w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Association
of
sociodemographic
and
clinical
factors
with
spirituality
and
hope
for
cure
of
ostomized
people
Carmelita
Naiara
de
Oliveira
Moreira,
Camila
Barbosa
Marques,
Marcial
Alexandre
Pereira
da
Silva,
Fernanda
Augusta
Marques
Pinheiro,
Geraldo
Magela
Salomé
∗UniversidadedoValedoSapucaí(UNIVÁS),PousoAlegre,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19January2016 Accepted20April2016 Availableonline21June2016
Keywords: Intestinalstoma Internal-externalcontrol Spirituality
Religion Hope
a
b
s
t
r
a
c
t
Objective:Toevaluatethesociodemographicandclinicalfactorsrelatedtopatientswith intestinalstomaandcorrelatethemtothehealthlocusofcontrol,spiritualityandhopefor acure.
Method:ThisstudywasconductedatthePoloofOstomizedPatientsofthecityofPouso Ale-gre,MinasGerais.Participantswere52patientswithintestinalstoma.ThescaleforHealth LocusofControl,theHerthHopeScale,andtheSelf-ratingScaleforSpiritualitywereused fordatacollection.
Results:Thepatientswereagedupto50years,withthefollowingmeans:HerthHopeScale: 17.53;Self-ratingScaleforSpirituality:19.33.Withregardtomaritalstatus,singlepeople hadameanof21.00fortheHerthHopeScale.Retiredostomizedpatientshadameanof 20.53fortheHerthHopeScale,of10.38fortheSelf-ratingScaleforSpirituality,andofScale forHealthLocusofControl,of18.79.Thepatientswhosecauseofmakingthestomawas neoplasiaattainedameanof19.43fortheSelf-ratingScaleforSpirituality.Regardingthe characterofthestoma,themeanfortheHerthHopeScalewas18.40.Intheostomized individualswholivedwiththestomaforlessthanfouryearsthemeansfortheHerthHope Scale,Self-ratingScaleforSpirituality,andScaleforHealthLocusofControlwere17.39, 20.35,and23.09,respectively.Patientswhodidnotparticipateofanassociationorsupport hadmeansfortheHerthHopeScale,Self-ratingScaleforSpirituality,andScaleforHealth LocusofControlof19.08,17.25,and20.63respectively.
Conclusion:Ostomizedpatientsbelievetheycancontroltheirhealthandthatthoseinvolved intheircareandrehabilitationcancontributetotheirimprovement.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](G.M.Salomé). http://dx.doi.org/10.1016/j.jcol.2016.04.009
Associac¸ão
dos
fatores
sociodemográficos
e
clínicos
com
a
espiritualidade
e
esperanc¸a
de
cura
dos
ostomizados
Palavras-chave: Estomaintestinal Controleinterno-externo Espiritualidade
Religiosidade Esperanc¸a
r
e
s
u
m
o
Objetivo:Avaliarosfatoressociodemográficoseclínicosrelativosaospacientescomestoma intestinalecorrelacioná-losaolocusdecontroledasaúde,espiritualidadeeesperanc¸ade cura.
Métodos:EsteestudofoirealizadonoPolodosOstomizadosdacidadedePousoAlegre,Minas Gerais.Fizerampartedoestudo52pacientescomestomaintestinal.Foramutilizadospara coletadedadosaEscalaparaLocusdeControledaSaúde;EscaladeEsperanc¸adeHerth,e Self-ratingScaleforSpirituality.
Resultados:Ospacientesnafaixaetáriaaté50anostiveramasseguintesmédias:HerthHope Scale:17,53;Self-ratingScaleforSpirituality:19,33.Noqueconcerneaoestadocivil,as pes-soassolteirastiveramamédiade21,00paraaEscaladeEsperanc¸adeHerth.Osostomizados aposentadosatingiramasseguintesmédiasparaasescalas:EscaladeEsperanc¸adeHerth: 20,53;Self-ratingScaleforSpirituality:10,38eEscalaparaLocusdeControledaSaúde:18,79. Ospacientescujacausadaconfecc¸ãodoestomafoineoplasiativeramamédiade19,43para aSelf-ratingScaleforSpirituality.Comrelac¸ãoaocaráterdoestoma,amédiadaEscalade Esperanc¸adeHerthfoi18,40.Nosostomizadosqueconviviamcomoestomahaviamenos de4anosasmédiasdasEscalasdeEsperanc¸adeHerth,Self-ratingScaleforSpirituality,e EscalaparaLocusdeControledaSaúdeforamde17,39,20,35,e23,09,respectivamente. Conclusão: ospacientesostomizadosacreditamquepodemcontrolarsuasaúdeequeas pessoasenvolvidasnocuidadoenasuareabilitac¸ãopodemcontribuirparasuamelhora.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Whenthepatientissubjectedtoanostomyandgoesthrough asurgicalprocedure,thephysicianperformsthe externaliza-tionofaholloworgansuchasthebowelorbladder,througha holeintheabdomen,calledstoma.1–3Thisprocedureiscarried
outinordertomaintaintheeliminationfunction,provoking variouschanges,amongwhichwecanhighlighttheremoval ofgases,odorsandfecesthroughthestomathatislocatedon theabdomen.Thus,thereisachangeinbodyimage,sexuality andinthewayofdressing,affectinginterpersonal relation-shipsandimpactingnegativelyonthephysical,psychological, socialandsexualhealthoftheindividualwhomustlivewith thislifecondition.2–5
Thesechanges that occur inthe dailylifeofostomized people,andeventhepsychosocial,emotionalandbiological changes,mayleadthese individualsto alossofcontrolof eliminationand to theneed touse ofcollectorequipment forfecesand/orurine,whichcausesachangeinthe individ-ual’sbody image.Thus,aconstant feararises,ofnotbeing abletoresumetheactivitiesofdailylivingpriortothestoma, withconsequent socialisolation, anegativefinancial com-mitment,andpsychologicaldistress.Giventhissituation,the patientoftenloseshis/herfaithandhopetogetabetterhealth, becomingdoubtfulastowhetherhe/shewillbeableto per-formself-care,especiallyintermsofstomacleaningandbag exchanging.1,6–11
Oftenthepatientendsuphavingachangeinhis/her reli-giousness,losingfaithandanyhopeofcureorimprovement, forfearofnotbeingabletodoself-care,includingcleaningthe
peristomal skinand exchangingand cleaningthe bag.This fact has,asaconsequence,changes inqualityoflife, self-esteem, spirituality,self-image,sexuality, familyand social lifeandleisureactivities.
