithinGod.FaithinGodisadeep-seatedfeelingin ourcultureandisasnecessaryastheotherwaysofcoping;
thediscourseshowsthatthespiritualdimensionoccupiesa prominentplaceinpeople’slivesandalsoshowsthatitisthat itessentialtobeawareofthespiritualityoftheuserstoplan anursingcare.35
Spiritualitycontributestothewell-beingofostomized peo-ple,favoring theirresilienceinthesuccessofself-care and rehabilitation. Certainreligious andspiritualbehaviors and beliefsaredirectlyrelatedtooverallhappinessandphysical health, consideringthattheydiscourageanengagementin unhealthy behaviors.Through thisstudy,weconclude that ostomizedpatientsbelievethatcancontroltheirhealthand that those people involvedin their careand rehabilitation cancontributetotheirimprovement.Theybelieveinadivine influenceonthecureorimprovement,throughreligious prac-ticesorbeliefs.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PittmanJ,RawlSM,SchmidtCM,GrantM,KoCY,WendelC,
etal.Demographicandclinicalfactorsrelatedtoostomy
complicationsandqualityoflifeinveteranswithanostomy.J
WoundOstomyContNurs.2008;35:493–503.
2.SampaioFAA,AquinoOS,AraújoTL,GalvãoMTG.Nursing
caretoanostomypatient:applicationoftheOrem’stheory.
ActaPaulEnferm.2008;21:94–100.
3.GomesIC,BrandãoGMON.Permanentintestinalostomes:
changesinthedailyuser.EnfermUFPE.2012;6:1331–7.
4.MauricioVC,OliveiraNVD,LisboaMTLO.enfermeiroesua
participac¸ãonoprocessodereabilitac¸ãodapessoacom
estoma.EscAannaNery.2013;17:416–22.
5.SaloméGM,AlmeidaSA,SilveiraMM.Qualityoflifeand
self-esteemofpatientswithintestinalstoma.JColoproctol.
2014;34:231–9.
6.SaloméGM,CarvalhoMRF,MassahudMR,MendesB.Profileof
ostomypatientsresidinginpousoalegrecityperfildos
pacientesostomizadosresidentesnomunicípiodepouso
alegre.JColoproctol.2015;35:106–12.
7.SalomeGM,AlmeidaSA.Associationofsociodemographic
andclinicalfactorswiththeself-imageandself-esteemof
individualswithintestinalstoma.JColoproctol.
2014;34:159–66.
8.SaloméGM,SantosLF,CabeceiraHS,PanzaAMM,PaulaMAB.
Knowledgeofundergraduatenursingcourseteachersonthe
preventionandcareofperistomalskin.JColoproctol.
9. CostaVF,AlvesSG,EufrásioC,SalomeGM,FerreiraLM.Body
imageandsubjectivewell-beinginostomistsinBrazil.
GastrointestNurs.2014;12:37–47.
10.AaadM,MasieroD,BattistellaLR.Espiritualidadebaseadaem
evidências.ActaFisiátr.2001;8:107–12.
11.SaloméGM,AlmeidaAS,FerreiraLM.Associationof
sociodemographicfactorswithhopeforcure,religiosity,and
spiritualityinpatientswithvenousulcers.AdvSkinWound
Care.2015;28:76–82.
12.HerthK.Therelationshipbetweenlevelofhopeandlevelof
copingresponseandothervariablesinpatientswithcancer.
OncolNursForum.1989;16:67–72.
13.JakobssonA,SegestenK,NordholmL,OreslandS.
EstablishingaSwedishinstrumentmeasuringhope.ScandJ
CaringSCI.1993;7:135–9.
14.HerthK.Abbreviatedinstrumenttomeasurehope:
developmentandpsychometricevaluation.JAdvNurs.
1992;17:1251–9.
15.HaslamSA,ReicherS.Stressingthegroup:socialidentityand
theunfoldingdynamicsofresponsestostress.JApplPsychol.
2006;91:1037–52.
16.RotterJB.Internalversusexternalcontrolofreinforcement:a
casehistoryofvariable.AmPsycholAssoc.1990;45:489–93.
