ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
The
representation
of
getting
ill
in
adolescents
with
systemic
lupus
erythematosus
夽
Ondina
Lúcia
Ceppas
Resende
a,b,∗,
Maria
Tereza
Serrano
Barbosa
c,d,
Bruno
Francisco
Teixeira
Simões
d,e,
Luciane
de
Souza
Velasque
d,faUniversidadeFederaldoEstadodoRiodeJaneiro(UNIRIO),RiodeJaneiro,RJ,Brazil bHospitalFederaldosServidoresdoEstado,RiodeJaneiro,RJ,Brazil
cUniversidadedoEstadodoRiodeJaneiro(UERJ),RiodeJaneiro,RJ,Brazil
dDepartamentodeMatemáticaeEstatística,UniversidadeFederaldoEstadodoRiodeJaneiro(UNIRIO),RiodeJaneiro,RJ,Brazil ePontifíciaUniversidadeCatólicadoRiodeJaneiro(PUC-Rio),RiodeJaneiro,RJ,Brazil
fEscolaNacionaldeSaúdePública(ENSP),Fundac¸ãoOswaldoCruz(Fiocruz),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received20July2015 Accepted25February2016 Availableonline12April2016
Keywords:
Systemiclupuserythematosus Chronicdisease
Health-diseaseprocess Freeassociation Userembracement
a
b
s
t
r
a
c
t
Introduction:Thisstudy,developedinafederalhospitalinthecityofRiodeJaneiro,hasaimed toanalyzethesocialrepresentationofchronicdiseaseanditstreatment,intheperspective ofadolescentsandtheircaregivers.
Methods:Thesampleconsistedof31 adolescents(11–21years)withsystemiclupus ery-thematosusand19caregivers(32–66years),followedinthepediatricsandintheinternal medicineoutpatientclinicsforaperiodofsixmonths.Datawascollectedfromthefree associationofwordstest,usingchronicdiseaseandtreatmentofchronicdiseaseimpulses,and latersubmittedtotheMultipleCorrespondenceAnalysisusingtheRsoftware.
Results:Thegroupofadolescentsassociatedtheimpulsechronicdiseasewiththewords medication,bad,illness,difficulty,nocure,faithandjoy;andinthegroupofcaregivers,tocare, treatment,nocureandtheword‘no’.Theimpulsetreatmentofchronicdiseasewasassociated, inthegroupofadolescents,withthewordspatience,improvement,help,affection,careand bad;andinthegroupofcaregivers,tocaring,hope,schedule,knowledge,obedience,medication, professionalandimprovement.Caregiversalsoassociatedimpulsesandwordsaccordingto age:chronicdiseasewasassociatedwiththewordcare(over61years),painandimpotence (42–61years),treatment(22–41years);andtreatmentofchronicdisease,withthewordsstrength (over61years),professional,knowledgeandimprovement(42–61years),affectionandschedule (22–41years).
Conclusions:Consideringassubjectiveanddynamictheexperienceofgettingill,knowingthe representationscancontributetotheorientationofconductandtypeofpsychotherapeutic interventionneeded.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
ThisresearchwasdevelopedintheHospitalFederaldosServidoresdoEstado,RiodeJaneiro,RJ,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](O.L.CeppasResende). http://dx.doi.org/10.1016/j.rbre.2016.03.016
A
representac¸ão
do
adoecer
em
adolescentes
com
lúpus
eritematoso
sistêmico
Palavras-chave:
Lúpuseritematososistêmico Doenc¸acrônica
Processosaúde-doenc¸a Associac¸ãolivre Acolhimento
r
e
s
u
m
o
Introduc¸ão: Esseestudo,feitoem umhospitalfederalnacidadedoRio deJaneiro,teve por objetivoanalisara representac¸ãosocialdadoenc¸acrônicaedeseutratamento,na perspectivadeadolescentesedeseuscuidadores.
Métodos: A amostra consistiu de31 adolescentes(11–21 anos)com lúpuseritematoso sistêmico e 19 cuidadores (32–66 anos),seguidos em servic¸ospediátricos e de clínica médicaduranteseismeses.Foramcoletadosdadoscomaaplicac¸ãodoTestedeAssociac¸ão Livrede Palavras,comousodos impulsosdoenc¸a crônicae tratamentoda doenc¸acrônica, maistardesubmetidosàAnálisedeCorrespondênciaMúltiplacomousodoprogramade computadorR.
Resultados: Ogrupodeadolescentesassociouoimpulsodoenc¸acrônicacomaspalavras remédio,ruim,doenc¸a,dificuldade,semcura,fé,ealegria;eogrupodecuidadorescomaspalavras carinho,tratamento,semcura,ecomapalavra“não”.Oimpulsotratamentodadoenc¸acrônicafoi associado,nogrupodeadolescentes,comaspalavraspaciência,melhoria,ajuda,afeto,carinho eruim;e,nogrupodoscuidadores,comaspalavrascarinho,esperanc¸a,horário,conhecimento, obediência,remédio,profissionalemelhoria.Oscuidadorestambémassociaramosimpulsos epalavrasdeacordocomafaixaetária:doenc¸acrônicafoiassociadoàpalavracarinhoofsti (>61anos),doreimpotência(42–61anos),tratamento(22–41anos);etratamentodadoenc¸acrônica foiassociadoàspalavrasforc¸a(>61anos),profissional,conhecimentoemelhoria(42–61anos), afetoehorário(22–41anos).
