REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Use
of
neuromuscular
blockers
in
Brazil
Giovani
de
Figueiredo
Locks
∗,
Ismar
Lima
Cavalcanti,
Nadia
Maria
Conceic
¸ão
Duarte,
Rafael
Martins
da
Cunha,
Maria
Cristina
Simões
de
Almeida
UniversidadeFederaldeSantaCatarina,Florianópolis,SC,Brazil
Received1May2014;accepted2March2015
Availableonline15August2015
KEYWORDS
Neuromuscular blockers;
Researchonhealth services;
Neuromuscular monitoring
Abstract TheobjectiveofthisstudywastoevaluatehowBraziliananesthesiologistsareusing neuromuscularblockers,focusingonhowtheyestablishthediagnosisofpostoperativeresidual curarizationandtheincidenceofcomplicationsassociatedwiththeuseofneuromuscular block-ers.Aquestionnairewassenttoanesthesiologistsinvitingthemtoparticipateinthestudy.The onlinedatacollectionremainedopenfromMarch2012toJune2013.Duringthestudyperiod, 1296responseswerecollected.Rocuronium,atracurium,andcisatracuriumwerethemain neu-romuscularblockersusedincasesofelectivesurgery.Succinylcholineandrocuroniumwerethe mainneuromuscularblockersusedincasesofemergencysurgery.Lessthan15%of anesthesiolo-gistsreportedthefrequentuseofneuromuscularfunctionmonitors.Only18%ofthoseinvolved inthestudyreportedthatallworkplaceshavesuchamonitor.Mostrespondentsreportedusing onlytheclinicalcriteriatoassesswhetherthepatientisrecoveredfromthemusclerelaxant. Mostrespondentsalsoreportedalwaysusingsomeformofneuromuscularblockadereversal. Themajorcomplicationsattributedtoneuromuscularblockerswereresidualcurarizationand prolonged blockade.Eighteenanesthesiologistsreporteddeathattributed to neuromuscular blockers.Residualorprolongedblockadeispossiblyrecordedasaresultofthehighrateof usingclinicalcriteriatodiagnosewhetherthepatienthasrecoveredornotfrommotorblock and,asacorollary,thepooruseofneuromusculartransmissionmonitorsindailypractice. © 2015SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Bloqueadores neuromusculares; Pesquisassobre servic¸osdesaúde; Monitorac¸ão neuromuscular
UsodebloqueadoresneuromuscularesnoBrasil
Resumo O objetivo desta pesquisa foi avaliar como os anestesiologistas brasileiros estão usandoos bloqueadoresneuromusculares(BNM), comfoconaformade estabelecero diag-nósticodacurarizac¸ãoresidual pós-operatóriaeaincidênciadecomplicac¸ões atribuídasao uso de BNM.Um questionáriofoienviado a anestesiologistasconvidando-os aparticipar da pesquisa(tabela1).Acoleta onlinededadospermaneceuabertademarc¸ode2012ajunho
∗Correspondingauthor.
E-mail:[email protected](G.F.Locks).
http://dx.doi.org/10.1016/j.bjane.2015.03.001
de2013.Duranteoperíododeestudoforamcoletadas1.296respostas.Rocurônio,atracúrio ecisatracúrioforamosprincipaisbloqueadoresneuromuscularesusadosemcasosdecirurgia eletiva.Succinilcolina erocurônio foram osprincipais BNM usadosem casos de cirurgia de emergência.Menosde15%dosanestesiologistasreferiramqueusamfrequentementemonitores dafunc¸ãoneuromuscular.Apenas18%dosenvolvidosnoestudoreferiramquetodososlocais detrabalhotêmtalmonitor.A maioriadosentrevistadosafirmouqueusasomenteocritério clínicoparaavaliarseopacienteestárecuperadodorelaxante.Amaioriadosentrevistados tambémrelatouquesempreusaalgumtipodereversãodebloqueioneuromuscular.Asprincipais complicac¸ões atribuídas aosBNM foram curarizac¸ão residuale bloqueio prolongado. Houve relatopor18anestesiologistasdeóbito atribuídoaBNM.Obloqueioresidualouprolongado seregistra,possivelmente,comoconsequênciadoaltoíndicedousodecritériosclínicospara diagnosticarseopacienteestárecuperadoounãodobloqueiomotore,comoumcorolário,o baixousodemonitoresdatransmissãoneuromuscularnapráticadiária.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Postoperativeresidualcurarization(PORC)isacomplication ofconsiderableimpactandprovensideeffects,sometimes potentiallylife-threatening.1---6
The diagnosisof deeprelaxationdegreesat theendof anesthesiacanbedonewiththeuseofbedsidetests; how-ever,curareresidualblocksareonlydetectedwiththeuse ofneuromusculartransmission(NMT)objectivemonitoring bytrain-of-four(TOF)andaccelerometry.7---11Althoughthere
isaconsensusintheliteratureonhowtodiagnose,aswell astheconsequencesofthiscomplication,thefrequencyof usingNMT monitors remains very low, even in developed countries.12---14
TheobjectiveofthisstudywastoevaluatehowBrazilian anesthesiologistsareusingneuromuscularblockers (NMB), focusingonhowtoestablishthediagnosisofPORCandthe incidenceofcomplicationsassociatedwiththeuseofNMB, andcompare theresults withthose obtained in a similar survey10yearsagoinBrazil15(Table1).
