w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Therapeutic
itinerary
of
colorectal
cancer
patients
treated
in
the
state
of
Rio
Grande
do
Sul
夽
Eliara
Fernanda
Foletto
a,
Sabine
Elisa
Jackisch
a,
Marcelo
Luis
Dotto
b,
Cátia
Severo
b,
Emelin
Pappen
c,
Andreia
Rosane
de
Moura
Valim
c,
Jane
Dagmar
Pollo
Renner
c,
Lia
Gonc¸alves
Possuelo
c,∗aDepartmentofBiologyandPharmacy,UniversidadedeSantaCruzdoSul,SantaCruzdoSul,RS,Brazil
bIntegratedOncologyCenter,HospitalAnaNery,SantaCruzdoSul,RS,Brazil
cPost-GraduatePrograminHealthPromotion,UniversidadedeSantaCruzdoSul,SantaCruzdoSul,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19May2015 Accepted25March2016 Availableonline14April2016
Keywords:
Colorectalcancer Epidemiology Cancerstaging
a
b
s
t
r
a
c
t
Objectives: Theobjectiveofthestudywastoevaluatethetherapeuticitineraryofpatients treatedinaspecializedcenter,includingitstrajectoryinseekingtreatmentandtheirclinical andepidemiologicalcharacteristics.
Methods:Thisisacross-sectionalprospectivedescriptivestudy;patientswithcolorectal canceragedover18yearsandwhosignedtheconsentformwereincludedintheanalysis. Tumorcharacteristics,suchasstagingandtumorfeatures;epidemiologicalcharacteristics suchasage,gender,professionanditineraryintheformofthenumberofclinicalvisits neededtoobtainthediagnosis;themainsymptoms;andmeantimebetweendiagnosisand onsetoftreatmentwereevaluated.
Results:34%ofpatientsinitiallysoughtprimarycare(firstlevelofcareinthepublichealth system)and50%werediagnosedinsecondarycare(secondlevelofcareinthepublichealth system);themeannumberofvisitsuntilobtainingadiagnosiswas2.5times;and52%of patientsreceivedpalliativetherapyand40%hadastageIVdiagnosis.
Conclusions: Themeantimebetweenthediagnosisandtheonsetoftreatmentisinline withtherecommendationsoftheMinistryofHealthofBrazil.However,itwasfoundthat thepatientsareunawareofthesymptomsofthedisease,sincethemeantimebetweenthe onsetofsymptomsuntilthedecisiontovisitthedoctorwas177days–whichmayhave beenadeterminingfactorforadiagnosisinanadvancedstageofdisease.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
ThestudywasconductedattheGraduatePrograminHealthPromotion,UniversidadedeSantaCruzdoSul,SantaCruzdoSul,RS, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.G.Possuelo). http://dx.doi.org/10.1016/j.jcol.2016.03.008
Itinerário
terapêutico
de
pacientes
com
câncer
colorretal
tratados
no
interior
do
Rio
Grande
do
Sul
Palavras-chave:
Neoplasiascolorretais Epidemiologia
Estadiamentodeneoplasia
r
e
s
u
m
o
Objetivos: Oobjetivodoestudofoiavaliaroitinerárioterapêuticodepacientestratados emumcentroespecializado,compreendendosuatrajetórianabuscadotratamentoeas característicasclínicaseepidemiológicas.
Métodos: estudodescritivoprospectivotransversal;foramincluídosnaanálisepacientes portadoresdecâncercolorretal(CCR)maioresde18anosqueassinaramotermode con-sentimento.Foramavaliadascaracterísticastumorais,comoestadiamentoecaracterísticas dotumor;característicasepidemiológicascomoidade,sexoeprofissãoeatrajetóriacomo númerodeconsultasatéodiagnóstico,principaissintomasetempomédioentreo diag-nósticoeiníciodotratamento.
Resultados: 34%dospacientesprocuraraminicialmenteaatenc¸ãoprimária(primeironível deatenc¸ãonasaúdepública),50%receberamodiagnósticonaatenc¸ãosecundária(segundo níveldeatenc¸ãonasaúdepública),amédiadeconsultasatéodiagnósticofoide2,5vezes, 52%dospacientesfizeramterapiapaliativae40%fizeramdiagnósticoemestádioIV.