Conclusões: Considerandoa experiênciadoadoecer comosubjetivae dinâmica,o con-hecimento dasrepresentac¸ões podecontribuirparaa orientac¸ão da condutae tipode intervenc¸ãopsicoterapêuticanecessária.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theconceptofhealthhasbeendiscussedovertheyearsand, withthecreationoftheUnifiedHealthSystem(SUS),healthis nowconsideredasarightofallcitizensandadutyoftheState (HealthOrganicLawn◦8080/1990,basedonArticle198ofthe FederalConstitutionof1988).Withtheincreaseinthedebates prioritizinghumanization,in2004theMinistryofHealth reg-ulated the National Humanization Policy (NHP),aiming to improverelationsbetweenprofessionals,users,hospitaland community.1
Humanizationappearsasatransversalpolicythatintents toovercometheboundariesofthedifferentknowledgeand powerintheproductionofhealth.2
With the proposal to humanize care and management
practice,the NHPpervades the SUSnetwork from aset of
actions and mechanisms3 – among which we must
high-lighttheattentionthatreferstoamodeofoperationofwork processes,rangingfromtheuser’sreceptioninthehealth sys-tem and full accountof their needs, to the solving ofthe problem.3,4
Regardingthepillarsoftheattention,onecanfindthe qual-ificationofrelationswithextendedlisteningandattentionto userneeds.Thatis,theattentionappearsasanintervention toolthatinvolvesconcernforthequalityandthekindof listen-ingthatisoffered.Beingabletohearandmakeoneselfheard isessentialsothatonecanbringup,onthehealthcarescene,
twosubjectsandamediatorobject(suffering,risks, dysfunc-tion),andnotasubject-professionalandhis/herobject-user.5
Especially inachronic illnesssituation –a conditionin whichthesubjecthastolivewithfortherestofhis/herlife6–
becomesessentialapracticebasedonthedialogical, interac-tiveandcaretakingdimension,wherethesubjectisperceived asanactiveandco-responsibleparticipantintheprocessof healthproduction.7,8
Knowing the meanings ofgetting ill, from the study of socialrepresentations,mayfavorthelisteningabilityofthe professionalsduringthecaringprocess,facilitatesocial com-municationandguideconducts.9
TheconceptofSocialRepresentation(SR)wasdefinedby MoscoviciinhisdoctoralthesisentitledLapsychanalyse,son imageetsonpublic(1961)andsubsequentlyfurtherdeveloped byJodelet(2001).Thus,SRwouldbe“asociallydevelopedand sharedformofknowledgethatcontributestotheconstruction ofacommonrealitytoaparticularsocialgroup”.10,11
Severalauthors statethatthereissuccessive correspon-dencebetweenthemeaningsthateachpersonattributesto the factsintheworldsharedincommon,12,13 andthat the
socialrealityinfluencesthewayeachpersonthinksandacts, includingonthediseasesituation.14–16Thatis,theexperience
ofthediseasedependsonwhatindividualsandsocialgroups understandbydisease,andhowtoplacethemselvesinface
ofit.14,17,18
andperceptionsofthesubjects,inascenarioofgettingilland ofcare.
The chosen disease was systemic lupus
erythemato-sus(SLE)–achronic, multisysteminflammatorydisease of unknowncauseandautoimmunenature,characterizedbythe presenceofautoantibodies,19,20 andthatcanleadto
physi-caland/orfunctionaldisability.21,22Accordingtosomestudies,
24–59%ofSLEpatientsmayhaveneurologicalimpairmentand neuropsychiatricandpsychofunctionalsyndromes.19–21
Theinclusionoftheenvironmentandofsocialfactorsin theunderstandingofSLEpatientswasshowntoberelevant,to theextentthatthereisaconsensusinthescientific commu-nityaboutthemultifactorialetiologyofSLE,suggestingthat thisdiseasehashormonal,genetic,infectious,environmental andpsychologicalcauses.20–23Formanyinvestigators,this
lat-tercausationisassociatedasamajorfactorfortheworsening ofthedisease.20,23–25
From the above, this study aimed to analyze the social representationsofchronicdiseaseanditstreatment,inthe perspectiveofadolescentsand/ortheircaregivers,hopingto bringacontributiontotheattentionofadolescentswithSLE.
Methods
ThisstudywasapprovedbytheResearchEthicsCommittee oftheHospitalFederaldosServidoresdoEstado(HFSE)under theopinionn◦456,572.
Data collectionwas conductedfrom February toAugust 2014,inthepediatricsandinternalmedicineoutpatientclinics andinthedaycarehospital.Allparticipantssignedaconsent form.
Inclusionandexclusioncriteria
Adolescentsaged11–21yearsdiagnosedwithawell-defined SLE,accordingtotheAmericanCollegeofRheumatology crite-ria and their caregivers were defined as participants. The classificationcriteria proposed in1982and revised in1997 arebasedonatleastfourofelevencriteria:malarrash, dis-coidlesion,photosensitivity,oralandnasalulcers,arthritis, serositis,renalimpairment,neurological,hematologicaland immunologicalchanges,andantinuclearantibodies.25–28
Asinclusioncriteria,onlypatientswithdiseasedurationof atleastsixmonthswereconsidered.
Takingintoaccountthatdifferentdiseaseshavedifferent impactsonthequalityoflifeofaffectedindividuals,aswellas intheperceptionofthediseaseandgettingill,theadolescents whohadotherdiseases,inadditiontolupus,wereexcluded, apartfromthefactthatthetypeandtheintensityofSLE mani-festationsimplylargerorsmallerdosesofcorticosteroids,and thatthismedicationcausespsychiatricdisordersintheshort term,inadditiontovariousadverseeffectsinthelongrun, thatmayinterfereinthesearchresults.
