Women on Maternal and Child Health in Rural Sierra
Leone: A Cross-Sectional Survey
Joseph Sam Kanu, Yuan Tang, Yawen Liu*
Department of Epidemiology & Biostatistics, School of Public Health, Jilin University, Changchun City, Jilin Province, P. R. China
Abstract
Background:Globally, Sierra Leone is ranked among the countries with the worst maternal and child health indicators. The mortality of women and children is significantly higher compared with other developing countries. The death of women and children can be prevented by simple cost-effective community-based interventions. The aim of this present study was to learn the knowledge levels of women on maternal and child health, and treatment-seeking and preventive behaviours in rural Sierra Leone and provide appropriate suggestions for policy makers. Moreover, the study also aimed to evaluate the effect of a husband’s involvement on health knowledge and practices of women in rural Sierra Leone.
Methods:Women with at least a child of five years or below were interviewed in their households through a structured questionnaire. Characteristics of the households and of the respondents were collected and the number of correct answers given to the health knowledge and practice questions and their percentage distributions were tabulated and an overall health knowledge score was calculated.
Results:The mean score of the derived overall health-related knowledge was 61.6% (maximum of 91% and a minimum of 18%) with a standard deviation of 14.7% and a median of 63.3%. Multivariable regression analyses showed education and number of pregnancies are associated with knowledge score, with significantly improved health knowledge scores amongst those who accessed higher education. There were some inappropriate practices in hygiene and sanitation. However, vaccination coverage was high with almost 100% coverage for BCG.
Conclusions:Based on the findings of this study, women’s knowledge on maternal and child health care are inadequate in rural Sierra Leone. Health promotion activities focusing on prevention of diarrhoea, malaria and pneumonia, improvement in health-related knowledge on pregnancy, delivery, neonatal care and environmental sanitation would be invaluable.
Citation:Kanu JS, Tang Y, Liu Y (2014) Assessment on the Knowledge and Reported Practices of Women on Maternal and Child Health in Rural Sierra Leone: A
Cross-Sectional Survey. PLoS ONE 9(8): e105936. doi:10.1371/journal one.0105936
Editor:Andrew Vallely, University of New South Wales, Australia
ReceivedMarch 17, 2013;AcceptedJuly 30, 2014;PublishedAugust 28, 2014
Copyright:ß2014 Kanu et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding:This study was supported by grants from the National Natural Science Foundation of China (30870952) and Science and Technology Department of
Jilin Province (200905185, 20080735). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests:The authors have declared that no competing interests exist.
* Email: [email protected]
Introduction
The death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes i.e., maternal mortality (WHO Statistics) [1]– has been a priority area for the global health and development community at least since the Nairobi Safe Motherhood Confer-ence in 1987 [2]. Neonatal mortality, infant mortality, and child mortality in general are still at unacceptably high levels despite the efforts invested in decreasing these mortalities in sub Saharan Africa and Southern Asia [3]. Deaths of children under the ages of five years are increasingly concentrated in these areas [3].
Sierra Leone has one of the highest child and maternal mortality rates in the world, and despite recent progress, it is not on track to reach the 2015 MDGs for MDG 4 (reducing child mortality rates) and MDG 5 (improving maternal health) unless
rapid acceleration takes place [4]. The mortality rate of under-five children remains at 140 deaths per 1,000 live births and of infants at 89 deaths per 1,000 live births [5]. The maternal mortality is at 857 maternal deaths for every 100,000 live births in Sierra Leone [5].
out safe child delivery, particularly when there are complications. Infection is likely to develop after an abortion or childbirth and is a major cause of death. Sepsis that is not related to unsafe abortion accounts for up to 15% of maternal deaths in developing countries. The majority of unsafe abortions take place in developing countries [5,9–12]. After pregnancy-related causes of death, sexually transmitted infections are the second most important causes of healthy life lost in women [13]. Many sexually transmitted infections affect the outcome of pregnancy and some are passed to unborn and newborn babies [13–16]. Preterm birth is the leading cause of neonatal mortality in both developed and developing countries, accounting for an estimated 24% of neonatal deaths [9,17–20].
Pneumonia is the leading cause of death in children under five years old, killing about 1.6 million children annually and accounting for 18% of all deaths of children worldwide [21–23]. Diarrhoeal disease is the second leading cause of death and a leading cause of malnutrition in children under five years old, killing more than 1.3 million children every year [24,25]. Every 45 seconds a child dies of malaria in Africa. In 2008, there were 247 million cases of malaria and nearly one million deaths – mostly children in Africa [26]. Other infections such as neonatal sepsis are also well documented as causes of death in neonates and infants [21,27–29]. An estimated 164 000 people died from measles in 2008 – mostly children under the age of five [30].
Available knowledge and tools are effective in reducing maternal and newborn suffering and death [31]. Experience has shown these interventions are affordable and can be effectively delivered even in the poorest countries [31]. However, only when these available knowledge and tools are accessible, will they help the suffering people [31–33]. Health promotion programmes worldwide have long been premised on the idea that providing knowledge about causes of ill health and choices available will go a long way towards promoting a change in an individual’s behaviour towards more beneficial health seeking behaviour. The way in which women reach the decisions they take can have a profound effect on child morbidity and mortality and is therefore worthy of continued study [34].
In public health today, there are consistent and powerful findings revealing the strong association between mothers’ education and child mortality [35–38]. The causal link between health outcomes and education is reported in many surveys [41– 44]. Every one year increment in education level is associated with a 7–9% reduction in mortality of children less than 5 years old [39]. The mortality rate of children whose mothers have above 7-year schooling is 58% lower than those whose mothers have no education [40]. Other studies also share this finding; with a causal link been established between a range of health outcomes and education [41–44].
Accessibility to health interventions, especially among the poorest people in the world requires the improvement of poor-organized health systems,–typically characterised by insufficient numbers of health workers, poorly functioning supply chains, and low-quality care [45]. The common barriers to health services and interventions in the poorest settings include lack of financial support, unhealthy lifestyle, and cultural background [45]. These limitations result in poor delivery of health promotion messages to women during antenatal visits, vaccination and treatment of their children. In Sierra Leone, the introduction of the free health care initiative (FHCI) makes it possible for more women and children have easier access to health care. With the limited number of health workers, the heavy workload results in health workers having little time for counseling and passing on health promotion messages that are mainly delivered at the time of clinic visits.
Although the high maternal and child mortality rates in Sierra Leone are well documented in the international literature, far less is known about women’s knowledge of maternal and child health in this setting.
The main aim of this study was to assess the knowledge and practices of women on maternal and child health in rural Sierra Leone. The study also sought to identify impact factor(s) of knowledge and practices and investigate the effect of the husbands’ involvement on maternal and child health. Direct observations were recorded on households and suggestion and advices on health improvement were given.
Methodology Ethics statement
This study was approved by the Institutional Review Board of School of Public Health, Jilin University and by the Ministry of Health and Sanitation in Sierra Leone. Signed informed consents were obtained from all participants before the interviews.
Study location and participants
The study was carried out in a rural area of Sierra Leone. Five villages (clusters) in the Bombali district of northern Sierra Leone were selected randomly from the list of towns/villages in the province. From each village, households with at least a woman with a child under five years old were identified. For households having more than one woman that met the inclusion criteria, only one woman was selected by simple random sampling and interviewed. As a result, a total of 244 mothers in 244 different households were selected and interviewed.
