doi: 10.3389/fnint.2018.00027
Edited by: Timothy Roberts, Children’s Hospital of Philadelphia, United States Reviewed by: Lindsay M. Oberman, Uniformed Services University of the Health Sciences, United States Stephanie Ameis, Hospital for Sick Children, Canada *Correspondence: Albino J. Oliveira-Maia albino.maia@neuro.fchampalimaud.org Received:28 February 2018 Accepted:06 June 2018 Published:09 July 2018 Citation: Barahona-Corrêa JB, Velosa A, Chainho A, Lopes R and Oliveira-Maia AJ (2018) Repetitive Transcranial Magnetic Stimulation for Treatment of Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Front. Integr. Neurosci. 12:27. doi: 10.3389/fnint.2018.00027
Repetitive Transcranial Magnetic
Stimulation for Treatment of Autism
Spectrum Disorder: A Systematic
Review and Meta-Analysis
J. Bernardo Barahona-Corrêa1,2,3,4,5, Ana Velosa3, Ana Chainho6, Ricardo Lopes5,6and Albino J. Oliveira-Maia1,2,3,4*
1Champalimaud Clinical Centre, Champalimaud Centre for the Unknown, Lisbon, Portugal,2Champalimaud Research,
Champalimaud Centre for the Unknown, Lisbon, Portugal,3Department of Psychiatry and Mental Health, Centro Hospitalar
de Lisboa Ocidental, Lisbon, Portugal,4NOVA Medical School|Faculdade de Ciências Médicas, Universidade Nova de
Lisboa, Lisbon, Portugal,5CADIN–Neurodesenvolvimento e Inclusão, Cascais, Portugal,6Centro de Investigação e de
Intervenção Social (CIS-IUL), Instituto Universitário de Lisboa (ISCTE-IUL), Lisbon, Portugal
Background: Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder manifesting as lifelong deficits in social communication and interaction, as well as restricted repetitive behaviors, interests and activities. While there are no specific pharmacological or other physical treatments for autism, in recent years repetitive Transcranial Magnetic Stimulation (rTMS), a technique for non-invasive neuromodulation, has attracted interest due to potential therapeutic value. Here we report the results of a systematic literature review and meta-analysis on the use of rTMS to treat ASD.
Methods: We performed a systematic literature search on PubMed, Web of Science, Science Direct, Bielefeld Academic Search, and Educational Resources Information Clearinghouse. Search terms reflected diagnoses and treatment modalities of interest. Studies reporting use of rTMS to treat core ASD or cognitive symptoms in ASD were eligible. Two researchers performed article selection and data extraction independently, according to PRISMA guidelines. Changes in ASD clinical scores or in cognitive performance were the main outcomes. Random effects meta-analysis models were performed.
Results: We found 23 eligible reports, comprising 4 case-reports, 7 non-controlled clinical trials, and 12 controlled clinical trials, comparing the effects of real TMS with waiting-list controls (n = 6) or sham-treatment (n = 6). Meta-analyses showed a significant, but moderate, effect on repetitive and stereotyped behaviors, social behavior, and number of errors in executive function tasks, but not other outcomes. Most studies had a moderate to high risk of bias, mostly due to lack of subject- and evaluator-blinding to treatment allocation. Only 5 studies reported stability of these gains for periods of up 6 months, with descriptions that improvements were sustained over time.
Conclusions: Existing evidence supports that TMS could be useful to treat some dimensions of ASD. However, such evidence must be regarded with care, as most studies did not adequately control for placebo effects. Moreover, little is known regarding the most effective stimulation parameters, targets, and schedules. There is an urgent
need for further randomized, double-blind, sham-controlled trials, with adequate follow-up periods, to test the efficacy of transcranial magnetic stimulation to treat these disorders. Available evidence must be regarded as preliminary and insufficient, at present, to support offering TMS to treat ASD.
Keywords: autism, Asperger’s, non-invasive brain stimulation, TMS, rTMS, TBS, meta-analysis
INTRODUCTION
Rationale
Autism Spectrum Disorder (ASD) is a diagnostic category that encompasses a group of neurodevelopmental disorders with varying degrees of severity, sharing a common syndromatic core dyad of significant deficits in social communication and interaction, and repetitive behaviors with restricted interests and
activities (American Psychiatric Association, 2013; Volkmar and
McPartland, 2014). Deficits in communication can present as absent or severely impaired language development, and restricted interests can vary from extremely stereotyped, non-functional repetitive behavior, to milder forms of over-involvement or over-investment in a limited span of interests and activities (Volkmar and McPartland, 2014). Other features that are frequently associated include cognitive delay, epilepsy, and motor clumsiness, as well as significant psychiatric co-morbidity, such as obsessive-compulsive disorder, affective disorders, and
attention deficit and hyperactivity disorder (Stahlberg et al.,
2004; Russell et al., 2005; Hutton et al., 2008; Mouridsen et al.,
2008). Furthermore, ASD patients are impaired in a number
of neuropsychological tasks, namely theory of mind tests and tasks depending on executive functions such as working memory,
prepotent response inhibition or interference control (Kana et al.,
2015; Wallace et al., 2015; Geurts and Lever, 2017). ASD is a lifelong disorder, and most patients remain severely impaired in terms of psychosocial functioning throughout their adult lives (Billstedt et al., 2005; Farley et al., 2009). Currently there are important limitations in the treatment of ASD. Pharmacological treatment is only indicated for psychiatric comorbidity and has no measurable impact on ASD core manifestations. Available non-pharmacological interventions, on the other hand, are generally expensive, time-consuming and have modest results (Buescher et al., 2014).
In more recent years the availability of non-invasive neuromodulation techniques has raised hope that they might prove an effective tool in the treatment of ASD core
manifestations (Oberman and Enticott, 2015). Transcranial
Magnetic Stimulation (TMS) is a non-invasive neuromodulation technique that has attracted particular interest. TMS uses electromagnetic induction to generate transient, localized electrical fields in the brain cortex, causing depolarization and
firing of local neurons (Hallett, 2000). Repetitive TMS (rTMS)
Abbreviations:ASD, autism spectrum disorders; CI, confidence interval; cTBS, continuous theta burst stimulation; DLPFC, dorsolateral prefrontal cortex; DMPFC, dorsomedial prefrontal cortex; iTBS, intermittent theta burst stimulation; rTMS, repetitive transcranial magnetic stimulation; TMS, transcranial magnetic stimulation.
delivers patterns of multiple TMS pulses over a chosen brain area, at frequencies that typically vary between 0.5 Hz and 20 Hz (Pascual-Leone et al., 1999). At low frequencies, rTMS results in long-term suppression of cortical excitability on the target cortical tissue, while at frequencies above 5 Hz, rTMS mostly
induces long-term facilitation of cortical excitability (
Pascual-Leone et al., 1998). These effects, however, are subject to
significant inter-individual variability (Maeda et al., 2000). An
alternative modality of rTMS delivery is Theta-burst Stimulation (TBS), where TMS pulses are delivered in 50 Hz 3-pulse bursts, at 200 ms intervals (i.e., with a 5 Hz burst frequency). Continuous TBS (cTBS) suppresses cortical excitability, while intermittent TBS (iTBS), where TBS is delivered for 2 s every
10 s, has facilitatory effects on the cortex (Huang et al.,
2005).
Use of TMS in humans is generally safe and well tolerated, and rTMS has received formal approval for the treatment of
drug-resistant Major Depression (Rossi et al., 2009). For these
reasons, TMS has become an attractive treatment option in ASD, stimulating interest in particular among ASD patients and their parents, who are characteristically attentive to innovative
treatments (Levy and Hyman, 2005). Unfortunately, it remains
unsettled whether there is indeed a place for rTMS in the treatment arsenal for ASD. In a narrative review published
in 2016, Oberman et al. (2016) found 12 studies and three
case-reports describing the use of rTMS protocols in ASD
with therapeutic intent (Oberman et al., 2016). Stimulation
parameters and targets varied widely across studies, and most of them were open-label. The authors concluded that evidence for improvement of specific ASD-related behavioral symptoms resulting from rTMS applied to specific cortical regions, while encouraging, was limited. In fact, results at the individual level were mixed, and large-scale controlled trials were lacking. Here we describe an update of this work, 3 years after its initial online
publication. In further development of prior methods (Oberman
et al., 2016) we conducted a systematic review of the literature, for published reports on the therapeutic use of rTMS in patients with ASD. Furthermore, we performed meta-analyses of the data in these reports, thus offering the first estimation of pooled effects sizes for the effects of TMS on several clinical dimensions of ASD.
Objectives
While there are clinical programs offering rTMS to treat ASD symptoms, the evidence-base sustaining efficacy and safety in this context remains unclear. Moreover, the optimal stimulation parameters and brain targets remain undefined. Here we conducted a systematic literature review and meta-analysis to
explore available data regarding the therapeutic use of rTMS for ASD.
Research Question
We were interested in understanding whether the published literature supports use of TMS for amelioration of core-symptoms of ASD, or of the cognitive impairments associated with these disorders.
METHODS
Study Design
We conducted a systematic review of the literature with meta-analyses of studies reporting quantitative data, separated according to the outcome of interest.
Participants, Interventions, Comparators
We were interested in reviewing studies conducted in patients with any ASD, regardless of age or gender. Given the limitations in the available literature, we were interested in any clinical trial, regardless of design, as well as case-studies or case-series, reporting the effects of rTMS on ASD core symptoms and/or cognitive performance.Systematic Review Protocol
The systematic review was conducted according to a protocol following PRISMA guidelines.
Search Strategy
The search was performed on PubMed, Web of Science, BASE (Bielefeld Academic Search), ERIC (educational resources information clearinghouse) and Science Direct, between June 2016 and January 2018. Search terms reflected the diagnoses of interest (Autism, Autism Spectrum Disorders, Asperger) and the interventions of interest (Transcranial, TMS, rTMS, TBS).
After eliminating duplicates, two researchers reviewed the list of articles separately, selecting eligible reports according to PRISMA procedures. Articles in English, French, German, Portuguese or Spanish were considered, regardless of publication date or country of origin. Only full articles published in peer-review journals were considered. Literature reviews were excluded, but were screened for additional references, as were reference lists of eligible articles.
Data Sources, Studies Sections, and Data
Extraction
Two researchers extracted data separately according to PRISMA guidelines. From each eligible paper, whenever possible we extracted information separately for patients included in the active treatment and those in the control intervention arm, namely author, publication year and journal, number of participants, gender distribution, mean age, mean intelligence quotient, number of dropouts, type of TMS stimulation, stimulation parameters and target, stimulation schedule, behavioral outcome measures, cognitive outcome measures, number and nature of any reported side-effects, follow-up period duration, additional information. Risk of selection bias,
performance bias, attrition bias and detection bias were also
registered according to Cochrane guidelines (Higgins and Green,
2006).
For each outcome variable from each eligible study, depending on what was reported in the original paper, we extracted pre-treatment and post-pre-treatment mean and standard deviation, F-value from Analysis of Variance tests, and/or Cohen’s d estimates. If reported we also extracted mean change from baseline, standard deviation of this measure and/or paired t-test t-values. Data were extracted either directly from the text and tables or extrapolated from figures. In the latter situation values (mean and standard deviation or standard error of the mean) were extracted using Adobe Acrobat Reader measurement tools. To account for measurement error, each value from each figure was measured five times, and the mean value computed. In cases where data included in the original manuscript were insufficient, we contacted the corresponding author to request further information. Data is described in the manuscript as mean ± standard deviation. Original data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Data Analysis
To estimate effect-sizes we computed Hedges g
for each study, using Meta-essentials workbooks
( http://www.erim.eur.nl/research%7D-support/meta-essentials/). For controlled studies, computations were conducted using one of the following, according to what was reported: post-treatment means and standard deviations of both the active treatment and the control intervention groups, F-values from Analysis of Variance tests, or Cohen’s d estimates. When, instead of raw outcome data, authors reported mean change from baseline, within-group standard deviation for the outcome measures
was estimated using σ = σD
√
2(1−ρ), where σD stands for
the standard deviation of the difference relative to baseline, and ρ for the correlation between pre- and post-treatment
scores (Borenstein et al., 2009a). For non-controlled studies
a repeated measures approach was adopted for calculation of Hedges g, with use of either pre- and post-treatment means and standard deviations, or mean change from baseline, the
respective standard deviation (SD2D) and correlation coefficient
between pre- and post-treatment scores. When the latter was not provided we computed the correlation coefficient using the
formulas r = SDpre2+ SDpost2−SD2D
2 x SDpre x SDpost and SD2D = n(Mpost−Mpre)
2
t2
RM ,
where t2RM is the post paired t-test value, Mpre is the
pre-TMS mean score and Mpost the post-pre-TMS mean score (Morris
and DeShon, 2002). When reported data were insufficient for this computation, r-values were extrapolated from other papers with similar clinical populations, or, when this was not possible, from published data on the test-retest reliability of that specific measure.