The caregivers were not carriers of lupus or any other chronicdisease,buttheirinclusioninthestudywas impor-tant,inordertobeawareofthemeaningsattributedtothe gettingill conceptfortheseindividuals,forthe purposeof comparingtheresultsbetweenthetwogroups(adolescents
and caregivers), considering that the family/cultural back-groundcaninterferewiththesignificanceprocess.12,13
Thesampleconsistedof31adolescentsand19caregivers (mother,father,grandparents),andtheageandlevelof edu-cationwerecategorized.Agegroups:11–21yearsrelativeto adolescents;over 61years,42–61years and22–41yearsfor caregivers.Thelevelofeducation(LE)was: higherlevelsof education(over12years);highschool(10–12years); elemen-taryschoollevelII(6–9years);andilliteracy/elementaryschool levelI(0–5years).
Thegroupofadolescentsaged11–21yearswascomposed of4boysand27girls;andthatofcaregiverswith32–66years old,2menand17women.Thelevelofeducation(LE)varied ineachgroup.TheLEofadolescentswas:higherlevelof edu-cation,12.90%,highschool,64.52%,andelementaryschoolII, 22.58%.TheLEofcaregiverswas:higherlevelofeducation, 15.79%,highschool,31.58%,elementaryschoolII,21.05%,and illiteracy/elementaryschoolI,31.58%.
Our adolescents presented the following SLE classifica-tion criteria:discoidlesion,photosensitivity, arthritis,renal
impairment, hematological changes, and immunological
changes.
Datacollectioninstrument
The toolusedfor datacollection was theFree Association WordsTest(FAWT),designedbyCarlJung(1905)inorderto obtainthepsychologicaldiagnosisonthepersonality struc-tureofindividuals.29In1981,thistestwasadaptedtothefield
ofSocialPsychology byDiGiacomo,becoming widelyused instudiesonSocialRepresentations.Inthesecases,inorder toidentifythelatentdimensionsofrepresentationswithout filteringcensorshipinevocation,bysettinganassociative net-workbetweenaninducingstimulusandevokedcontent.30,31
Thetest isperformedfrom the enunciation ofinducing stimuli, and analyzed subjects must quickly define words associatedwithstimulipresented.FAWTisbasedona con-ceptual repertoire that allowsunifying semantic universes andhighlightinguniversesofcommonwords,inthefaceof inducingstimuliandparticipantsinthestudy.29–33
Applicationmethod
Forabetterdefinitionoftheinducingstimulitobeused,apilot studystagewascarriedout,whereweevaluatedsome stimuli-candidates.Fromthisstage,ourdefinedstimuliwere:chronic disease(stimulus1)andtreatmentofchronicdisease(stimulus2). Withthesestimuli,weconsideredthatitwouldbepossibleto obtainthemeaningsgiventotheexperienceofchronicillness aswellastocare.
Thetestwasadministeredindividuallyinaprivateplace, toavoidinterferenceand ensureprivacy duringoutpatient consultationsinpediatricsandinternalmedicineoutpatient clinic and in the day-care hospital when the adolescents shouldbereceivingintravenousmedication.Theinvestigator, havinginhandpenandpaper,askedthesubjecttoassociate fivewordstoeachoneofthestimulicontainedinthe ques-tions,“WhatcomestoyourmindwhenIsaychronicdisease?”;and then,“WhatcomestoyourmindwhenIsaytreatmentofchronic disease?”.
Statisticalanalysis
Thefiveresponsestoeachstimulusandthe personal char-acteristicsofrespondentsgaverise toa multi-dimensional matrix,whoseexistingassociationscouldgivemeaningtothe feelingsrelatedtochronicillness.
Themostcommonmethodofanalysisusedinthe litera-tureofsocialrepresentationsistheMultipleCorrespondence Analysis (MCA), this being a multivariate technique that makesit possibletodescribetheassociationsfoundinthe dimensionsofafive-dimensionalspaceonatwo-dimensional graphical representation ofthe different existing interrela-tionsbetweenwordsorvariables.Inthiscase,ACMallowed ustoanalyzewhichexpressionsorwordsareassociated,both foradolescentsandcaregivers,aswellasassociationswiththe variables29that,inthisstudy,wereageandlevelofeducation.
Thistechnique,basedonoperations inthe datamatrix, definesproximityandoppositionrelationshipsbetweenthe wordsobtainedforeachstimulus,orwithotheractive vari-ables.Theimportanceofeachwordorvariable,ineachofthe dimensionsorfactors,isdeterminedfromitsweight,called “loadfactor”.TherepresentationintheCartesianaxisofwords andvariablesfromthesefactorloadingsandfromoppositions andvicinitiesallowsasearchforaninterpretationoftheaxes ofeachdimensionrelatedtotheproblem.Withthisanalysis, onecanalsoverifythelevelsofparticipationofthevariables intermsofabsolutecontribution.
StatisticalanalysiswasperformedusingtheFactomineR library,dedicatedtotheExploratoryMultivariateAnalysisof Data34oftheprogramR(freesoftware),atoolwidelyusedin
statistics.