Inclusion criteria
1. All mothers of 5-year-old children and below were included in the study.
2. All women who have given birth in the past 5 years, regardless of whether the child was still alive or not were included in the study.
Exclusion criteria
1. Women of childbearing age who do not fulfill the inclusion criteria above were excluded from the study.
2. Women who were pregnant at the time of the study but had not given birth before and those without at least a child five years or younger, were not included in the study.
Data collection
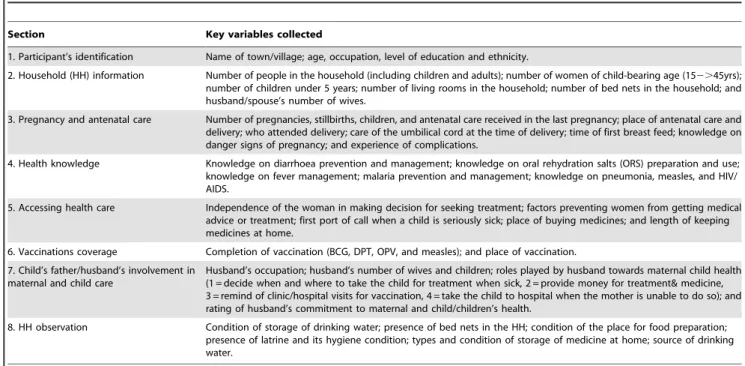
The questionnaire was organized into eight sections: partici-pant’s identification, household information, pregnancy and antenatal care, health knowledge, treatment-seeking behaviour, vaccination status, involvement of husband in maternal and child care, and household observation (key variables collected in each section are presented in Table 1). Interviews were done in local languages (krio, limba, and temne) at the participants’ homes. It was mandatory that interviews occur at home as direct observa-tions on the participants’ dwelling places were part of the research. Interviews were done by five personnel who were well trained on the use of the questionnaire before data collection. Sections one to seven were completed by each participant whilst section eight was done by interviewer making direct observation (inspection of the household sanitary condition using checklist included in the questionnaire - see key variables collected under section 8 in Table 1). In total, 22 questions were included in deriving the heath knowledge scores with each question contributing a maximum of only one point. Questions with more than one correct answer were weighed by dividing the number of correct answers given by the total number of correct answers. The questionnaire was tested in one other village (which was excluded in the main study) and amendments made before the questionnaire was used in the main study. Responses were collected, organized and analyzed.
Analysis of Data
The data was collected on forms (questionnaires), and all forms were screened, cross-checked and package for further processing and safe keeping. The collected information was first double entered into the Epidata 3.1 data base using necessary checks (to prevent entering of values outside the range of a particular question), and was then exported to other statistical softwares (Excel & SPSS), screened again before analyses done. Both Excel and SPSS were used for data analyses. This process was managed by the first and second authors of this manuscript.
Households and demographic characteristics of the respondents were tabulated and analyzed. Descriptive statistics for continuous
variables such as mean, standard deviation, median, and range and for categorical variables the numbers and percentages were calculated. The number of correct answers given to the health knowledge questions and their percentage distribution were tabulated by items. An overall health knowledge score for each participant was derived by summing the total number of correct responses given to the health knowledge questions in the questionnaire. Using the derived health knowledge score as dependent variable, factors affecting health knowledge scores were investigated using simple and multiple linear regression analyses models.
Results
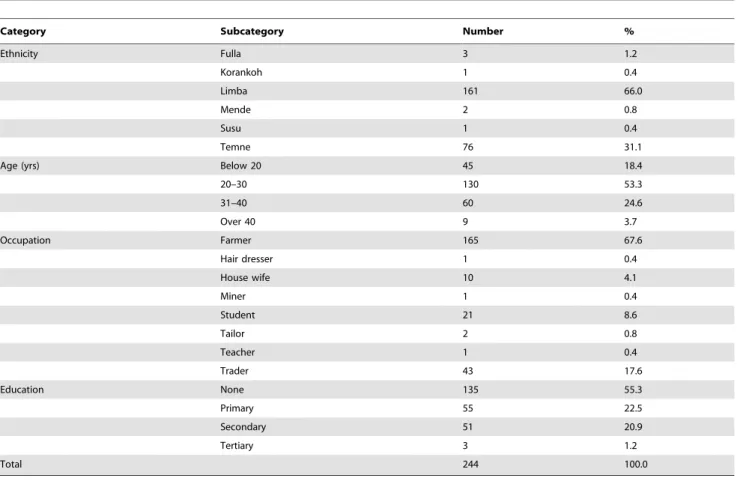
Participants’ demographic characteristics are presented in Table 2. Out of the 244 participants interviewed, 32 (13.1%) were from Gbankan town, 70 (28.7%) were from Kabombeh town, 28 (11.5%) were from Robureh, 59 (24.2%) were from Katherie, and 55 (22.5%) were from Robuya town. Respondents were mainly farmers 165 (67.6%) and traders 43 (17.6%) with 21 (8.6%) being students at the time of the interview. More than half of the interviewed women 135 (55.3%) had never attended school and thus no form of formal education; with only 3 (1.2%) attaining tertiary education.
Table 3 and 4 give summary of the household characteristics. The average number of people per household was 9 with a minimum of 3, maximum of 25 people and a standard deviation of 4.6. On average, there were 2 females of childbearing age and a similar average of children under five years of age. The average number of living rooms in each household was 2. An average of 4 people shared a living room with an average of 2.2 bed nets in each household. Most of these bed nets 165 (67.6%) never required retreatment as they were long-lasting insecticide-treated bed nets. Direct observations made in the households by the interviewers revealed that 215 (88.1%) of the households had bed nets in the place where the youngest child sleeps. Nearly all of the observed households 230 (94.3%) had no form of well defined
Table 1.Key Variables collected in each section.
Section Key variables collected
1. Participant’s identification Name of town/village; age, occupation, level of education and ethnicity.
2. Household (HH) information Number of people in the household (including children and adults); number of women of child-bearing age (152.45yrs); number of children under 5 years; number of living rooms in the household; number of bed nets in the household; and husband/spouse’s number of wives.
3. Pregnancy and antenatal care Number of pregnancies, stillbirths, children, and antenatal care received in the last pregnancy; place of antenatal care and delivery; who attended delivery; care of the umbilical cord at the time of delivery; time of first breast feed; knowledge on danger signs of pregnancy; and experience of complications.
4. Health knowledge Knowledge on diarrhoea prevention and management; knowledge on oral rehydration salts (ORS) preparation and use; knowledge on fever management; malaria prevention and management; knowledge on pneumonia, measles, and HIV/ AIDS.
5. Accessing health care Independence of the woman in making decision for seeking treatment; factors preventing women from getting medical advice or treatment; first port of call when a child is seriously sick; place of buying medicines; and length of keeping medicines at home.
6. Vaccinations coverage Completion of vaccination (BCG, DPT, OPV, and measles); and place of vaccination.
7. Child’s father/husband’s involvement in maternal and child care
Husband’s occupation; husband’s number of wives and children; roles played by husband towards maternal child health (1 = decide when and where to take the child for treatment when sick, 2 = provide money for treatment& medicine, 3 = remind of clinic/hospital visits for vaccination, 4 = take the child to hospital when the mother is unable to do so); and rating of husband’s commitment to maternal and child/children’s health.