Spiritualitycanbedefinedasabeliefsystemthatincludes intangibleelementsthatconveyvitalityandmeaningtolife events.Suchabeliefcanmobilizeextremelypositiveenergies andinitiatives,withanunlimitedpotentialtoimprovethe per-son’squalityoflife.Religiouspeoplearephysicallyhealthier, havemorehealthfullifestyles andrequire lesshealthcare. Thereisanassociationbetweenspiritualityandhealth,which isprobablyvalidandpossiblycausal.Itisfullyrecognizedthat thehealthofindividualsisdeterminedbytheinteractionof physical,mental,socialandspiritualfactors.12,13
Hope is a state associated with a positive outlook for the future, a way to cope with the situation that one is experiencing,14,15 inwhichthe individualhasfaithand the
hope of his/her cure or improvement. Hope induces the individualtoactandgivesstrengthtosolveproblemsand con-frontations,suchasloss,tragedy,lonelinessandsuffering.16
Healthlocusofcontrolisasetofbeliefsthatindividuals layatthesourceofcontrolofusualbehaviorsoreventsthat occur to themselves or to the environment in which they areinserted,indicatingtheexistenceofacontrolof internal-externalreinforcement,withregardtothedegreetowhichthe individualbelievesthatthereinforcementsarecontingenton his/herconduct.17,18
reinforcementswouldbedependentontheactionofpowerful others(suchasfamily,teachersordoctors).Thesubjectswho believethatpowerfulotherscontroltheirlivescanact differ-ently,incomparisonwiththosewhobelievethattheevents oftheirlivesemergechaoticallyandunpredictably.19,20
Theevaluationofthehealthlocusofcontroland spiritu-alityandhopeofcurecanbecomeanessentialinstrumentin guidinghealthactionsforostomizedpeople,consideringthat thisprovidessubsidiesforabetterunderstandingofthe psy-chosocialandemotionalfactorsinvolvedwiththedifficulties oflivingwiththestomaandintheachievementofself-care.
Inacontextofcomplexityandproblemswithwhichthe ostomizedindividualmustdeal,thestudyofaspectsofhealth control,bytheindividual,abouthis/herspiritualityleveland hope ofcure willprovide relevant informationwhich may influencetheself-carebytheostomizedindividual,helping inhis/heracceptanceofbeinganostomizedpatientandin livingwiththestoma.Thus,thisstudyaimstoevaluate socio-demographicandclinicalfactorslinkedtopatientswithan intestinalstoma,correlatingthesefactorstothehealthlocus ofhealthcontrol,spirituality,andhopeofacure.
Methods
Thisisadescriptive,cross-sectionalanalyticalstudy. ThisstudywasconductedatthePoloofOstomized Peo-pleinthecityofPousoAlegre,MinasGerais.52patientswith intestinalstomawereincluded.
Theinclusion criteriawere age ≥18 years and being an intestinalstomacarrier,andexclusioncriteriawerepatients withdementia syndromesand other conditionsthat could preventthemfromunderstandingandansweringtothe ques-tionnaires.
DatawerecollectedafterapprovalbytheEthics Commit-teeonResearchoftheFaculdadedeCiênciasdaSaúde“Dr. JoseAntonioGarciaCoutinho”andaftertheFreeandInformed Consent Form was signed by the patient or his/her care-giver(opinionnumber:620462). Data werecollected bythe researchersthemselves. Theinclusion ofthepatientinthe studyfollowedtheorderofarrivalattheoutpatientclinic.The samplewasselectedinanon-probabilistic,byconvenience, way.
Fordatacollection,threequestionnaireswereapplied:first, aquestionnaireondemographicandstoma-relateddata;then theScaleforHealthLocusofControl;thethirdquestionnaire wastheHerthHopeScaleand,finally,theSelf-ratingScalefor Spirituality.Eachinterviewlastedapproximately25min.