Results
Thewordsevokedbythetestweregroupedtakingintoaccount semanticsimilaritiesandsynonyms(byconsultationofa dic-tionaryofthePortugueselanguage)35inthesingularformof
thenoun,andwiththeverbintheinfinitive.Thewordswould beretainedwhenappearingwithacertainfrequency,29and
inthisstudywordsmentionedthreeormoretimeswere con-sidered.Thiswasdoneforbothgroupsandforeachstimulus, resultinginafinalcompositionoffourwordlists.
Adatabasewasgeneratedforeachgroupandforeach stim-ulus,composedbyage,gender,levelofeducationandthefive evokedresponses.
In the face of the stimulus chronic disease, adolescents evoked147words,ofwhich 92wereretained(14different), whilecaregiversevoked87words,ofwhich57wereretained(9
Stimulus chronic disease
Adolescents
Adolescents
Caregivers
Caregivers Stimulus treatment of chronic disease
LEARNING DIFFICULTYLIMITATIONDISEASE
MEDICATION FAITH
PAIN
OVERCOMINGCARE
JOY
NO CURE SORROW
BAD
IMPOTENCE
NO
NO CURETREATMENT
HOPE
CARE
PAINSORROW
DOESN’T KNOW
STRENGTH KNOWLEDGE
IMPROVEMENT WARMTH
HOPE
STRENGTHCONSULTATION HOPE
DISCIPLINEMEDICATIONHAPPINESS
RESPONSIBILITY IMPROVEMENT
HEALTH
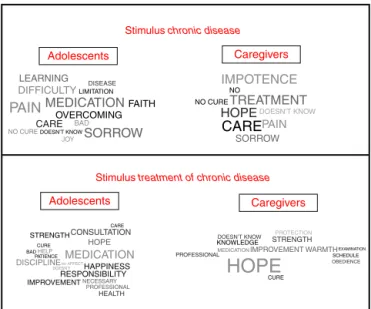
Fig.1–Cloudofwordsinthefacemuli1and2.
Source:http://www.wordle.net/create.
different).Inthefaceofthestimulustreatmentofchronicdisease, adolescentsevoked148words,ofwhich107wereretained(18 different),whilecaregiversevoked94words,ofwhich70were retained(13different).Torepresentthewordfrequency,we usedacloudofwordsproducedbyanapplicationsoftware availableatthesitehttp://www.wordle.net/create.36
Inthecloudofwords,thefontsizeisassociatedwithword frequency. Thelargerthe sizeofthe word,the moreoften thewordwasevokedinassociationwiththestimulus.Inthe clouds,onlythewordsretained(frequencyequalto,orgreater than,threeoccurrences)appear,andthedifferentshadesor colors are emptyofmeaning, servingonlyto facilitatethe visualizationofwordsretained(Fig.1).
Fromthecloudsofwordsproducedbythegroupof adoles-cents,therewasanassociationbetweenthestimuluschronic diseaseandthewords(indescendingorder):sadnessandpain (toagreaterdegree),medication,difficulty,learning,nocure,care, disease, limitation, faith, joy, bad; and some adolescents did notknowhowtonominate.Inthefaceofthestimulus treat-mentofchronicdisease,associationsemergedwiththewords (in descending order): medication and strength (toa greater degree),hope,improvement,consultation,discipline,joy, responsi-bility,health,needed,professional,help,care,cure,theword“no”, patience,bad,andaffection.
Thecloudsofwordsproducedbythegroupofcaregivers illustratedanassociationbetweenthestimuluschronicdisease andthewords(indescendingorder):impotence,treatment,care, pain,hope,sadness,nocure,theword“no”;andsomedidnot knowhowtonominate.Thestimulustreatmentofchronic dis-easeappearedassociatedwiththewords(indescendingorder): hope(highfrequency),care, improvement,strength, medication, knowledge, schedule, professional, cure, examination, obedience, protection(sun);andsomedidnotknowhowtonominate.
2
>12 years
Medication
Limitation
Sorrow Care
Learning
Joy Faith
10-12 years 6-9 years
Bad Disease Doesn’t know
Pain
1
0
Dim 2 (9.47%)
Dim 1 (11.61%) –1
–2
–4 0 2 4 6
Difficulty No cure
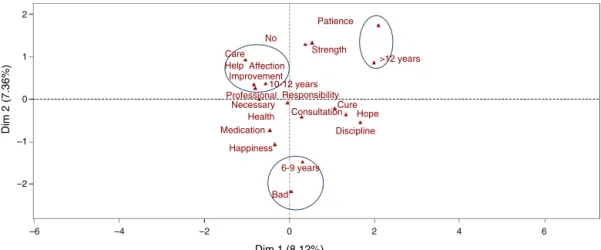
Fig.2–MultipleCorrespondenceAnalysis(MCA)–Adolescentgroup:Stimulus“chronicdisease”.
Source:softwareR.
Inthevisualrepresentationofthisresult,itwaspossibleto perceivethattheadolescentswithhigherlevelsofeducation (above12yearsofstudy) associatedchronicdiseasewiththe wordmedication;thosewithhighschoollevel(10–12yearsof schooling)withthewordsdifficulty,nocure,faith,andjoy;and thosewithelementarylevelII(6–9yearsofstudy)withthe wordsbadanddisease(Fig.2).
IntheanalysisofMCAresultsfromthefirststimulusinthe groupofcaregivers,factors1and3,whichtogetherexplained 27.48%ofthevariancestructureofthedata,wereselected.