Method
After approval by the Human ResearchEthics Committee under the protocol # 2205/2011, an e-mail was sent to anesthesiologistsregisteredinthedatabaseoftheBrazilian Societyof Anesthesiology andAnestech,invitingmembers toparticipateinthesurvey‘‘Useofneuromuscular block-ersinBrazil’’.Intheemailmessagebody,participantswere informedthatparticipationwasnotmandatory,the collec-tionofresponses wouldbeanonymousanddatawouldbe confidentialand untraceable.The questionnaireconsisted of 10 questions, 2 about demographics and 8 about the choice of using NMB, neuromuscular function monitoring, blockade reversal, and complications associated withthe useofthesedrugs.
Theparticipantsaccessedalinktoawebsiteforonline data collection (Survey Monkey, USA). Data collection remainedopenfromMarch2012toJune2013.Toincrease theresponserate,threeinvitationsweresenttothe partic-ipants.Dataarepresentedasfrequency(percentage).
Results
Theinvitationtoparticipateinthesurveywassentto9910 anesthesiologists.Duringthestudyperiod,1296 responses werecollected.
Regardingtheyearsinpracticeofanesthesiology,there wasapredominanceofanesthesiologistswithover11years ofpractice(53.8%);30.7%and15.5%ofresponderswithup to5yearsofspecialtyandbetween6and10years, respec-tively.
Most participants were from the Southeast region (52.4%), followed by participantsfrom theSouth (20.6%), Northeast(15.6%),Midwest(8.4%),andNorth(3%)regions.
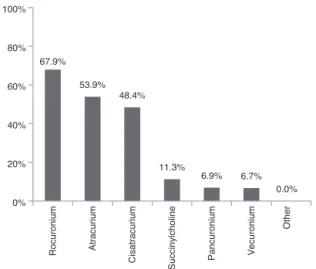
Most anesthesiologists who responded to the ques-tionnaire reported that rocuronium, atracurium, and cisatracuriumwerethemainNMBusedincasesofelective surgery.ThesedataareshowninFig.1.
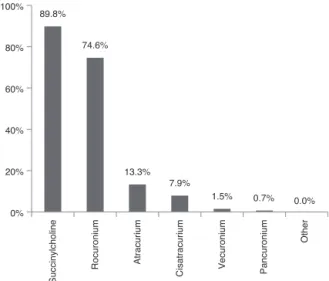
Mostanesthesiologistsindicatedthatsuccinylcholineand rocuroniumwerethemainNMBusedincasesofemergency surgery.DataareshowninFig.2.
67.9%
53.9% 48.4%
11.3%
6.9% 6.7% 0.0% 0%
20% 40% 60% 80% 100%
Rocuronium Atracurium
Cisatracurium
Succinylcholine Pancuronium
Vecuronium
Other
Figure1 MostcommonlyusedNMBfortrachealintubationin
Table1 Questionnairesenttosurveyparticipants.
1.Howmanyyearshaveyoubeeninpracticeof anesthesiology?
Upto5years
Between6and10years Over11years
2.Whatistheregionwhereyouexerciseyouroccupation?
North Northeast Midwest Southeast South
3.Checkthetwo(2)neuromuscularblockersyouusemost fortrachealintubationincasesofelectivesurgery.
Atracurium Cisatracurium Rocuronium Vecuronium Pancuronium Succinylcholine Other
4.Checkthetwo(2)neuromuscularblockersyouusemost fortrachealintubationincasesofemergencysurgery.