TheScaleforHealthLocusofControlhasbeentranslated andvalidated forthePortugueselanguage.Theinstrument validation,afterapplicationinfoursamples,wasverifiedas to the reliability (internal consistency) through Cronbach’s alpha,andthevaluesfoundforthesubscaleswere: Internal-ityforhealth,0.62–0.71;Externality-chanceforhealth,0.51–0.78; andExternality-powerfulothers,0.62–0.67.Thisscaleconsists ofthreesubscales,each containingsixitemsregardingthe followingdimensions:Internalityforhealth(items1,6,8,12,13 and17),wherein thescoresreflectthe degreetowhichthe subjectbelievesthathe/shehimselfcontrolshis/herstateof health;externality-powerfulothersforhealth (items3,5,7,10,
14 and 18), wherein the scoresreflectthe degree towhich the subjectbelievesthatother persons orentities(doctors, nurses,friends,family,God,etc.)cancontrolhis/herhealth; andExternality-chanceforhealth(items2,4,9,11,15and16), in whichthe scoresindicate thedegree towhicha person believes that his/herhealth iscontrolled atrandom, with-outhis/herinterferenceortheinterferencefromotherpeople The scores for each dimension range from 1to 5; for the alternatives“Itotallyagree,”“Ipartiallyagree,”“Iam unde-cided,” “I partiallydisagree,” and “I strongly disagree,” the followingvaluesarerespectivelyadded:5,4,3,2,and1.The scoreobtainedforthedimensionswillbethesumoftheitems ofthesubscaleatissue.Thetotalvalueofitemsbelongingto eachofthethreesubscalesrepresentsthetotalscoreswith respecttothedimensionofthehealthlocusinquestion.The totalamountobtainedfromeachsubscalemayvarybetween6 and30andindicatesthatthehigherthevalue,thestrongerthe beliefinthisdimension.Thescaleispresentedinitsentirety, inwhichtheitemsofthesubscalesareinterleaved.14,21
The Escala da Esperanc¸a de Herth (EEH),that is, the Por-tuguese version of the Herth Hope Scale, is a tool which consistsof12itemswithatotalscoreof12–48points,with responsesproducedinaLikert-likescale,withscoresfrom1to 4pointsforeachoneoftheseitems.Thehigherthescore,the greaterthehope.Theitems3and6haveaninvertedscore.20,22
TheSelf-ratingScaleforSpiritualityisaself-report instru-ment consisting of six items that assess aspects of the individual’sspirituality.Respondentsmustmarkoneoffive optionsrangingfrom1–“Istronglyagree,”2–“Iagree,”3–“I partiallyagree,”4–“Idisagree,”and5–“Istronglydisagree;” and theanswersshouldbeproduced accordingtothe indi-vidual’sperceptionatthetimeofansweringthequestions. For itsuse,onemustsumupthepoints,whosetotalrange from 6to30.Todothis,onemustpreviouslyrecodify each itemofthisinstrument(forexample,ascore=5becomes1, 2becomes4,andsoon).Therecodedresponsesaresummed toproducethetotalscore,andthis,inturn,representsthe levelofspiritualguidance.Tomakeacomparisonofscores betweengroups,oneshouldworkwiththeaveragesobtained ineachgroup,applyinganappropriatestatisticaltesttocheck fordifferencesbetweenthem.Thesummingofitemsallows thereadingofscores,thatis,thehigherthescore,thehigher thelevelsofspiritualguidance.Theitemsinthisscalereferto adivineinterventioninthepatient’sdailylifeandthepractice ofreligiousrituals,likepraying.Thisscale,whichevaluates thelevelsofspirituality,wasvalidatedinBrazil.Thescale reli-abilitytestinvolvingthetwoscaleshadaCronbach’salpha coefficientof0.86,avaluewhichwasconsideredacceptable, whichvalidatesitsuseintheBraziliancontext.23,24
Results
Regardingsocio-demographicdata,forthe52ostomypatients seenatthePolo ofOstomized Patientsofthe cityofPouso Alegre,wefoundthat33(63.50%)werefemale,meanage67 years;35(67.40%)weremarried;34(65.40%)wereretiredand 40(76.90%)ofthepatientswereparticipantsattendingto sup-portgroupsorassociations.Astodatarelatedtothestoma,40 (76.90%)werearesultofneoplasia,44(84.60%)ofthemwere ofthe colostomy type,40(76.90%) werepermanent stomas havingadiameterbetween20and40mm,and39(75%)were two-piecedevices.Thirty-onepatients(51.70%)livedwiththe stomaforupto4years.
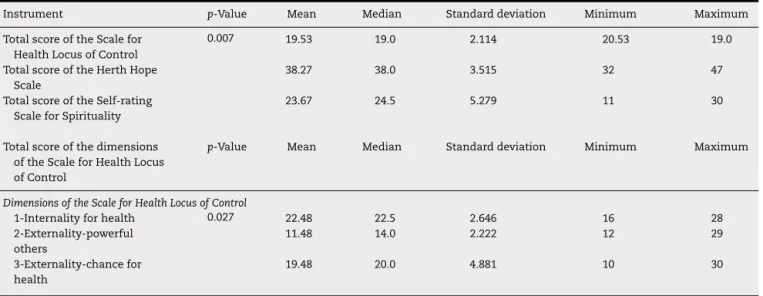
Table 1lists the means ofthe total score of the scales usedinthisstudy:fortheScaleforHealthLocusofControl, 19.53;fortheHerthHopeScale,38.27;andfortheSelf-rating ScaleforSpirituality,23.67,withdifferencestatistically signif-icant.RegardingthedimensionsoftheScaleforHealthLocus ofControl,changes inmean totalscorewerenotedforthe dimensionsExternality-chanceforhealth,11.48;and Externality-powerfulothers,19.48.Differencesstatisticallysignificantwere noted between dimensions. These findings imply that the individualswhoparticipatedinthestudydonotbelievethat professionalsorotherpeople involvedinthe carecan con-troltheir health;on theother hand,theybelievethat they themselves control their health. But they believe that the improvementofhealth ortheircurecan dependondivine intervention.
Table2liststhemeanofthetotalscoresoftheHerthHope Scale,Self-ratingScaleforSpirituality,andScaleforHealth LocusofControl.Withregardtosocio-demographicdata,the variablesthatshowedchangeswere:patientsagedupto50 years,withthefollowingmeans:HerthHopeScale:17:53,and Self-ratingScaleforSpirituality:19:33.Regardingmarital sta-tus,singlepeoplehadameanof21.00fortheHerthHopeScale.
Retired ostomizedpatients presentedthefollowingmeans: HerthHopeScale:20.53;Self-ratingScaleforSpirituality:10:38, andScaleforHealthLocusofControl:18.79.Thesefindings meanthatostomizedpatientswhoweresingle,retired,and agedupto50yearsdonotbelieveindivineinterventionto obtainimprovementorcure.Thestatisticaldifferenceswere mixed.However,retiredostomizedpatientsalsodonotbelieve thattheprofessionalsinvolvedinthecareoftheirhealthcan contributetotheirimprovement.
Table3liststhemeansofthedimensionsoftheScalefor HealthLocusofControlrelatedtosociodemographicvariables. Thedimensionsthatexhibitedchangeswere:forostomized patientsagedupto50years:Externality-powerfulothers,mean 18.73, and Externality-chance for health: 10.40. Also for the dimensionExternality-chanceforhealth,alterationswerefound inthemeansforthefollowingvariables:single(unmarried) patients:15.12;widowers,19.80;retirees,8.79;19.83.Changes inthemeanoccurredonlyinthedimensionExternality-chance forhealth.