Conclusões: otempomédioentreodiagnósticoeoiníciodotratamentoestádeacordo comorecomendadopeloMinistériodaSaúdedoBrasil;entretanto,identificou-sequeos pacientesdesconhecemossintomasdadoenc¸a,umavezqueamédiadetempoentreo iníciodossintomasatéatomadadedecisãodeprocurarummédicofoide177dias,oque podetersidodeterminanteparaumdiagnósticonafaseavanc¸adadadoenc¸a.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este éumartigoOpenAccesssobalicençadeCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Colorectalcancer(CRC)isthethirdmostcommonmalignancy inhumans.Thisdiseaseisconsideredaseriouspublichealth problembecauseofitshugesocioeconomicimpacton soci-etyandbyrequiringanindividualized,long,exhaustingand expensivetreatment.Thelowincomeandlackofhealth poli-ciestoalertthepopulationarecrucialforanearlydiagnosis.1
Asto2014,theNationalCancerInstitute(INCA)estimated theoccurrenceof32,600newcases,15,070inmenand17,530 inwomen,accountingfor15.44newcasesper100,000menand 17.24newcasesper100,000women.IntheSouthregion,CRC isthethirdmostcommoncancerinmen(20.43/100,000)and thesecondmostcommoninwomen(21.85/100,000).In2011, 14,016deaths(6818menand7198women)wererecordedin Brazil.2
Thesealarmingdatacanbedirectlyrelatedtoalate diagno-sisofthediseaseandmainlyrelatedtothedifficultytoofferan adequatecare.Thetherapeuticitineraryisawaytoknowthe trajectoryofthediseaseprocessinseekingmedicalattention insuchawaythatthepatientandhis/herfamilycan under-stand.Inhealthcareservicesdifficultiescanariseinthefield oforganization,whichisabarriertotheprovisionofamore effectivecareforpatients.3
Understanding of the timing and how individuals seek healthcareisawaytoorganizeandevaluatehealthsystems withaviewtoconductingaplanningofthecriticalpoints.4
Studies involvingknowledgeofthetherapeuticitinerary of patientswithCRCareextremelyimportant,butsuchpapers arestillscarce.5
Basedondataintheliteratureandinthefaceofthefew studies publishedonthis topicinoncology,the aimofthis study was to evaluatethe therapeuticitinerary ofpatients withCRCtreatedinaspecializedcenter,asawayto under-standthetrajectoryofeachpatientandhis/herclinicaland epidemiologicalcharacteristics.
Methodology
Thisisaprospective,descriptivecross-sectionalstudywhich was conductedattheIntegrated OncologyCenter,Hospital AnaNery,locatedinSanta CruzdoSul/RS.Thishospitalis a referenceincancertreatmentbythe UnifiedHealth Sys-tem(SistemaUnificadodeSaúde–SUS),anditsdatabaseis connectedtotheNationalCancerInstitute(INCA).The hos-pitalcovers about 820,000people inthe regionsofValedo Rio Pardo, Central Serra, and Carbonífera. On average, the IntegratedOncologyCenterserves950chemotherapypatients (94% bySUS). Inradiotherapy, the Center servesabout 100 patientspermonth(84.7%SUS).Thedatacollectionbeganin November2012andwascompletedinApril2014.Thisstudy wasapprovedbytheResearchEthicsCommittee(CEP)ofthe UniversidadedeSantaCruzdoSul.
status (accompanied/unaccompanied), diabetes (yes/no), familyhistoryofCRC(yes/no),familyhistoryofothertypes of cancer (yes/no), time between onset of symptoms and the first health service sought (days), type of health care servicesoughtforthefirstconsultation(primary,secondary or tertiary care), number ofmedical visitsto establish the diagnosis,andservicewherethe diagnosiswas carriedout (primary, secondary or tertiary care).During the interview, thepatientswereinformedthatthedatawouldbeusedfor scientificresearch,withoutanypersonalreturn.
Inadditiontotheinterview,areviewofmedicalrecords wasperformed.Thedatafrommedicalrecordswereevaluated andtranscribedtoadatacollectionformpreviouslyprepared. Inthemedicalrecords,weevaluatedtheprimarysiteof dis-ease(colon/rectum),dateofonsetoftreatmentandstageof developmentaccordingtotheTNMclassification,issuedby theInternationalUnionforCancerControl(UICC), whereT referstotheextentofthetumor,Ntotheabsenceorpresence ofmetastasesinregionallymphnodes,andMtotheabsence orpresenceofdistantmetastases.Addingnumberstoeachof thoseletterscanalsoindicatetheextentofmalignancy.6
Statistical
analysis
Allinformationwasencodedand storedanonymouslyina databasecreatedforthispurpose.Clinicaland epidemiolog-icaldatawere storedinadatabase createdinthe software Statistical Package for Social Sciences (SPSS), version 20.0 (SPSSInc.,Chicago,IL)forstatisticalanalysis.Ourresultswere describedusingdescriptivestatistics(absolutenumbers, fre-quenciesandmeans).
