REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
MISCELLANEOUS
Translation
and
transcultural
adaptation
of
Pain
Quality
Assessment
Scale
(PQAS)
to
brazilian
version
夽
Anamada
Barros
Carvalho
a,b,c,∗,
João
Batista
Santos
Garcia
a,b,d,
Thayanne
Kelly
Muniz
Silva
b,
João
Victor
Fonseca
Ribeiro
baOutpatientChronicPain,HospitalUniversitáriodaUniversidadeFederaldoMaranhão(HU-UFMA),SãoLuís,MA,Brazil bLigaAcadêmicadeDorMaranhão,SãoLuís,MA,Brazil
cHealthSciences,UniversidadeFederaldoMaranhão(UFMA),SãoLuís,MA,Brazil
dDepartmentofAnesthesiologyPainandPalliativeCare,UniversidadeFederaldoMaranhão(UFMA),SãoLuís,MA,Brazil
Received9August2013;accepted30October2013 Availableonline26November2014
KEYWORDS
Neuropathy; Chemotherapy; Self-report instruments; Translation; Cross-cultural adaptation
Abstract
Introduction:Most cancer patients aretreated withchemotherapy, andperipheral neurop-athyisaseriousandcommonclinicalproblemaffectingpatientsundergoingcancertreatment. However,thesymptomsaresubjectiveandunderdiagnosedby healthprofessionals.Thus,it becomesnecessarytodevelopself-reportinstrumentstoovercomethislimitationandimprove thepatient’sperceptionabouthismedicalconditionortreatment.
Objective:TranslateandculturallyadapttheBrazilianversionofthePainQualityAssessment Scale,constitutingausefultoolforassessingthequalityofneuropathicpainincancerpatients. Method: Theprocedure followed thesteps oftranslation, back translation, analysisof Por-tugueseandEnglishversionsby acommitteeofjudges,andpretest.Pretestwas conducted with30cancerpatientsundergoingchemotherapyfollowinginternationallyrecommended stan-dards,andthefinalversionswerecomparedandevaluatedbyacommitteeofresearchersfrom BrazilandMAPIResearchTrust,thescale’screators.
Results:Versionsoneandtwo showed100%semanticequivalence withtheoriginalversion. Back-translationshoweddifferencebetweenthelinguistictranslationandtheoriginalversion. Afterevaluationbythecommitteeofjudges,aflawwasfound intheempiricalequivalence andidiomaticequivalence.Inpretest,twopeopledidnotunderstandtheitem12ofthescale, withoutinterferinginthefinalelaboration.
Conclusion:Thetranslatedandculturallyadaptedinstrumentisnowpresentedinthis publica-tion,andcurrentlyitisintheprocessofclinicalvalidationinBrazil.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
夽
Institution:InstitutoMaranhensedeOncologiaAldenoraBello.
∗Correspondingauthor.
E-mail:[email protected](A.B.Carvalho). http://dx.doi.org/10.1016/j.bjane.2013.10.018
PALAVRAS-CHAVE Neuropatia; Quimioterapia; Instrumentosde auto-relato; Traduc¸ão; Adaptac¸ão transcultural
Traduc¸ãoeadaptac¸ãotransculturaldaPainQualityAssessmentScale(PQAS)paraa
versãobrasileira
Resumo
Introduc¸ão: Amaioriadospacientescomcâncersãotratadoscomquimioterápicosea neu-ropatiaperiféricaéumproblemaclínicosérioecomumqueafetaospacientesemtratamento oncológico.Entretanto,taissintomassãosubjetivossendosubdiagnosticadopelosprofissionais desaúde.Assim,torna-senecessárioodesenvolvimentodeinstrumentosdeautorrelatopara superaressalimitac¸ãoemelhorarapercepc¸ãodopacientesobreoseutratamentooucondic¸ão clínica.
Objetivo: TraduzireadaptartransculturalmenteaversãobrasileiradoPainQualityAssessment Scale(PQAS),constituindoemuminstrumentoútildeavaliac¸ãodaqualidadedadorneuropática empacientescomcâncer.