Thesefindingsimplythatindividualsagedupto50years believethattheirimprovementorcuredependsonother peo-ple (family members, caregivers, health professionals) and onthemselves.Butsingle,widowed,unemployed,orretired ostomizedpatientsdonotbelievethattheirimprovementor curedepends onexternalassistance, orthat theremay be interferencefromothers(familymembers,caregivers,health professionals).
Table4liststhemeansofthetotalscoreoftheHerthHope Scale,Self-ratingScaleforSpirituality,and ScaleforHealth LocusofControlinrelationtointestinalstomadata.Variables thatshowedchangeswere:patientsforwhomthecauseof making the stomawas neoplasia,witha mean of19.43in theSelf-ratingScaleforSpirituality.Regardingthecharacter ofthestoma,themeanoftheHerthHopeScalewas18.40.For ostomizedpatientslivingwiththestomaforlessthan4years, themeanoftheHerthHopeScalewas17.39;Self-ratingScale
Table1–ResultsobtainedformeanscoresoftheScaleforHealthLocusofControl,HerthHopeScale,andSelf-rating ScaleforSpirituality,andthemeansoftheScaleofDimensionsforHealthLocusofControlinindividualswithintestinal stomaseenatthePoloofOstomizedPatientsofthecityofPousoAlegre.
Instrument p-Value Mean Median Standarddeviation Minimum Maximum TotalscoreoftheScalefor
HealthLocusofControl
0.007 19.53 19.0 2.114 20.53 19.0
TotalscoreoftheHerthHope Scale
38.27 38.0 3.515 32 47
TotalscoreoftheSelf-rating ScaleforSpirituality
23.67 24.5 5.279 11 30
Totalscoreofthedimensions oftheScaleforHealthLocus ofControl
p-Value Mean Median Standarddeviation Minimum Maximum
DimensionsoftheScaleforHealthLocusofControl
1-Internalityforhealth 0.027 22.48 22.5 2.646 16 28 2-Externality-powerful
others
11.48 14.0 2.222 12 29
3-Externality-chancefor health
19.48 20.0 4.881 10 30
Table2–MeansfortotalscoresoftheHerthHopeScale,Self-ratingScaleforSpirituality,andScaleforHealthLocusof Control,forthehealthlocusofcontrolrelatedtosocio-demographicdataofpatientswithintestinalstomaseenatthe PoloofOstomizedPatientsofthecityofPousoAlegre.
Instrument Agegroup
≤50years 51–69years >70years
Mean Median Standard deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-Value
HerthHopeScale 17.53 18.0 3.980 39.00 39.0 3.671 38.06 38.0 2.883 0.040a
Self-ratingScaleforSpirituality 19.33 20.0 7.355 24.20 25.0 4.312 25.12 25.0 3.426 0.010a
ScaleforHealthLocusof Control
30.60 30.0 8.798 63.05 64.5 6.581 63.29 64.0 8.809 0.581
Instrument Gender
Male Female
Mean Median Standarddeviation Mean Median Standarddeviation p-Value HerthHopeScale 21.84 22.0 2.588 22.85 23.0 2.647 0.808 Self-ratingScaleforSpirituality 22.79 22.0 3.809 19.15 18.0 4.280 0.027 TotallocusoftheScalefor
HealthLocusofControl
21.11 21.0 4.841 18.55 20.0 4.724 0.021a
Instrument Maritalstatus
Single Married Widow(er) Mean Median Standard
deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-Value
HerthHopeScale 21.00 28.0 8.725 23.77 25.0 7.999 61.78 64.0 7.480 0.017a
Self-ratingScaleforSpirituality 18.00 19.5 4.106 38.29 39.0 3.569 38.44 38.0 3.127 0.050a
TotallocusoftheScalefor HealthLocusofControl
20.25 22.0 6.964 63.11 63.0 5.042 26.33 25.0 2.739 0.967
Instrument Scholarship
Fundamentaleducationunfinished Fundamentaleducationcompleted
Mean Median Standarddeviation Mean Median Standarddeviation p-Value HerthHopeScale 24.04 24.0 7.183 23.25 25.0 8.854 0.533 Self-ratingScaleforSpirituality 37.86 38.0 3.274 38.75 39.5 3.791 0.366 TotallocusoftheScalefor
HealthLocusofControl
63.04 63.5 4.333 61.71 62.0 6.278 0.598
Instrument Occupation
Retiree Unemployed Working Mean Median Standard
deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-Value
HerthHopeScale 20.53 21.0 2.286 22.33 22.5 1.633 22.42 24.0 3.942 0.039a
Self-ratingScaleforSpirituality 10.38 12.0 4.192 21.33 23.0 4.457 20.33 19.5 5.416 0.023a
TotallocusoftheScalefor HealthLocusofControl
18.79 19.5 4.904 19.83 20.5 6.555 21.25 20.0 3.720 0.024a
Instrument Familyincome
≤3minimumwages >3minimumwages
Mean Median Standarddeviation Mean Median Standarddeviation p-Value HerthHopeScale 38.33 38.0 3.694 38.08 39.0 3.040 0.805 Self-ratingScaleforSpirituality 23.77 24.0 5.239 23.38 26.0 5.606 0.830 TotallocusoftheScalefor
HealthLocusofControl
61.03 61.0 7.607 66.62 66.0 7.719 0.027a
Pearson’sChi-squaredtest,Mann–WhitneytestandKruskal–Wallistest.
Table3–MeansofthedimensionsoftheScaleforHealthLocusofControl,relatedtosocio-demographicdataofpatients withintestinalstomaseenatthePoloofOstomizedPatientsinthecityofPousoAlegre.