Where a sufficient number of studies were available, results for relevant symptom dimensions or cognitive functions were included in random effects model meta-analyses, separately for controlled and uncontrolled studies. Controlled studies that did not report outcome data for the control group regarding
a specific clinical outcome dimension were entered in the corresponding meta-analysis of uncontrolled studies. For each meta-analysis, the decision to include any given study was essentially determined by the availability of sufficient quantitative data reporting treatment effects on the clinical dimension of interest. Due to the small number of available studies, study quality was not considered in the decision of inclusion. Meta-essentials workbooks 1, 3, and 4 were used to compute bias-adjusted standardized mean differences (Hedges g, expressed as 95% confidence intervals−95% CI), as well as combined effect sizes with hypothesis testing. Individual studies were weighed according to the inverse variance weighting method, with an added between-studies variance component based on
the DerSimonian-Laird estimator (Sánchez-Meca and
Marín-Martínez, 2008). Confidence intervals were estimated using the
weighted variance method, as described previously (
Sánchez-Meca and Marín-Martínez, 2008). This approach takes into account the uncertainty resulting from the need to estimate heterogeneity variance and within-study variances, resulting in wider estimated confidence intervals for the combined effect size in analyses based on small numbers of studies. In the latter situation, and especially when heterogeneity is high, confidence intervals may include 0 even when classical z-distribution confidence intervals would not. To assess heterogeneity of
studies, in each meta-analysis we used Cochrane’s Q-test to examine the null hypothesis that all studies estimated the
same effect. We further computed I2 to estimate the ratio
of true heterogeneity to total observed variation, and Tau2
(T2) to estimate between-study variance (Higgins et al., 2003).
Publication bias was examined by means of funnel-plots, with Egger regression and trim-and-fill analysis for estimation of the
adjusted effect size and of missing studies (Borenstein et al.,
2009b).
RESULTS
Study Selection and Characteristics
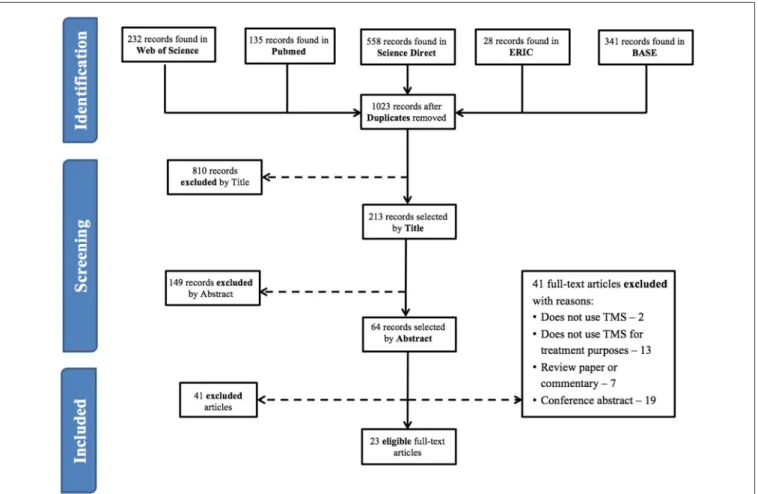
Figure 1 shows a flow diagram of the process leading to the identification of 23 eligible papers, using rTMS for therapeutic purposes in subjects with ASD (refer to Tables 1–3 for individual
study details). Four of these papers were case-reports (Enticott
et al., 2011; Niederhofer, 2012; Cristancho et al., 2014; Avirame et al., 2017), 7 were non-controlled trials (Sokhadze et al., 2010, 2016, 2017; Casanova et al., 2014; Wang et al., 2016; Abujadi et al., 2017; Gómez et al., 2017) and the remaining 12 were controlled
trials (Sokhadze et al., 2009, 2012, 2014a,b; Baruth et al., 2010;
Fecteau et al., 2011; Casanova et al., 2012; Enticott et al., 2012, 2014; Panerai et al., 2014; Anninos et al., 2016; Ni et al., 2017).
T A B L E 1 | S u m m a ry ta b le o f st u d y d e si g n , m o d a lit y o f T M S , re c ru ite d su b je c ts , a n d st u d y q u a lit y. S o u rc e T M S mo d a li ty E x p e ri me n ta l g ro u p C o n tr o l g ro u p C o n tr o l in te rv e n ti o n R is k o f s e le c ti o n B ia s R is k o f p e rfo rma n c e B ia s R is k o f a tt ri ti o n B ia s R is k o f d e te c ti o n B ia s N M e a n a g e (y e a rs ) In te ll e c tu a l a b il it y N M e a n a g e (y e a rs ) In te ll e c tu a l a b il it y A n n in o s e t a l., 2 0 1 6 P ic o te sl a T M S 1 0 (6 m a le ) 8 .3 ± 2 .1 N o t re p o rt e d S a m e g ro u p su b je c t to sh a m T M S L o w (r a n d o m iz e d o rd e r) L o w (d o u b le -b lin d ) L o w (n o d ro p o u ts ) L o w (d o u b le -b lin d ) B a ru th e t a l., 2 0 1 0 rT M S 1 6 1 3 .9 ± 5 .3 IQ = 8 6 ± 2 4 .7 9 A S D + 2 0 h e a lth y su b je c ts A S D : 1 3 .5 ± 2 ; h e a lth y su b je c ts : 1 5 .3 ± 5 .1 N o t re p o rt e d W a iti n g L is t L o w (r a n d o m iz e d ) H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) C a sa n o va e t a l., 2 0 1 2 rT M S 2 5 1 2 .9 ± 3 .1 IQ > 8 0 2 0 1 3 .1 ± 2 .2 IQ > 8 0 W a iti n g L is t L o w (r a n d o m iz e d ) H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) E n tic o tt e t a l., 2 0 1 2 rT M S 1 1 (1 0 m a le ) 1 7 .5 5 ± 4 .0 6 N o t re p o rt e d S a m e g ro u p su b je c t to sh a m T M S S h a m rT M S (le ft p rim a ry m o to r c o rt e x) L o w (r a n d o m iz e d o rd e r) H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) E n tic o tt e t a l., 2 0 1 4 D e e p rT M S 1 5 (1 3 m a le ) 3 3 .8 7 ± 1 3 .0 7 N o t re p o rt e d 1 3 a d u lts (1 0 m a le s) 3 0 .5 4 ± 9 .8 3 N o t re p o rt e d S h a m rT M S L o w (r a n d o m iz e d ) L o w (d o u b le -b lin d ) M o d e ra te (2 dro p o u ts ) L o w (e va lu a to r-b lin d e d ) F e c te a u e t a l., 2 0 1 1 rT M S 1 0 3 6 .6 ± 1 6 .0 IQ = 1 2 2 .4 ± 7 .2 1 0 h e a lth y c o n tr o ls ; sh a m rT M S in e xp e rim e n ta ls u b je c ts S h a m rT M S (c e n tr a l lo b e m id lin e ) L o w (p se u d o -ra n d o m iz e d , m u lti p le c ro ss o ve r) L o w (d o u b le -b lin d ) L o w (n o d ro p o u ts ) L o w (d o u b le -b lin d ) N ie t a l., 2 0 1 7 iT B S 1 9 (1 4 m a le ) 2 0 .8 ± 1 .4 IQ = 1 0 0 .5 ± 1 4 S a m e g ro u p su b je c t to sh a m iT B S S h a m iT B S (o ve r th e in io n ) L o w (r a n d o m iz e d o rd e r) H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) P a n e ra ie t a l., 2 0 1 4 ; S tu d y I rT M S 9 1 3 .5 6 ± 1 .8 3 S e ve re m e n ta l re ta rd a tio n S a m e g ro u p su b je c t to sh a m T M S S h a m T M S L o w (r a n d o m iz e d o rd e r) L o w (d o u b le -b lin d ) L o w (n o d ro p o u ts ) L o w (d o u b le -b lin d ) P a n e ra ie t a l., 2 0 1 4 ; S tu d y II rT M S H F rT M S : 6 ; L F rT M S : 6 H F rT M S : 1 3 .7 ± 1 .9 6 ; L F rT M S : 1 3 .3 3 ± 1 .8 8 S e ve re m e n ta l re ta rd a tio n 5 1 3 .2 4 ± 2 .9 5 S e ve re m e n ta l re ta rd a tio n S h a m T M S L o w (r a n d o m iz e d ) L o w (d o u b le -b lin d ) L o w (n o d ro p o u ts ) L o w (d o u b le -b lin d ) P a n e ra ie t a l., 2 0 1 4 ; S tu d y III rT M S 6 1 6 .1 3 ± 3 .1 1 S e ve re m e n ta l re ta rd a tio n S a m e g ro u p su b je c t to sh a m T M S S h a m T M S L o w (r a n d o m iz e d o rd e r) L o w (d o u b le -b lin d ) H ig h (2 d ro p o u ts ) L o w (d o u b le -b lin d ) (C o n tin u e d )
T A B L E 1 | C o n tin u e d S o u rc e T M S mo d a li ty E x p e ri me n ta l g ro u p C o n tr o l g ro u p C o n tr o l in te rv e n ti o n R is k o f s e le c ti o n B ia s R is k o f p e rfo rma n c e B ia s R is k o f a tt ri ti o n B ia s R is k o f d e te c ti o n B ia s N M e a n a g e (y e a rs ) In te ll e c tu a l a b il it y N M e a n a g e (y e a rs ) In te ll e c tu a l a b il it y P a n e ra ie t a l., 2 0 1 4 ; S tu d y IV rT M S H F rT M S : 4 ; H F rT M S+ E ye – h a n d in te g ra tio n tr a in in g : 4 H F rT M S : 1 2 .7 9 ± 2 .8 8 ; H F rT M S+ tr a in in g 1 3 .7 5 ± 5 .1 8 S e ve re m e n ta l re ta rd a tio n 5 1 4 .1 7 ± 4 .2 4 N o t re p o rt e d E ye –h a n d in te g ra tio n tr a in in g L o w (r a n d o m iz e d ) H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) S o kh a d ze e t a l., 2 0 0 9 rT M S 8 1 8 .3 ± 4 .8 IQ = 1 0 4 ± 1 9 .9 5 1 6 .2 ± 5 .7 IQ : 1 0 0 .8 ± 1 2 .4 W a iti n g L is t H ig h (n o t ra n d o m iz e d ) H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) S o kh a d ze e t a l., 2 0 1 2 rT M S 2 0 (1 6 m a le ) 1 3 .5 ± 2 .5 IQ = 9 0 .8 ± 1 5 .2 2 0 (1 6 m a le ) 1 3 .5 ± 2 .5 N o t re p o rt e d W a iti n g L is t H ig h (n o c o n c e a lm e n t, u n ra n d o m iz e d , u n p a ire d ) H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) S o kh a d ze e t a l., 2 0 1 4 b rT M S 2 0 1 4 .7 ± 3 .3 IQ > 8 0 2 2 1 4 .2 ± 2 .8 IQ > 8 0 W a iti n g L is t H ig h (n o c o n c e a lm e n t, u n ra n d o m iz e d , u n p a ire d ) H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) S o kh a d ze e t a l., 2 0 1 4 a rT M S 2 7 1 4 .8 ± 3 .2 IQ > 8 0 2 7 1 4 .1 ± 2 .6 IQ > 8 0 W a iti n g L is t H ig h (n o c o n c e a lm e n t, u n ra n d o m iz e d , u n p a ire d H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) S o kh a d ze e t a l., 2 0 1 6 rT M S 2 5 (1 9 m a le ) 1 3 .6 ± 3 .2 2 IQ > 8 0 2 1 h e a lth y c o n tr o ls 1 4 .9 ± 4 .3 N o t re p o rt e d N o c o n tr o l in te rv e n tio n N o t a p p lic a b le H ig h (u n b lin d e d ) M o d e ra te (2 dro p o u ts ) H ig h (u n b lin d e d ) A b u ja d ie t a l., 2 0 1 7 iT B S 1 0 (m a le ) 9 -1 7 IQ > 5 0 N o c o n tr o lg ro u p N o t a p p lic a b le H ig h (o p e n la b e l) L o w (n o d ro p o u ts ) H ig h (o p e n la b e l) C a sa n o va e t a l., 2 0 1 4 rT M S 1 8 (1 4 m a le ) 1 3 .1 ± 2 .2 IQ > 8 0 N o c o n tr o lg ro u p N o t a p p lic a b le H ig h (u n b lin d e d ) H ig h (2 d ro p o u ts ; 2 exc lu d e d ) H ig h (u n b lin d e d ) G ó m e z e t a l., 2 0 1 7 rT M S /t D C S 2 4 1 2 .2 (r T M S≥ 1 1 ;t D C S < 1 1 ) N o t re p o rt e d N o c o n tr o lg ro u p N o t a p p lic a b le H ig h (u n b lin d e d ) L o w (n o d ro p o u ts ) H ig h (u n b lin d e d ) (C o n tin u e d )
