www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Effect
of
conductive
hearing
loss
on
central
auditory
function
夽
Arash
Bayat
a,∗,
Mohammad
Farhadi
b,
Hesam
Emamdjomeh
c,
Nader
Saki
a,
Golshan
Mirmomeni
d,
Fakher
Rahim
aaAhvazJundishapurUniversityofMedicalSciences,HearingandSpeechResearchCenter,Ahvaz,Iran
bIranUniversityofMedicalSciences,HazratRasoulAkramHospital,HeadandNeckSurgery,DepartmentandResearchCenterof Otolaryngology,Tehran,IR,Iran
cIranUniversityofMedicalSciences,HaztatRasoulAkramHospital,DepartmentofAudiology,Tehran,IR,Iran dAhvazJundishapurUniversityofMedicalSciences,StudentResearchCommittee,Ahvaz,Iran
Received27May2015;accepted7February2016 Availableonline22April2016
KEYWORDS
Adult;
Auditorytemporal processing; Conductivehearing loss;
Gapinnoise
Abstract
Introduction:It hasbeen demonstratedthat long-term Conductive HearingLoss (CHL)may influencetheprecisedetectionofthetemporalfeaturesofacousticsignalsorAuditoryTemporal Processing(ATP).ItcanbearguedthatATPmaybetheunderlyingcomponentofmanycentral auditoryprocessingcapabilitiessuchasspeechcomprehensionorsoundlocalization.Littleis knownabouttheconsequencesofCHLontemporalaspectsofcentralauditoryprocessing. Objective: Thisstudywasdesignedtoassessauditorytemporalprocessingabilityinindividuals withchronicCHL.
Methods:During this analytical cross-sectional study, 52 patients with mild to moderate chronicCHLand52normal-hearinglisteners(control),agedbetween18and45year-old,were recruited.Inordertoevaluateauditorytemporalprocessing,theGaps-in-Noise(GIN)testwas used.Theresultsobtainedforeachearwereanalyzedbasedonthegapperceptionthreshold andthepercentageofcorrectresponses.
Results:TheaverageofGINthresholdswassignificantlysmallerforthecontrolgroupthanfor theCHLgroupforbothears(right:p=0.004;left:p<0.001).IndividualswithCHLhad signifi-cantlylowercorrectresponsesthanindividualswithnormalhearingforbothsides(p<0.001). NocorrelationwasfoundbetweenGINperformanceanddegreeofhearinglossineithergroup (p>0.05).
夽 Pleasecitethisarticleas:BayatA,FarhadiM,EmamdjomehH,SakiN,MirmomeniG,RahimF.Effectofconductivehearinglosson
centralauditoryfunction.BrazJOtorhinolaryngol.2017;83:137---41.
∗Correspondingauthorat:HearingandSpeechResearchCenter,AhvazJundishapurUniversityofMedicalSciences,Ahvaz,Iran.Tel.:+98
9183615157.
E-mail:[email protected](A.Bayat).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.02.010
Conclusion:TheresultssuggestreducedauditorytemporalprocessingabilityinadultswithCHL compared tonormalhearing subjects.Therefore,developingaclinicalprotocoltoevaluate auditorytemporalprocessinginthispopulationisrecommended.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Adulto; Processamento temporalauditivo; Perdaauditiva condutiva;
Gapnoruído
Efeitodaperdaauditivacondutivanafunc¸ãoauditivacentral
Resumo
Introduc¸ão:Jáfoidemonstradoqueaperdaauditivacondutiva(PAC),emlongoprazo,pode influenciarnadetecc¸ãoprecisadascaracterísticastemporaisdossinaisacústicosoudo pro-cessamento auditivotemporal(PAT).Pode-seargumentarqueoPAT podeserocomponente subjacentedemuitosrecursosdoprocessamentoauditivocentral,comoacompreensãodafala oulocalizac¸ãodosom.PoucosesabesobreasconsequênciasdaPACnosaspectostemporaisdo processamentoauditivocentral.