Results
Intotal,50subjectsparticipatedinthisstudy,withamean ageof56(±12.7)years.Table1liststheepidemiological char-acteristicsofthepatients. Itwas foundthatmostpatients were Caucasian and had a family income ofup to3 min-imumwages.Amongtheprofessions citedbypatients,the mostfrequentwereagriculture(Table1).
Regarding the tests for the diagnosis of CRC, 38 (76%) participantshad neverbeen submittedto,ordidnotknow, colonoscopy.48%hadneverbeenscreenedforoccultbloodin thestool.
Table1–Epidemiologicalcharacteristicsofpatientswith colorectalcancer.
Characteristic n◦ %
Malegender 28 56
Whiteskincolor 39 78
Income(upto3minimumwages) 48 96
Profession(farmers) 19 38
Maritalstatus(accompanied) 36 72
FamilyhistoryofCRC 09 18
Familyhistoryofothertypesofcancer 22 44
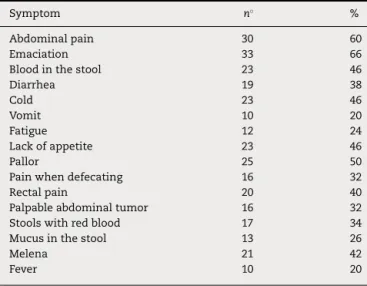
Table2–Symptomsthatledourpatientstoseekhealth care.
Symptom n◦ %
Abdominalpain 30 60
Emaciation 33 66
Bloodinthestool 23 46
Diarrhea 19 38
Cold 23 46
Vomit 10 20
Fatigue 12 24
Lackofappetite 23 46
Pallor 25 50
Painwhendefecating 16 32
Rectalpain 20 40
Palpableabdominaltumor 16 32
Stoolswithredblood 17 34
Mucusinthestool 13 26
Melena 21 42
Fever 10 20
Amongthesymptomscausingthevisitofpatientstothe healthservice,abdominalpain,andweightlosswerethemost frequentlycited(Table2).
Themeantimebetweentheonsetofsymptomsandthe decisiontoseekahealthservicewas177±336.88days, ran-gingfrom2to2160daysandwithamedianof60days.On average,eachpatientvisitedthedoctoratleast2.5(±0.6)times betweentheinitialconsultationandtheestablishmentofthe diagnosis.Themeantimebetweenthefirstconsultationwith thechemotherapyserviceandtheonsetoftreatmentwas32 (±33.0)days.Amongthepatientsstudied,13(26%)werebeing medicatedsimultaneouslywithradiotherapyand chemother-apy.
InFig. 1, onecanseethe firsttypeofservicesoughtby patientsaftermakingthedecisiontoseekadoctor.Regarding theserviceresponsibleforthediagnosisofcancer,itwasfound thatin50%ofcasesthisdiagnosiswasconfirmedina sec-ondarycareservice.Fig.2showsthetrajectoryofeachpatient. InTable3,thecharacteristicsrelatedtothetumorandthe typeoftreatment.52%ofpatientsreceivedpalliativetherapy and40%werediagnosedwithastageIVcancer.
34%
34% 22%
10%
Primary care Secondary care Tertiary care Could not inform
17 visits
n=4
n=5
n=16
n=1 n=1
n=9
n=2 n=1 n=2
n=2 n=1 n=2 2 diagnoses
2 diagnoses
1 diagnoses 4 diagnoses
7 diagnoses
12 diagnoses
1 diagnoses
3 diagnoses
Primary attention Secondary attention Tertiary attention
2 diagnoses
1 diagnoses 1 diagnoses 1 diagnoses
1 diagnoses
1 diagnoses 1 diagnoses
n=1 n=1 n=2
n=1 n=8
17 visits
11 visits 2 diagnoses
Fig.2–TypeofservicesoughtinafirstvisitbypatientswithCRCafterthedecisiontoseekmedicalattention.