8. HH observation Condition of storage of drinking water; presence of bed nets in the HH; condition of the place for food preparation; presence of latrine and its hygiene condition; types and condition of storage of medicine at home; source of drinking water.
place for hand washing; and of the 14 (5.7%) with place for hand washing, only one household had soap for hand washing. Only 15 (6.1%) of the observed households were without latrine facilities. In more than half of the households, that is, 141 (57.8%), the main source of drinking water is from tap water, 63 (25.8%) from open wells and 40 (16.4%) from hand operated wells.
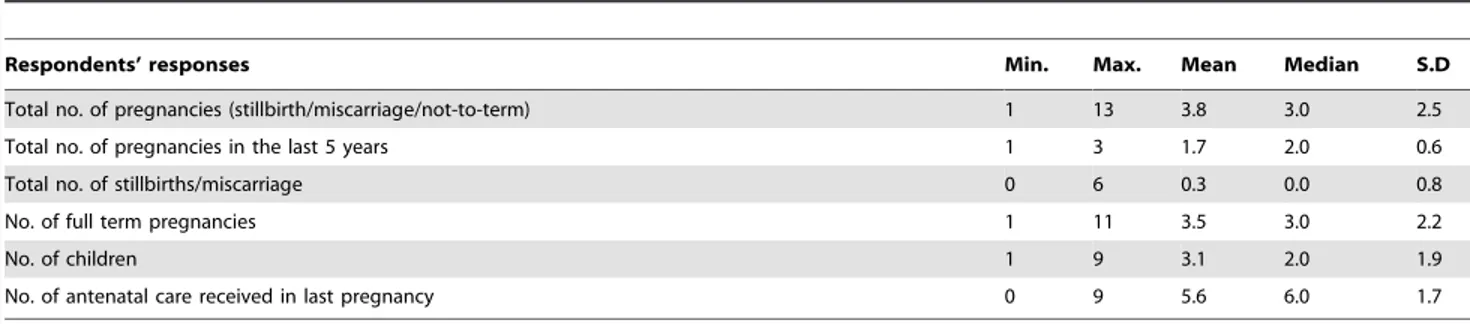
Tables 5 and 6 summarize the respondents’ pregnancies and antenatal care practices. High birth rates were recorded in most of the participants with an average of 3.8 total pregnancies, a mean of 1.7 pregnancies in the last five years, and an average of 0.3 stillbirths. Participants had an average of 3 children at the time of
the study. Respondents reported an average of 5.8 antenatal care (ANC) visits with most women attending health clinics 231 (94.7%) in their last pregnancies. Most participants 155 (63.5%) could not identify any danger sign that necessitates compulsory institutional (clinic or hospital) deliveries. Non-institutional deliveries were reported by 80 (32.8%) at home and 50 (20.5%) at TBAs’ places, with only 114 (46.8%) deliveries occurring in heath institutions [101 (41.4%) in clinics and 13 (5.3%) in hospitals]. In 42.2% of participants, deliveries were attended by TBAs, 40.6% attended by nurse/midwife, only 7.4% attended by medical doctors and 8.2% attended by relatives and friends. Excluding TBAs as formal skilled
Table 2.Participants’ characteristics (demographics).
Category Subcategory Number %
Ethnicity Fulla 3 1.2
Korankoh 1 0.4
Limba 161 66.0
Mende 2 0.8
Susu 1 0.4
Temne 76 31.1
Age (yrs) Below 20 45 18.4
20–30 130 53.3
31–40 60 24.6
Over 40 9 3.7
Occupation Farmer 165 67.6
Hair dresser 1 0.4
House wife 10 4.1
Miner 1 0.4
Student 21 8.6
Tailor 2 0.8
Teacher 1 0.4
Trader 43 17.6
Education None 135 55.3
Primary 55 22.5
Secondary 51 20.9
Tertiary 3 1.2
Total 244 100.0
doi:10.1371/journal one.0105936.t002
Table 3.Household Information (Responses of Interviewee).
Responses of Interviewee Min. Max. Mean Median S.D
No. of people in HH* 3 25 9.1 8.00 4.6
No. of females of child-bearing age** 1 7 2.0 2.00 1.1
No. of children under 5 yrs 1 7 2.4 2.00 1.3
No. of living rooms in HH 1 9 2.4 2.00 1.3
No. of people per room 2 11 4.4 4.00 1.6
No. of bed nets in the HH*** 0 6 2.2 2.00 1.2
*HH- Household.
**Child-Bearing age = 15 to 45 years of age.
***Out of the 244 participants, 5 (2.0%) responded that the bed nets did not need impregnation at the time of the study, 2 (0.8%) responded that the bed nets were treated within the last six months, 165 (67.6%) said the nets were never treated, 61 (25.0%) didn’t know whether the nets were treated or not; whilst 11 (4.5%) had no bed nets..
health personnel, in this study, only 48.0% of respondents had supervised delivery by skilled health personnel in their last pregnancy [medical doctors 18 (7.4%) and nurse/midwives 99 (40.6)]. Razor blade 138 (56.6%) and scissors 52 (21.3%) were reported to be used for cutting the umbilical cord in the last pregnancies. Immediate breast feeding 162 (66.4%) was reported for the last live delivered babies. Most respondents 173 (70.9%) gave the correct answer that at the age of six months a child can be given other food in addition to breast milk.
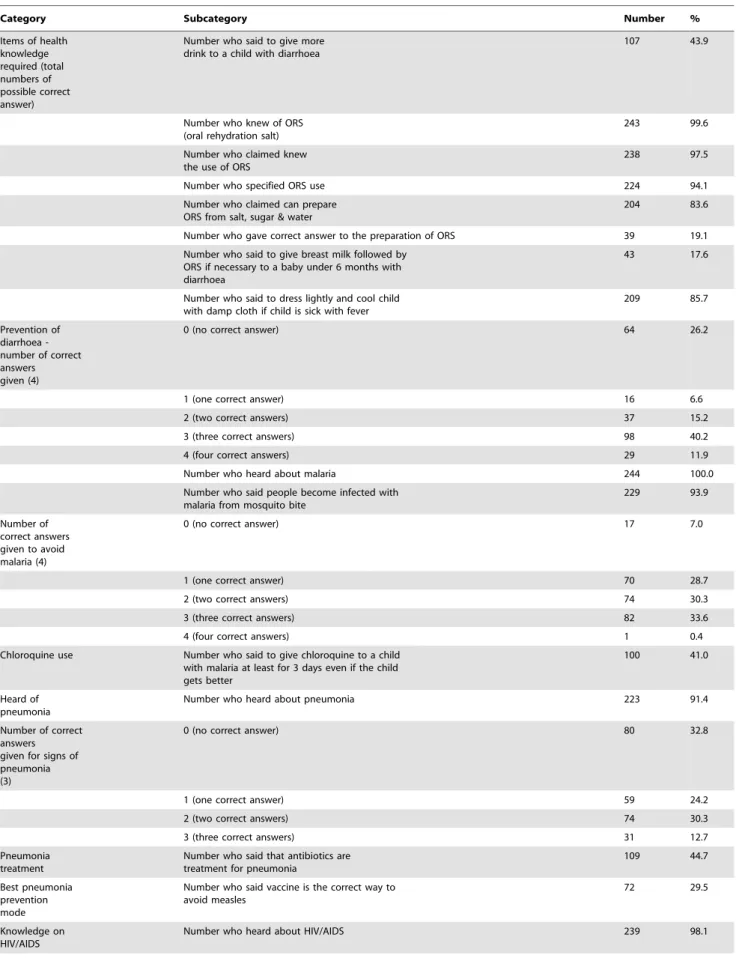
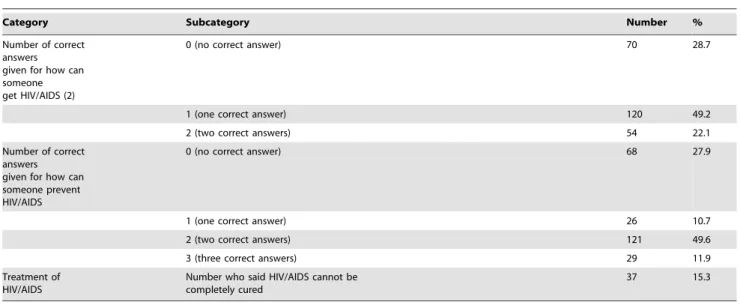
Responses to health knowledge are presented in Table 7. Only 107 (43.9%) of participants knew that a child with diarrhoea needs to be given more fluids to drink than usual. Although almost all respondents 243 (99.6%) knew ORS (oral rehydration salt), only 39 (19.1%) correctly explained how to prepare ORS solution from sugar, salt and water when the readymade ORS is not available. Sixty-four (26.2%) of the total respondents could not give any correct answer on the ways to prevent diarrhoea and only 29 (11.9%) were able to give all four correct answers on the prevention of diarrhoea included in the questionnaire. Only 43 (17.6%) respondents knew that a baby under 6 months with diarrhoea need to be given breast milk followed by ORS if