T A B L E 1 | C o n tin u e d S o u rc e T M S mo d a li ty E x p e ri me n ta l g ro u p C o n tr o l g ro u p C o n tr o l in te rv e n ti o n R is k o f s e le c ti o n B ia s R is k o f p e rfo rma n c e B ia s R is k o f a tt ri ti o n B ia s R is k o f d e te c ti o n B ia s N M e a n a g e (y e a rs ) In te ll e c tu a l a b il it y N M e a n a g e (y e a rs ) In te ll e c tu a l a b il it y S o kh a d ze e t a l., 2 0 1 0 rT M S 1 3 (1 2 m a le ) 1 5 .6 ± 5 .8 IQ = 9 4 .3 ± 1 6 .6 N o c o n tr o lg ro u p N o t a p p lic a b le H ig h (u n b lin d e d ) M o d e ra te (1 d ro p o u t) H ig h (u n b lin d e d ) S o kh a d ze e t a l., 2 0 1 7 rT M S 3 2 e n ro lle d ; fin a l sa m p le 2 7 (2 1 m a le ) 1 2 .5 2 ± 2 .8 5 IQ > 8 0 N o c o n tr o lg ro u p N o t a p p lic a b le H ig h (u n b lin d e d ) H ig h (3 d ro p u ts ; 2 c a se s e xc lu d e d ) H ig h (u n b lin d e d ) W a n g e t a l., 2 0 1 6 rT M S 3 3 (2 8 m a le ) 1 2 .8 8 ± 3 .7 6 IQ > 8 0 ; 1 0 h a d IQ 6 5 -7 9 N o c o n tr o lg ro u p N o t a p p lic a b le H ig h (u n b lin d e d ) M o d e ra te (3 dro p o u ts ) H ig h (u n b lin d e d ) A vi ra m e e t a l., 2 0 1 7 , c a se 1 D e e p T M S 1 (fe m a le ) 2 5 N o t re p o rt e d N o c o n tr o lg ro u p N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le A vi ra m e e t a l., 2 0 1 7 , c a se 2 D e e p T M S 1 (m a le ) 3 0 N o t re p o rt e d N o c o n tr o lg ro u p N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le C ris ta n c h o e t a l., 2 0 1 4 T M S 1 (m a le ) 1 5 N o t re p o rt e d N o c o n tr o lg ro u p N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le E n tic o tt e t a l., 2 0 1 1 D e e p rT M S 1 (fe m a le ) 2 0 N o t re p o rt e d N o t re p o rt e d N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le N ie d e rh o fe r, 2 0 1 2 rT M S 1 (fe m a le ) 4 2 N o t re p o rt e d S a m e p a tie n t su b je c t to sh a m T M S N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le N o t a p p lic a b le A S D , A u tis m S pe c tr u m D is o rde r; H F rT MS , H ig h -f re qu e n c y re pe titi ve tr a n sc ra n ia l m a gn e tic sti m u la tion ; iTB S , In te rm itte n t Th e ta -bu rs t sti m u la tion ; L F rTMS , L ow -f re qu e n c y re pe titi ve tr a n sc ra n ia l m a gn e tic sti m u la tion ; rTMS , R e pe titi ve tr a n sc ra n ia lm a g n e tic sti m u la tio n ; tD C S , Tr a n sc ra n ia ldi re c t c u rr e n t sti m u la tion ; TMS , Tr a n sc ra n ia lm a gn e tic sti m u la tion .
T A B L E 2 | S u m m a ry ta b le o f T M S ta rg e ts a n d p a ra m e te rs . S o u rc e Ta rg e t a re a T M S P ro c e d u re N o f s e s s io n s F re q u e n c y H z M T (% ) P u ls e s /s e s s io n In te r-tr a in in te rv a l D u ra ti o n /s e s s io n (mi n u te s ) A n n in o s e t a l., 2 0 1 6 F ro n ta l, ve rt e x, rig h t a n d le ft te m p o ra l, rig h t a n d le ft p a rie ta l, o c c ip ita lc o rt e x 1 c ro ss o ve r se ss io n w ith a c tiv e a n d sh a m T M S , th e n d a ily fo r 1 m o n th D a ily 8 –1 3 N o t a p p lic a b le N o t re p o rt e d N o t re p o rt e d 2 B a ru th e t a l., 2 0 1 0 L e ft a n d rig h t D L P F C , 5 c m a n te rio r to th e si te o f m a xi m a l F D Is tim u la tio n 1 2 (6 le ft ;6 rig h t) W e e kl y 1 9 0 1 5 0 (1 5 × 1 0 ) 2 0 –3 0 s N o t re p o rt e d C a sa n o va e t a l., 2 0 1 2 L e ft a n d rig h t D L P F C 1 2 (6 le ft ;6 rig h t) W e e kl y 1 9 0 1 5 0 (1 5 × 1 0 ) 2 0 –3 0 s N o t re p o rt e d E n tic o tt e t a l., 2 0 1 2 L e ft p rim a ry m o to r c o rt e x a n d su p p le m e n ta ry m o to r a re a 3 W e e kl y 1 1 0 0 9 0 0 N o t re p o rt e d 5 E n tic o tt e t a l., 2 0 1 4 D M P F C , c o il c e n te re d a n d 7 c m a n te rio r to M 1 , 3 -4 c m fr o m n a si o n 1 0 D a ily 5 1 0 0 3 0 × 1 0 2 0 N o t re p o rt e d F e c te a u e t a l., 2 0 1 1 L e ft a n d rig h t p a rs tr ia n g u la ris (B A 4 5 ) a n d p a rs o p e rc u la ris (B A 4 4 ) 4 (1 se ss io n fo r e a c h ta rg e t a re a )+ 1 (fi ft h se ss io n o f sh a m rT M S ) In te rv a ls o f a t le a st 5 d a ys , o ve r 4 w e e ks 1 7 0 N o t re p o rt e d N o t re p o rt e d 3 0 N ie t a l., 2 0 1 7 L e ft a n d rig h t D L P F C ; p o st e rio r su p e rio r te m p o ra ls u lc u s 1 se ss io n fo r e a c h ta rg e t a re a 1 w e e k in te rv a l b e tw e e n se ss io n s 5 0 H z 3 -p u ls e b u rs ts 8 0 fo r a c tiv e iT B S ; 6 0 fo r sh a m c o n d iti o n (a c tiv e M T ) Tw o c o u rs e s o f 6 0 0 o n e a c h h e m is p h e re , le ft fir st , 5 m in u te s a p a rt 2 0 tr a in s a t 1 0 s in te rv a ls 2 x 4 P a n e ra ie t a l., 2 0 1 4 ; S tu d y I L e ft a n d rig h t p re m o to r c o rt e x, 2 .5 c m ro st ra lt o p rim a ry m o to r c o rt e x 1 se ss io n o f H F rT M S L F rT M S a n d sh a m b o th o n th e le ft a n d rig h t E ve ry 2 w e e ks L F rT M S : 1 ; H F rT M S : 8 9 0 (r e st in g M T ) L F rT M S : 9 0 0 ; H F rT M S : 3 0 tr a in s o f 3 0 st im u li e a c h tr ia ll a st in g 3 .6 s 5 6 .4 s L F rT M S : 1 5 ; H F rT M S : 3 0 P a n e ra ie t a l., 2 0 1 4 ; S tu d y II L e ft p re m o to r c o rt e x, 2 .5 c m ro st ra lt o p rim a ry m o to r c o rt e x 1 0 (H F rT M S , L F rT M S ) E ve ry w e e kd a y (1 0 d a ys ), o ve r 2 w e e ks L F rT M S : 1 ; H F rT M S : 8 9 0 (r e st in g M T ) L F rT M S : 9 0 0 ; H F rT M S : 3 0 tr a in s o f 3 0 st im u li e a c h tr ia ll a st in g 3 .6 s 5 6 .4 s L F rT M S : 1 5 ; H F rT M S : 3 0 P a n e ra ie t a l., 2 0 1 4 ; S tu d y III L e ft p re m o to r c o rt e x, 2 .5 c m ro st ra lt o p rim a ry m o to r c o rt e x 4 H F rT M S o r sh a m ; C ro ss o ve r d e si g n T M S -s h a m -T M S -s h a m D a ily (5 d a ys ) L F rT M S : 1 ; H F rT M S : 8 9 0 (r e st in g M T ) L F rT M S : 9 0 0 ; H F rT M S : 3 0 tr a in s o f 3 0 st im u li e a c h tr ia ll a st in g 3 .6 s 5 6 .4 s L F rT M S : 1 5 ; H F rT M S : 3 0 P a n e ra ie t a l., 2 0 1 4 ; S tu d y IV L e ft p re m o to r c o rt e x, 2 .5 c m ro st ra lt o p rim a ry m o to r c o rt e x 1 0 H F rT M S o r 1 0 H F rT M S+ E H I E ve ry w e e kd a y (1 0 d a ys ), o ve r 2 w e e ks 8 9 0 (r e st in g M T ) L F rT M S : 9 0 0 ; H F rT M S : 3 0 tr a in s o f 3 0 st im u li e a c h tr ia ll a st in g 3 .6 s 5 6 .4 s L F rT M S : 1 5 ; H F rT M S : 3 0 S o kh a d ze e t a l., 2 0 0 9 L e ft D L P F C , 5 c m a n te rio r to m a xi m a lF D Ir e sp o n se 6 Tw ic e a w e e k 0 .5 9 0 1 5 0 (1 5 × 1 0 ) 2 0 -3 0 s N o t re p o rt e d S o kh a d ze e t a l., 2 0 1 2 L e ft a n d rig h t D L P F C 1 2 (6 le ft ;6 rig h t) W e e kl y 1 9 0 1 5 0 (1 5 × 1 0 ) N o t re p o rt e d N o t re p o rt e d (C o n tin u e d )
T A B L E 2 | C o n tin u e d S o u rc e Ta rg e t a re a T M S P ro c e d u re N o f s e s s io n s F re q u e n c y H z M T (% ) P u ls e s /s e s s io n In te r-tr a in in te rv a l D u ra ti o n /s e s s io n (mi n u te s ) S o kh a d ze e t a l., 2 0 1 4 b R ig h t a n d le ft D L P F C , 5 c m a n te rio r to m a xi m a lF D Ir e sp o n se 1 8 (6 le ft , 6 rig h t, 6 b ila te ra lly )+ N F B (2 0 m in u te s) W e e kl y 1 9 0 1 8 0 N o t re p o rt e d N o t re p o rt e d S o kh a d ze e t a l., 2 0 1 4 a L e ft a n d rig h t D L P F C 1 8 (6 rig h t, 6 le ft , 6 a lte rn a tin g rig h t a n d le ft ) W e e kl y 1 9 0 1 8 0 (9 × 2 0 ) N o t re p o rt e d N o t re p o rt e d S o kh a d ze e t a l., 2 0 1 6 R ig h t a n d le ft D L P F C , 5 c m a n te rio r to m a xi m a lF D Ir e sp o n se 1 8 (6 rig h t, 6 le ft , 6 b ila te ra lly ) W e e kl y 1 9 0 1 8 0 (9 × 2 0 ) 2 0 –3 0 s N o t re p o rt e d A b u ja d ie t a l., 2 0 1 7 R ig h t D L P F C 1 5 5 d a ys a w e e k, o ve r 3 w e e ks 5 0 H z 3 -p u ls e b u rs ts a t 5 H z 1 0 0 9 0 0 (3 0 0 b u rs ts ) 8 s O n /2 s O ff 5 C a sa n o va e t a l., 2 0 1 4 L e ft a n d rig h t D L P F C 1 8 (6 le ft , 6 rig h t, 6 b ila te ra lly ) W e e kl y 0 .5 9 0 1 6 0 (8 × 2 0 ) N o t re p o rt e d N o t re p o rt e d G ó m e z e t a l., 2 0 1 7 L e ft D L P F C 2 0 D a ily 1 9 0 (r e st in g M T ) 1 5 0 0 (4 × 3 7 5 ) 6 0 s 3 0 S o kh a d ze e t a l., 2 0 1 0 L e ft D L P F C , 5 c m a n te rio r to m a xi m a lF D Ir e sp o n se 6 Tw ic e a w e e k 0 .5 9 0 1 5 0 (1 5 × 1 0 ) N o t re p o rt e d N o t re p o rt e d S o kh a d ze e t a l., 2 0 1 7 B ila te ra lD L P F C , 5 c m a n te rio r to a n d in a p a ra sa g itt a lp la n e to th e si te o f m a xi m