Dimensions Agegroup
≤50years 51–69years >70years
Mean Median Standard deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-Value
IHLC–Internalityforhealth 22.53 23.0 3.114 22.65 23.0 2.815 22.24 22.0 2.078 0.893 POLC–Externality-powerfulothers 18.73 19.0 5.092 20.50 19.0 3.777 21.41 22.0 4.823 0.041a
CHLC–Externality-chancefor health
10.40 08.0 2.867 19.90 20.0 4.128 19.65 21.0 5.678 0.778
Dimensions Gender
Male Female
Mean Median Standarddeviation Mean Median Standarddeviation p-Value IHLC–Internalityforhealth 21.84 22.0 2.588 22.85 23.0 2.647 0.189 POLC–Externality-powerfulothers 22.79 22.0 3.809 18.55 20.0 4.724 0.003a
CHLC–Externality-chancefor health
21.11 21.0 4.841 11.15 09.0 2.280 0.050a
Dimensions Maritalstatus
Single Married Widow(er) Mean Median Standard
deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-Value
IHLC–Internalityforhealth 23.13 23.5 1.885 22.54 22.0 2.894 21.67 21.0 2.179 0.519 POLC–Externality-powerfulothers 20.00 19.0 5.155 20.77 20.0 4.492 19.78 19.0 3.962 0.798 CHLC–Externality-chancefor
health
15.12 14.5 4.970 19.80 20.0 4.928 20.33 22.0 4.500 0.17a
Dimensions Scholarship
Fundamentaleducationunfinished Fundamentaleducationcompleted
Mean Median Standarddeviation Mean Median Standarddeviation p-Value IHLC–Internalityforhealth 22.36 22.0 2.376 22.63 23.0 2.975 0.720 POLC–Externality-powerfulothers 20.61 19.0 3.775 20.33 20.5 5.198 0.827 CHLC–Externality-chancefor
health
20.07 21.0 5.099 14.79 18.0 4.625 0.013a
Dimensions Occupation
Retiree Unemployed Working Mean Median Standard
deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-value
IHLC–Internalityforhealth 22.53 22.0 2.286 22.33 22.5 1.633 22.42 24.0 3.942 0.982 POLC–Externality-powerfulothers 20.38 19.0 4.192 21.33 23.0 4.457 20.33 19.5 5.416 0.886 CHLC–Externality-chancefor
health
8.79 9.5 1.904 19.83 20.5 6.555 21.25 20.0 3.720 0.327
Dimensions Familyincome
≤3minimumwages >3minimumwages
Mean Median Standarddeviation Mean Median Standarddeviation p-Value IHLC–Internalityforhealth 22.18 22.0 2.713 23.38 23.0 2.293 0.157 POLC–Externality-powerfulothers 19.64 19.0 3.983 23.00 22.0 4.950 0.017a
CHLC–Externality-chancefor health
19.23 20.0 4.826 13.23 11.0 3.166 0.040a
Pearson’sChi-squaredtest,Mann–WhitneytestandKruskal–Wallistest.
Table4–MeansfortheHerthHopeScale,Self-ratingScaleforSpirituality,andScaleforHealthLocusofControl,related toostomydataofpatientswithintestinalstomaseenatthePoloofOstomizedPatientsinthecityofPousoAlegre.
Instrument Causeofmakingthestoma
Neoplasia Other
Mean Median Standarddeviation Mean Median Standarddeviation p-Value ScaleforHealthLocusofControl 62.33 63.0 7.816 62.75 63.0 8.709 0.873 HerthHopeScale 38.55 39.0 3.441 37.33 37.0 3.750 0.298 Self-ratingScaleforSpirituality 19.43 20.5 4.540 21.17 23.0 6.873 0.006a
Stomatype
Colostomy Ileostomy
Mean Median Standarddeviation Mean Median Standarddeviation p-Value ScaleforLocusofHealthControl 62.84 64.0 7.971 60.13 60.0 7.900 0.379 HerthHopeScale 38.52 38.5 3.084 36.88 35.5 5.384 0.423 Self-ratingScaleforSpirituality 24.23 25.0 4.974 20.63 20.0 6.209 0.076
Stomacharacter
Definitive Temporary
Mean Median Standarddeviation Mean Median Standarddeviation p-Value ScaleforHealthLocusofControl 62.85 64.0 8.285 61.00 62.0 6.809 0.932 HerthHopeScale 18.40 318.0 3.828 37.83 38.5 2.250 0.021a
Self-ratingScaleforSpirituality 20.45 22.0 4.260 21.08 21.0 7.440 0.033a
Instrument Stomadiameter
0–20mm 20–40mm 40–80mm Mean Median Standard
deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-Value
ScaleforHealthLocusofControl 64.08 62.0 9.634 63.26 64.0 7.025 59.15 59.0 7.766 0.224 HerthHopeScale 37.17 37.0 2.623 39.37 40.0 3.564 37.00 36.0 3.606 0.049a
Self-ratingScaleforSpirituality 21.42 23.0 6.788 24.78 25.0 4.627 23.46 23.0 4.684 0.047a
Instrument Devicetype
One-piecedevice Two-piecedevice
Mean Median Standarddeviation Mean Median Standarddeviation p-Value ScaleforHealthLocusofControl 60.85 63.0 5.713 62.95 64.0 8.559 0.709 HerthHopeScale 36.92 38.0 2.629 38.72 39.0 3.685 0.112 Self-ratingScaleforSpirituality 24.15 26.0 5.786 23.51 24.0 5.170 0.401
Stomatime(years)(groups)
>4years 4–7years 8–11years 12–21years MeanMedian Standard
deviation
MeanMedian Standard deviation
MeanMedian Standard deviation
MeanMedian Standard deviation
p-Value
ScaleforHealthLocusofControl23.09 25.0 8.224 62.46 64.0 6.173 64.13 64.0 10.316 64.50 64.5 0.011a
HerthHopeScale 17.39 18.0 3.513 38.54 38.0 2.989 38.75 39.5 2.550 39.88 39.5 0.017a
Self-ratingScaleforSpirituality 20.35 21.0 6.087 27.00 28.0 3.291 25.50 26.0 3.162 23.13 23.0 0.032a
Instrument Participationinsupportassociationorgroup
Yes No
Mean Median Standarddeviation Mean Median Standarddeviation p-Value ScaleforHealthLocusofControl 20.63 19.545 8.002 61.75 19.0 8.058 0.041a
HerthHopeScale 38.03 38.0 3.214 19.08 08.5 4.441 0.030a
Self-ratingScaleforSpirituality 30.60 30.0 08.798 17.25 O9.0 2.751 0.011a
Pearson’sChi-squaredtest,Mann–WhitneytestandKruskal–Wallistest.