Table3–Clinicalcharacteristicsofpatients.
Characteristic n◦ %
Siteoftheprimarytumor–colon 32 64
Staging
II 16 32
III 13 26
IV 20 40
Purposeoftreatment
Previous 02 04
Adjuvant 21 42
Palliative 26 52
Withoutinformation 01 02
Pathology
Welldifferentiated 05 10
Moderatelydifferentiated 31 62
Poorlydifferentiated 02 04
Invasive 06 12
Noinformation 06 12
Discussion
CRCisa prevalentmalignancyworldwide,affectingmostly richcountries.InBrazil,thereisahighincidenceintheSouth andSoutheastregions,especiallyinolderindividualsandin males.7
In this study, the mean age was 56 years, which is in linewiththeliteraturefindings.8,9TheexactcauseofCRCis
unknown,butthereisstronginvolvementofgeneticand envi-ronmentalcharacteristics.10Currently,clinicalandbiological
factorshavebeenstudiedinordertobetterunderstandthe progressionofthedisease.11
Malignancies havebeenassociatedwiththe use of pes-ticides.Thechroniceffectofthesediseasesoccursthrough therespiratory,dermalanddigestivetract.Pesticideswhich present organochlorinatedcompoundsin theirformulation
areretainedintissues,andsomestudieshaveshownthatsuch agentsareassociatedwithmalignancies.12Inthisstudy,ahigh
prevalenceoffarmers(38%)diagnosedwithCRCwasobserved. Theregionswherethisstudywasconductedhavean econ-omybasedontobaccoandricefarming,whichexplainsthe high frequencyofindividualswho reportfarmingasa pro-fessional activity.AsdescribedinastudyconductedinSão Paulo,thesecondlargestrelatedprofessionalactivitywasalso agriculture.13
Inthisstudy,18%ofpatientsreportedafamilyhistoryof CRC.Thesefiguresareclosetothosefoundintheliterature, suggestingthatin20–25%ofcasesonecanobserveafamily componenttoCRC.14
We observed in this study that patients are not aware of preventive tests such as colonoscopy and fecal occult blood, since 76% of patients had never been submitted to colonoscopyand48%neverhadafecaloccultbloodtest.These figuresareworryingbecausethatmortalityfromCRCdecrease andthatthesurvivalofindividualsaffectedbythisdisease increase, conductingscreening testsare the mosteffective methods.14–16
Inourstudythemostfrequentsymptomswere abdomi-nalpain(60%)weightloss(66%)andbloodinthestool(46%), whichisinlinewiththefindingsdescribedbyEl-Halabietal. (2014).17Theseauthorsreportthatweightloss,obstruction,
occultbloodinthestool,abdominalpainandpalpable abdom-inalmassarecommoninallpatients.
These data are worrying, given that the most effective methodforreducingmortalityfromCRCandincreasing sur-vival of individuals affected by this disease is to perform screening tests.14 In addition to these tests, genetic tests
havebeendevelopedandusedaspredictiveandprognostic biomarkersforCRC.15,16
elapsedsincetheonsetofsymptomstothedecisiontoseek ahealthservicewas177(±336.88)days.Thisextendedtime isnotonlyduetoalackofknowledgeofpatients,butduring theirquestioningitwaspossibletoidentifytheprivatefears andanxieties,suchaslackoftime,overwork,thefearofa diag-nosiswithouthealingchancesandeventhesimplefactthat theyfeelthatcertainsymptomswouldbeconsiderednormal. Therefore,theculturalandsocialfactors,lifeexperiencesand beliefsmaketheseindividualsoptfordifferentwaystotryto solvetheirhealthproblems;thus,theymayresorttoa special-izedsupportortoself-treatment,resultinginadelayintheir demandformedicalhelpand,asaconsequence,withalate diagnosis.18Somestudieshaveshownthatsomepeople
con-sultthedoctorassoonasthefirstsignsandsymptomsofthe diseaseappear;ontheotherhand,otherpeoplewithsimilar symptomsdonotproceedinthismanner,becauseoffinancial difficultiestogetprofessionalhelp.19Thetimeelapsedsince
theonsetofsymptomsuntilthefirstconsultationiscritical, becausethetumorsalreadyareinanadvancedTstage.20The
resultofalatediagnosisisthepalliativechemotherapy,with thetumoralreadyinstageIV.