Objetivo:Esteestudofoiprojetadoparaavaliaracapacidadedeprocessamentoauditivo tem-poralemindivíduoscomPACcrônica.
Método: Duranteesteestudotransversalanalítico,52pacientescomPACcrônicalevea moder-adae52indivíduoscomaudic¸ãonormal(controle),idadesentre18e45anos,foramrecrutados. Paraavaliaroprocessamentoauditivotemporal, foiutilizadootestederesoluc¸ãotemporal Gaps-in-Noise (GIN). Osresultados obtidos para cadaorelha foramanalisados com baseno limiardepercepc¸ãodaquebradecontinuidade(gap)enaporcentagemderespostascorretas. Resultados: AmédiadoslimiaresnoGINfoisignificativamentemenorparaogrupocontroleque paraogrupoPACemambasasorelhas(direita:p=0,004;esquerda:p<0,001).Osindivíduos comPACapresentaramrespostascorretassignificativamentemaisbaixasqueosindivíduoscom audic¸ãonormalemambasasorelhas(p<0,001).Nãohouvecorrelac¸ãoentreodesempenhono GINeograudeperdaauditivaemambososgrupos(p>0,05).
Conclusão:Osresultadossugeremumareduc¸ãodacapacidadedeprocessamentoauditivo tem-poralemadultoscomPACcomparadoscomindivíduosapresentandoaudic¸ãonormal.Portanto, odesenvolvimentode umprotocolo clínico paraavaliaroprocessamento auditivotemporal nessapopulac¸ãoérecomendado.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
ChronicConductiveHearing Loss(CHL)ischaracterizedby reducedefficiencyofsoundtransmissionthroughthe exter-nal and/ormiddle earand usuallyinvolves a reductionin soundlevelortheabilitytohearfaintsounds.Several inves-tigatorshavearguedthatthislong-termsensorydeprivation may produce irreversible changes in the anatomical and functional integrity of the central auditory structures,1---3
suchaschangesintherelativesizeofneurondendritesin subcorticalnuclei4,5orsynapticandspikeadaptation
disrup-tionsintheauditorycortex.6
It has been also demonstrated that auditory depriva-tion following CHL may be associated with a number of sensory and cognitive difficulties as well as deficits in psychosocial development.6---8 These problems may
con-tinue long after hearing thresholds return to normal limits.
CHLmayinfluencetheaccurateprocessingofthe time structureoftheacousticsignal,e.g.delayslowfrequency
sounds entering the inner ear by up to150s.9 Auditory
Temporal Processing (ATP), one of the (central) auditory processingmechanisms,referstotheabilityoftheauditory systemtoprocesstemporalcharacteristicsofasound stim-ulus withinaspecific timeperiod.2,5,10,11 Itcanbe argued
thatATPmaybetheunderlyingcomponentofmanyauditory processingcapabilities,includingtheprocessingofspeech transientsandvoicinginformation,segregationofauditory figure fromauditory groundandlocalizationcues,12,13 and
beingaprerequisiteforspeechandlanguageacquisition.14
Thisnotioncanbeobservedatdifferentlevelsrangingfrom theneuronalsensitivityoffirstorderneuronstothecortical level.15,16
TheGaps-In-Noise (GIN)testprovidesaclinically feasi-blemethodofassessingATP,temporalresolution,wherein thesubjectsarerequiredtodetectgapswithinacontinuous auditorystimulus.3,17Thistestcouldbeeasilyadministered
auditory nervous system dysfunction in adult populations while still demonstrating clinical feasibility.15 It has been
shownthatGINismoresensitivetocorticalcompromiseas opposedtobrainstemdeficits.15
Aravindkumaretal.7reportedbilaterallyimpaired
tem-poral processingability in their study of 26 patients with refractory complex partial seizures and Mesial Temporal Sclerosis(MTS).Patientsweredividedintotwogroups:right MTS(n=13;meanage:31years)andleftMTS(n=13;mean age: 25.76years). Fiftyhealthy subjects(mean age: 26.3 years) constituted the control group. They reported that bothMTSgroupsshowedlongerGINthresholdsandless per-centageofcorrectresponsesinbothearswhencomparedto thecontrolgroup.ThesefindingsshowthatGINissensitive tocorticallesions.