Método: Oprocedimentoseguiuasetapasdetraduc¸ão,retrotraduc¸ão,análisedasversões por-tuguêseinglêsporumcomitêdejuízesepré-teste.Opré-testefoirealizadoem30pacientes com câncer em tratamento quimioterápico seguindo normas internacionalmente recomen-dadas,sendoasversõesfinaiscomparadaseavaliadasporcomitêdepesquisadoresbrasileiros edaMAPIResearchTrust,originadoresdaescala.
Resultados: Asversõesum edoisapresentaram100%deequivalênciasemânticacoma ver-sãooriginal.Naretrotraduc¸ãohouvediferenc¸asnatraduc¸ãolinguísticacomaversãooriginal. Apósaavaliac¸ãodoComitêdeJuízes,foiencontradaumafalhanaequivalênciaempíricaena equivalênciaidiomática.Nopré-teste,duaspessoasnãoentenderamoitem12daescala,sem interferirnaelaborac¸ãofinaldamesma.
Conclusão:Oinstrumentoagoratraduzidoeadaptadotransculturalmenteéapresentadonessa publicac¸ãoe,atualmente,encontra-seemprocessodevalidac¸ãoclínicanoBrasil.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Painfulexperiencesareexactlyalike.Peopleusetheword
‘pain’to describea wide varietyof sensations and
expe-riences arising from various etiologies Although the pain
intensity or magnitude is themost evaluated
characteris-ticonclinicalexperienceandscientificresearch,currently
weknowthatpeoplecanfeelthesamepainintensity,but
withdifferentqualities.1
Most cancer patients are treated with chemother-apy. Bone marrow suppression and renal and neurologic toxicity are the most common adverse events seen after the use of chemotherapeutic agents for treat-ing malignancies and the main reasons for anticancer treatment discontinuationor changing thetreatment reg-imen. The neurotoxicity, involving both the peripheral and the central nervous system, tends to occur early and persist even with the chemotherapy reduction or discontinuation.2---7
Currently, the interest in the subjective percep-tions of patients about the intensity and the effects of chemotherapy-induced peripheral neuropathy (CIPN) increased, and several self-report instruments are being developed to assess the patient’s perception of his/her treatmentormedicalcondition.4,6---11
Among the self-report instruments used in clinical practicethereisthePainQualityAssessmentScale(PQAS) (Fig. 1).PQAS is nonspecific for CIPN, but derives froma scale called Neurophatic Pain Scale (NPS). The NPS was developedtoassess distinctpainqualitiesassociatedwith neuropathicpain,thefirstinstrumentspecificallydesigned for this purpose.12 The scale includes two items that
assess the overall dimensions of intensity and intolera-ble pain, plus eight items in which specific qualities of neuropathicpain aredescribed as: ‘sharp’, ‘hot’,‘poorly localized,‘cold’,‘sensitiveasrawwound’,‘itchy’, ‘super-ficial’ and ‘deep’.12 Later, it was necessary to add 10
descriptors related to the quality of pain (‘sensitive as a wound’, ‘numbness’, ‘shocks’, ‘tingling’, ‘radiating’, ‘pounding’, ‘like a toothache’, ‘sting’, ‘cramp-like’, and ‘weight’type)increasingtheNPScontentvalidityandthree items related to the temporality of pain (‘constant with intermittent increases’, ‘intermittent’, or ‘constant with fluctuation’),whichwasusefultoevaluatebothneuropathic andnon-neuropathicpain;1,13---16thus,originatingthePQAS.
Althoughuseful,thisscalehasnotbeenvalidatedforBrazil yet.
Instrument selection
Compatibility of translations by the
researcher
Initial translation (V1+V2 = V3)
Two independent translators Compatibility of translations by the researcher Back-translation One back-translator
First translated version of the instrument (V4)
Expert committee review
Empirical and conceptual equivalence
Final version (V5)
Pretest (Proof technique in
30 patients) Semantic and idiomatic
equivalence
Figure1 Flowchartshowingthestepsoftranslationandcross-culturaladaptationofthePainQualityAssessmentScale(PQAS)at areferralhospitalforcancerinBrazil.
for assessing the quality of neuropathic pain in patients undergoingchemotherapy ina cancer referral public hos-pital.