Inthisstudy,34%ofpatientshadtheirfirstconsultation inprimarycareand50%werediagnosedinsecondarycare, aftertwotothreevisitsonaverage.Thesedatashowthatthe healthsystemisnotafragmentedbody,andcan intercom-municatetopass alongthe informationofitsusers,which facilitatesthediagnosisafterthepatientmadethedecisionto seekmedicaladvice,asopposedtothefindingsdescribedin otherstudies,i.e.Mendeletal.(2010)21inwhichtheauthors
reporttheprecariousness ofpublichealthservices andthe lackofcommunicationofhealthnetworks.
Themeantimesincethefirstconsultationatthehealth serviceuntilthebeginningoftreatmentwas32days,which isinaccordance witha Brazilianlawapprovedin 2012for patientswithprovenmalignancy.Thislawestablishesthat everycancerpatientshouldreceivethefirsttreatmentwithin 60daysafterthediagnosisconfirmedbyamedicalreport.22
Intheirstudy,Arribasetal.(2014)23foundthatin78%of
thepatientsstudiedthe primarytumorsitewas thecolon, andthat32.92%ofpatientshadapathologyreportofa well-differentiatedtumor.Thetumorstageatdiagnosisiscrucialto determinethepurposeofthetreatment.24Isveryimportant
thatthedoctorisawareofthepathologyreport(tumor char-acteristics),becausethetumoractsasaprognosticmarker, orindicatesaworst(orbetter)result,regardlessoftreatment. Thus,onecanevaluateeachindividualandchoosean indi-vidualizedtherapy,accordingtothepathologicalfeatures.The biologicalbehaviorofthetumor,aswellasfactorsthatinduce angiogenesis,may beconsidered decisive in the choice of treatmentandinpredictingtheindividual’sresponse.25
Conclusion
Weconcludethathealthsystemsarenotfragmentedbecause, onaverageeachpatienthadtwovisits,anumberthatis con-sideredappropriate.Thisshowsthattheserviceswherethe studywascarriedoutwereabletocommunicatesothatthe patient hasa rapiddiagnosis.Patients are not knowledge-ableabout screeningtests; therefore, it isclearthe lackof
campaignswarningontheneedforanearlydiagnosisofCRC, sincethemeantimebetweentheonsetofsymptomsandthe decisiontovisitadoctorwasof177days–andthismayhave beendecisiveforalowperspectiveofcure,consideringthat 40% ofsubjectswere instage IVand52% were referredto palliativechemotherapy.
Funding
Fundac¸ão de Amparo à Pesquisa do Rio Grande do Sul (FAPERGS).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WeareindebtedtoFundac¸ãodeAmparoàPesquisadoRio GrandedoSul(FAPERGS)forthefunding.
r
e
f
e
r
e
n
c
e
s
1.BrambillaE,PonteMD,RuschelLG,BosiHR,BragaGLD,Silva PGD.Stagingofcolorectalcancerintheprivateserviceversus BrazilianNationalPublicHealthSystem:whathaschanged afterfiveyears.JColoproctol.2012;32:144–7.
2.InstitutoNacionaldoCâncer(INCA).Availableat:
http://www2.inca.gov.br/wps/wcm/connect/tiposdecancer/ site/home/colorretal/definicao[accessed20.10.14]. 3.MufatoLF,AraújoLFSD,BellatoR,NepomucenoMAS.
Mediac¸ãonasredesparaocuidadodepessoaefamíliaque vivenciaocâncercolorretal.TextoContexto–Enferm. 2013;22:407–15.
4.CabralALLV,Martinez-HemáezA,AndradeEIG,Cherchiglia ML.Itineráriosterapêuticos:oestadodaartedaproduc¸ão científicanoBrasil.CiêncSaúdeColet.2011;16:4433–42. 5.NevesRDF,NunesMDO.Dalegitimac¸ãoa(res)significac¸ão:o
itinerárioterapêuticodetrabalhadorescomLER/DORT.Ciênc SaúdeColet.2010;15:211–20.
6.InstitutoNacionaldoCâncer.UICC.Availableat:
http://www1.inca.gov.br/tratamento/tnm/[accessed05.04.15]. 7.EisenhardtMF,HuweF,DottoML,SeveroC,FontellaJJ,Valim
ARDM,etal.Clinicalandepidemiologicalevaluationof patientswithcolorectalcancerfromRioGrandedoSul.J Coloproctol(RioJ).2012;32:136–43.