necessary; which revealed that the overall knowledge of the respondents on the management of diarrhoea was poor. The respondents’ knowledge on fever management in children was sufficient with 209 (85.7%) knowing that a child with fever needs to be dressed lightly and cooled with damp cloth. Knowledge on malaria was poor. Although 244 (100%) of respondents had heard of malaria and 229 (93.9%) stated that people became infected with malaria from mosquito bite; only 1 (0.4%) could give all four preventive means for malaria and 17 (7.0%) could not give any preventive method for malaria. Only 100 (41.0%) of respondents knew that chloroquine should be given to a child with malaria for at least 3 days even if the child gets better. Two hundred and twenty-three - 223 (91.4%) of respondents heard of pneumonia, but up to 80 (32.8%) could not give any correct sign of pneumonia, whilst only 31 (12.7%) gave all the three signs of pneumonia as included in the questionnaire. Similarly, 109 (44.7%) knew that antibiotics are used for treatment of pneumonia. Only 72 (29.5%) knew that the best way to prevent measles was by vaccination. Assessment of the participants’ knowledge on HIV/AIDS revealed that 239 (98.1%) heard of HIV/AIDS but only 29 (11.9%) knew
Table 4.Household information (interviewer’s direct observation).
Category Subcategory Number %
Bed nets at youngest child’s sleeping place Yes 215 88.1
No 29 11.9
Water storage facility Clean 176 72.1
Covered 202 82.8
Dedicated ladle or cup to remove water that is not used to drink from directly 3 1.2
Ladle or cup to remove water that is use to drink from directly 169 69.3
others 17 7.0
Have a place for hand washing Yes 14 5.7
No 230 94.3
Soap present in hand washing facility? Yes 1 7.1
No 13 92.9
Clean latrine Yes 80 32.8
No 164 67.2
Latrine covered with lid Yes 109 44.7
No 135 55.3
Latrine with water for cleaning Yes 4 1.6
No 240 98.4
Latrine with brush for cleaning Yes 4 1.6
No 240 98.4
Latrine with place for hand washing close by Yes 167 68.4
No 77 31.6
Latrine condition not applicable (no latrine) Yes 15 6.1
No 229 93.9
Medicine at home Good storage of medicine at home 74 30.3
Fair storage of medicine at home 4 1.6
Poor storage of medicine at home 48 19.7
No medicine at home 118 48.4
Main Source of drinking water Tap water 141 57.8
Open well water 63 25.8
Hand operated well water 40 16.4
all the three major ways of preventing HIV infection; and only 37 (15.3%) knew that HIV/AIDS cannot be completely cured.
The derived overall health knowledge revealed a mean score of 61.6% (maximum of 91% and a minimum of 18%) with a standard deviation of 14.7% and a median of 63.3%.
A Simple linear regression analyses (Tables 8 and 9) revealed people with higher levels of education achieved substantially higher scores (p,0.05) with a 2.7% increase in score with each unit increase in educational level. This was also true in the multiple regression models. Total number of pregnancy was also found to significantly influence health knowledge score (p = 0.021) but this was not statistically significant in the multiple regression models when the total number of children each participant had were included at the same time using step wise. Of statistical
significance in the multiple regression model using stepwise were educational level and total number of pregnancies, and the formula was: {yscore= 54.3+3.8xeducation+1.2xno. of pregnancy}; with both education and total number of pregnancies having p-values less than 0.05. Also investigated was the linear regression relationship between the husband’s roles scores and health knowledge score of the respondents but this was not statistically significant in both the simple and multiple regression models.
Accessing health care and treatment seeking behaviours of participants are summarized in Table 10. In this study 81.0% of the respondents reported they can make independent decision for a child’s treatment when seriously ill. Still considered as big problems by women in this study were getting money for needed treatment 49 (87.3%), distance to health facility 155 (63.5%),
Table 5.Pregnancy and antenatal care (continuous variables).
Respondents’ responses Min. Max. Mean Median S.D
Total no. of pregnancies (stillbirth/miscarriage/not-to-term) 1 13 3.8 3.0 2.5
Total no. of pregnancies in the last 5 years 1 3 1.7 2.0 0.6
Total no. of stillbirths/miscarriage 0 6 0.3 0.0 0.8
No. of full term pregnancies 1 11 3.5 3.0 2.2
No. of children 1 9 3.1 2.0 1.9
No. of antenatal care received in last pregnancy 0 9 5.6 6.0 1.7
doi:10.1371/journal one.0105936.t005
Table 6.Pregnancy and antenatal care (categorical variables).
Category Subcategory Number %
Place of antenatal care Clinic 231 94.7
Hospital 11 4.5
No. antennal care visits 2 0.8
Place of delivery At home 80 32.8
TBA’s place 50 20.5
Clinic 101 41.4
Hospital 13 5.3
Who attended the delivery TBA 103 42.2
Nurse/midwife 99 40.6
Doctor 18 7.4
Relatives/friends 20 8.2
No one (self delivered) 4 1.6
Umbilical cord cutting instrument Razor blade 138 56.6
Scissor 52 21.3
Others/don’t know 54 22.1
Sterilized instrument for cord cutting Yes 149 61.1
Don’t know 95 38.9
How long before first breast feeding Immediately 162 66.4
Hours 59 24.2
Days 22 9.0
Others 1 0.4
Give child other food at age 6 months Correct answers 173 70.9
Wrong answers 71 29.1
Danger pregnancy signs Can’t identify any danger sign 155 63.5
Table 7.Health knowledge*.