Materials
and
methods
PQAScomprises20itemsofglobalassessmentofpain sever-ityanditsinconveniences,twospatialaspectsofpain,and 16differentqualitiesofpain.Althoughtheitemshave sim-ilarcharacteristicswithmorethanonemeasure,theirbest abilityistocapturethequalitiesordomainsaffectedbythe paintreatment. Each itemusesa verbalnumerical scale, inwhich0=nopainornosensationand10=theworstpain imaginable.Asmentionedabove,painisassessedusingtwo globaldomains(painseverityanddiscomfortcausedbyit), twospatialdomains(deeporsurface)and16qualitydomains (sharp,hot,poorlylocalized,cold,sensitiveasrawwound, ‘mosquito bite’, sting,numbness, shock, tingling, cramp, radiating,pounding,‘likeatoothache’,andweight). Addi-tionally,PQASalsohasanitemthatassessesthetemporal patternofpain(intermittentwithoutpainat othertimes, minimal painall the timewithexacerbation periods,and constant pain that does not change very much from one momenttoanother).1,13---16
PQAS translation and adaptation were performed fol-lowingtheinternationallyrecommendedstandards.17 PQAS
was translated into Portuguese by two Brazilians who are fluent in English and Portuguese, which generated two independent versions (V1 and V2). These two ver-sions were evaluated by the Brazilian researchers who developed a third version (V3). The third version was then subjected to back-translation into English, per-formed by a physician fluent in Portuguese and English, who was unaware of the original instrument and the translation purpose, which produced an English version (V4).17,18
experts’opinions,thefinal versionof theinstrument(V5) wasdeveloped.17,18
Thedecisionsmadebythiscommitteewerebasedonthe equivalencebetweenthesourceandtargetversioninfour aspects:
a) Semantic equivalence:knowingifthetranslatedwords havethesamemeaning;ifmultiplemeaningscomefrom aparticular item,andifthereweregrammatical diffi-cultiesintranslation.
b) Idiomaticequivalence:equivalentexpressionswere for-mulated in the target version, avoiding difficulties in translatingcolloquialismsandidioms.
c) EmpiricalEquivalence:termsinthequestionnairewere replacedbysimilartermswhichareusedinourculture oforigin,seekingtocapturedailylifeexperiences. d) Conceptual equivalence: it was observed if the words
had different meanings across cultures, replacing the inadequateterms.17---19
Consensuswasreachedonallitems,withthepresence ofalltranslatorsonthecommittee,providingagood under-standingimmediately.17,18
After choosing the final version (V5), the pre-test was conducted with 30 patients undergoing chemotherapy at a referral hospitalfor oncology inBrazil after signing the informedconsent.Theycompletedthequestionnaire,were askedwhattheythoughtofeachitem,andchoosethebest answer.17,18
Semanticequivalence wasperformedunderthe coordi-nationoftheMAPIResearchTrust,Lyon,France,researchers whodrafted the original PQASwiththe main investigator participation.
Results
The final Brazilian version of the PQAS resulted from the back-translationandexperts’reviewandisbeingsubmitted toanevaluationofitspsychometricpropertiesinanongoing studybythepainteamoftheUniversityHospital,areferral centerinBrazil.
During the preparationof the V1 and V2 versions, we observed 100% semantic agreement among translators. In item4, in whichwe asked howdull your painfeels?----the word‘‘dull’’wastranslatedas‘‘indefinida’’(undefined)on thesetwoversions,whichdidnotpersistaftertheexperts review.
Inback-translation,wesawdifferencesinlanguage trans-lationwiththeoriginalversion.Initem1,theword‘intense’ inthe originalwasback-translatedas‘severe’.In item2, ‘likeaspike’wasreplacedby‘likeaneedle’and‘themost sharp’by‘themostprickling’.Allotheritemsare summa-rizedinTable1.
Duringtheexpertcommitteeevaluation,therewereno differencesinsemanticandconceptualequivalence.As pre-viouslymentioned,theword‘dull’initem4wastranslated as‘undefined’inversions1and2.However,suchexpression wasjudgedashavinglittleinformationaboutthepatient’s painfulfeatureinournativelanguage,whichwasidentified asagapinempiricalequivalence.Thus,itwasreplacedby
Table1 Theback-translationprocessforPQAS. Originalscale Back-translatedscale
4/Dull. Difficultwastolocate yourpain.