17.LevensonH.Activismandpowerfulothers:distinctions
withintheconceptofinternal-externalcontrol.JPersAssess.
1974;38:377–83.
18.SartoreAC,GrossiSAA.Herthhopeindex:instrument
adaptedandvalidatedtoPortuguese.EscEnfermUsp.
2008;42:227–32.
19.Rodríguez-RoseroJE,FerrianiMGC,DelaCMF.Escaladelocus
decontroledasaúde–MHLC:estudosdevalidac¸ão.
Latino-AmEnferm.2002;10:179–84.
20.BalsanelliACS,GrossiSAA,HerthK.Assessmentofhopein
patientswithchronicillnessandtheirfamilyorcaregivers.
ActaPaulEnferm.2011;24:354–8.
21.GalanterM,DermatisH,BuntG,WilliamsC,TrujilloS.
Assessmentofspiritualityanditsrelevancetoaddiction
treatment.JSubstAbuseTreat.2007;33:257–64.
22.Gonc¸alvesMAS,PillonSC.Adaptac¸ãotransculturale
avaliac¸ãodaconsistênciainternadaversãoemportuguêsda
SpiritualityRatingScale.PsiquiatrClín.2009;36:10–5.
23.MacedoMS,NogueiraLT,LuzMHBA.Perfildosestomizados
atendidosemhospitaldereferênciaemteresina.Estima.
2005;3:25–8.
24.AguiarESS,SantosAAR,SoaresMGO,AncelmoMNS,Santos
RS.Complicac¸õesdoestomaepeleperiestomaempacientes
comestomasintestinais.Estima.2011;9:22–30.
25.BatistaMRFF,RochaFCV,SilvadMG,JúniorFJGS.Self-imageof
clientswithcolostomyrelatedtothecollectingbag.Bras
Enferm.2011;64:1043–7.
26.FortesRC,MonteiroTMRC,KimuraCA.qualityoflifefrom
oncologicalpatientswithdefinitiveandtemporary
colostomy.JColoproctol.2012;32:253–9.
27.NakagawaH,MisaoH.Effectofstomalocationonthe
incidenceofsurgicalsiteinfectionsincolorectalsurgery
patients.JWoundOstomyContNurs.2013;40:287–96.
28.CunhaRR,FerreiraAB,BackesVMS.Caractyeristica
sócio-demograficoeclínicodepessoasestomizados:revisão
deliteratura.Estima.2013;11:29–35.
29.TosatoSR,ZimmermannMH.Conhecimentodoindivíduo
ostomizadoemrelac¸ãoaoautocuidado.UEPG.2006;1:34–7.
30.FernandesRM,MiguirELB,DonosoTV.Perfildaclientela
estomizadaresidentenomunicípiodePonteNova,Minas
Gerais.BrasColoproct.2011;30:385–92.
31.NascimentoCMS,TrindadeGLB,LuzMHBA,SantiagRF.
Vivênciadopacienteestomizado:umacontribuic¸ãoparaa
assistênciadeenfermagem.TextoContexto–Enferm.
2011;20:557–64.
32.VieiraLM,RibeiroBNM,GattiMAN,SimeãoSFAP,ContiMHS,
VittaA.Câncercolorretal:entreosofrimentoeorepensarna
vida.Saúdedebate.2013;37:267–9.
33.SaloméGM,deAlmeidaAS,deJesusPMT,MassahudMR,de
OliveiraMCN,deBritoMJA,etal.Theimpactofvenousleg
ulcersonbodyimageandself-esteem.AdvSkinWoundCare.
2016;29:316–21.
34.CarvalhoSRM,BudóMLD,SilvaMM,AlbertiGF,SimonBS.
comumpoucodecuidadoagentevaiemfrente:vivênciasde
pessoascomestomia.TextoContextoEnferm.2015;24:
279–87.
35.KuritaGP,PimentaCAM.Adesãoaotratamentodador
crônicaeolocusdecontroledasaúde.EscEnfermUSP.