Category Subcategory Number %
Items of health knowledge required (total numbers of possible correct answer)
Number who said to give more drink to a child with diarrhoea
107 43.9
Number who knew of ORS (oral rehydration salt)
243 99.6
Number who claimed knew the use of ORS
238 97.5
Number who specified ORS use 224 94.1
Number who claimed can prepare ORS from salt, sugar & water
204 83.6
Number who gave correct answer to the preparation of ORS 39 19.1
Number who said to give breast milk followed by ORS if necessary to a baby under 6 months with diarrhoea
43 17.6
Number who said to dress lightly and cool child with damp cloth if child is sick with fever
209 85.7
Prevention of diarrhoea -number of correct answers given (4)
0 (no correct answer) 64 26.2
1 (one correct answer) 16 6.6
2 (two correct answers) 37 15.2
3 (three correct answers) 98 40.2
4 (four correct answers) 29 11.9
Number who heard about malaria 244 100.0
Number who said people become infected with malaria from mosquito bite
229 93.9
Number of correct answers given to avoid malaria (4)
0 (no correct answer) 17 7.0
1 (one correct answer) 70 28.7
2 (two correct answers) 74 30.3
3 (three correct answers) 82 33.6
4 (four correct answers) 1 0.4
Chloroquine use Number who said to give chloroquine to a child with malaria at least for 3 days even if the child gets better
100 41.0
Heard of pneumonia
Number who heard about pneumonia 223 91.4
Number of correct answers given for signs of pneumonia (3)
0 (no correct answer) 80 32.8
1 (one correct answer) 59 24.2
2 (two correct answers) 74 30.3
3 (three correct answers) 31 12.7
Pneumonia treatment
Number who said that antibiotics are treatment for pneumonia
109 44.7
Best pneumonia prevention mode
Number who said vaccine is the correct way to avoid measles
72 29.5
Knowledge on HIV/AIDS
taking transport 151 (61.9%), only a male health provider present at the health facility 87 (35.7%), absence of care provider at the clinic or the clinic closed at the time of health need 138 (56.6%), the clinic unable to cure the patient 226 (92.6%), and the clinic not having the appropriate medicines 237 (97.1%). Almost half of the respondents 121 (49.6%) reported that when a child is seriously ill, their first port of call for help is their relatives, 40 (16.4%) clinic, 62 (25.4%) hospital, and up to 5 (2.0%) seek help first from traditional healers. Places of buying medicines vary greatly among respon-dents with 113 (46.3%) buying medicines from local clinics or hospitals, 73 (29.9%) from local persons, and 53 (21.7%) from pharmacies or drug stores; and respondents taking on average 46.9 minutes to reach these places of buying medicines.
Vaccination coverage was summarized in Table 11. One hundred and ninety-nine - 199 (81.6%) of the interviewed women presented the vaccination cards for their youngest child that was alive whilst 45 (18.4%) could not; and 234 (95.9%) of these vaccinations occurred in regional clinics, 5 (2.0%) in hospitals and 5 (2.0%) in non-governmental organization (NGO) clinics. Vaccination coverage was high for the first vaccine BCG and decreased as we moved from the first to the last (measles) vaccination.
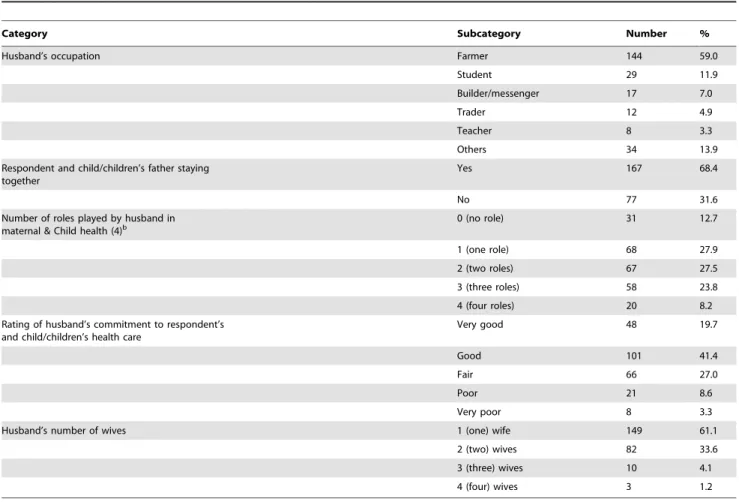
Table 12 summarizes the husband’s characteristics and role in maternal and child health care. Seventy-seven - 77 (31.6%) of the husbands were not staying with the participants at the time of the study. Four major roles expected to be played by husbands towards maternal and child health were included in the questionnaire. These roles include: decide when and where to take the child for treatment when sick, provide money for treatment and medicine, remind partner of clinic/hospital visits for vaccination, and take the child to hospital when partner is unable to do so. Of these, 31 (12.7%) of husbands played no role, 68 (27.9%) played only one role, 67 (27.5%) two roles, 23.8% three roles and only 20 (8.2%) contributed all the four roles investigated. On average each husband had 4 children (Minimum 1, maximum 20); 149 (61.1%) had only one wife, 82 (33.6%) had two wives, 10 (4.1%) had three wives whilst 3 (1.2%) had four wives. Only 48 (19.7%) of the respondents rated their husbands’ commitment to their health and their children’s health care as very good, and 8 (3.3%) as very poor.
Discussions
The sample in the study were mainly limba 161 (66.0%) and temne 76 (31.1%). Although the combined age groups 20–30 and
Table 7.Cont.
Category Subcategory Number %
Number of correct answers given for how can someone get HIV/AIDS (2)
0 (no correct answer) 70 28.7
1 (one correct answer) 120 49.2
2 (two correct answers) 54 22.1
Number of correct answers given for how can someone prevent HIV/AIDS
0 (no correct answer) 68 27.9
1 (one correct answer) 26 10.7
2 (two correct answers) 121 49.6
3 (three correct answers) 29 11.9
Treatment of HIV/AIDS
Number who said HIV/AIDS cannot be completely cured
37 15.3
*Health Knowledge score calculated from the various health knowledge questions with each question contributing a maximum of one point. Expressed in percentages, the results gave a minimum of 18%, maximum of 91%, with mean of 61.6, median 63.3 and standard deviation 14.7.
doi:10.1371/journal one.0105936.t007
Table 8.Results of Linear regressions for health knowledge score (univariable model).
Variable (unit) Change in scorea 95%CL P-value
Age (years) 0.6 21.9 3.0 0.653
Husband’s scoreb 4.7 21.7 11.1 0.148
Total no. of pregnancy 0.9 0.1 1.6 0.023
No. of children 1.2 0.3 2.2 0.013
Education 2.7 0.5 4.9 0.015
aChange in the average health knowledge score for a unit increase in the continuous variables or being in a category versus the baseline category for categorical variables.
31–40 years of age formed the largest proportions of respondents 210 (77.9%), as much as 45 (18.4%) of the mothers interviewed were below the age of 20 years. Our finding that nearly 20% mothers were under 20 years old was in accordance with the UNFPA consultancy report on the determinants and consequences of teenage pregnancy and motherhood in Sierra Leone [47]. Most of the respondents were poor subsistence farmers 165 (67.6%), lacking formal education and 135 (55.3%) of them never attended school, putting them at disadvantage for health and other social amenities in society.
According to our study, there were on average 9 people living together per household. Within this household there was an average of 2.4 living spaces/rooms where people reside and 4.4 people sharing each room/living space. This overcrowding phenomena results in a diminished quality of life due to increased physical contact, lack of sleep, lack of privacy, poor hygiene practices and an inability to care adequately for sick household members [48]. Up to 29 (11.9%) of respondents lack bed nets in the places where the youngest child sleeps. Overall sanitary conditions were poor with 230 (94.3%) households lacking place for hand washing. These poor sanitary conditions are thus associated with outbreaks and spread of cholera and other infectious diseases.