a la b d u c to r p o lli c is b re vi s st im u la tio n 1 8 W e e kl y 0 .5 9 0 (r e st in g M T ) 1 6 0 (8 × 2 0 ) 2 0 s N o t re p o rt e d W a n g e t a l., 2 0 1 6 L e ft a n d rig h t D L P F C , 5 c m a n te rio r to th e si te o f m a xi m a l F D Is tim u la tio n 1 2 (6 le ft , 6 rig h t) W e e kl y 0 .5 9 0 1 6 0 2 0 –3 0 s N o t re p o rt e d A vi ra m e e t a l., 2 0 1 7 c a se 1 B ila te ra lm e d ia lp re fr o n ta lc o rt e x 2 7 D a ily , o ve r 6 w e e ks (m is se d 3 tr e a tm e n ts ) 5 N o t re p o rt e d 6 0 × 1 0 2 0 s 3 0 A vi ra m e e t a l., 2 0 1 7 c a se 2 B ila te ra lm e d ia lp re fr o n ta lc o rt e x 2 9 D a ily , o ve r 6 w e e ks (m is se d 1 tr e a tm e n t) 5 N o t re p o rt e d 6 0 × 1 0 2 0 s 3 0 C ris ta n c h o e t a l., 2 0 1 4 L e ft a n d rig h t D L P F C 3 6 (1 0 rig h t, 2 6 le ft ) R ig h t: d a ily ; L e ft : a ft e r 2 0 se ss io n s, T M S w a s ta p e re d o ve r 3 w e e ks 1 9 0 (r e st in g M T ) R ig h t: 1 5 0 P P S in c re a se d to 3 0 0 P P S in th e se c o n d w e e k; L e ft : 3 0 0 P P S in c re a se d to 6 0 0 P P S in th e fo u rt h w e e k R ig h t: 1 0 s O n /1 0− 3 0 s O ff ; L e ft : 1 0 s O n / 1 0− 1 5 s O ff N o t re p o rt e d E n tic o tt e t a l., 2 0 1 1 B ila te ra lm e d ia lp re fr o n ta lc o rt e x 9 E ve ry w e e kd a y (1 0 d a ys ), o ve r 2 w e e ks 5 1 0 0 3 0 × 1 0 2 0 s 1 5 N ie d e rh o fe r, 2 0 1 2 S u p p le m e n ta ry m o to r a re a 5 D a ily 1 N o t re p o rt e d 1 ,2 0 0 N o t re p o rt e d 6 0 D L P F C , D o rs o la te ra l pr e fr o n ta l c o rte x; D MP F C , D o rs om e di a l pr e fr on ta l c or te x; F D I, F ir st D o rs a l In te ros se ou s m u sc le ; H F rTMS , H igh -f re qu e n c y re pe titi ve tr a n sc ra n ia l m a gn e tic sti m u la tion ; iTB S , In te rm itte n t Th e ta -bu rs t sti m u la tion ; L F rT MS , L o w -f re qu e n c y re pe titi ve tr a n sc ra n ia lm a gn e tic sti m u la tion ; MT , Motor th re sh ol d; N F B , N e u rof e e dba c k; P P S , P u ls e s P e r S e ss ion ; rTMS , R e pe titi ve tr a n sc ra n ia lm a gn e tic sti m u la tion ; TMS , Tr a n sc ra n ia lm a gn e tic sti m u la tion .
T A B L E 3 | S u m m a ry o f st u d y o u tc o m e m e a su re s a n d re su lts , in c lu d in g fo llo w -u p a n d a d ve rs e e ff e c ts . S o u rc e B e h a v io ra l me a s u re s C o g n it iv e me a s u re s B e h a v io ra l R e s u lt s C o g n it iv e R e s u lt s A d v e rs e re a c ti o n s F o ll o w u p A d d it io n a l c o mme n ts A n n in o s e t a l., 2 0 1 6 D e fic its in so c ia l c o m m u n ic a tio n a n d in te ra c tio n , im a g in a tiv e p la y, o r m a ki n g fr ie n d s; in te lle c tu a ld is a b ili ty A c tiv e tr e a tm e n t: 4 p a tie n ts sh o w e d m a jo r c h a n g e s; 3 m in o r c h a n g e s a n d 1 m ix e d c h a n g e s in th e lis t o f d is o rd e rs . N o c h a n g e s in th e sh a m g ro u p N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n B a ru th e t a l., 2 0 1 0 A B C (Ir rit a b ili ty a n d H yp e ra c tiv ity S u b sc a le s) ; S R S (S o c ia lA w a re n e ss S u b sc a le ); R B S -R K a n iz sa Ill u so ry F ig u re Te st : R T, e rr o r ra te s (c o m m is io n , o m is si o n , to ta l), p o st -e rr o r R T 1 -A B C : si g n ific a n t re d u c tio n in re p e tit iv e b e h a vi o r a n d irr ita b ili ty su b sc a le s. N o c h a n g e s in h yp e ra c tiv ity o r so c ia la w a re n e ss su b sc a le s. 2 -R B S -R : re d u c tio n in re p e tit iv e a n d re st ric te d b e h a vi o r p a tt e rn s. 3 -S R S n o t re p o rt e d N o si g n ific a n t d iff e re n c e s in R T a n d E rr o rs , in a n y o f th e g ro u p s 5 /1 6 itc h in g se n sa tio n a ro u n d n o se d u rin g st im u la tio n ; 1 /1 6 re p o rt e d m ild , tr a n si e n t te n si o n -t yp e h e a d a c h e a ft e r st im u la tio n N o fo llo w u p a ft e r st im u la tio n C a sa n o va e t a l., 2 0 1 2 A B C ; S R S (S o c ia l A w a re n e ss S u b sc a le ); R B S -R st e re o ty p e d (s e lf-in ju rio u s, c o m p u ls iv e , rit u a lis tic , sa m e n e ss , a n d re st ric te d ra n g e su b sc a le s) K a n iz sa Ill u so ry F ig u re Te st : R T, e rr o r ra te (c o m m is si o n , o m is si o n , to ta le rr o r ra te ) 1 -A B C : si g n ific a n t re d u c tio n in irr ita b ili ty su b sc a le p o st -T M S . N o c h a n g e s in h yp e ra c tiv ity su b sc a le . 2 -R B S -R : si g n ific a n t d e c re a se in re p e tit iv e a n d re st ric te d b e h a vi o r p a tt e rn s p o st -T M S . 3 -S R S : N o c h a n g e s in so c ia la w a re n e ss a ft e r T M S . W a iti n g -l is t: n o si g n ific a n t c h a n g e s in a n y m e a su re 1 -R T: n o si g n ific a n t c h a n g e a s a re su lt o f rT M S . 2 -O m is si o n e rr o r ra te : si g n ific a n t d e c re a se in T M S g ro u p in c o m p a ris o n to w a iti n g lis t. 3 -T o ta le rr o r ra te : si g n ific a n t d e c re a se p o st T M S N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n E n tic o tt e t a l., 2 0 1 2 R T; M o ve m e n t tim e 1 -R T: n o si g n ific a n t d iff e re n c e p o st -T M S . 2 -M o ve m e n t tim e : n o si g n ific a n t d iff e re n c e p o st -T M S b u t si g n ific a n t re d u c tio n a ft e r sh a m st im u la tio n N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n E n tic o tt e t a l., 2 0 1 4 R A A D S ;A S Q ; IR I R e a d in g th e m in d in th e e ye s te st ; a n im a tio n s m e n ta liz in g te st 1 -R A A D S : si g n ific a n t re d u c tio n o n th e so c ia lr e la te d n e ss su b sc a le p o st -T M S , b u t n o t p o st -s h a m . S ig n ific a n t tim e c o n d iti o n in te ra c tio n fo r th e a c tiv e c o n d iti o n . 2 -IR I: si g n ific a n t re d u c tio n o n th e fa n ta sy su b sc a le p o st -T M S , b u t n o t p o st -s h a m . 3 -A S Q : N o e ff e c t N o si g n ific a n t e ff e c ts o f c o n d iti o n (T M S o r sh a m ) in m e n ta liz in g m e a su re s 1 /1 5 lig h th e a d e d n e ss fo r 5 m in u te s a ft e r T M S ; 2 /1 5 m in o r fa c ia ld is c o m fo rt d u rin g T M S 1 m o n th fo llo w -u p : si g n ific a n t re d u c tio n in so c ia lr e la tin g sy m p to m s in T M S p a rt ic ip a n ts re la tiv e to sh a m p a rt ic ip a n ts 4 0 % o f T M S g ro u p a n d 3 8 % o f sh a m g ro u p o n p sy c h o tr o p ic m e d ic a tio n (m o st ly a n tid e p re ss a n ts ) F e c te a u e t a l., 2 0 1 1 B o st o n N a m in g Te st W o rs e p e rf o rm a n c e fo llo w in g T M S to th e le ft p a rs o p e rc u la ris ; b e tt e r p e rf o rm a n c e a ft e r T M S to th e le ft p a rs tr ia n g u la ris th a n a ft e r sh a m st im u la tio n 2 /1 0 sl e e p y; 1 /1 0 m o re e m o tio n a l; 1 /1 0 st iff n e c k; 1 /1 0 d iz zi n e ss N o fo llo w u p a ft e r st im u la tio n N e u ro n a vi g a tio n g u id e d (C o n tin u e d )
T A B L E 3 | C o n tin u e d S o u rc e B e h a v io ra l me a s u re s C o g n it iv e me a s u re s B e h a v io ra l R e s u lt s C o g n it iv e R e s u lt s A d v e rs e re a c ti o n s F o ll o w u p A d d it io n a l c o mme n ts N ie t a l., 2 0 1 7 Y-B O C S ; S R S C C P T; W C S T 1 -Y -B O C S : c o m p u ls iv e b e h a vi o rs si g n ific a n tly d e c re a se d a t 8 h a n d 2 d a ys a ft e r p o st e rio r su p e rio r te m p o ra ls u lc u s iT B S c o m p a re d to sh a m (p a re n t-re p o rt s) . N o c h a n g e in se lf-re p o rt e d sc o re s. N o d iff e re n c e b e tw e e n D L P F C a n d sh a m st im u la tio n . 2 -S R S : im p ro ve m e n t in p a re n t-re p o rt e d sc o re s o f so c ia lc o m m u n ic a tio n d e fic its 8 d a ys a ft e r D L P F C iT B S c o m p a re d to sh a m . N o c h a n g e in se lf-re p o rt e d sc o re s 1 -C C P T: d e c re a se in R T, o m is si o n e rr o rs , a n d c o m m is si o n e rr o rs p o st -iT B S o ve r th e D L P F C . S ig n ific a n t re d u c tio n in R T a ft e r D L P F C iT B S c o m p a re d to sh a m , b u t n o d iff e re n c e s in e rr o rs . 