While it has been known that a CHL can distort audi-tory processing, the effect of CHL on temporal aspects of auditory processing has received little attention. The purpose of this study was to investigate the effects of CHL on auditory temporal ability by employing the GIN test.
Methods
Participants
This was an analytical cross-sectional study approved by theLocalResearchEthicsCommittee,andinformedconsent wasobtainedfromallparticipants.Thesampleconsistedof 104adultsaged18---45years(mean:27.02years)whowere referredtotheotolaryngologydepartmentinageneral hos-pital.Theywereselectedinaconsecutivesamplingmethod andclassifiedintotwogroups:
Control group (n=52): This group was composed of healthy subjects without a history of otitis media and showed a threshold of 10dB HL or less for octave frequenciesbetween 250Hzand 8000Hz,bilaterally. Tym-panograms were recorded normally (Type An) in both ears.
CHLgroup(n=52):Thisgrouphadbilateralsymmetrical mildtomoderateCHLwithpure-toneaverages(500,1000, 2000Hz)rangingfrom34to51dBHLandmonosyllabicword recognitionscoresinquiet of90%orgreater.The onsetof diseasewasgreaterthantwoweeksandthechiefcomplaint was hearing loss sensation. The patients were evaluated usingotomicroscopicandComputedTomography(CT) exam-inations, and subjects with cholesteatoma or craniofacial abnormalitieswereexcluded.
Bothgroupswerematched forageandgender.All sub-jectswereright-handedandnativespeakersofPersianand showed normal scores onthe Mini-Mental State Examina-tion(MMSE).TheMMSEisausefulscreeninginstrumentfor assessingglobalcognitivefunction.Itevaluatesfiveareasof cognitivefunction:orientation,registration,attentionand calculation,recall,andlanguage.Scoringonthistestvaries from0to30points;higherscoresindicatebettercognitive functioning.Acut-offof23pointswasusedforourIranian sample.16
Individuals with a history of metabolic, psychiatric, developmentalorneurologicalproblemswerealsoexcluded fromthestudy.
Procedures
Allparticipantsweretestedwhileseatedinadouble-walled sound-treatedbooth.Pure-toneaudiometrywasperformed usinga calibrated audiometer (Amplaid A321, Italy), and frequencies from 250 to 8000Hz were tested using the ascending---descendingmethodwithastepsizeof5dBHL.
TheGINstimuli,whichwererecordedonacompactdisc, wereplayed on a SonyDVPN728H DVD player and passed throughthe speechcircuitry of an audiometer toTDH-39 matchedheadphones. Thestimuliwere presented monau-rallyat45dBSL(relativetothemeanpuretonethresholds at500,1000and2000Hz)andthetestdurationwas approx-imately16minforeach participant.TheGIN lists1,2and 3 were applied, alternately, in the right and left ears of eachindividual.Subjectswereaskedtoidentifythegaps dis-tributedthroughout6secondsofwhitenoisepresentation. Eachtest listwascomposedof0---3silentintervalsorgaps containedwithineach6-secondsegmentofwhitenoise.The interstimulusintervalbetweennoisesegmentswas5s.The durationofeachgapwas2,3,4,5,6,8,10,12,15or20ms, andtheywererandomly distributed sothat 60gaps(6 of eachduration)werepresentedin eachlist.Eight practice itemsprecedethe administrationof thetest items.15 The
participantswere instructed topressthe responsebutton assoon astheyperceived a gap or a silencein the noise segmentspresented.