Inthevisualrepresentationofthisresult,anassociation betweencertainwords,ageandlevelofeducationwasnoted. Oldercaregiversassociatedchronicdiseasewiththewordcare, whiletheyoungeroneswiththewordtreatment.Astothe asso-ciationsaccordingtothelevelofeducation,itwasobserved thatcaregiverswithhighschoollevel(10–12yearsof school-ing)associatedchronicdiseasewiththewordstreatmentandno cure;thosewithelementaryschoolII(6–9yearsofstudy),tothe word“no”;andthosewithilliteracy/elementaryschoollevelI (0–5yearsofstudy)caregivers,withthewordcare(Fig.3).
In the analysis of MCA results obtained from the sec-ondstimulus,thefactors1and2wereselectedtoreportin bothgroups;thesefactorsexplained15.48%ofthevariability
1.0 No cure
Treatment
10-12 years
22-41 anos
42-61 years
>61 years
Pain
6-9 years
Impotence
No
Sorrow
Care 0-5 years
Doesn’t know >12 years
0.5
0.0
–0.5
–1.0
–1.5
–2.0
–1
–2 0 1
Dim 1 (14.47%)
Dim 3 (13.01%)
2 3 4
Hope
Fig.3–MultipleCorrespondenceAnalysis(MCA)– Caregivergroup:Stimulus“chronicdisease”.
Source:softwareR.
structureofthedataobtainedinthegroupofadolescents,and 20.04%inthegroupofcaregivers.
InthevisualrepresentationoftheresultofMCAobtained fromthesecondstimulusinthegroupofadolescents,a cor-relation was noted between wordsand level ofeducation.
2
1 Care
Help Affection Improvement
Professional Necessary Health Medication
Happiness
6-9 years No
Bad
Cure Consultation Responsibility 10-12 years
Strength Patience
>12 years
Hope
Discipline
0
–1
–2
–2 –4
–6
Dim 1 (8.12%)
Dim 2 (7.36%)
0 2 4 6
Fig.4–MultipleCorrespondenceAnalysis(MCA)–Adolescentgroup:Stimulus“treatmentofchronicdisease”.
>12 years
Warmth
22-41 years
>61 years 42-61 anos
Schedule
10-12 years Hope
6-9 years Profissional Knowledge Obedience Improvement
Doesn’t know 0-5 years
Examination
Strength Protection
Cure
Medication 2
1
0
–1
–1
–2 0
Dim 1 (10.30%)
Dim 2 (9.74%)
1 2
Fig.5–MultipleCorrespondenceAnalysis(MCA)– Caregivergroup:Stimulus“treatmentofchronicdisease”.
Source:softwareR.
Adolescentswithhigherlevelsofeducation(above12years ofstudy)associatedtreatmentofchronicdiseasewiththeword patience; those with high school education (10–12 years of schooling)withthewordsimprovement,help,affectionandcare; andthosewithelementaryschoollevelII(6–9yearsofstudy) withthewordbad(Fig.4).
InthevisualrepresentationoftheresultofMCAobtained
from the second stimulus in the group of caregivers, we
noticedanassociationbetweenwords,ageandlevelof educa-tion.Oldercaregivers(above61years)associatedtreatmentof chronicdiseasewiththewordstrength;thoseaged42–61years, withthe wordsprofessional, knowledgeand improvement;and thoseyoungerones(22–41years),withthewordschedule. Care-giverswithhigherlevelsofeducation(above12yearsofstudy) associatedtreatmentwiththewordcare;thosewithhighschool level(10–12yearsofschooling)withthewordhope;thosewith elementaryschoollevelII(6–9yearsofstudy)withthewords knowledgeandobedience;andthosewithilliteracy/elementary schoollevelI(0–5yearsofstudy)withthewordsmedicationand “Don’tknow”(Fig.5).
Discussion
and
conclusion
Thebirthofachildisalwaysfullofdesires,dreams, expecta-tionsandmeanings–basichallmarksofitssubjectivity,based ontheinitialmother–babybond.37 Althoughtheactualson
nevermatchestheimaginarychildbecausethisisalways ide-alized,thebirthofachildwithadisabilityorillnesscanaffect themother–childrelationship,confirmingthemother’s fan-tasiesinherabilitytobegetornotbegeta“perfectchild”.37–39
Having a child with a chronic health condition causes
changes in family routine and can reflect on family
dynamics13andalsocausesanimpactoneverydaylife.15 A
studyofmaternalrepresentationsaboutthebirthofachild withsevereorganicdiseaseshowsthatthespeechof moth-ersabouttheirchildrenbeginswiththehealthproblemofthe child,asiftheydidnotfindanotherpossibilityof symboliza-tionabouttheirchildthanthedisease.37Forallthesereasons,
webelievethattheinclusionofcaregivers–thoseresponsible forthetreatmentoftheadolescent–inthisstudyisimportant,
andtheknowledgeoftheirperceptionofthediseaseandofthe careoffered,andifthereissimilaritybetweenthemeanings assignedbythetwogroups.
Chronic disease, especially when it occurs in children or adolescents, affects all parties involved(patient, family, professionals)throughmultiplefactors:difficultiesand lim-itations arising from the disease itself, treatment for life, sufferinginthe faceofthesocialstigma,13 the narcissistic
woundstemmingfrom nothavingaperfectchild,40,41
eco-nomicissues(fromthecostoftreatmenttotheeducationand integrationinthelabormarket),42amongothers.