2 -W C S T: n o si g n ific a n t c h a n g e s a ft e r iT B S 3 p a rt ic ip a n ts fe lt tr a n si e n t d is c o m fo rt d u rin g iT B S o ve r th e D L P F C b e c a u se o f m u sc le tw itc h e s a ro u n d th e e ye s 2 d a ys fo llo w -u p : si g n ific a n t re d u c tio n in p a re n t-re p o rt e d Y-B O C S c o m p u ls io n su b sc a le sc o re s 1 p a tie n t o n se rt ra lin e ; 1 p a tie n t o n flu o xe tin e ; 1 p a tie n t o n m e th yl p h e n id a te P a n e ra ie t a l., 2 0 1 4 ; S tu d y I N u m b e r o f su c c e ss e s in e ye –h a n d in te g ra tio n ta sk s fr o m P E R -P H F rT M S : in c re a se in e ye –h a n d in te g ra tio n a ft e r T M S to le ft p re m o to r c o rt e x. L F rT M S a n d sh a m : n o d iff e re n c e s in e ye –h a n d in te g ra tio n . L F rT M S , H F rT M S , a n d sh a m p a irw is e c o m p a ris o n s: si g n ific a n t d iff e re n c e b e tw e e n H F rT M S a n d b o th L F rT M S a n d sh a m N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n P a n e ra ie t a l., 2 0 1 4 ; S tu d y II N u m b e r o f su c c e ss e s in e ye –h a n d in te g ra tio n ta sk s fr o m P E R -P L F rT M S , H F rT M S , a n d sh a m : h ig h e st in c re a se in m e a n p e rf o rm a n c e w ith H F rT M S , fo llo w e d b y L F rT M S a n d sh a m . P re -p o st c o m p a ris o n s sh o w e d d iff e re n c e o n ly fo r H F rT M S N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n P a n e ra ie t a l., 2 0 1 4 ; S tu d y III N u m b e r o f su c c e ss e s in e ye –h a n d in te g ra tio n ta sk s fr o m P E R -P S ig n ific a n t in c re a se in e ye -h a n d in te g ra tio n a ft e r T M S , in c o m p a ris o n to sh a m 1 /6 c h ild re n d e ve lo p e d in c re a se d re st le ss n e ss a n d ra p id m o o d sw in g s d u rin g th e fir st e xp e rim e n ta l c o n d iti o n 2 ,5 d a ys fo llo w u p ; H fr T M S sh o w e d n o d iff e re n c e fr o m sh a m T M S o r fr o m b a se lin e a ss e ss m e n t P a n e ra ie t a l., 2 0 1 4 ; S tu d y IV N u m b e r o f su c c e ss e s in e ye –h a n d in te g ra tio n ta sk s fr o m P E R -P P a irw is e c o m p a ris o n s sh o w e d a st a tis tic a l d iff e re n c e b e tw e e n H F rT M S+ E ye –h a n d in te g ra tio n tr a in in g a n d b o th tr e a tm e n ts a lo n e . N o d iff e re n c e b e tw e e n E ye –h a n d in te g ra tio n tr a in in g a n d H F rT M S N o t re p o rt e d 1 m o n th fo llo w u p ; T M S+ tr a in in g si g n ific a n tly b e tt e r th a n e ith e r in te rv e n tio n a lo n e a ft e r 1 w e e k; a t 2 w e e ks T M S+ tr a in in g su p e rio r to tr a in in g a lo n e ; a t 4 w e e ks n o d iff e re n c e s b e tw e e n g ro u p s (C o n tin u e d )
T A B L E 3 | C o n tin u e d S o u rc e B e h a v io ra l me a s u re s C o g n it iv e me a s u re s B e h a v io ra l R e s u lt s C o g n it iv e R e s u lt s A d v e rs e re a c ti o n s F o ll o w u p A d d it io n a l c o mme n ts S o kh a d ze e t a l., 2 0 0 9 A B C ; S R S ; R B S -R ; C G I K a n iz sa Ill u so ry F ig u re Te st : R T, e rr o r ra te (c o m m is si o n , o m is si o n , to ta le rr o rs ) 1 -R B S -R : o n ly T M S g ro u p re p o rt e d . S ig n ific a n t re d u c tio n in re p e tit iv e b e h a vi o r su b sc a le . N o si g n ific a n t d iff e re n c e s in o th e r R B S -R su b sc a le s. 2 -A B C /S R S /C G I: n o t re p o rt e d N o si g n ific a n t d iff e re n c e s in R T a n d E rr o rs , in a n y o f th e g ro u p s N o n e N o fo llo w u p a ft e r st im u la tio n S o kh a d ze e t a l., 2 0 1 2 3 -c a te g o ry o d d -b a ll ta sk , R T, e rr o r ra te (c o m m is si o n , o m is si o n a n d to ta le rr o rs ), p o st -e rr o r R T 1 -R T: n o c h a n g e ; 2 -O m is si o n e rr o r ra te : si g n ific a n t d e c re a se p o st -T M S , b u t n o t p o st w a iti n g p e rio d . 3 -C o m m is si o n e rr o r ra te : N o b e tw e e n g ro u p d iff e re n c e s. 4 -P o st -e rr o r R T: sl o w in g o f p o st -e rr o r R T in T M S g ro u p c o m p a re d to w a iti n g lis t g ro u p N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n S o kh a d ze e t a l., 2 0 1 4 b A B C (Ir rit a b ili ty , L e th a rg y/S o c ia lW ith d ra w a l a n d H yp e ra c tiv ity su b sc a le s) ; R B S -R T h re e -S tim u li O d d b a ll Ta sk : R T, e rr o r ra te s (c o m m is si o n , o m is si o n , to ta l), p o st -e rr o r R T 1 -A B C : si g n ific a n t re d u c tio n in L e th a rg y/S o c ia lW ith d ra w a la n d h yp e ra c tiv ity su b sc a le s. 2 -R B S -R : si g n ific a n t d e c re a se in to ta lR B S -R sc o re a n d in st e re o ty p ic b e h a vi o r a n d rit u a lis tic /s a m e n e ss b e h a vi o r su b sc a le s. N o si g n ific a n t c h a n g e s in w a iti n g lis t g ro u p in a n y m e a su re 1 -R T: n o c h a n g e . 2 -O m is si o n e rr o r ra te : n o d iff e re n c e s b e tw e e n g ro u p s. 3 -C o m m is si o n e rr o r ra te : si g n ific a n t d e c re a se p o st T M S -N F B . 4 -T o ta le rr o r ra te : si g n ific a n t d e c re a se p o st T M S -N F B . 5 -P o st -e rr o r R T: T M S -N F B g ro u p p re se n te d a sl o w in g o f p o st -e rr o r R T; w a iti n g lis t g ro u p sh o w e d n o c h a n g e s N o n e N o fo llo w u p a ft e r st im u la tio n S o kh a d ze e t a l., 2 0 1 4 a A B C ; S R S ; R B S -R V is u a lo d d -b a ll ta sk : R T, e rr o r ra te (c o m m is si o n , o m is si o n , to ta le rr o r ra te ), p o st -e rr o r R T 1 -A B C : si g n ific a n t re d u c tio n in irr ita b ili ty , le th a rg y/s o c ia lw ith d ra w a l a n d h yp e ra c tiv ity . 2 -R B S -R : si g n ific a n t d e c re a se in to ta lR B S -R sc o re , st e re o ty p ic b e h a vi o r su b sc a le a n d rit u a lis tic /s a m e n e ss b e h a vi o r. W a iti n g lis t: n o c h a n g e in a n y o f th e sc a le s 1 -R T: n o si g n ific a n t c h a n g e s p o st T M S . 2 : O m is si o n e rr o r ra te : N o b e tw e e n g ro u p d iff e re n c e s. 3 -C o m is si o n e rr o r ra te : si g n ific a n t d e c re a se p o st -T M S , W T L n o t re p o rt e d . 4 -P o st -e rr o r R T: T M S g ro u p sh o w e d p o st -e rr o r R T in c re a se N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n S o kh a d ze e t a l., 2 0 1 6 A B C ; R B S -R T h re e -s tim u li o d d b a ll ta sk : R T, e rr o r ra te s, p o st -e rr o r R T 1 -A B C : si g n ific a n t re d u c tio n in irr ita b ili ty , le th a rg y/s o c ia lw ith d ra w a l a n d h yp e ra c tiv ity su b sc a le s. 2 -R B S -R : si g n ific a n t d e c re a se in to ta l R B S -R sc o re , st e re o ty p ic b e h a vi o r, rit u a lis tic /s a m e n e ss b e h a vi o r a n d c o m p u ls iv e b e h a vi o r su b sc a le s 1 -R T: n o si g n ific a n t c h a n g e . 2 : To ta le rr o r ra te : si g n ific a n t d e c re a se m a in ly d u e to d e c re a se in c o m m is si o n e rr o rs . 3 -P o st -e rr o r R T: p re tr e a tm e n t sp e e d in g c h a n g e d in to p o st -e rr o r sl o w in g N o t re p o rt e d E ve ry p a rt ic ip a n t w a s e va lu a te d b e fo re T M S c o u rs e a n d w ith in 2 w e e ks fo llo w in g T M S tr e a tm e n t (C o n tin u e d )
T A B L E 3 | C o n tin u e d S o u rc e B e h a v io ra l me a s u re s C o g n it iv e me a s u re s B e h a v io ra l R e s u lt s C o g n it iv e R e s u lt s A d v e rs e re a c ti o n s F o ll o w u p A d d it io n a l c o mme n ts A b u ja d ie t a l., 2 0 1 7 R B S -R ; Y-B O C S W C S T; S tr o o p te st 1 -R B S -R : si g n ific a n t d e c re a se in m e a n sc o re s p o st tr e a tm e n t. 2 - Y-B O C S : d e c re a se in m e a n o ve ra ll c o m p u ls iv e b e h a vi o rs p o st tr e a tm e n t 1 -W S C T: im p ro ve m e n t in p e rs e ve ra tiv e e rr o s p o st tr e a tm e n t. 2 -S tr o o p te st : im p ro ve m e n t in to ta lt im e fo r c o m p le tio n p o st tr e a tm e n t N o n e 5 p a tie n ts w e re a ss e ss e d a t 5 m o n th s fo llo w u p : im p ro ve m e n t in a ll th e sc a le s w a s m a in ta in e d , e xc e p t fo r th e st ro o p te st N e u ro n a vi g a tio n g u id e d ; C a sa n o va e t a l., 2 0 1 4 A B C ; S R S ; R B S -R 1 -A B C : si g n ific a n t re d u c tio n in irr ita b ili ty , le th a rg y/s o c ia lw ith d ra w a l a n d in h yp e ra c tiv ity su b sc a le s. 2 -R B S -R : si g n ific a n t d e c re a se in to ta l R B S -R sc o re , st e re o ty p ic b e h a vi o r su b sc a le a n d rit u a lis tic /s a m e n e ss b e h a vi o r. 3 -S R S n o t re p o rt e d N o t re p o rt e d E ve ry p a rt ic ip a n t w a s e va lu a te d b e fo re T M S c o u rs e a n d w ith in 2 w e e ks fo llo w in g T M S tr e a tm e n t G ó m e z e t a l., 2 0 1 7 A B C ; A D I-R ; A T E C ; G C IS A B C /A D I-R /A T E C /G C IS : si g n ific a n t d e c re a se in th e to ta ls c o re s o n e m o n th a ft e r th e in te rv e n tio n N o t re p o rt e d F o llo w u p to 6 m o n th s: d e c re a se in A B C , A D I-R a n d A T E C re m a in e d si g n ific a n t S o kh a d ze e t a l., 2 0 1 0 A B C ; S R S ; R B S -R T h re e -S tim u li V is u a l O d d b a ll w ith N o ve l D is tr a c te rs : R T, e rr o r % 1 -R B S -R : si g n ific a n t re d u c tio n in re p e tit iv e b e h a vi o r su b sc a le . N o si g n ific a n t d iff e re n c e s in o th e r R B S -R su b sc a le s. 2 -A B C /S R S : n o t re p o rt e d 1 -E rr o r % : si g n ific a n t re d u c tio n p o st T M S . 2 -R T: n o d iff e re n c e N o n e P a rt ic ip a n ts w e re e va lu a te d p rio r to re c e iv in g T M S a n d 2 w e e ks fo llo w in g tr e a tm e n t S o kh a d ze e t a l., 2 0 1 7 A B C ; R B S -R ; S R S 1 -A B C : si g n ific a n t re d u c tio n in le th a rg y, h yp e ra c tiv ity a n d sp e e c h su b sc a le s. N o c h a n g e s in st e re o ty p e d b e h a vi o r. 2 -R B S -R : si g n ific a n t d e c re a se in R B S -R to ta l sc o re , st e re o ty p ic , rit u a lis tic a n d c o m p u ls iv e b e h a vi o r. 3 -S R S : si g n ific a n t im p ro ve m e n t in so c ia l a w a re n e ss , so c ia lc o g n iti o n a n d so c ia lm o tiv a tio n N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n (C o n tin u e d )