Based on a study conducted by researchers from John Hopkins University, the interval of three to five years for childbirth is important for the health of both mother and child [49]. The most powerful impact factor for child survival is birth spacing [50]. However, according to our study, there was an average of four children in one household and 2 children were under five, which suggested that the birth interval was less than three years and resulted in poor health of mothers and child survival. It was estimated that birth control could avoid 100,000 mothers’ death and death of one out of every five babies [51]. Sixty-three and half percent of the respondents could not identify any sign that indicates hospital/clinic delivery, and 32.8% of respondents admitted home deliveries. However, high numbers of antenatal care were received by respondents in their last pregnancies and 66.4% admitted immediate breastfeeding after delivery.
In rural settings, many factors can influence a woman’s access to health care facilities and treatment seeking behaviours. Despite the free healthcare initiative introduced for pregnant, lactating mothers and children under five years by the government of Sierra Leone in April 2010 (excluding women from the explicit costs for consultations, medicines and other hospital charges), there are still implicit costs or constrains that act as barriers to healthcare access. Lacking of financial support and distance to health facilities were still barriers to prompt and early treatment. Inability of healthcare facilities to provide the appropriate care and medicines and these institutions being closed at some times of need were reported as big problems by respondents in this study. Treatment seeking behaviour was also found to be inappropriate with 121 (49.6%) of respondents first contacting relatives for treatment when a child is seriously ill compared to only 40 (16.4%)
who immediately take the child to the clinic; and 73 (29.9%) buy medicines from local persons (who are usually with substandard drugs and lacking knowledge of their use).
In contrast to the 2008 demographic and health Survey [4], vaccination coverage was reported in this study to be 100% coverage for BCG. However, consistent with similar studies [36,46], vaccination coverage decreased as we moved down from the first vaccination BCG to the last, i.e., measles.
The health knowledge of women on maternal and child health varies widely as investigated in this study with calculated minimum score as low as 18% and as high as 91% (mean 61.6%, median 63.3% and standard deviation of 14.7). In accordance with other studies, our study showed that health knowledge scores improve significantly amongst those who have education [36,41– 44,46,52,53], especially secondary school (high school) and higher. It was also found in our study that the overall health score was higher among women who were multiparous irrespective of their level of education. This might be due to repeated health education messages during antenatal visits in several pregnancies or frequently sick children. Although this present study indicates that the respondents’ certain health knowledge improved compared to the findings of the Sierra Leone demographic and health Survey 2008 [4], however, the respondents’ knowledge on certain health parameters still remain unsatisfactory. For instance, knowledge on ORS and its use was found to be adequate with 243 (99.6%) respondents knowing ORS and 224 (94.1%) able to specify its use but only 39 (19.1%) were able to correctly explain the life saving procedure of preparing ORS from sugar, salt and water when the readymade ORS is unavailable. Knowledge on diarrhoea and its management was low with only 43.9% knowing that a child with diarrhoea need to be given more fluid; only 17.6% knew that breast milk followed by ORS if necessary is the management of choice for a child under six months old with diarrhoea; and only 11.9% of respondents were able to identify all the four preventive methods of diarrhoea included in the questionnaire. Similar findings were also found for malaria, pneumonia and HIV/AIDS with respondents admitting hearing of these conditions but lacking appropriate knowledge on their preventions and managements. Knowledge on the danger signs of pregnancy was low (not included in the Tables).
One of the aims of this study was to find out the relationship between the respondents’ health knowledge and the husband’s commitment to maternal and child health care. Fifty-nine percent of the respondents’ husbands were farmers, 11.9% were students. 31.6% of participants were not staying with their husbands, which resulted in child health care within the mother alone. Each participant’s husband had an average of 4.4 children; 38.9% of the participants’ husbands had two or more wives; only 19.7% of the participants rated their husbands’ commitment to maternal and child care as very good and only 1.2% of the interviewed women said their husbands performed all the four roles included in the questionnaire. These summaries indicated that men’s involvement in maternal and child care were not satisfactory.
Table 9.Results of Linear regressions for health knowledge score (multivariable model).
Variable (unit) Change in scorea 95%CL P-value
Total no. of pregnancy 1.2 0.5 2.0 0.001
Education 3.8 1.6 6.0 0.001
aChange in the average health knowledge score for a unit increase in the continuous variables or being in a category versus the baseline category for categorical variables.
This study has some limitations. In the first place, the findings of this cross sectional study on health knowledge levels, household information, treatment seeking and preventive behaviours and other results are only representative of areas selected in the Bombali district rather than the entire population of Sierra Leone. Second, the findings could be biased due to the fact that one of the clusters/villages had a regional clinic (Kabombeh), thus giving its representative participants relative advantage in terms of distance
to healthcare, source of medicines and health promotion information. This made inter-cluster analyses of health knowledge less informative. Thirdly, as a direct consequence of the selected area, higher numbers of Limbas (66.0%) and Temnes (31.1%) were included in this study with little or none of the other tribes of Sierra Leone.
Despite the limitations highlighted above, the method employed in this study has some useful implications and provide information
Table 10.Accessing health care and treatment seeking behaviourq.
Category Subcategory Number %
Woman making decision for child’s treatment when seriously ill
Yes 200 82.0
No 25 10.2
Depends 19 7.8
Number who said it is a big problem to the following questionnaire items:
Knowing where to go- a big problem
14 5.7
Getting permission to go- a big problem
49 20.1
Getting money for needed treatment-a big problem
213 87.3
Distance to health facility- a big problem
155 63.5
Taking transport- a big problem 151 61.9
Going alone- a big problem 42 17.2
There may only be a male health provider- a big problem
87 35.7
There may not be anyone at the clinic or clinic closed- a big problem
138 56.6
The clinic will not be able to cure you-A big problem
226 92.6
The clinic will not have appropriate medicines- a big problem
237 97.1
Person from whom help is sought if child is seriously ill
Another parent 6 2.5
Relative 121 49.6
Traditional healer 5 2.0
Matrona 2 0.8
Clinic 40 16.4
Hospital 62 25.4
Others 8 3.3
If you need medicines for your children, where do you normally go to buy them?
Local person (‘‘peppeh doctor’’) 73 29.9
Relative 1 0.4
Pharmacy/drug store 53 21.7
Local clinic/hospital 113 46.3
Patent medicine shop 1 0.4
Others 3 1.2
How long do you normally keep medicine at home?
Can’t exactly tell 145 59.4
Just one month 89 36.5
More than one year 2 0.8
Others 8 3.3
qSummary of the approximate time to source of medicine (Minutes) revealed a minimum and maximum of 1 and 165 minutes respectively; with mean 46.9, median
that could complement previous similar studies and future studies in this respect. Very few health knowledge, attitude and behaviour studies bring together the range of issues covered in the present study. Most studies conducted on mothers or women of reproductive age were done on single themes such as knowledge and practices on breastfeeding [54,55], prevention and treatment or management of diarrhea [56,57], pneumonia [58,59], and malaria [60,61], and as well as on knowledge and practice surrounding antenatal care and delivery [62,63]. Of the studies mentioned above, many were conducted at the healthcare delivery point (facility level) and/or in urban settings and very few studies attempted to assess women’s health knowledge, direct household observation and the contributions of husbands to maternal and child healthcare and investigate other practices on a range of issues related to child health at the household level in rural settings. Exceptions are publications in Ghana which examined community effects such as the proportion of literate adults and the presence of a market on health knowledge in Ghana [64] and a study in Guinea that assessed the knowledge and reported practices of men and women on maternal and child health in rural Guinea Bissau [46]. As integrated approaches to the reduction of child mortality at the community level become more widespread, it becomes critical to develop tools that can capture a range of knowledge and practice of women and men at the household level in rural settings in order to plan appropriate and effective interventions [46]. In addition, unlike other studies on health knowledge in rural settings that exclusively report descriptive statistics (numbers and percent-ages) or simple scoring system which increases by one for each answer that is correct [65,66], this study reported a weighted knowledge score derived by the inverse of the possible correct responses given by each respondent. Hence the authors of this study believe this method could be a useful tool in similar studies involving health knowledge in rural settings.