Theresultsobtainedforeachearwereanalyzedbasedon thegapperceptionthresholdandthepercentageofcorrect responses. The GIN threshold wasdefinedas theshortest gapduration forwhich therewereat least 4of 6 correct identifications.Sincetherewere 60gapsin each list,the percentageofcorrectresponseswasdefinedandcalculated as the percentage of correct responses scored across all gaps15: (Total number of gaps identified/total number of
gapsinthelist)×100.
The Statistical Package for the Social Sciences (SPSS) forWindowswasusedfor statisticalanalysis.The inferen-tial statistical analyses were conducted using parametric tests, since, after submitting the data set to the Kolmogorov---SmirnovTest (fornormaldistributionofdata) andthe Levene’sTest (for homogeneity of variances), we foundthattheresultsmettherequisitesfortheapplication ofparametrictests.Therefore,theindependentsample t -test and paired t-test were used. The level of statistical significancewassetat0.05.
Results
IntheCHLgroup,themeanPureToneAverage(PTA) thresh-old for the right and left ears were 41.03±7.29dBHL and40.89±8.37dBHL,respectively. Inthe control group, themean PTA thresholdfor theright andleft sideswere 6.08±3.44dBHLand5.56±4.15dBHL,respectively.
Table 1 Comparison of the percentage of correct responses(%)betweenthecontrolandConductive Hearing Loss(CHL)groups.
Ear Controlgroup CHLgroup p-Value
Mean SD Mean SD
Right 72.88 6.89 63.95 9.51 <0.001 Left 73.54 6.12 64.30 8.24 <0.001
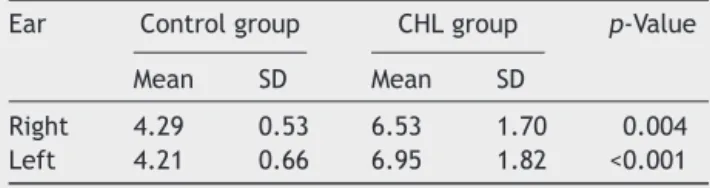
Table2 ComparisonoftheGINthreshold(ms)betweenthe controlandConductiveHearingLoss(CHL)groups.
Ear Controlgroup CHLgroup p-Value
Mean SD Mean SD
Right 4.29 0.53 6.53 1.70 0.004 Left 4.21 0.66 6.95 1.82 <0.001
numberofpercentcorrectresponses tothe GINtest. The comparisonofGINscoresbetweentheearsshowedno sig-nificantdifferences between earsin either group(control group,p=0.33;CHLgroup,p=0.19).
Table 2 shows the comparison of the GIN threshold between the control and the CHL groups. The results of theindependentsamplet-testrevealedthatthemeanGIN thresholdsweresignificantlysmaller(better)forthecontrol groupthanfortheCHLgroupforbothears.Theresultsofthe pairedt-testshowednosignificantdifferencesbetweenthe earsineithergroup,whichindicatessimilarityofresponses between ears in each group (control group, p=0.51; CHL group,p=0.21).
Inter-listcomparisons
Two lists of 60 GIN items per list were used in the cur-rentstudy.Thirtycontrolsubjectswereadministeredthree lists (list 1, list 2 and list 3) in random order to estab-lishinter-listequivalence. A one-wayanalysisof variance demonstrated no significant differences across lists for eitherear(p=0.12).
Discussion
Theresults ofthecurrent studyindicated thatindividuals withCHLneedalongerdurationtodetectgapsontheGIN testcomparedtoindividuals withnormalhearing sensitiv-ity.Additionally, we found ahigher percentageof correct responsesincontrollistenersversusCHLsubjects.The find-ingofreducedgapdetectionabilityinCHLpatientsagrees withfindingsofBalenetal.18 Theseauthorscomparedthe
temporal resolution ability of children with normal hear-ing (n=12), with those bearing CHL (n=7) and auditory processing disorders(n=12) usingRandom Gap Detection Test(RGDT).Theirfindingsdemonstratedthatchildrenwith hearingimpairmentexhibitedsignificantlyhighergap detec-tion thresholds than those children with normal hearing sensitivity.However,theystated thatRGDTtest hasgreat performancevariabilityinassessingtheauditorytemporal resolution.