forSpirituality,20.35;andScaleforHealthLocusofControl, 23.09.For those patients whodid notparticipateina sup-portassociationorgroup,themeanswere:fortheHerthHope Scale,19.08;fortheSelf-ratingScaleforSpirituality,17.25;and fortheScaleforHealthLocusofControl,20.63.
Differencesstatisticallysignificantwereobservedinthese variables. Ostomized patients whose cause of making the stomawasneoplasia(inthevariable“characterofthestoma”), those who lived with the injury for less than 4 years and thatdidnotattendtoanassociationorsupportgroup,donot believethattheirimprovementorcuredependsonthehelpof others,orthattheremaybeinterferencefromothers(family members,caregivers,healthprofessionals),and alsodonot believeintheinterventionofGodandhavenohopethatthey willimproveorobtainacure.Table5showsthemeanofthe dimensionsoftheScaleforHealthLocusofControlrelevant tothevariables pertainingtotheintestinalstoma,and one canseethatonlythedimensionExternality-chanceforhealth presentedchanges.Theostomizedpatientswhosecauseof themakingoftheostomywasneoplasiahadameanof9.78; peoplewithanileostomyhadameanof11.38,andforthose withatemporarystoma,themeanwas7.33.Patientsliving withthe stomafrom 4to7 yearshad a mean of8.65.For those ostomizedpatients who did notattend toa support associationorgroup,themeanwas19.37.Therewere statis-ticaldifferencesbetweenthevariables.Thesefindingsmean thatostomizedsubjectsdonotbelievethattheirimprovement orcuredependsonexternalassistance,orthattheremaybe interferencefromothers(familymembers,caregivers,health professionals).
Discussion
Regardingthesocio-demographiccharacterization,therewas apredominanceoffemaleostomizedpatients,withamean ageof67years,married,retiredandwhodidnotparticipate insupportgroupsorassociations,whichisinlinewithother studiesinvolvingpatientswithanintestinalstoma.1,4–6,9–11
Withrespecttodatarelatedtothe stoma,inthe major-ityofpatients,thecauseofmakingthestomawasneoplasia, theirstomawasofcolostomytype,withapermanentstoma measuringbetween20 and40mmofdiameterandusing a two-piecedevice.Mostindividualslived withthestomafor upto4years.Thesefindingscorroboratetheresultsofseveral studies.1,4,5,11
Inthis study,thepatientsevaluatedhadmeanscoresof the Scale forHealth Locusof Control. For the dimensions Externality-chanceforhealthandExternality-powerfulothers,the scoreswerelow.WithrespecttothemeanoftheHerthHope Scaleand Self-ratingScaleforSpirituality, thescores were normal.
Bycomparingsociodemographicandstomadatawiththe useoftheinstrumentsScaleforHealthLocusofControl,Herth HopeScale,andSelf-ratingScaleforSpirituality,onecansee thattherewerechangesandstatisticalsignificanceinthe fol-lowingvariables:agegroup,female gender,singlessubjects andretirees,and thecause ofmakingthe stomawas neo-plasia,with the use ofapermanent stoma, livingwith an ostomyforuptofouryears,andnotparticipatinginsupport
associationorgroup.Thesefindingsimplythattheindividuals whoparticipatedinthisstudydonotbelievethatprofessionals orpeopleinvolvedinthecarecancontroltheirhealthstatus, andalsodonotbelieveindivineintervention;ontheother hand,theybelievethattheythemselvescontroltheirhealth.
The health locus of control is a model that questions whetherthebeliefoftheindividual,i.e.,his/hermotivation (internal and external) determines the action to betaken. Thosewhobelievethattheresults,atleastinpart,are depend-entontheactionstaken,areconsideredinternallyoriented; those who follow an externalorientation generally donot believeordonotstronglybelieveintheexternalrelationof theoutcomeandoftheindividualaction.25Thebeliefs
influ-encepeoplewithastomaintheperceptionandexpression ofhopeinthetheirimprovementorcure,couragetoperform self-care,couragetoreactandtofightagainstprejudiceand stigmathattheirwillfaceintheirday-to-daylives,andhowto dealwithsuchasituationintheconvivialitywithastomized humanbeing.26–28
Spirituality and religion are related to each other, but althoughtheseconceptsareoftenusedinterchangeably,they donotsharethe samecharacteristics.Spiritualityis some-thingbroaderand morepersonal, andisrelatedtoasetof innervalues,innerwholeness,harmony,andconnectionwith others;itstimulatesaninterestinothersandinourselvesand looksforaunitywithlife,nature,andtheuniverse.Spirituality iswhatgivesmeaningtolife,regardlessofone’sreligion,and thus,generates thecapacity toendure debilitatingfeelings ofguilt,anger,andanxiety;furthermore,spiritualistaspects can mobilize positive energies and improve the quality of life.29,30Whenitcomestoostomizedpeople,spiritualitycan
becontemplatedasoneofthecopingresourcesinperforming self-careandrehabilitation.
Inonestudy,itsauthorsreportthatoneofthewaysof cop-ingwiththediseaseandwithdeathisdirectlylinkedtothe intensityoffaithandreligiousbeliefs–thatis,waysof express-ingspirituality.Theauthorsconcludedthatoneofthewaysof copingwithadverseandfavorablesituationsisfoundinthe feelingoffaithinGod.FaithinGodisadeep-seatedfeelingin ourcultureandisasnecessaryastheotherwaysofcoping31;
thediscourseshowsthatthespiritualdimensionoccupiesa prominentplaceinostomizedpeople’slivesandalsoshows thatitisessentialtobeawareofthespiritualityoftheusers toplananursingcareandtheguidanceofself-care.