Conclusions
Empowering communities with appropriate health knowledge is an appropriate and cost effective means of achieving the Millennium Development Goals especially the health-related ones (MDGs 4, 5 & 6). However, prior to formulating health promotion programmes, it is vital to assess the health knowledge of the community using specially designed surveys. Similar assessment is of immense importance in monitoring progress in already implemented programmes. Reports of this study revealed low levels of appropriate health knowledge on some of the major factors responsible for child mortality such as pneumonia, diarrhoea and malaria; as well as on breastfeeding and risk signs that dictate institutional delivery during pregnancy. It also found that the majority of births occurred at home mostly attended by Traditional Birth Attendants (TBAs) and that poor practices existed in relation to the care of the umbilical cord and immediate breastfeeding. Household sanitation and hygiene practices were found to be poor and that money for treatment and transportation still pose barriers to effective treatment seeking in rural settings. Therefore, health education activities that target these areas of knowledge and practice should be an integral part of an intervention package to improve maternal and child survival in rural Sierra Leone. However, high levels of vaccination coverage were found in this study.
Acknowledgments
The authors would like to thank Dr. S.A.S. Kargbo, Director of Reproductive and Child Health, and other staff of the Ministry of Health & Sanitation; Dr. Kennedy Ongwae, MCH Specialist, UNICEF Sierra
Leone, Pharm. Walton Beckley and other staff of UNICEF Sierra Leone; Mr. Saffea Gborie of the Information Desk, WHO Sierra Leone and staff of the Reproductive Health Division WHO Sierra Leone; and staff of the School of Midwifery; and Mr. Lamin Kanu and Mr. Abu Kanu, for their immense contributions during data collection in Sierra Leone. Thanks also to Ms Zhihui Yan, staff and students of the department of epidemiology and biostatistics; lecturers and students of the biostatistics department,
school of public health, Jilin University, China for their contributions in the analyses of this work.
Author Contributions
Conceived and designed the experiments: JSK YL. Performed the experiments: JSK. Analyzed the data: JSK YT YL. Contributed reagents/materials/analysis tools: YL. Wrote the paper: JSK YL.
References
1. WHO (2014) Health statistics and health information system. http://www.who. int/healthinfo/statistics/indmaternalmortality/en/. Accessed February 19, 2014. 22: 30.
2. Kenneth H, Kevin T, Carla A, Neff W, Lale S, et al. (2007) Estimates of maternal mortality worldwide between 1990 and 2005: an assessment of available data. Vol 370 (1311–1319).
3. UNICEF WHO, World Bank, UN population division (2012) Levels and trends in child mortality (estimates developed by the UN inter-agency group for child mortality).
4. Government of Sierra Leone (2011) Reproductive, newborn and child health policy. July 2011.
5. Statistics Sierra Leone (SSL) and ICF Macro (2008) Sierra Leone demographic and health survey.
6. WHO Geneva (2009) Guidelines for the management of postpartum haemorrhage and retained placenta.
7. WHO Geneva (2007) Recommendations for the prevention of postpartum haemorrhage.
8. Khan KS, Wojdyla D, Say L, Gu¨lmezoglu AM, Van Look PFA (2006) WHO analysis of causes of maternal death: a systematic review. Lancet: 367: 1066– 1074.
9. WHO Geneva (2007) Managing complications in pregnancy and childbirth: a guide for midwives and doctors. (Integrated management of pregnancy and childbirth).
10. Duley L (1992) Maternal mortality associated with hypertensive disorders of pregnancy in Africa, Asia, Latin America and the Caribbean. British journal of obstetrics and gynaecology: 99: 547–553.
11. Kulier R, Gu¨lmezoglu AM, Hofmeyr GJ, Cheng LN, Campana A (2007) Medical methods for first trimester abortion. Cochrane database of systematic r e v i e w s , I s s u e 4 . A r t . N o : C D 0 0 2 8 5 5 . D O I : 1 0 . 1 0 0 2 / 14651858.CD002855.pub3.
12. WHO Geneva (2007) Unsafe abortion. Global and regional estimates of incidence of unsafe abortion and associated mortality in 2003. Fifth edition. 13. Glasier A, Gu¨lmezoglu AM, Schmid GP, Moreno CG, Van look PF (2006)
Sexual and reproductive health: a matter of life and death. Lancet: 367: 1595– 607.
14. WHO Geneva (2007) Global strategy for the prevention and control of sexually transmitted infections: 2006–2015: breaking the chain of transmission. 15. WHO Geneva (2003) Guidelines for the management of sexually transmitted
infections.
Table 12.Summary of husband’s characteristics and role in maternal and child health carea.
Category Subcategory Number %
Husband’s occupation Farmer 144 59.0
Student 29 11.9
Builder/messenger 17 7.0
Trader 12 4.9
Teacher 8 3.3
Others 34 13.9
Respondent and child/children’s father staying together
Yes 167 68.4
No 77 31.6
Number of roles played by husband in maternal & Child health (4)b
0 (no role) 31 12.7
1 (one role) 68 27.9
2 (two roles) 67 27.5
3 (three roles) 58 23.8
4 (four roles) 20 8.2
Rating of husband’s commitment to respondent’s and child/children’s health care
Very good 48 19.7
Good 101 41.4
Fair 66 27.0
Poor 21 8.6
Very poor 8 3.3
Husband’s number of wives 1 (one) wife 149 61.1
2 (two) wives 82 33.6
3 (three) wives 10 4.1
4 (four) wives 3 1.2
aSummary of the husbands’ number of children revealed a minimum and maximum of 1 and 20 children respectively; with mean 4.4, median 4.0, and standard deviation 3.9.
bThere are four (4) main roles included in the questionnaire: Decide when and where to take the child for treatment when sick; provide money for treatment and medicine; remind partner of clinic/hospital visits for vaccination; and take the child to hospital when partner is unable to do so.
16. Delport SD, Pattinson RC (2000) Congenital and perinatal infections: prevention, diagnosis and treatment. Syphilis: prevention, diagnosis and management during pregnancy and infancy. In: Newell M-L, McIntyre J. Eds. Cambridge, UK, Cambridge University Press: 258–275.
17. King JF, Flenady VJ, Papatsonis DNM, Dekker GA, Carbonne B (2004) Calcium channel blockers for inhibiting preterm labour (Cochrane Review). The Cochrane Library, Issue 2. Chichester: JohnWiley & Sons.
18. Martin JA, Hamilton BE, Ventura SJ, Menacker F, Park MM, et al (2002) Births: final data for 2001. National Statistics Report: 51(2): 1–104. 19. Abu-Rashid N, Al-Jirf S, Bashour H (2012) Causes of death among Syrian
children using verbal autopsy. World Health Organization Regional Office for Eastern Mediterranean.
20. Darmstadt GL, Lawn JE, Costello A (2003) Advancing the state of the world’s newborns. Bulletin of the World Health Organization: 81: 224–225. 21. WHO Geneva (2005) Pocket book of hospital care for children: guidelines for
the management of common illnesses with limited resources.