7/Likeabruise. Likeawound. 8/Likepoisonivy. Likeatingle.
9/Zapping. Hooked.
13/Tight. Gripping.
15/Pounding. Pulsatile.
19/Howintenseisyour surfacepain?
Howintenseisyour shallowpain? 20/Ihavevariablepain
(backgroundpainall thetime,butalso momentsofmorepain orevensevere breakthroughpainor varyingtypesofpain).
Ihavevariablepainor evenwithmomentsof suddenlyseverepainor differentlevelsof intensityofpain.
PQAS,PainQualityAssessmentScale.
theterm‘poorlylocalized’,bestexemplifyingthis quality
ofpaininourregionalpopulation.
Theexpertsalsoidentifiedcolloquialismsandidiomsthat
couldinterferewiththecorrectdescriptionofthe quality
ofpaininourpopulation,suchasinitem1with‘nenhuma
dor’(nopainatall)inV1and‘semdor’(nopain)inV2,the
term‘semdor’(nopain)waschosenfor thefinalversion.
Thisfactresultsinachangeinidiomaticequivalence.After
completionof thisphase,version5of theinstrumentwas
generated.Tables2and3showtheotherterms.
Duringthepre-test,inwhichpatientsareaskedtochoose between the terms, only in item 12 two people did not choose becausethey did not understand the scale sense.
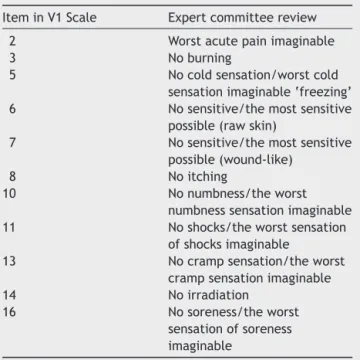
Table2 TermschosenforVersion1aftertheexpert com-mitteereview.
IteminV1Scale Expertcommitteereview
2 Worstacutepainimaginable
3 Noburning
5 Nocoldsensation/worstcold sensationimaginable‘freezing’ 6 Nosensitive/themostsensitive
possible(rawskin)
7 Nosensitive/themostsensitive possible(wound-like)
8 Noitching
10 Nonumbness/theworst
numbnesssensationimaginable 11 Noshocks/theworstsensation
ofshocksimaginable
13 Nocrampsensation/theworst crampsensationimaginable
14 Noirradiation
16 Nosoreness/theworst
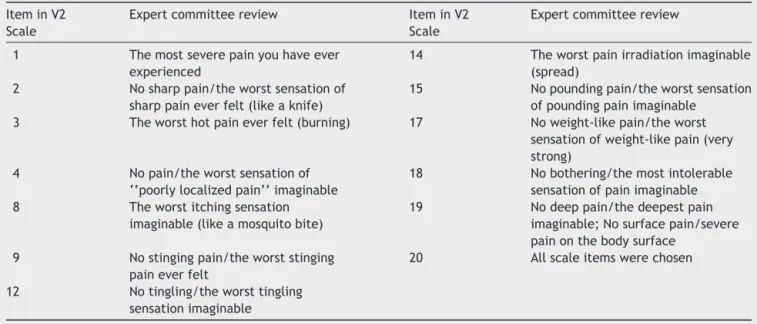
Table3 TermschoseninVersion2aftertheexpertcommitteereview. IteminV2
Scale
Expertcommitteereview IteminV2 Scale
Expertcommitteereview
1 Themostseverepainyouhaveever experienced
14 Theworstpainirradiationimaginable (spread)
2 Nosharppain/theworstsensationof sharppaineverfelt(likeaknife)
15 Nopoundingpain/theworstsensation ofpoundingpainimaginable
3 Theworsthotpaineverfelt(burning) 17 Noweight-likepain/theworst sensationofweight-likepain(very strong)
4 Nopain/theworstsensationof ‘‘poorlylocalizedpain’’imaginable
18 Nobothering/themostintolerable sensationofpainimaginable 8 Theworstitchingsensation
imaginable(likeamosquitobite)
19 Nodeeppain/thedeepestpain imaginable;Nosurfacepain/severe painonthebodysurface
9 Nostingingpain/theworststinging paineverfelt
20 Allscaleitemswerechosen
12 Notingling/theworsttingling sensationimaginable
Inotherterms,100%ofpatientsreportedunderstandingthe
itemschosenwithoutanydifficulty.