Inastudywheretheauthorsevaluatedtheroleofnurses intherehabilitationprocessofostomizedpatients,itwas con-cludedthattheprocessofrehabilitationofthesepeople,when designedina holisticand systematicmanner,through the applicationoftheNursingProcess,becomesatoolthat pro-motesthereturntoactivitiesofdailyliving,includingwork,as itisatthispointthattheguidelinesrelatedtoself-carewith thestomaandperistomalskinwillbeimplemented,showing totheuserthathe/shecanlivewithoutseveretensionswith his/herstoma.Itisnoteworthythatonlyaftertheadjustment ofthestomizedindividualtohis/hernewconditionoflifeis thathe/shewillacquireconfidenceandsecuritytoreturnto workandsocialactivities.32
Table5–MeanofdimensionsoftheScaleforLocusofHealthControlrelatedtoostomydataofpatientswithintestinal stomaseenatthePoloofOstomizedPatientsofthecityofPousoAlegre.
Instrument Stomacause
Neoplasia Other
Mean Median Standarddeviation Mean Median Standarddeviation p-Value IHLC–Internalityforhealth 22.17 22.0 2.827 23.50 24.0 1.624 0.049a
POLC–Externality-powerful others
20.38 19.5 4.418 20.83 21.5 4.707 0.757
CHLC–Externality-chance forhealth
09.78 20.0 4.764 21.88 19.899 5.351 0.433
Instrument Stomatype
Colostomy Ileostomy
Mean Median Standarddeviation Mean Median Standarddeviation p-Value IHLC–Internalityforhealth 22.50 22.5 2.732 22.38 22.5 2.264 0.904 POLC–Externality-powerful
others
20.84 20.0 4.398 18.50 17.5 4.440 0.173
CHLC–Externality-chance forhealth
19.50 20.0 4.934 11.38 13.120 3.897 0.048a
Instrument Stomacharacter
Definitive Temporary
Mean Median Standarddeviation Mean Median Standarddeviation p-Value IHLC–Internalityforhealth 22.55 22.5 2.689 22.25 22.5 2.598 0.734 POLC–Externality-powerful
others
20.17 19.5 4.361 21.50 20.5 4.758 0.370
CHLC–Externality-chance forhealth
20.13 20.0 4.936 07.33 06.5 4.185 0.052a
Instrument Stomadiameter
0–20mm 20–40mm 40–80mm Mean Median Standard
deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-Value
IHLC–Internalityforhealth 22.83 23.0 2.691 21.96 22.0 2.738 23.23 23.0 2.351 0.324 POLC–Externality-powerful
others
20.67 19.5 5.630 20.26 20.0 4.053 20.77 19.0 4.362 0.934
CHLC–Externality-chance forhealth
20.58 19.5 5.265 21.07 21.0 3.668 15.15 14.0 4.413 0.006a
Instrument Devicetype
One-piecedevice Two-piecedevice
Mean Median Standarddeviation Mean Median Standarddeviation p-Value IHLC–Internalityforhealth 23.00 23.0 2.614 22.31 22.0 2.667 0.419 POLC–Externality-powerful
others
20.15 19.0 4.375 20.59 20.0 4.517 0.763
CHLC–Externality-chance forhealth
Table5–(Continued)
Stomatime
<4years 4–7years 8–11years 12–21years Mean Median Standard
deviation
MeanMedian Standard deviation
Mean Median Standard deviation
Mean Median Standard deviation
p-Value
IHLC–Internalityforhealth22.13 22.0 2.616 23.00 24.0 3.240 21.75 22.0 2.053 23.38 24.0 2.200 0.500 POLC–Externality-powerful
others
20.35 19.0 5.219 19.23 19.0 3.632 22.12 21.0 4.291 21.25 21.5 3.240 0.509
CHLC–Externality-chance forhealth
08.65 09.0 3.628 20.23 20.0 4.285 20.25 21.0 6.861 19.88 20.5 4.853 0.013a
Participationinsupportassociationorgroup
Yes No
Mean Median Standarddeviation Mean Median Standarddeviation p-Value IHLC–Internalityforhealth 22.68 23.0 2.759 21.83 21.0 2.209 0.338 POLC–Externality-powerful
others
20.60 20.0 4.528 20.08 18.5 4.316 0.728
CHLC–Externality-chance forhealth
22.48 22.5 2.646 19.37 20.0 5.097
Pearson’sChi-squaredtest,Mann–WhitneytestandKruskal–Wallistest.
a Statisticalsignificancep≤0.05.
aspectsinvolvedinthe recoveryofthis typeofclient. The teachingofself-care,understoodasthefirststepinthe reha-bilitationprocess,shouldalsogoverntheguidelinesaimedat the recoveryofself-esteem ofthepatients, reinforcing the importanceofsocialinclusionintheirlives.Thus,withthe helpofthenursingstaff andfamily,ostomizedpeoplemay seekabetterqualityoflife,eveninthepresenceofastoma, whentheseindividualswillrealizethattheycanreturntothe multipleactivitiesofdailyliving,pursuingtheirlifeplans.33
Spiritualitycontributestothewell-beingofostomized peo-ple,favoringtheirresilienceinthesuccessofself-careand rehabilitation.Certainreligious andspiritual behaviorsand beliefsaredirectlyrelatedtooverallhappinessandphysical health,consideringthattheydiscourage anengagementin unhealthybehaviors. Throughthis study,weconcludethat ostomizedpatientsbelievethatcancontroltheirhealthand thatthosepeopleinvolvedintheircareandrehabilitationcan contributetotheirimprovement.Theyconsiderthatthecure orimprovementisunderthedivineinfluencethrough reli-giouspracticesorbeliefs.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MotaMS,GomesGC,PetucoVM,HeckRM,BarrosEJ,Gomes VL.Facilitatorsofthetransitionprocessfortheself-careof thepersonwithstoma:subsidiesforNursing.RevEscEnferm USP.2015:82–8.