22. WHO Geneva (2005) Technical updates of the guidelines on the integrated management of childhood illness (IMCI): evidence and recommendations for further adaptations.
23. Theodoratou E, Al-Jilaihawi S, Woodward F, Ferguson J, Jhass A, et al (2010) The effect of case management on childhood pneumonia mortality in developing countries. Int. J. Epi., (suppl 1): i155–i171.
24. WHO Geneva (2005) Treatment of diarrhea. A manual for physicians and other senior health care workers.
25. Munos M, Fischer Walker CL, Black RE (2010) The effect of oral rehydration solution and recommended home fluids on diarrhea mortality. Int J Epi: 39; i75– i87.
26. WHO Geneva (2010) Guidelines for the treatment of malaria. 2nd ed. 27. WHO Geneva (2010) Antiretroviral therapy for HIV infection in infants and
children: towards universal access: recommendations for a public health approach.
28. WHO Geneva (2010) Rapid advice. Use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Version 2. 29. WHO Geneva (2010) HIV diagnosis and treatment in infants and children. 30. Yang HM, Mao M, Wan CM (2009) Vitamin A for treating measles in children.
Cochrane Review: 2009(3).
31. Islam M, Yoshida S (2009) MDG 5: How close are we to success? British journal of obstetrics and gynaecology: 116 (Suppl.1), 2–5.
32. Bhutta ZA, Ahmed T, Black RE, Cousens S, Dewey K, et al (2008) What works? Interventions for maternal and child under nutrition and survival. Lancet: 371: 417–440.
33. WHO Geneva (2011) Priority medicines for mothers and children. Ensuring access to priority medicines for mothers and children improves health and saves lives. WHO reference number: WHO/EMP/MAR/2011.1.
34. Sara M (2006) A review of health seeking behaviour: problems and prospects: HSD/WP/05/03.
35. Bicego GT, Ties BJ (1993) Maternal education and child survival: a comparative study of survey data from 17 countries. Soc Sci Med; 36: 1207–1227. 36. Caldwell JC (1979) Education as a factor in mortality decline: an examination of
Nigerian data. Popul Stud (Camb); 33: 395–413.
37. Ozaltin E, Hill K, Subramanian SV (2010) Association of maternal stature with offspring mortality, underweight, and stunting in low- to middle income countries. JAMA 2010; 303: 1507–1516.
38. Emmanuela G, Krycia C, Rafael L, Christopher JLM (2010) Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: a systematic analysis. Lancet; 376: 959–74. 39. Cleland JG, van Ginneken JK (1988) Maternal education and child survival in
developing countries: The search for pathways of influence. Soc Sci Med; 27: 1357–1368.
40. Hobcraft J (1993) Women’s education, child welfare and child survival: a review of the evidence. Health Transit Rev; 3: 159–175.
41. Chou SY, Liu JT, Grossman M, Joyce T (2010) Parental Education and Child Health: Evidence from a natural experiment in Taiwan. Am Econ J Appl Econ; 2: 33–61.
42. Lynch SM (2003) Cohort and life-course patterns in the relationship between education and health: a hierarchical approach. Demography 2003; 40: 309–331. 43. Boyle MH, Racine Y, Georgiades K, Snelling D, Hong S, et al (2006) The influence of economic development level, household wealth and maternal education on child health in the developing world. Soc Sci Med; 63: 2242–2254.
44. Cutler DM, Lleras-Muney A (2006) Education and health: evaluating theories and evidence.
45. UNICEF (2011) UN inter-agency group for child mortality estimation. Levels and trends in child mortality. New York City: United Nations International Children’s Emergency Fund.
46. Rebecca K, Vera M, Peter DB (2010) Knowledge and reported practices of men and women on maternal and child health in rural Guinea Bissau: a cross sectional survey. BMC Public Health, 10: 319. 1471–2458.
47. Armand CT (2010) The Determinants and consequences of teenage pregnancy and motherhood in Sierra Leone: ‘‘children bearing children’’.
48. Gray Allison (2001) Definitions of crowding and the effect of crowding on health. Ministry of Social Policy, Te Manatu monga Kaupapa Oranga Tangata. 49. Johns Hopkins University (2002) Population information program. ‘‘Three to
Five Saves Lives’’, population reports, Volume XXX, Number 3, Series L, Number 13.
50. Maine D, McNamara R (1985) Birth spacing and child survival. Center for population and family health. Columbia University. New York.
51. Kabir M, Sufian AJM (1983) Life table analysis of birth interval for Bangladesh in Hunter: Health and Society. United Nation university food and nutrition bulletin Vol. 05, No.3.
52. UNICEF (2008) Tracking progress in maternal, newborn and child survival. The 2008 report. New York.
53. Glewwe P (1999) Why does mother’s schooling raise child health in developing countries: evidence from Morocco. The journal of human resources: 34(1): 124– 136.
54. Chatman LM, Salihu HM, Roofe ME, Wheatle P, Henry D, et al (2004) Influence of knowledge and attitudes on exclusive breastfeeding practice among rural Jamaican mothers. Birth: 31(4): 265–271.
55. Chandrashekhar TS, Joshi HS, Binu V, Shankar PR, Rana MS, et al (2007) Breast-feeding initiation and determinants of exclusive breastfeeding - a questionnaire survey in an urban population of western Nepal. Public Health Nutrition: 10(2): 192–197.
56. Taha AZ (2002) Assessment of mother’s knowledge and practice in use of oral rehydration solution for diarrhoea in rural Bangladesh. Saudi Medical Journal: 23(8): 904–908.
57. Rasania SK, Pathi D, Matta S, Singh S (2005) Knowledge and attitude of mothers about oral rehydration solution in few urban slums of Delhi. Health and population perspectives and issues: 28(2): 100–107.
58. Uwaezuoke SN, Emodi IJ, Ibe BC (2002) Maternal perception of pneumonia in children: a health facility survey in Enugu, eastern Nigeria. Annals of tropical paediatrics: 22(3): 281–285.
59. Galvez CA, Modeste N, Lee JW, Betancourt H, Wilkins RL (2002) Peruvian mothers’ knowledge and recognition of pneumonia in children under 5 years of age. Revista Panamericana de Salud Publica/Pan American Journal of Public Health: 11(2): 99 108.
60. Rakhshani F, Moghadam ARA, Alemi R, Moradi A (2003) Knowledge, perceptions and prevention of malaria among women in Sistan va Baluchestan, Islamic Republic of Iran. Eastern Mediterranean health journal: 9(3): 248–256. 61. Seck I, Fall IS, Faye A, Ba O, Tal-Dia A (2008) Malaria knowledge, attitudes and practices among women living in the rural area of Poponguine, Senegal. Revue Medecine Tropicale: 68(6): 629–633.
62. Mayhew M, Hansen PM, Peters DH, Edwards A, Singh LP, et al (2008) Determinants of skilled birth attendant utilization in Afghanistan: a cross-sectional study. American journal of public health: 98(10): 1849–1856. 63. Abdulsalam A (2005) Syrian women’s preferences for birth attendant and birth
place. Birth 2005: 32(1): 20–26.
64. Andrzejewski CS, Reed HE, White MJ (2009) Does where you live influence what you know? Community effects on health knowledge in Ghana. Health and Place 2009: 15: 228–238.
65. Senarath U, Fernando DN, Vimpani G, Rodrigo I (2007) Factors associated with maternal knowledge of newborn care among hospital-delivered mothers in Sri Lanka. Transactions of the Royal society of tropical medicine and hygiene: 101(8): 823–830.