8.GuimaraesRM,RochaPGM,MuziCD,RamosRDS.Increase incomeandmortalityofcolorrectalcancerinBrazil, 2001–2009.ArqGastroenterol.2013;50:64–9. 9.MagajiBA,MoyFM,RoslaniAC,LawCW.Descriptive
epidemiologyofcolorectalcancerinUniversityMalaya MedicalCentre,2001to2010.APJCP.2014;15:6059–64. 10.IsidroRA,CruzML,IsidroAA,BaezA,ArroyoA,
Gonzalez-MarquesWA,etal.Immunohistochemical
expressionofSP-NK-1R-EGFRpathwayandVDRincolonic inflammationandneoplasia.WJG.2015;21:1749–58. 11.AnsolinPA,AlexandreCOP,DaminDC.Analysisofthe
polymorphicgenesGSTM1,GSTT1andGSTP1inasampleof
colorectalcancerpatientsfromtheSouthofBrazil.RevBras OncolClín.2010;7:12–7.
agrotóxicos?Umacontribuic¸ãoaodebate.CiêncSaúdeColet. 2010;15:277–88.
13.FernandesGMDM,LemeCVD,Ruiz-CintraMT,PavarinoÉC, NetinhoJG,Goloni-BertolloEM.Clinicalandepidemiological evaluationofpatientswithsporadiccolorectalcancer.J Coloproctol.2014;34:216–23.
14.Mirpuri-MirpuriPG,Alvarez-CordovesMM,Perez-MonjeA. Screeningprogramfortheearlydiagnosisofcolorectalcancer intheCanaryIslands:presentationofacase.Semer.
2013;39:71–4.
15.CastellsA.Theusefulnessoffecaltestsincolorectalcancer screening.GastroenterolHepatol.2014;37:71–6.
16.CubiellaJ,CastroI,HernandezV,Gonzalez-MaoC,RiveraC, IglesiasF,etal.Characteristicsofadenomasdetectedbyfecal immunochemicaltestincolorectalcancerscreening.Cancer EpidemiolBiomark.2014;23:1884–92.
17.El-HalabiMM,ChaabanSA,MeouchyJ,PageS,SalyersWJJr. Coloncancermetastasistomediastinallymphnodeswithout liverorlunginvolvement:acasereport.OncolLett.
2014;8:2221–4.
18.FundatoCT,PetrilliAS,DiasCG,GutiérrezMGR.Itinerário terapêuticodeadolescenteseadultosjovenscom osteossarcoma.BrasCancerol.2012;58:197–208.
19.VisentinA,LenardtMH.Oitinerárioterapêutico:históriaoral deidososcomcâncer.ActaPaulEnferm.2010;23:486–92.
20.OliveiraRG,FariaFF,LimaJuniorACB,RodriguesFG,Andrade MMA,GomesDMBM,etal.Cirurgianocâncercolorretal: abordagemcirúrgicade74pacientesdoSUSportadoresde câncercolorretalemprogramadepós-graduac¸ãolatosensu emcoloproctologia.RevBrasColoproctol.2011;31:44–57. 21.MendesEV.Asredesdeatenc¸ãoàsaúde.CiêncSaúdeColet.
2010;15:2297–305.
22.PresidênciadaRepublica,CasaCivil,Subchefiaparaassuntos jurídicos.Lein◦12.732,de22denovembrode2012.Dispõe
sobreoprimeirotratamentodepacientecomneoplasia malignacomprovadaeestabeleceprazoparaseuinício. Availableat:http://www.planalto.gov.br/ccivil03/
Ato2011-2014/2012/Lei/L12732.htm[accessed05.04.15]. 23.Arribas-MartinA,Diaz-Pizarro-GrafJI,Munoz-HinojosaJD,
Valdes-CastanedaA,Cruz-RamirezO,BertrandMM. Laparoscopicversusopensurgeryforcolorectalcancer.A comparativestudy.CirCir.2014;82:274–81.
24.HashimSM,FahTS,OmarK,RashidMR,ShahSA,SagapI. Knowledgeofcolorectalcanceramongpatientspresenting withrectalbleedinganditsassociationwithdelayinseeking medicaladvice.APJCP.2011;12:2007–11.
25.VolpatoMG,KochKDS.Fatoresdemauprognósticonaspec¸as operatóriasdepacientessubmetidosaotratamentocirúrgico docâncercolorretal.RevBrasColo-proctol(RioJ).