2. AngSG,ChenHC,SiahRJ,EleHG,Klainin-YobasP.Stressors relatingtopatientpsychologicalhealthfollowingstoma surgery:anintegratedliteraturereview.RevOncolFórum Enferm.2013:587–94.
3.AltschulerA,RamirezM,GrantM,WendelC,HornbrookMC, HerrintonL,etal.Theinfluenceofhusbands‘ormale partners’supportonwomen’spsychosocialadjustmentto havinganostomyresultingfromcolorectalcancer.JWound OstomyContinenceNurs.2009:299–305.
4.SaloméGM,AlmeidaSA.Associationofsociodemographic andclinicalfactorswiththeself-imageandself-esteemof individualswithintestinalstoma.JColoproctol.2014: 159–66.
5.SaloméGM,AlmeidaSA,SilveiraMM.Qualityoflifeand self-esteemofpatientswithintestinalstoma.JColoproctol. 2014:231–9.
6.MongeRA,AvelarMCQ.Assistênciadeenfermagemaos pacientescomestomiaintestinal:percepc¸ãodosenfermeiros. OnlineBrazJNurs.2009:45–52.
7.MauricioVC,SouzaNVDO,LisboaMTL.Determinantes biopsicossociaisdoprocessodeinclusãolaboraldapessoa estomizada.RevBrasEnferm.2014:415–21.
8.SaloméGM,CarvalhoMRF,MassahudMR,MendesB.Profileof ostomypatientsresidinginPousoAlegrecity.JColoproctol. 2015:106–12.
9.SaloméGM,SantosLF,CabeceiraHS,PanzaAMM,PaulaMAB. Knowledgeofundergraduatenursingcourseteachersonthe preventionandcareofperistomalskin.JColoproctol. 2014:224–30.
10.CostaVF,AlvesSG,EufrásioC,SalomeGM,FerreiraLM.Body imageandsubjectivewell-beinginostomistsinBrazil. GastrointestNurs.2014:37–47.
11.MotaM,GomesGC.Changesintheprocessoflivingof ostomizedpatientsaftersurgery.JNursUFPE.2013:7074–81. 12.SaloméGM,AlmeidaSA,MendesB,CarvalhoMRF,Junior
MRM.Assessmentofsubjectivewell-beingandqualityoflife inpatientswithintestinalstoma.JColoproctol.2015:168–74. 13.SaloméGM,AlmeidaAS,FerreiraLM.Associationof
sociodemographicfactorswithhopeforcure,religiosity,and spiritualityinpatientswithvenousulcers.AdvSkinWound Care.2015:76–82.
15.JakobssonA,Segestenk,NordholmL,OreslandS.
Establishingaswedishinstrumentmeasuringhope.ScandJ CaringSCI.1993:135–9.
16.HerthK.Abbreviatedinstrumenttomeasurehope: developmentandpsychometricevaluation.JAdvNurs. 1992:1251–9.
17.HaslamSA,ReicherS.Stressingthegroup:socialidentityand theunfoldingdynamicsofresponsestostress.JApplPsychol. 2006:1037–52.
18.RotterJB.Internalversusexternalcontrolofreinforcement:a casehistoryofvariable.AmPsycholAssoc.1990:489–93. 19.LevensonH.Activismandpowerfulothers:distinctions
withintheconceptofinternal-externalcontrol.JPersAssess. 1974:377–83.
20.SartoreAC,GrossiSAA.Herthhopeindex:instrument adaptedandvalidatedtoportuguese.RevEscEnfermUsp. 2008:227–32.
21.Rodríguez-RoseroJE,FerrianiMGC,DelaCMF.Escaladelocus decontroledasaúde–MHLC:estudosdevalidac¸ão.Rev Latino-AmEnfermagem.2002:179–84.
22.BalsanelliACS,GrossiSAA,HerthK.Assessmentofhopein patientswithchronicillnessandtheirfamilyorcaregivers. RevActaPaulEnferm.2011:354–8.
23.GalanterM,DermatisH,BuntG,WilliamsC,TrujilloS. Assessmentofspiritualityanditsrelevancetoaddiction treatment.JSubstAbuseTreat.2007:257–64.
24.Gonc¸alvesMAS,PillonSC.Adaptac¸ãotransculturale avaliac¸ãodaconsistênciainternadaversãoemportuguêsda
SpiritualityRatingScale.RevPsiquiatrClín.2009: 10–5.
25.DelaCMF.Escalamultidimensionaldelocusdecontrolede Levenson.ArqBrasPsicol.1987:79–97.
26.SantanaJCB,deSouzaÂB,DutraBS.Percepc¸õesdeumgrupo deenfermeirassobreoprocessodocuidardepacientesde ostomiadefinitiva.JNursUFPE.2011:1710–5.
27.MartinsML,PeruginiVC,SilvaRDM.Processodevivercom estomia:facilidadeselimites.RevEstima.2006:15–20. 28.CascaisAFM,MartiniJG,AlmeidaPJS.Oimpactodaostomia
noprocessodeviverhumano.RevTextoContextoEnferm. 2007:163–7.
29.AaadM,MasieroD,BattistellaLR.Espiritualidadebaseadaem evidências.RevActaFisiátr.2001:107–12.
30.KuritaGP,PimentaCAM.Adesãoaotratamentodador crônicaeolocusdecontroledasaúde.RevEscEnfermUSP. 2004:254–61.
31.SaloméGM,PereiraVR,FerreiraLM.Spiritualityand subjectivewellbeingofpatientswithlower-limbulceration.J WoundCare.2013:230–6.
32.MauricioVC,OliveiraNVD,LisboaMTL.Thenurseandher participationintheprocessofrehabilitationoftheperson withastoma.RevEscAnnaNery.2013:416–22.