Despitethissmalldifference,theoriginatorsofthescale
decidedthattherewassemanticconcordancebetweenthe
twotranslations,andthatthe validationprocesscouldbe
started.
Discussion
Themainobjectiveofthisstudywasachievedwiththe
suc-cessfultranslationandcross-culturaladaptationofthePQAS
intoPortuguese.
Among the various adverse events resulting from
chemotherapy, CIPN remains the diagnosis in later stages
ofthe diseasewithmoderate toseveresymptoms of
sen-soryand/or motorneuropathy,whenthe qualityof lifeof
theseindividualsisalreadycompromisedbothphysicallyand
emotionally. Thus, we chose tovalidate the PQAS in this
populationofpatientswhooftenreporttingling,stingingor
burning,numbness,pinpricks andbilateral shock-like
sen-sationsinhandsandfeetassymptomsresultingfromCIPN
in early stages of the disease. Furthermore, the absence
ofa goldstandard instrumenttoidentifythisdisease
fur-therhinders anypossibilityof preventionandappropriate
treatment.10
Other studies, which compared the effects of differ-ent paintreatments for patients with similarqualities of pain,reported effects both similar and different for cer-tain qualities, depending on the studied population and treatment.1Onestudycomparedtheeffectsof5%lidocaine
patchwith corticoid injectionalone in carpal tunnel syn-drome (CTS). The results showed a decrease in tingling, numbness,unpleasantsensation,deepache, electric-like, intense,superficial,sharp,burning,andunpleasant sensa-tionsinbothtreatments,withgreatereffectsonpounding and numbness with the lidocaine patch9. In the group
of neuropathic pain patients with postherpetic neuralgia
anddiabetic neuropathy,a combinationof oxycodoneand pregabalinshowedsignificantimprovementinfreezingcold pain,although thecombinationof pregabalinandplacebo had improved burning and sharp pain.1 The results of
thesestudiessuggest theefficacyofvarious pharmacolog-ical treatments for certain qualities of pain in patients with specific diagnoses. Thus, the translation and cross-cultural adaptation of PQAsand itssubsequent validation willprovideausefultoolforthispurposeinourpopulation. The development of the V1 and V2 versions was not difficult.However,thephysicianwhoperformedthe back-translationreporteddifficultytofinishit,asherepresents adifferentspecialtyfromtheresearchedtopic,inaddition tothefactthatmanytermsthatrefertopainfulconditions arenoteasytoexpressexactlythequalityofthepainthe patientfeels.Thisgeneratedmorereliabilitytothisstage oftheresearch,astheback-translatedversionwasdeemed compatiblebytheoriginatorsofthescale.
Thepretestphaseisnecessaryforthecompletionofthe translation and cultural adaptation process of the scales. Duringthe study,itwasnecessary togivemore extensive explanationsofsometermsduetotheloweducationallevel ofthepopulationsurveyed.InastudyconductedinJapan,18
patientsreportedproblemsregardingtheunderstandingof items,somebeingconsideredirrelevant,divergingfromthis study wheresuch actionwasnot necessary.Therewasno problemwiththescalecreators’authorizationtostartthe process of its translation, cross-cultural adaptation, and validation.
terms, as most patients had a more elementary level of education. It was then possible to reduce the interview timeto8---10minuteswithout compromisingthe visittime and achieving patient satisfaction. However, it is known thatpatients have difficultyexpressingpainful symptoms, especiallywhentheyareassociatedwithCIPN.10 This may
explain the difficulty faced by patients to complete the questionnaire.