T A B L E 3 | C o n tin u e d S o u rc e B e h a v io ra l me a s u re s C o g n it iv e me a s u re s B e h a v io ra l R e s u lt s C o g n it iv e R e s u lt s A d v e rs e re a c ti o n s F o ll o w u p A d d it io n a l c o mme n ts W a n g e t a l., 2 0 1 6 A B C ; R B S -R 1 -A B C : si g n ific a n t re d u c tio n in st e re o ty p e d b e h a vi o r, h yp e ra c tiv ity a n d in a p p ro p ria te sp e e c h . 2 -R B S -R : si g n ific a n t d e c re a se in to ta lR B S -R , a n d rit u a lis tic /s a m e n e ss , st e re o ty p ic a l a n d c o m p u ls iv e b e h a vi o r su b sc a le s N o n e N o fo llo w u p a ft e r st im u la tio n A vi ra m e e t a l., 2 0 1 7 , c a se 1 IR I; A u tis m S p e c tr u m in vo c a la sp e c ts C o m p u ta riz e d C o g n iti ve B a tt e ry (M in d st re a m , N e u ro tr a x) a n d a b a tt e ry o f e m o tio n a lr e c o g n iti o n ta sk s fr o m th e A u tis m re se a rc h c e n te r in C a m b rid g e (e ye te st , fa c e te st s, C A M fa c e -v o ic e ) 1 -IR I/A u tis m S p e c tr u m in vo c a l a sp e c ts : im p ro ve m e n t in a u tis tic sy m p to m s a n d e m p a th y. 2 -Y -B O C S : d e c re a se in O C D sy m p to m s. 3 -E ye s te st /C A M vo ic e : re d u c tio n in e rr o r ra te . 4 -F a c e s te st a n d C A M fa c e : n o e ff e c t 1 -M in d st re a m : in c re a se in g lo b a ls c o re s, e xe c u tiv e fu n c tio n , a tt e n tio n , sp e e d p ro c e ss in g , m o to r sk ill s, m e m o ry a n d ve rb a lflu e n c y sc o re s N o t re p o rt e d 2 m o n th fo llo w u p (s e lf-a ss e ss m e n t q u e st io n n a ire s) : O b se ss iv e c o m p u ls iv e d is o rd e r sy m p to m s w e re st ill si g n ific a n tly lo w e r th a n b a se lin e , in b o th c a se s A vi ra m e e t a l., 2 0 1 7 , c a se 2 1 -IR I/A u tis m S p e c tr u m in vo c a l a sp e c ts : im p ro ve m e n t in a u tis tic sy m p to m s a n d e m p a th y. 2 -Y -B O C S : d e c re a se in O C D sy m p to m s. 3 -E ye s te st /C A M vo ic e /C A M fa c e : re d u c tio n in e rr o r ra te . 4 -F a c e s te st : n o d iff e re n c e in e rr o r ra te 1 -M in d st re a m : in c re a se in g lo b a ls c o re s, e xe c u tiv e fu n c tio n , a tt e n tio n , sp e e d p ro c e ss in g , vi su a ls p a c ia l a n d m o to r sk ill s sc o re s; d e c re a se in m e m o ry a n d ve rb a lflu e n c y sc o re s N o t re p o rt e d C ris ta n c h o e t a l., 2 0 1 4 Im p ro ve m e n t in p a tie n t’s b e h a vi o r, so c ia li n te ra c tio n s, a b ili ty to c o p e w ith c h a n g e a n d a b ili ty to c o n c e n tr a te in sc h o o l M ild h e a d a c h e s, ja w tw itc h d u rin g st im u la tio n a n d tr a n si e n t d iz zi n e ss im m e d ia te ly a ft e r tr e a tm e n ts N o fo llo w u p a ft e r st im u la tio n P a tie n t o n o la n za p in e / flu o xe tin e , g u a n fa c in e , c lo n a ze p a m E n tic o tt e t a l., 2 0 1 1 IR I; A S Q ; R A A D S D e c re a se in a ll th e sc a le s a ft e r tr e a tm e n t N o n e 1 m o n th fo llo w u p : su st a in e d im p ro ve m e n t in A S Q a n d R A A D S sc o re s N ie d e rh o fe r, 2 0 1 2 A B C Im p ro ve m e n t in A B C irr ita b ili ty a n d st e re o ty p y sc a le s, w h e re a s so c ia l w ith d ra w a la n d in a p p ro p ria te sp e e c h -a ss o c ia te d ite m s d id n o t sh o w a n y b e n e fit N o t re p o rt e d N o fo llo w u p a ft e r st im u la tio n A B C , A be rr a n t B e h a vi o r C h e c kl is t; A D I-R , A u tis m D ia gn os tic In te rv ie w -R e vi se d; A S Q , A u tis m S pe c tr u m Q u oti e n t; A TEC , A u tis m Tr e a tm e n t Ev a lu a tion C h e c kl is t; C A M, C a m br idge m in dr e a di n g fa c e -v oi c e te sts ; C C P T, C on n e rs ’ C o n tin u o u s P e rf o rm a n c e Te st; C G I, C lin ic a lG lo ba lI m pr e ss ion S c a le ; D L P F C , D o rs ol a te ra lpr e fr on ta lc or te x; G C IS , G loba lC lin ic a lI m pr e ss ion S c a le ; H F rTMS , H igh -f re qu e n c y re pe titi ve tr a n sc ra n ia lm a gn e tic sti m u la tion ; IR I, In te rpe rs on a l R e a c tiv ity In de x; iT B S , In te rm itte n t T h e ta -bu rs t sti m u la tion ; L F rTMS , L ow -f re qu e n c y re pe titi ve tr a n sc ra n ia l m a gn e tic sti m u la tion ; N F B , N e u rof e e dba c k; R A A D S , R itv o A u tis m -A spe rge rs D ia gn os tic S c a le ; R B S -R , R e pe titi ve B e h a vi or S c a le ; R T, R e a c tio n tim e ; rT MS , R e pe titi ve tr a n sc ra n ia lm a gn e tic sti m u la tion ; P EP -R , P sy c h oe du c a tion a lP rofi le -R e vi se d; TMS , Tr a n sc ra n ia lm a gn e tic sti m u la tion ; S R S , S oc ia lR e spon si ve n e ss S c a le ; W C S T, W is c on si n C a rd S or tin g Te st; Y -B O C S , Y a le -B ro w n O bs e ss iv e C o m pu ls iv e S c a le .
Six of the controlled studies used sham rTMS as the control
intervention (Fecteau et al., 2011; Enticott et al., 2012, 2014;
Panerai et al., 2014; Anninos et al., 2016; Ni et al., 2017) while the remaining 6 compared rTMS-treated patients with wait-list controls. Three studies recruited exclusively adult subjects to
the experimental arm (Fecteau et al., 2011; Enticott et al., 2014;
Ni et al., 2017), with the remainder focusing predominantly on children and adolescents. Overall, data were reported from 371 rTMS-treated patients, with a mean age of 15.9 ± 5.2 years, 5 of whom in case-reports (26.4 ± 9.3 years-old) and the remaining 366 from intervention studies (15.8 ± 5.1 years-old). The overwhelming majority of studies recruited patients with an
IQ higher than 80. The 4 trials reported in the paper byPanerai
et al. (2014)were all performed on subjects with severe cognitive
impairment, while Abujadi et al. (2017), Baruth et al. (2010),
andWang et al. (2016)included patients both with and without cognitive impairment.
One study used a pico-Tesla TMS protocol (Anninos et al.,
2016) while two others used TBS protocols (Abujadi et al.,
2017; Ni et al., 2017). Pico-Tesla TMS is a technology invented
and used by a specific research group (Anninos and Tsagas,
1995). It uses a modified helmet containing up to 122 coils
arranged in several arrays. This allows for delivery of low-intensity transcranial magnetic stimulation, at the pico-Tesla
level (1 pico-Tesla = 10−12 Tesla), simultaneously to several
brain areas, at frequencies of 2–7 Hz (Anninos et al., 2016). The
remaining studies used other, more conventional rTMS methods. Most studies targeted stimulation to the dorsolateral prefrontal cortex (DLPFC), either bilaterally or in the left hemisphere,
using low stimulation frequencies (0.5–1 Hz). Ni et al. (2017)
additionally stimulated the posterior superior temporal sulcus
using iTBS, while Fecteau et al. (2011) used 1 Hz rTMS to
stimulate the pars triangularis and pars opercularis of the inferior
frontal gyrus, bilaterally. Avirame et al. (2017) and Enticott
et al. (2011, 2014) targeted the dorsal medial prefrontal cortex
(DMPFC) with stimulation frequencies of 5 Hz. Panerai et al.
(2014)stimulated the left premotor cortex (and in a subgroup of
patients also the right premotor cortex) at 8 Hz, whileEnticott
et al. (2012) chose to stimulate the left primary motor cortex and supplementary motor area with 1 Hz rTMS. The pico-Tesla TMS trial targeted stimulation to the vertex, frontal and occipital cortex, left and right parietal cortex, and left and right
temporal cortex, at frequencies of 8–13 Hz (Anninos et al., 2016).
Treatment schedules also varied widely. While most studies delivered treatment in weekly or twice-weekly sessions, some
delivered daily sessions for 5–29 days consecutively (Niederhofer,
2012; Cristancho et al., 2014; Enticott et al., 2014; Panerai et al., 2014; Anninos et al., 2016; Avirame et al., 2017; Gómez et al.,
2017). A limited number of studies used a single session in a
proof of concept approach (Fecteau et al., 2011; Panerai et al.,
2014; Ni et al., 2017). Only two studies used neuronavigation to guide stimulation of the intended cortical region. All studies used
conventional figure of eight coils, with the exception ofEnticott
et al. (2014), where an H-coil was used, andAnninos et al. (2016), where a specially designed helmet, containing up to 122 coils, was chosen.
