Braz. Dent. J. vol.21 número3
Texto
Imagem
Documentos relacionados
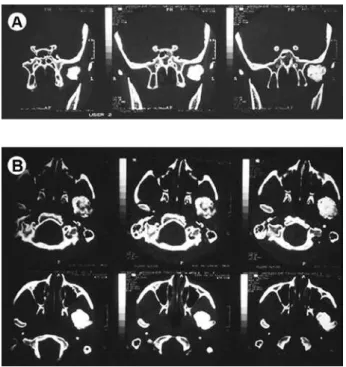
The clinical features of the fibrous-ankylosis are severely limited mouth-opening capacity (limited range of motion during the opening), usually no pain and no joint sounds,
Dos objectivos traçados no nosso trabalho, verificamos que da análise quantitativa da transição das Lux GAAP para as IFRS nas diferentes rubricas, bem como nos
Figura 20: Utilização do cluster pelos experimentos com 90% para limite superior, 40% para limite inferior e 45% para média exponencial. tempo para a finalização dos
In the former Chapter, I have given you a short Account of that Part of the Laws of England which is called Lex Scripta, namely, Statutes or Acts of Parliament, which in their
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
[r]
Ousasse apontar algumas hipóteses para a solução desse problema público a partir do exposto dos autores usados como base para fundamentação teórica, da análise dos dados
Esta pesquisa pode ser descrita como um estudo de caso, com abordagem qualitativa e quantitativa, que utilizou a técnica de entrevista (mapeamento cognitivo) para coletar dados
