w w w . r b o . o r g . b r
Case
Report
Nodular
fasciitis
in
finger
simulating
soft
tissue
malignancy
夽,夽夽
Soraya
Silveira
Monteiro,
Diva
Helena
Ribeiro,
Tatiane
Cantarelli
Rodrigues
∗,
Gerson
Ferreira
Gontijo
Junior,
Kylza
Arruda,
Eloy
De
Avila
Fernandes
HospitaldoServidorPúblicoEstadual,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4February2013
Accepted9April2013
Keywords:
Fasciitis/radiography
Computedtomography
Magneticresonancespectroscopy
Softtissueneoplasms
a
b
s
t
r
a
c
t
Nodularfasciitis(NF)isararefibroblasticproliferativelesion,characterizedclinicallyasa
solitarymassofhardenedandslightlypainfulonpalpation,fastgrowingandnogender
preference.TheobjectiveofthisstudyistoreportthecaseofapatientwithNFinthird
fingeroflefthand,describethefindingsofplainradiography,computedtomographyand
magneticresonanceimagingandcorrelatewiththeliterature.SincethediagnosisofNFis
achallenge,beingnecessarytoconciliatetheclinical,radiologicalandpathological.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
Fasciíte
nodular
em
quirodáctilo
que
simula
neoplasia
maligna
de
partes
moles
Palavras-chave:
Fasciíte/radiografia
Tomografiacomputadorizada
Espectroscopiaderessonância
magnética
Neoplasiasdetecidosmoles
r
e
s
u
m
o
Fasciítenodular(FN)éumalesãoproliferativafibroblásticarara,caracterizadaclinicamente
comoumamassasolitáriadeconsistênciaendurecida,poucodolorosaàpalpac¸ão,de
cresci-mentorápidoesempredilec¸ãoporsexo.Oobjetivodestetrabalhoérelatarocasodeuma
pacientecomFNnoterceiroquirodáctilodamãoesquerda,descreverosachadosda
radio-grafiasimples,tomografiacomputadorizadaeressonânciamagnéticaecorrelacionarcom
aliteratura.VistoqueodiagnósticodeFNéumdesafio,énecessárioconciliarosachados
clínicos,radiológicosepatológicos.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora
Ltda.Todososdireitosreservados.
夽
Pleasecitethisarticleas:MonteiroSS,RibeiroDH,RodriguesTC,JuniorFGK,ArrudaG,FernandesEDeA.Fasciítenodularem
quirodác-tiloquesimulaneoplasiamalignadepartesmoles.RevBrasOrtop.2014;49:89–93.
夽夽
StudyconductedatHospitaldoServidorPúblicoEstadual,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](T.C.Rodrigues).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Nodularfasciitis(NF)isabenignsofttissueinjuryofunknown
etiology,1–4 characterizedby proliferation offibroblastsand
often confused histologically with sarcomas, because of
its rapid growth, high cellularity and increased mitotic
activity.1,3,4
Thelesionsarecommonlysolitary,occurinadultsbetween
20and40yearsold,1–4andaffectanyregionofthebody.1,5
Thisisaself-limitingdisease.2,3 Patients usuallyhave a
history of rapid growth and nodulation, and may develop
numbnessorparesthesia.1–3,6
Its diagnosis is challenging and can be confused with
malignanttumors,becauseoftheaggressiveclinical
behav-iorassociatedwithimagingandhistologyfindings.1–3Multiple
lesionsarerare,1,7aswellaslesionsinhandsandfeet,andvery
rareinthefingers.8
Giventhisfact,wereportacaseofFNonthefinger,since
theknowledgeoftheappearanceoftheimagingstudiescan
avoidaggressiveinvasiveprocedures,sincethe histological
studywithoutimagemayleadtosuspicionofalesionwith
highaggressiveness.
Case
report
Patient, female, 45 yearsold, teacher,referringappearance
ofnodulationofrapidgrowthinthethirdleftfingerfortwo
years;painless,butwithlocaldiscomfort.Shedeniedtrauma
orprevioussurgery.Thephysicalexaminationshowedvolar
nodulationintheproximalphalanxofthethirdchirodactyl,
adheredtotheskinwithoutretractionorphlogisticsigns,and
measuringapproximately2cm.