Synthesized Findings and Risk of Bias
Effects on BehaviorSixteen studies assessed the effects of rTMS on ASD symptoms or ASD associated behavioral problems. Seven of these studies
were prospective and non-controlled (Sokhadze et al., 2010, 2016,
2017; Casanova et al., 2014; Wang et al., 2016; Abujadi et al., 2017; Gómez et al., 2017). Data from the study byGómez et al. (2017), who used both rTMS and transcranial direct current stimulation in their sample, could not be used as authors did not provide separate outcome data for the rTMS intervention. Two other studies, while reporting a waiting-list control design, did not provide data for the control group, and were thus analyzed jointly with non-controlled studies in a pre-post
meta-analysis design (Sokhadze et al., 2009; Baruth et al., 2010). The
remaining seven studies were controlled with either
waiting-list controls (Casanova et al., 2012; Sokhadze et al., 2014a,b),
sham-rTMS (Enticott et al., 2014; Ni et al., 2017), or sham
pico-Tesla TMS (Anninos et al., 2016, 2017). Anninos et al. (2016)
provided only a qualitative description of symptom change in their treated patients, with no quantitative assessment of change. In a recently published study from the same research group, similarly-designed to test the effects of pico-Tesla TMS on ASD symptoms, and that was not retrieved by our systematic
search strategy (Anninos et al., 2017), clinical improvement was
reported in 6 of 8 children, but described only qualitatively, rather than quantitavely, and was also not included in the data synthesis. The different studies assessed the effects of rTMS on one or more of three behavioral dimensions: restricted and repetitive or stereotyped behavior; impairments in social behavior; other non-core ASD-related symptoms, such as hyperactivity or irritability. The specific instruments used in each study are detailed in
Table 3.
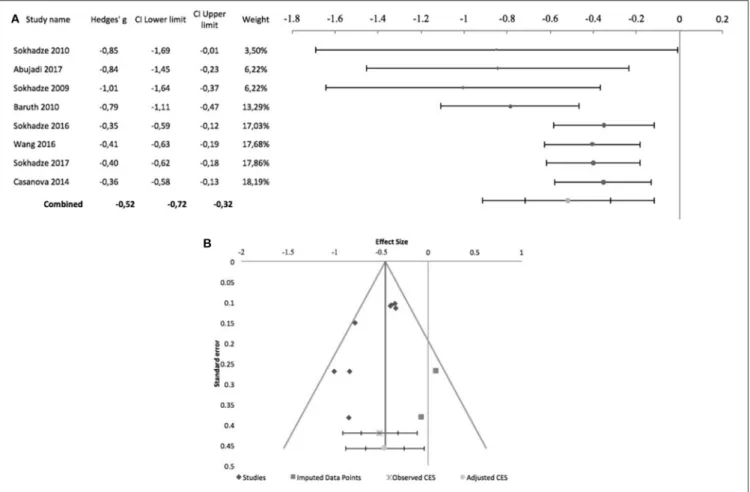
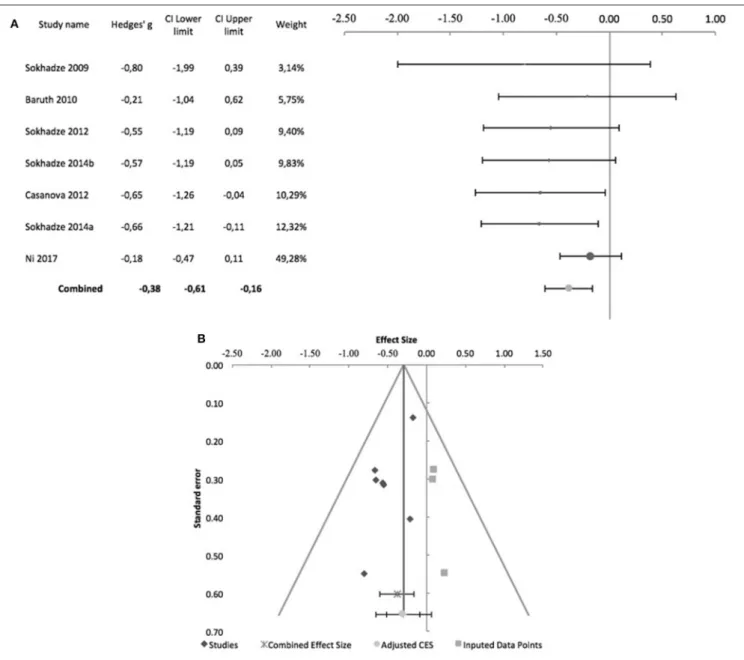
With regards to stereotyped and repetitive behavior, the effects of rTMS were measured using the total Repetitive Behavior Scale-Revised (RBS-R), stereotypy subscale of the Aberrant Behavior Checklist (ABC), Attention Switching subscale of the Autism Spectrum Quotient, or compulsion subscale of the Yale-Brown Obsessive-Compulsive Scale. In all of these scales higher scores reflect higher symptom severity. Figure 2 shows the forest plot of the pre-post analysis for 8 non-controlled studies. Three of these studies included a control group but were included in this meta-analysis as no outcome data were reported for the control
group (Sokhadze et al., 2009, 2016; Baruth et al., 2010). All of the
eight studies incurred in risk of bias, as none was subject- or rater blinded, and none used an intent-to-treat approach regarding
dropouts. All butAbujadi et al. (2017), that used iTBS, applied
low-frequency rTMS with stimulus frequencies between 0.5 and
1 Hz.Sokhadze et al. (2010)andSokhadze et al. (2009)targeted
the left DLPFC, whileAbujadi et al. (2017)stimulated the right
DLPFC. The remaining five trials chose bilateral stimulation of the DLPFC. We found a significant combined effect size of−0.52 (95% CI: −0.72 to −0.32; z = −6.17; p < 0.001), with a significant
Cochrane’s Q-test of Heterogeneity (Q = 14.4, p = 0.04), I2
-value of 51.5% and T2of 0.02. The funnel plot and trim-and-fill
analysis were suggestive of publication bias, with two missing negative studies and an adjusted effect size of−0.46 (95% CI:
FIGURE 2 | Effects of rTMS on repetitive and restricted behavior in non-controlled studies. (A) Forest-plot. Dots represent each study, with dot size reflecting study weight in the model and error bars indicating the effect size (with confidence interval). The lower line represents the combined effect size with its confidence interval (narrow interval) and its 95% prediction interval (wide interval). The latter gives the range in which, in 95% of the cases, the outcome of a future study will fall, assuming that the effect sizes of studies are normally distributed. (B) Funnel-plot. There is evidence of significant publication bias. Square-shaped dots represent studies imputed by trim-and-fill analysis.
−0.67 to −0.25; Figure 2). Egger statistic was also significant (intercept = −3.2, 95%CI: −5.5 to −0.9; t = −3.3, p = 0.02), suggesting a significant bias.
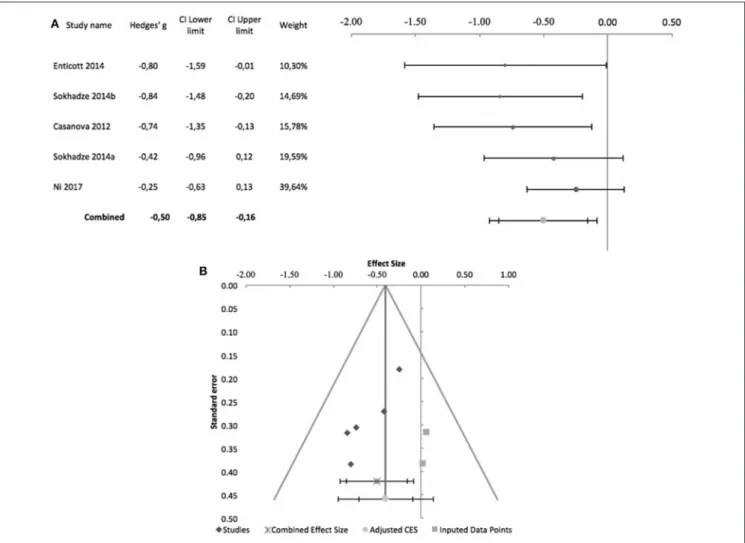
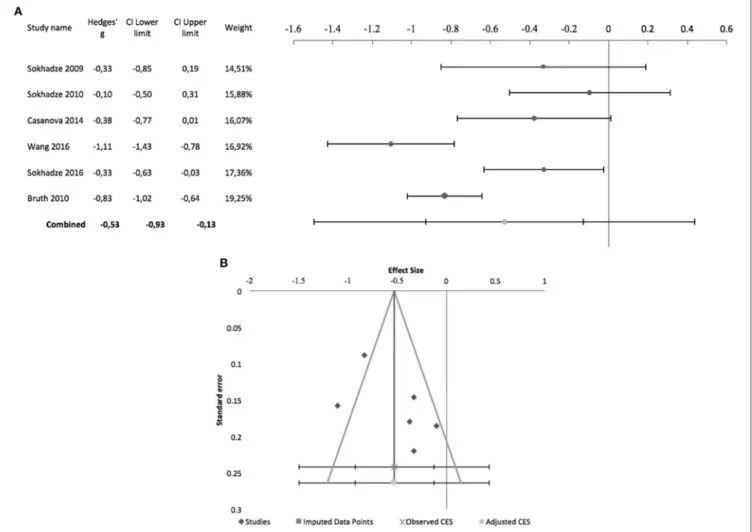
Figure 3 shows the forest plot of 5 controlled studies that assessed the effects of rTMS on stereotyped and repetitive behavior. Only one of these studies was randomized,
sham-controlled and double-blind (Enticott et al., 2014). The remaining
incurred in risk of bias due to lack of randomized treatment
attribution or adequate blinding. Moreover, onlyEnticott et al.
(2014) and Ni et al. (2017) adopted sham-controlled designs, the remainder comparing the active TMS arm with wait-list
condition.Enticott et al. (2014)stimulated the DMPFC bilaterally
at 5 Hz, using a H-coil, while Ni et al. (2017) used iTBS to
stimulate both right and left DLPFC. The remaining three studies also stimulated the DLPFC bilaterally with 1 Hz rTMS. A combined effect size of −0.5 was found (95% CI: −0.85 to −0.16; z = −4.1; p < 0.001) with a non-significant Cochrane’s
Q-test (Q = 4.4, p = 0.4), I2-value of 9% and T2 of 0.01.
The funnel plot for this combined effect size estimation was asymmetrical, and the trim-and-fill analysis was suggestive of publication bias, with two missing studies and an adjusted
effect size of −0.4 (95% CI: −0.71 to −0.1; Figure 3). Egger statistic was significant (intercept = −3.5, 95%CI: −5.7 to −1.2; t = −4.3, p = 0.02).