The ability to make fine temporal discriminations of acoustic signals is an important element in analyzing the characteristicsofsensoryinputandcontributestoanumber of auditoryperceptions,includingcertainspeech compre-hensionsituationsandsoundlocalization.19,20Neuronsalong
the central auditory pathways maintain the precise tim-ingofspikes, whichis attributabletospecializedsynaptic mechanisms (for example, via calyx synapses, the largest synapses intheauditory brainstem)andbiophysical mem-brane properties.21---23 It seems that these characteristics
areveryimportantfordetectingtheacousticfeaturesthat changeonmillisecondtimescales.6
Ithasbeen shownthatthecentralpartoftheauditory systemrespondsdynamicallytothelevelofneuralinputit receivesfromthe ears.Xuetal. 6 revealedthat CHL
sig-nificantly alters temporally-preciseproperties of auditory cortexsynapsesandspikes,andthismaycontributetoATP deficitscausedbymildtomoderatehearingloss.These find-ingsshowthattheauditorysystemrespondsdynamicallyto thelevelofneuralinputitreceivesfromtheears.
Musiek et al. 15 showed that the GIN test is sensitive
in confirming lesions of the central auditory nervous sys-tem,beingevenmoresensitivetocorticaldamage.Inthe presentstudy,thedifferencefoundbetweenthetwogroups intheperformanceontheGINtestindicatescentral audi-tory nervous system dysfunction in patients with chronic CHL.
In the present study, signals were presented at an equalsensationlevelfor alllisteners,whichissignal level re-absolute threshold. Stimulus level is known to be an important factor in psychophysical assessments such as temporalresolutiontests.Insomeoccasions,subject’s per-formance may improvewith an increase in stimulus level untilasymptoticperformanceisachieved.18,24
TheGIN test resultsinourstudy showedasimilar per-formance in test lists 1, 2 and 3 regardless of which ear startedtheexam.Thesefindingsindicatenolearningeffect orfatigue,ashasbeenobservedinothersimilarstudies.11
Noadvantageof oneearover theother in GIN thresh-oldsandpercentageofcorrectanswerswereobserved.Our resultsareinagreementwithotherpublishedpaperswhere noperceptualasymmetrybetweentheearswasreportedfor gap detection.11,15 However,SiningeranddeBode25 found
asmaller left-earadvantagefor gapdetectionusingtonal stimuli.
Conclusion
The findings of the current investigation showed that auditory temporal resolution ability has been impaired in individuals with CHL versus normal hearing subjects. Therefore, developing a clinical protocol to evaluate auditory temporal processing in this population is highly recommended. Furthermore, identification of such cen-tralauditorydisordersin patientswithhearingloss would provideabetterinsighttomoreeffectiveinterventions.
Conflicts
of
interest
References
1.DoyleWJ,WebsterDB.Neonatalconductivehearinglossdoes notcompromisebrainstemauditoryfunctionand structurein rhesusmonkeys.HearRes.1991;54:145---51.
2.PopescuMV,PolleyDB.Monauraldeprivationdisrupts develop-mentofbinauralselectivityinauditorymidbrainandcortex. Neuron.2010;65:718---31.
3.TollinDJ.Thedevelopmentofsoundlocalizationmechanisms. In: BlumbergMS, FreemanJH, Robinson SR, editors.Oxford handbookofdevelopmentalbehavioral.Neuroscience:Oxford UniversityPress;2010.p.262---82.
4.TucciDL,CantNB,DurhamD.Effectsofconductivehearingloss ongerbilcentralauditorysystemactivityinsilence.HearRes. 2001;155:124---32.
5.SumnerCJ,TucciDL,ShoreSE.Responsesofventralcochlear nucleusneuronstocontralateralsoundafterconductivehearing loss.JNeurophysiol.2005;94:4234---43.