Plainradiography(RX)revealedossificationofsofttissues
of the radial and flexor diaphyseal faces of the proximal
phalanx of the finger, with irregular and partially defined
contours, cortical erosion and lamellar periosteal reaction
proximalanddistaltothenodule,andincreasedvolumeand
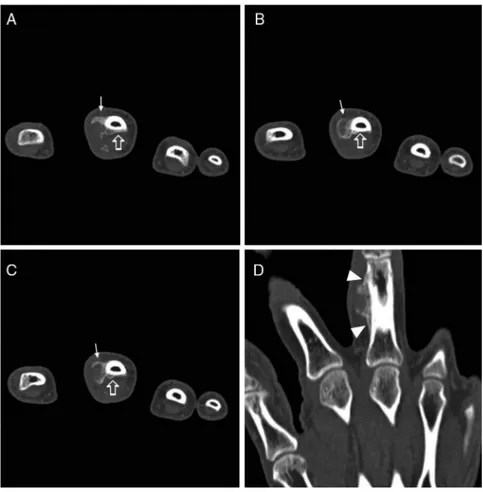
densityofpartsoftheadjacentsofttissue(Fig.1).Computed
moreclearlythe ossification,extendingfrom the boneand
externally involvingthe corticalflexorcontiguous withthe
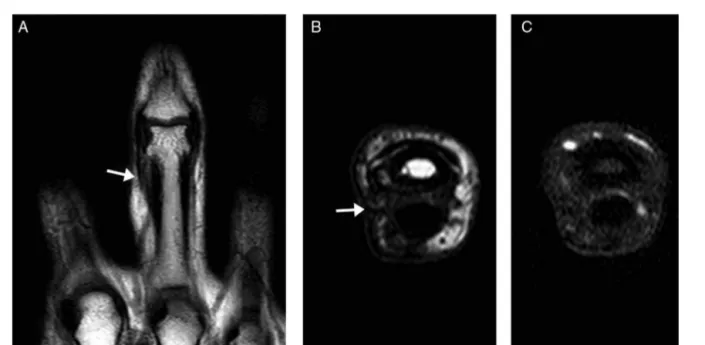
radial and flexor aspect nodulation (Fig. 2). MRI revealed
expansive formationon softparts oftheradialface ofthe
proximalphalanx,whichpromotedslightthinningofthe
cor-tical bone with intimate contact, and superiorly displaced
the extensor hood.Thelesion depictedthe iso/hypersignal
relative to muscle on T1, heterogeneous signal with mild
hypersignalon T2,andsignificant heterogeneous
enhance-ment toparamagnetic contrastmedium, associatedwitha
bonemarrowedemapattern(Fig.3).
The patient underwent surgical exeresis, and the
histopathological examination revealed fibrous
connec-tive tissue with neoformation and trabeculation, favoring
the diagnosis of NF. Five months later, MRI depicted only
fibrocicatricial changes in soft tissues, without significant
enhancementinthecontrastmedium(Fig.4).
Discussion
FNisabenignlesionofunknownetiology,1,5 butwith
possi-ble associationwithtrauma.1,3,7FNaffectseverybody part,
and mostcommonly1,5 the upperextremity (48%), besides
the trunk(20%),headand neck(17%),and lower extremity
(15%).1,2Itsoccurrenceisrareinhandsandfeet,andveryrare
infingers.8
Themostaffectedagegroupis20–40years;FNalsoaffects
bothgenders.1,3 Symptomssuchasnumbness,paraesthesia
and pain are infrequent,implying nervous compression.2,3
Multiplelesionsarerare.1,7Theaveragediameterofthelesion
isabout2cm,andlargerlesionsareexceptional.1,3,7
Basedontheanatomicallocation,FNcanbedividedinto
threetypes: subcutaneous,intramuscular,and fascial.
Sub-cutaneous FN is three to10 times more frequent.1,2,4 The
intramuscular typemoreperfectlysimulatesaneoplasmof
soft tissues.1 Intravascular and intradermal formsare rare
subtypes.2
Fig.2–AxialsliceCTscanrevealstheossification(arrows)advancingfromtheboneandthatexternallyinvolvedthe corticalflexor(openarrows)contiguoustotheradialandflexoraspectnodulation.Thereconstructioninthecoronalplane (D)depictscontinuityofnodularlesionwithperiostealreaction(arrowheads)extendingtotheflexorside.
Accordingtothepredominanthistologiccomposition,FN
canbefibrous,myxoidorcellular.1,3,4Histologically,thislesion
consistsoffibroblasts arrangedinshortbundlesand
fasci-clesscattered withina myxoid stroma, and may simulate
sarcoma.1,2,8Someauthorsbelievethattheamountandtype
ofextracellularmatrixreflecttheageofthelesion:inearly
FN,predominatesthemyxoidcomponent;inmatureFN,the
fibrouscomponentismoreabundant.1,2,4Thevarious
compo-nentscancoexistinthesame lesion,withcombinationsof
myxoid-cellular,andofcellular-fibroustypes,thataremore
commonthancombinationsofmyxoid-fibroustypes,
suggest-inghistologicaltransitionfrommyxoidtocellularand,later,
tofibroustype.1
ImagingstudiesmaybeusedtoevaluatepatientswithFN.
Thepresent studyshowssomeoftheimagechangestobe
characterizedandrecognized.RXshowsincreasedsofttissue.