Thepsycho-emotionalaspectisalwayspresentatdifferent levelsandtimes,notjustin“psychosomatic”diseaseswhere theemotionalaspectcomesasatriggeringfactor,butinthe veryconditionofbeingill.AlthoughSLEdisplayanevolution typicallymarked byperiodsofremissionand exacerbation, sufferingtheimpactofseveralfactors,someauthorsidentify theonsetofthediseaseaftersituationsof“stress”and worsen-ingofclinicalactivity,precededbyeverydaystressorsrelated tointerpersonalrelationships.43,44Othersnotetheinfluence
ofemotions and ofthe environment inthe immunity and
physicalconditionofthepatients.45
Sincethe experienceofgettingill dependsonwhat the
person means by disease,18 and given that the meanings
attributed tothe facts are influenced bythe socio-cultural environment,14,16,18wehavetriedtoanalyzethesocial
rep-resentationsofadolescentswithlupusandoftheircaregivers inrelationtochronicillnessandtotreatment,bymeansofan associativenetworkofwords.
Fromthelistsofwordsproduced,weobserved antagonis-ticfeelingsandperceptions,althoughsomeevocationswere similarbetweenthetwogroups.
Theassociations madebytheadolescents inthisstudy, whenfacedwiththetwostimuli,illustratedevocationsofpain and,atthesametime,oftheneedtofight:sadness,difficulty, overcoming,faith,joy,strength,hope,patience–pointingto theimportanceofsupport(family,friends,professionals)in fightingthedisease.Intheirevocations,theadolescents rec-ognizedtheimportanceoftreatmentfortheimprovementof thedisease(medication,consultation,discipline,responsibility, nec-essary,patience),emphasizingthefigureoftheprofessionaland ofcare.
Theassociationsperceivedinthecloudsofwordsevoked bycaregiversshowedthesameantagonism:ontheonehand, wordssuchaspain,impotence,sadness,nocure;andontheother, wordslikehope,care,strength.Thewordsmedication,schedule, knowledge,obedience,andthefigureoftheprofessionalwere alsoevoked,pointingtotheimportanceoftreatment
adher-enceandcommitment.
Words common to both groups emerged, corroborating
the findings of some authors about the influence of the
environment in the process of signification in a disease situation14,16,18: the stimuluschronicdiseaseassociatedwith
thewordscare/treatment,pain,sorrow,limitation/impotence;and the stimulustreatment ofchronicdiseaseassociatedwiththe wordsstrength,medication,improvement.
with the words care (over 61 years), pain and impotence (42–61years),andtreatment(22–41years).Theentailmentof chronicdiseasetocare/treatmentpointstotheperceptionofa situationthatrequiresacontinuousmonitoring.6
Thestimulus chronicdisease treatment was associatedby caregiverswiththewords:strength(over61years);professional, knowledge and improvement (42–61 years); and affection and schedule(22–41years).Thatistosay,thecaregiversnotonly entailedthedisease tocare,but broughtinto this scenario thefigureoftheprofessionalandaffections–affectionand strength.
Itwasobservedthatinthefaceofthetwostimuli, differ-entassociationsemergedfromthelevelofeducationinboth groups,adolescentsassociatedchronicdiseasewiththewords: medication(over12years);difficulty,nocure,faith,andjoy(10–12 years);badanddisease(6–9years),whilecaregiversassociated chronicdiseasewiththewords:treatment,nocure,andtheword “no”(10–12yearsofschooling);andcare(0–5yearsof school-ing).
AlthoughsomestudiesshowthatpatientswithSLEhave asignificantrateindicativeofpsychiatricdisorder (anxiety, irritability, depression),25 the results of our study showed
ambivalentfeelingsandperceptionsofadolescentswithSLE, relativetothestimuluschronicdisease:evocationsexpressing negativeandpositivefeelings, enhancementoftherapeutic possibilities,andexaltationoffaithinthisconfrontation.If, ontheonehand,thesefindingsbroughtapoorprognosisfor thedisease(difficulty-bad-nocure),thefactthatthediseaseis treatable(joy-medication)prevailed.
Caregivers,despiteunderscoringtheimportanceof treat-ment andcare, associatedchronicdiseasetopain, impotence, andnocure, perhapsthankstotheburdenofresponsibility ontheseindividuals,fortheirresponsibilityforthetreatment ofthechild,inadditiontotheconcernaboutthefutureofthe teenagerwhooftenhavehis/herschoollifedisrupteddueto constantcomingsandgoingstothehospital.42
In general, treatment was seen positively (improvement, hope,help),withactiveparticipationofthepatient(knowledge, obedience,schedule,medication).And participantswithhigher levelsofeducationbrought,incommon,thevaluationofthe diseasebeingtreatable,theperceptionoftreatmentoutcome, andfeelingsofhopeandaffectioninthisconfrontation.That is,thelevelofeducationseemstointerferewiththeprocess ofsignification,inpromotingtheexpansionoftheworldview, theperceptionofthelimitsandpossibilities–aresultthat corroboratesthefindingsofotherauthorsaboutthe experi-ences,whichareindividual;butthemeaningsareinfluenced byfamilyandsocioculturalenvironment.14,16–18,46
Theinclusionofthefigureoftheprofessionalsinthe ther-apeutic scene calls for a reflection on the messages they transmitintheconsultations:Howcantheyinterfereby offer-ing,ornotofferingsupport,strength,careandtransmission ofinformation?