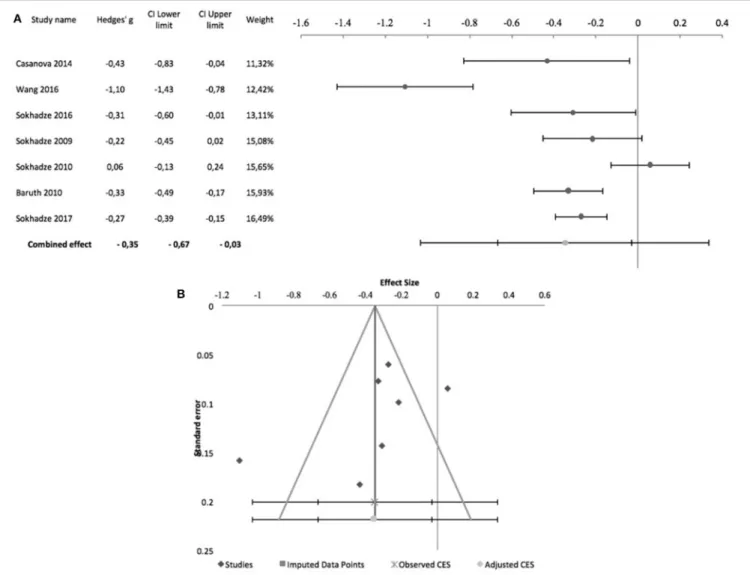
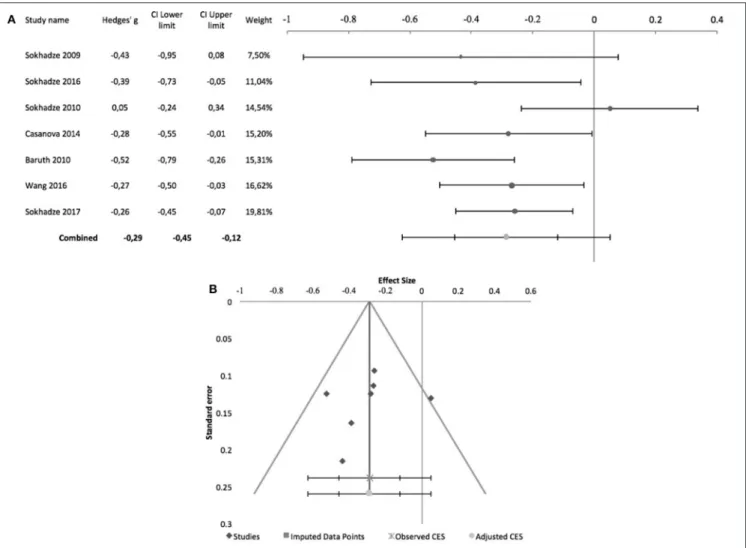
The effects of rTMS on the social behavior were computed based on the scores of the Social Responsiveness Scale (SRS), Lethargy and Social Withdrawal subscale of the ABC, or Social Relatedness subscale of the Ritvo Autism-Aspergers Diagnostic Scale (RAADS). Figure 4 summarizes pre-post design studies, comprising 7 studies, all by the same research group. Three of these studies included a control group but were included in this meta-analysis as no outcome data were reported for this
group (Sokhadze et al., 2009, 2016; Baruth et al., 2010). None of
the studies used subject or rater blinding, or an intent to treat analysis. All used stimulation frequencies between 0.5 and 1 Hz
and, except forSokhadze et al. (2009)andSokhadze et al. (2010),
all targeted the DLPFC bilaterally. These studies had a significant combined effect size of −0.35 (95% CI: −0.67 to −0.03; z = −2.7; p = 0.008). The Cochrane’s Q-test was significant (Q = 44.9,
p < 0.001), with an I2-value of 86.6% and T2 of 0.06. The
funnel plot and trim-and-fill analysis for this combined effect size estimation were not suggestive of publication bias or missing
FIGURE 3 | Effects of rTMS on repetitive and restricted behavior in controlled studies. (A) Forest-plot. Dots represent each study, with dot size reflecting study weight in the model and error bars indicating the effect size (with confidence interval). The lower line represents the combined effect size with its confidence interval (narrow interval) and its 95% prediction interval (wide interval). (B) Funnel-plot. There is evidence of significant publication bias. Square-shaped dots represent studies imputed by trim-and-fill analysis.
studies (Figure 4) and the Egger statistic was not significant (intercept = −10.4, 95% CI: −26.2 to 5.4; t = −1.6, p = 0.2).
Regarding controlled studies,Casanova et al. (2012)did not
report data on social behavior, and thus only four studies were
entered in the meta-analysis. Only Enticott et al. (2014) and
Ni et al. (2017), adopted sham-controlled designs, and only the former adopted a randomized controlled double-blind design.
Regarding stimulation targets, Enticott et al. (2014)used a
H-coil to stimulate the DMPFC at 5 Hz.Ni et al. (2017)used iTBS
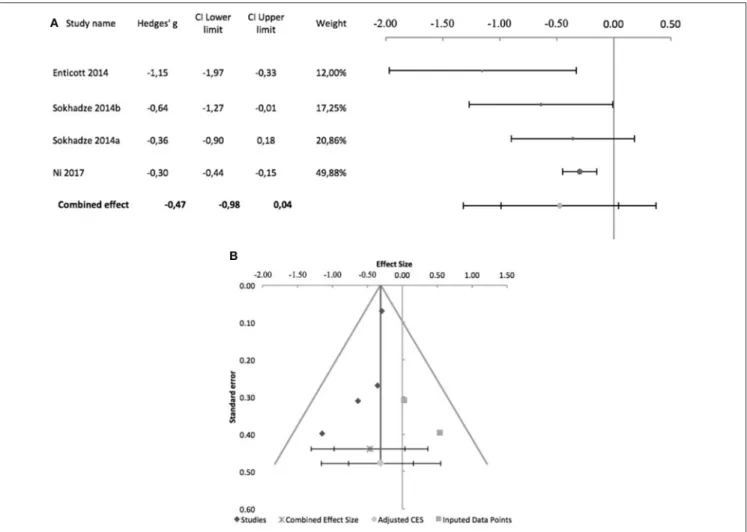
to stimulate the DLPFC, which was the target stimulated in the other two studies, albeit at low frequency (1 Hz). Figure 5 shows the forest plot of these studies, with a combined effect size of −0.47 (95% CI: −0.98 to 0.04; although z = −2.93; p = 0.003),
a non-significant Cochrane’s Q-test (Q = 5.4, p = 0.1), I2-value
of 45% and T2of 0.04. The funnel plot and trim-and-fill analysis
were suggestive of publication bias (Figure 5), with two missing studies, but Egger statistic was not significant (intercept = −2.8, 95% CI: −6.6 to 0.9; t = −2.39.3, p = 0.1). Furthermore, one
study (Enticott et al., 2014) described follow up assessments
1 month after treatment, when differences between sham and active rTMS remained significant (Hedges’ g = −1.38; 95% CI: −2.27 to −0.57, p = 0.016).
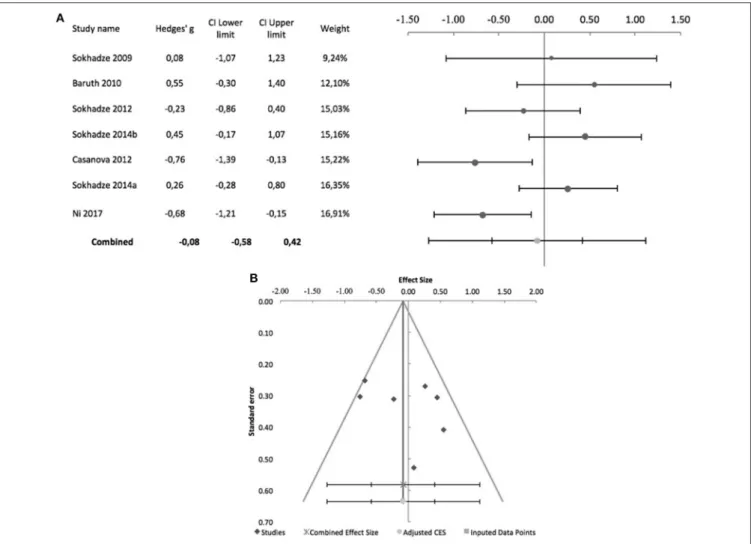
Effects of rTMS on irritability and hyperactivity were measured with the corresponding ABC subscales. Figure 6 shows the forest plot of pre-post studies for hyperactivity, with a significant combined effect size of −0.29 (95% CI: −0.45 to −0.12; z = −4.2; p < 0.001), non-significant Cochrane’s
Q-test (Q = 11.3; p = 0.08), I2-value of 46.7% and T2 of 0.01.
The funnel plot and trim-and-fill analysis for this combined effect size estimation were not suggestive of publication bias or missing studies (Figure 6), with a non-significant Egger statistic (intercept = −1.8, 95% CI: −9.1 to 5.5; t = −0.6, p = 0.6). All 7 of these studies were by the same research group. None of them was subject or rater-blinded, and all used low-frequency rTMS to stimulate the DLPFC, either bilaterally or unilaterally (see Table 2 for details). Only two controlled studies reported the effects of TMS on hyperactivity, both by Sokhadze
FIGURE 4 | Effects of rTMS on social behavior deficits in non-controlled studies. (A) Forest-plot. Dots represent each study, with dot size reflecting study weight in the model and error bars indicating the effect size (with confidence interval). The lower line represents the combined effect size with its confidence interval (narrow interval) and its 95% prediction interval (wide interval). (B) Funnel-plot.
no significant differences between active TMS and waiting-list condition (Hedges’ g = −0.36, 95% CI: −0.91 to 0.18) and the
other (Sokhadze et al., 2014a) reporting a significant interaction
between treatment arm and time (Hedges’ g = −0.71, 95% CI: −1.36 to −0.09).
Figure 7shows the forest plot of pre-post studies regarding
irritability, excludingSokhadze et al. (2017)who did not provide
data on this measure. Again, these 6 studies were all by the same research group and all incurred in risk of bias due to lack of blinding (see above and Table 2 for further details) A significant combined effect size of −0.53 was found (95% CI: −0.93 to −0.13; z = −3.4; p = 0.001) with a significant Cochrane’s Q-test
(Q = 30.8; p < 0.001), I2-value of 83.8% and T2 of 0.1. The
funnel plot and trim-and-fill analysis for this combined effect size estimation were not suggestive of publication bias or missing studies (Figure 7) and the Egger statistic was not significant (intercept = 11.5, 95% CI: −11 to 33.9; t = 1.3, p = 0.3). Figure 8 shows the forest plot of controlled studies that assessed the effects
of TMS on Irritability, excludingNi et al. (2017)andSokhadze
et al. (2014b)who did not provide data on this outcome. From
these 3 studies, only Enticott et al. (2014)had a randomized,
sham-controlled, double-blind design, while the remaining two compared active rTMS with wait-list condition (see above for stimulation parameter details). Their combined effect size was −0.3 (95% CI: −1.32 to 0.72; z = −1.3; p = 0.2), with a
non-significant Cochrane’s Q-test (Q = 3.3, p = 0.2), I2-value of
39.9% and T2 of 0.06. Funnel plot and Egger statistic were not
interpretable due to the low number of studies (data not shown). Effects on Cognitive Function
Eleven studies assessed the effects of rTMS on cognitive performance in ASD patients, eight of which were controlled studies comparing active rTMS treatment with either
waiting-list controls (Sokhadze et al., 2009, 2012, 2014a,b; Baruth et al.,
2010; Casanova et al., 2012) or sham-rTMS (Fecteau et al., 2011; Ni et al., 2017). The 3 remaining studies, comparing
FIGURE 5 | Effects of rTMS on social behavior deficits in controlled studies. (A) Forest-plot. Dots represent each study, with dot size reflecting study weight in the model and error bars indicating the effect size (with confidence interval). The lower line represents the combined effect size with its confidence interval (narrow interval) and its 95% prediction interval (wide interval). (B) Funnel-plot. There is evidence of possible significant publication bias, with 2 imputed studies (square-shaped dots) estimated by trim-and-fill analysis.
cognitive performance before and after rTMS, could not be used for meta-analysis because a common cognitive domain
was not assessed in all of them (Sokhadze et al., 2010, 2016;
Abujadi et al., 2017). Most of these studies report performance measures on a visual oddball-type task, which requires subjects to respond (e.g., press a button), or omit a response, when an infrequent stimulus appears within a series of frequent standard stimuli, presented rapidly. This type of task loads on several dimensions of executive control, namely attention control, working memory, response inhibition, and ability to shift
between alternative response strategies (Huettel and McCarthy,
2004). Performance is conventionally described in terms of
reaction-time do target stimuli, omission errors (failing to respond to the target), commission errors (responding to
non-targets), and total number of errors.Ni et al. (2017)andAbujadi
et al. (2017)used the Wisconsin Card Sorting Test, a classical and widely known neuropsychological test used to assess cognitive
set-shifting ability. Abujadi et al. (2017)additionally used the
Stroop color-word test, a classical interference control task,
while Fecteau et al. (2011) used the Boston Naming Test, a
widely used test of confrontational naming, to assess naming skills.
Sokhadze et al. (2010, 2016) while reporting no change in reaction time in oddball-type tasks after rTMS in their ASD samples, did not provide details on the underlying data, and meta-analysis was not conducted. Figure 9 shows the forest plot of the 7 controlled studies assessing the effects of rTMS on reaction time to target stimuli. All were by the same research
group except Ni et al. (2017), which was also the only that
used iTBS and a sham-treated control group. The remaining studies all used low-frequency rTMS. All studies stimulated the
DLPFC bilaterally, with the exception ofSokhadze et al. (2009)
who only stimulated the left DLPFC. None of the seven studies used subject or rater-blinding, and thus all were exposed to both performance and detection bias. The combined effect size of −0.08 was not significant (95% CI: −0.58 to 0.42; z = −0.4; p = 0.7), with a significant Cochrane’s Q-test (Q = 17.66,