Althoughthereisnogoldstandardprocesstobestrictly followed byall researchersin ordertoperforma transla-tionandcross-culturaladaptation,threestepsareessential: translation/back-translation,expertcommitteereview,and pretest. All three steps in this study were rigorously monitored.18
Thus, the Brazilian version of PQAS is now translated andculturallyadaptedand,afteritsvalidation(currentlyin progressbythePainResearchGroupattheUniversity Hos-pital,areferralcenterinBrazil),itwillcertainlybeauseful toolforcliniciansandresearcherstoevaluatethesignsand symptomsofdifferentqualitiesofpain,neuropathicornot, helpingtoelucidate the painful mechanism, evaluatethe effectivenessoftreatmentofdifferentdiseases,and espe-ciallyintheearlydetectionofsensorysymptomsinpatients atriskofdevelopingmoreseriousstagesofCIPN.
Conflicts
of
interest
References
1.JensenMP,GalerBS,GammaitomiAR,etal.ThePainQuality AssessmentScale(PQAS)andRevisedPainQualityAssessment Scale(PQAS-R):ManualandUserGuide;2010.MapiResearch Trustwebsite(http://www.mapi-trust.org).
2.Quasthoff S, Hartung HP. Chemotherapy-induced peripheral neuropathy.JNeurol.2002;249:9---17[review].
3.Stillman M, Cata JP. Management of chemotherapy-induced peripheral neuropathy. Curr Pain Headache Rep. 2006;10: 279---87.
4.Cavaletti G, Marmiroli P. Chemotherapy-induced peripheral neurotoxicity.NatRevNeurol.2010;6:657---66.
5.WindebankAJ,GrisoldW.Chemotherapy-inducedneuropathy. JPeripherNervSyst.2008;13:27---46[review].
6.SmithEM, CohenJA,Pett MA,etal. Thevalidityof neurop-athyand neuropathic painmeasures in patientswithcancer receivingtaxanesandplatinums.OncolNursForum.2011;38: 133---42.
7.NaleschinskiD,BaronR,MiaskowskiC.Identificationand treat-mentof neuropathic pain inpatients withcancer. Pain Clin Updates.2012;XX.
8.Cavaletti G, Frigeni B, Lanzani F, et al. Chemotherapy-inducedperipheralneurotoxicityassessment:acriticalrevision of the currently available tools. Eur J Cancer. 2010;46: 479---94.
9.FerreiraKA,TeixeiraMJ,MendonzaTR,etal.Validationofbrief pain inventoryto Brazilianpatientswith pain.Support Care Cancer.2011;19:505---11.
10.SasaneM,TencerT,FrenchA,etal.Patient-reportedoutcomes inchemotherapy-induced peripheral neuropathy:a review.J SupportOncol.2010;8:E15---21.
11.FerreiraKASL,WilliamNWJr,MendonzaTRK,etal.Traduc¸ão paraa Língua PortuguesadoM.D.Anderson Symptom Inven-tory---headandneckmodule(MDASI-H&N).RevBrasCirCabec¸a Pescoc¸o.2008;37:109---13.
12.GalerBS,JensenMP.Developmentandpreliminaryvalidation ofapainmeasurespecifictoneuropathicpain:theneuropathic painscale.Neurology.1997;48:332---8.
13.JensenMP,GammaitoniAR,OlaleyeDO,etal.Thepainquality assessmentscale:assessmentofpainqualityincarpaltunnel syndrome.JPain.2006;11:823---32.
14.VictorTW,JensenMP,GammaitoniAR,etal.Thedimensions ofpainquality:factoranalysisofthepainqualityassessment scale.ClinJPain.2008;24:550---5.
15.Waterman C, Victor TW, Jensen MP, et al. The assessment of pain quality: an item response theory analysis. J Pain. 2010;11:273---9.
17.BeatonDE,BombardierC,GuilleminF,etal.Guidelinesforthe process ofcross-culturaladaptation ofself-report measures. Spine.2000;25:3186---91.
18.FumimotoH,KobayashiK,ChangC-HE,etal.Cross-cultural vali-dationofaninternationalquestionnaire,thegeneralmeasure
ofthefunctionalassessmentofcancertherapyscale(FACT-G), forJapanese.QualLifeRes.2001;10:701---9.