Inlinewithsomeauthors,ourstudyshowsthatthe anal-ysisofrepresentationscancontributeto extendthe ability of listening and the interpretation of the statements and demandsofpatients,47byprovidingaccesstothelatent
mean-ingsofchronicillness.Thismethodologynotonlyfavorsthe occurrenceofaqualifiedlistening tothe needsofpatients and caregivers, but brings subsidies to actions that offer
psychological support,in order tohelp the patient’s adap-tation to SLE, reducing his/herpain and worsening of the
disease, improving depression and anxiety, and also the
patient’sself-esteemandqualityoflife.48,49
Somelimitationsofthestudy occurredbylackof socio-demographic characteristics, considering that the patient’s housing location produce interesting social and economic data, and the lackofdataon the administrationand dose ofmedicationsused,whichcouldperhapsinterferewiththe representation of illness by the adolescents, as these are
patients with heterogeneous treatments and with adverse
events,especiallyinchildrenandadolescents.
However,themeaningsthatthepersonusestoexplainthe diseaseprovidepartialandunfinishedpictures,becausethe realityisdynamicandtheexperiencerathercomplex.15
Fur-ther studiesarerequiredtoelucidatevarious issues,tothe extentthatthereisarangeoffactorsthatmayinterferewith theprocessofsignification.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Brasil.HumanizaSUS:PolíticaNacionaldeHumanizac¸ão:a humanizac¸ãocomoeixonorteadordaspráticasdeatenc¸ãoe gestãoemtodasasinstânciasdoSUS.Brasília:Secretaria Executiva,MinistériodaSaúde;2004.
2.SouzaWS,MoreiraMCN.Atemáticadahumanizac¸ãona saúde:algunsapontamentosparadebate.Interface– Comunicac¸ão,Saúde,Educac¸ão.2008;12:327–38. 3.BrehmerLCF,VerdiM.Acolhimentonaatenc¸ãobásica:
reflexõeséticassobreaatenc¸ãoàsaúdedosusuários.Ciência SaúdeColetiva.2010;15:3569–78.
4.AyresJRCM.Cuidadoehumanizac¸ãodaspráticasdesaúde. In:DeslandesSF,editor.Humanizac¸ãodoscuidadosem saúde:conceitos,dilemasepráticas.RiodeJaneiro:Fiocruz; 2006.p.49–83.
5.FrancoTB,BuenoW,MerhyEE.Oacolhimentoeosprocessos detrabalhoemsaúde:ocasodeBetim,MinasGerais,Brasil. CadSaudePubl.1999;15:345–53.
6.CanesquiAM.Olharessocioantropológicossobreos adoecidoscrônicos.SãoPaulo:Hucitec/Fapesp;2007. 7.KleinmamA.Theillnessnarratives:suffering,healingand
thehumancondition.NewYork:BasicBooksInc.;1988. 8.BuryM.Illnessnarrative:factorfiction?SociolHealthIlln.
2001;23:263–85.
9.MinayoMCS,AssisSG,SouzaER,NjaineK,DeslandesSF,Silva CMFP,etal.Falagalera:juventude,violênciaecidadaniana cidadedoRiodeJaneiro.RiodeJaneiro:Garamond;1999. 10.MoscovicS.Arepresentac¸ãosocialdapsicanálise.Riode
Janeiro:Zahar;1978.
11.JodeletD.Representac¸õessociais:umdomínioemexpansão. In:JodeletD,editor.Asrepresentac¸õessociais.RiodeJaneiro: Eduerj;2001.p.17–44.
12.BergerP,LuckmannT.Aconstruc¸ãosocialdarealidade: tratadodesociologiadoconhecimento.Petrópolis:Vozes; 2006.
14.AtkinsonS.Anthropologyinresearchonthequalityofhealth services.CadSaúdePúbl.1993;9:283–99.
15.LiraGV,NationsMK,CatribAMF.Cronicidadeecuidadosem saúde:oqueaantropologiadasaúdetemnosensinar?Texto ContextoEnferm.2004;13:147–55.
16.EstevamID,CoutinhoMPL,AraújoLF.Osdesafiosdaprática socioeducativadeprivac¸ãodeliberdadeemadolescentesem conflitocomalei:ressocializac¸ãoouexclusãosocial?Rev PsicoPortoAlegre.2009;40:64–72.
17.OliveiraFA.Antropologianosservic¸osdesaúde: integralidade,culturaecomunicac¸ão.Interface–Comun, Saúde,Educ.2002;6:63–74.
18.GomesR,Mendonc¸aEA.Arepresentac¸ãoeaexperiênciada doenc¸a:princípiosparaapesquisaqualitativaemsaúde.In: MinayoMCS,DeslandesSF,editors.Caminhosdo
pensamento:epistemologiaemétodo.RiodeJaneiro:Fiocruz; 2008.p.109–32.
19.SatoEL,BonfáED,CostallatLTL,SilvaNA,BrenolJCT, SantiagoMB,etal.Consensobrasileiroparaotratamentodo lúpuseritematososistêmico.RevBrasReumatol.2002;42: 362–70.
20.AyacheDCG,CostaIP.Alterac¸õesdapersonalidadenolúpus eritematososistêmico.RevBrasReumatol.2005;45:313–8. 21.AppenzellerS,CostallatLTL.Comprometimentoprimáriodo
sistemanervosocentralnolúpuseritematososistêmico.Rev BrasReumatol.2003;43:20–5.
22.BorbaEF,LatorreLC,BrenolJCT,KayserC,SilvaNA, ZimmermannAF,etal.Consensodelúpuseritematoso sistêmico.RevBrasReumatol.2008;48:196–207.
23.FreireEAM,SoutoLM,CiconelliRM.Medidasdeavaliac¸ãoem lúpuseritematososistêmico.RevBrasReumatol.
2011;51:70–80.