6.Xu H, KotakVC, SanesDH. Conductivehearing lossdisrupts synapticand spikeadaptation indevelopingauditorycortex. JNeurosci.2007;27:9417---26.
7.AravindkumarR,ShivashankarN,SatishchandraP,SinhaS,Saini J,SubbakrishnaDK.Temporalresolutiondeficitsinpatientswith refractorycomplexpartialseizuresandmesialtemporal scle-rosis(MTS).EpilepsyBehav.2012;24:126---30.
8.BalenSA,BretzkeL,MottecyCM,LiebelG,BoenoMR,Gondim LM.Temporalresolutioninchildren:comparingnormalhearing, conductivehearinglossandauditoryprocessingdisorder.Braz JOtorhinolaryngol.2009;75:123---9.
9.MooreDR,HartleyDE,HoganSC.Effectsofotitismediawith effusiononcentral auditoryfunction.IntJPediatr Otorhino-laryngol.2003;67:S63---7.
10.KoravandA, JutrasB, Roumy N. Peripheralhearing lossand auditorytemporal ordering ability in children. IntJ Pediatr Otorhinolaryngol.2007;74:50---5.
11.AmaralMI,Colella-SantosMF.Temporalresolution:performance ofschool-agedchildrenintheGIN---Gaps-in-noisetest.BrazJ Otorhinolaryngol.2010;76:745---52.
12.CampbellK,MacdonaldM.Theeffectsofattentionand con-sciousstateonthedetectionofgapsinlongdurationauditory stimuli.ClinNeurophysiol.2011;122:738---47.
13.Soros P,Teismann IK,Manemann E,Lutkenhoner B. Auditory temporal processing in healthy aging: a magnetoencephalo-graphicstudy.BMCNeurosci.2009;10:34.
14.Murphy CF, Schochat E. How auditory temporal processing deficits relate to dyslexia. Braz J Med Biol Res. 2009;42: 647---54.
15.MusiekFE,ShinnJB,JirsaR, Bamiou DE,Baran JA,ZaidaE. GIN (Gaps-In-Noise) test performance in subjects with con-firmedcentralauditorynervoussysteminvolvement.EarHear. 2005;26:608---18.
16.AnsariNN,NaghdiS,HassonS,ValizadehL,JalaieS.Validation ofaMini-MentalStateExamination(MMSE)forthePersian pop-ulation:apilotstudy.ApplNeuropsychol.2010;17:190---5. 17.FrisinaRD.Subcorticalneuralcodingmechanismsforauditory
temporalprocessing.HearRes.2001;158:1---27.
18.Weihing JA, Musiek FE, Shinn JB. The effect of presenta-tionlevelontheGaps-In-Noise(GIN)test.JAmAcadAudiol. 2007;18:141---50.
19.Michalewski HJ, Starr A, Nguyen TT, Kong YY, Zeng FG. Auditory temporal processes in normal-hearing individuals and inpatients withauditoryneuropathy.ClinNeurophysiol. 2005;116:669---80.
20.HelferKS,VargoM.Speechrecognitionandtemporalprocessing inmiddle-agedwomen.JAmAcadAudiol.2009;20:264---71. 21.Rose HJ, Metherate R. Auditory thalamocortical
transmis-sion is reliable and temporally precise. J Neurophysiol. 2005;94:2019---30.
22.Eric Lupo J, Koka K, Thornton JL, Tollin DJ. The effects of experimentallyinducedconductivehearinglossonspectraland temporalaspectsofsoundtransmissionthroughtheear.Hear Res.2011;272:30---41.
23.OertelD.Theroleoftiminginthebrainstemauditorynuclei ofvertebrates.AnnRevPhysiol.1999;61:497---519.
24.ReedCM,BraidaLD,ZurekPM.Reviewarticle:reviewofthe literature on temporal resolution in listeners with cochlear hearing impairment: a critical assessment of the role of suprathresholddeficits.TrendsAmplif.2009;13:4---43. 25.SiningerYS,deBodeS.Asymmetry oftemporalprocessingin