Toourknowledge,thereisonlyonecaseintheliteraturethat
depictstheradiographicappearanceofthelesion,considering
itasnonspecific.8
OnCT,lesionsofFNusuallyappearasasuperficialmassof
softtissue,withdensitysimilartootherlesions,1well-defined,
andthatcaninvadeanddestroyadjacentbone.7
At MRI, the appearance is nonspecific,1,2,7,8 most
com-monlyiso/hyperintenseonT1andhyperintenseonT2,with
variedenhancementbyparamagneticcontrastbecauseofthe
differenthistologicaltypes.3,4Itisunknownwhichinfluences
moredecisivelyinsignalintensity:thecellularityorcollagen.
Someauthorsadvocatethatmyxoidformspresent
hyperin-tensivityrelativetomuscleonT1,andtosubcutaneousfaton
T2;andthatfibrousformsarehypointensetothemuscleinall
sequences.Otherauthorsstatethatthelesionisisointenseto
muscleonT1,andtovenousstructuresonT2.1The
hypercel-lularlesionspresentisointensesignaltomuscleonT1,and
arehyperintensetofatonT2.4
Because of the nonspecific findings, many differential
diagnoses can be proposed, including neuroma,
neurofi-broma,sarcoidosis,aggressivefibromatosis,dermatofibroma,
fibrosarcoma,andmalignantfibroushistiocytoma.2,3,7Inthe
intramuscularlesions,onecanthinkofmyositisossificansin
earlystage.4 Giantcelltumorsofthetendonsheathcanbe
differentiatedfromFNbyitsslowgrowthandbythefixation
ofthetumortothetendon.8Insomecases,thesimilarityin
clinical and microscopicpresentationbetweenFN and
sar-coma makesdifficulttheestablishmentofadiagnosis,but
some clinicaland radiological features makethediagnosis
ofNFlesslikely,includinglesionsinpatientsover 70years
old,lesionslocatedinthehandsandfeet,orsimultaneous,
multiple,recurrentlesions,withperilesionaltissueedemaor
intralesionaldepositionofhemosiderininMRIstudies.2
Thephysicianmustobtainabiopsytoestablishadefinitive
diagnosis.2,8 Theexcision,usuallycurative,isthemainstay
oftreatment,5 althoughintralesionalinfusionof
corticoste-roidshasbeensuggestedbysomeauthors.2,6 Theremaybe
Fig.3–MRIrevealsexpansiveformationonsoftpartsoftheradialfaceoftheproximalphalanxwithiso/hypersignal relativetomuscleonT1(AandC),mildhypersignalonT2(B),andsignificantheterogeneousenhancementtoparamagnetic contrastmedium(D);slightthinningofthecorticalbone(arrows),whichsuperiorlydisplacestheextensorhood
(arrowheads),associatedwithbonemarrowedemapattern.
of patients and being usually observed immediately after
excision.2,8
Insummary,FNcanbeinterpretedasamalignantlesion
becauseofitsrapidgrowthandaggressivehistologicalnature.
However,the correctdiagnosis can beestablishedby
com-bining the characteristics of the image, localization and
histology.1
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WangXL,DeSchepperAM,VanhoenackerF,DeRaeveH, GielenJ,AparisiF,etal.Nodularfasciitis:correlationofMRI findingsandhistopathology.SkeletalRadiol.2002;31(3):155–61.
2.LeungLY,ShuSJ,ChanAC,ChanMK,ChanCH.Nodular fasciitis:MRIappearanceandliteraturereview.SkeletalRadiol. 2002;31(1):9–13.
3.DuncanSFM,AthanasianEA,AntonescuCR,RobertsCC. Resolutionofnodularfasciitisintheupperarm.Radiology CaseReports[Online].2006;1:3.
4.DinauerPA,BrixeyCJ,MoncurJT,Fanburg-SmithJC,Murphey MD.PathologicandMRimagingfeaturesofbenignfibrous soft-tissuetumorsinadults.Radiographics.2007;27(1): 173–87.
5.SouzaLS,AlmeidaWL,CostaALD,SilvaOS,SouzaLL.Fasceíte nodular.RevBrasCirCabPesc.2009;38:274–5.
6.GrahamBS,BarrettTL,GoltzRW.Nodularfasciitis:responseto intralesionalcorticosteroids.JAmAcadDermatol.
1999;40(3):490–2.
7.KimST,KimHJ,ParkSW,BaekCH,ByunHS,KimYM.Nodular fasciitisintheheadandneck:CTandMRimagingfindings. AJNRAmJNeuroradiol.2005;26(10):2617–23.
8.ParkJS,ParkHB,LeeJS,NaJB.Nodularfasciitiswithcortical erosionofthehand.ClinOrthopSurg.2012;4(1):