24.MiguelFilhoEC[TesedeDoutorado]Alterac¸ões
psicopatológicasnoLúpusEritematosoSistêmico.SãoPaulo: UniversidadedeSãoPaulo;1992.
25.MeloLF,Da-SilvaSL.Análiseneuropsicológicadedistúrbios cognitivosempacientescomfibromialgia,artritereumatoide elúpuseritematososistêmico.RevBrasReumatol.
2012;52:175–88.
26.TanEM,CohenAS,FriesJF,MasiAT,McShaneDJ,RothfieldNF, etal.The1982revisedcriteriafortheclassificationof systemiclupuserythemathosus.ArthritisRheum. 1982;25:1271–7.
27.HochbergMC.UpdatingtheAmericanCollegeof Rheumatologyrevisedcriteriafortheclassificationof systemiclupuserythemathosus.ArthritisRheum. 1997;40:1725.
28.CostallatLTL,AppenzellerS,BértoloMB.Lúpus
neuropsiquiátricodeacordocomanovanomenclaturae definic¸ãodecasosdocolégioAmericanodeReumatologia (ACR):análisede527pacientes.RevBrasReumatol. 2001;41:133–41.
29.GuerreiroMR,CuradoMA.Picar...fazdoer!Representac¸ões
dedornacrianc¸a,emidadeescolar,submetidaapunc¸ão venosa.RevEnfermeiraGlobalEnero.2012;25:75–91. 30.NóbregaSM,CoutinhoMPL.Otestedeassociac¸ãolivrede
palavras.In:CoutinhoMPL,editor.Representac¸õessociais: abordageminterdisciplinar.JoãoPessoa:UniversitáriaUFPB; 2003.p.67–77.
31.DeRosaAS.Aredeassociativa:umatécnicaparacaptara estrutura,osconteúdoseosíndicesdepolaridade, neutralidadeeestereotipiadoscampossemânticos relacionadoscomasrepresentac¸õessociais.In:MoreiraASP, JesuinoBVCJC,NóbregaSM,editors.Perspectivas
teórico-metodológicasemrepresentac¸õessociais.João Pessoa:UniversitáriaUFPB;2005.p.61–128.
32.CoutinhoMPL.Depressãoinfantil:umaabordagem psicossocial.JoãoPessoa:UniversitáriaUFPB;2005. 33.BotêlhoSM,BoeryRNSO,VilelaABA,SantosWS,PintoLS,
RibeiroVM,etal.Ocuidarmaternodiantedofilhoprematuro: umestudodasrepresentac¸õessociais.RevEscEnfermUSP. 2012;46:929–34.
34.LêS,JosseJ,HussonF.FactoMineR:anRpackagefor multivariateanalysis.JStatSoftw.2008;25:1–18.
35.DicionárioEditoradaLínguaPortuguesa.Colec¸ãoDicionários Editora,PortoEditora,Edic¸ão2014,ISBN978-972-0-01866-3. 36.NuvensdePalavras.Availablein:
http://www.wordle.net/create.
37.BattikhaEC,FariaMCC,KopelmanBI.Asrepresentac¸ões maternasacercadobebêquenascecomdoenc¸asorgânicas graves.Psicol:TeoriaePesquisa.2007;23:17–24.
38.Cullere-CrespinG.Aclínicaprecoce:onascimentodo humano.SãoPaulo:CasadoPsicólogo;2004.
39.BeliniAEG,FernandesFDM.Olharecontatoocular:
desenvolvimentotípicoecomparac¸ãonaSíndromedeDown. RevSocBrasFonoaudiol.2008;13:52–9.
40.FreudS.Sobreonarcisismo:umaintroduc¸ão.Edic¸ãoStandard BrasileiradasObrasPsicológicasCompletasdeSigmund Freud,xiv.RiodeJaneiro:Imago;1976.p.103–8.
41.MartinsBSO.Ocorpo-sujeitonasrepresentac¸õesculturaisda cegueira.RevPsicol.2009;21:5–22.
42.ResendeOLC[Dissertac¸ãodeMestrado]Omédicoeadíade comdoenc¸aoculargrave.RiodeJaneiro:Fundac¸ãoOswaldo Cruz;2010.
43.PetriM.Systemiclupuserythematosus:clinicalaspects.In: KoopmanWJ,editor.Arthritisandalliedconditions:a textbookofRheumatology,26,14thed.LippincottWilliams; 2000.p.377–88.
44.NeryFG,BorbaEF,NetoFL.Influênciadoestressepsicossocial nolúpuseritematososistêmico.RevBrasReumatol.
2004;44:355–61.
45.SolomonGF,MoosRH.Emotions,immunity,anddisease;a speculativetheoreticalintegration.ArchGenPsychiatry. 1964;11:657–74.
46.GeertzC.Ainterpretac¸ãodasculturas.RiodeJaneiro:Livros TécnicoseCientíficosEditora;1989.
47.FavoretoCAO,CabralCC.Narrativassobreoprocesso saúde-doenc¸a:experiênciasemgruposoperativosde educac¸ãoemsaúde.Interface–Comunicac¸ão,Saúde, Educac¸ão.2009;13:7–18.
48.CalSF,BorgesAP,SantiagoMB.Prevalênciaeclassificac¸ãoda depressãoempacientescomlúpuseritematososistêmico atendidosemumservic¸odereferênciadacidadedeSalvador. JLIRNNE.2006;2:36–42.
49.CalSFLM.RevisãodaLiteraturasobreaeficáciada