Cisatracurium Rocuronium Vecuronium Pancuronium Succinylcholine Others
5.Regardingtheuseofneuromusculartransmission monitor:
Never Rarely Sometimes Often
6.Hospital(s)inwhichyouwork:
AllhavetheTOFneuromusculartransmissionmonitor SomehavetheTOFneuromusculartransmissionmonitor NonehastheTOFneuromusculartransmissionmonitor
7.Asacriterion‘‘thepatienthasrecoveredfromthe musclerelaxant’’,youuse:
Onlytheclinicalcriteriaonly
OnlytheTOFneuromusculartransmissionmonitor TheclinicalcriteriaandtheTOFneuromuscular transmissionmonitor
8.Doyouuseanytypeofneuromuscularblockadereversal (neostigmineorsugammadex)?
Always
ItdependsontheoutcomeoftheTOFmonitor Idonotuse
9.Haveyoueverhadanycomplicationthatyouassignedto themusclerelaxant?
Prolongedblockade Residualcurarization Severebronchospasm Allergicreaction
Table1(Continuación)
Prolongedapneaaftersuccinylcholine Malignanthyperthermia
Seriouscardiacdysrhythmias Recurarization
10.Ifyoucheckedanyconditioninquestion9,inthecase consideredmostserious,thepatient:
Withoutsequelae
WithsequelaethatIconsideredmild/moderate Withsequelae
Withdeath
Lessthan15%ofanesthesiologistswhoparticipatedinthe studysaidtheyoften useneuromuscularfunction monitor (Fig. 3). Only 18% of respondents reportedthat all work-placeshavesuchamonitor(Fig.4).
Regarding the reversal of neuromuscular blockade at the end of anesthesia, the majority of respondents said that theyuse only the clinical criteriato assess whether the patient has recovered from the muscle relaxant. Mostrespondentsalsoreported alwaysusing somesort of neuromuscularblockadereversalagent(neostigmineor sug-ammadex) at the end of anesthesia. Data are shown in
Figs.5and6.
89.8%
74.6%
13.3% 7.9%
1.5% 0.7% 0.0% 0%
20% 40% 60% 80% 100%
Succinylcholine
Rocuronium Atracurium
Cisatracurium Vecuronium Pancuronium
Other
Figure2 MostcommonlyusedNMBfortrachealintubationin
casesofemergencysurgery.Totalof1294responses.
36.6%
25.5% 23.3%
14.6%
0%
I do not use I rarely use
I use sometimes
I often use
25% 50%
Figure3 Standarduse of neuromuscularfunction monitor.
18.0%
55.3%
26.7%
0% 20% 40% 60%
None has the TOF neuromuscular
transmission monitor All have the
TOF neuromuscular transmission
monitor
Some have neuromuscular
transmission monitor TOF
Figure4 AvailabilityofTOFneuromusculartransmission
mon-itorattheworkplacesof1292anesthesiologists.
60.5%
4.7%
34.8%
0% 20% 40% 60% 80%
Clinical criteria and TOF neuromuscular
transmission monitor Only clinical
criteria only
Only TOF neuromuscular
transmission monitor
Figure5 Criterion used toevaluate patient recovery after
neuromuscularblockadeby1291anesthesiologists.
39.2%
44.7%
14.4%
1.7% 0%
20% 40% 60%
Depends on TOF monitor Always
Sometimes Never
Figure 6 Use of neuromuscular blockade reversal
(sugam-madexorneostigmine)attheendofanesthesia.Totalof1296
responses.
The complications associatedwith the use of NMB are described in Fig. 7. Residual curarization and prolonged blockade were the main complications. Mostrespondents indicated that patients evolved without sequelae after complications,but18anesthesiologistsreporteddeath asso-ciatedwithNMB(Fig.8).
Discussion
Inthisstudy,13%ofquestionnaireswerecompleted(1296 of 9910 questionnaires sent). We found a percentage of responsessimilartoNaguibetal.,16 whosepercentagewas
10% (1792 of 17,870) in the United States and 15% (844 of4807) in Europe. Phillipsetal.,17 in Australia andNew
Zealand,reporteda slightly higher numberin percentage terms(21%).However,thetotalnumberofrespondentswas limitedto678.
70.5%
46.2%
26.7%
16.5%
10.8% 9.7%
2.2% 1.8%
0% 20% 40% 60% 80%
Residual curarization Prolonged blockade
Allergic reaction
Severe bronchospasm
Recurarization
Prolonged apnea
after succinylcholine
Severe cardiac
arrhythmias
Malignant hyperthermia
Figure7 ComplicationsattributedtotheuseofNMBby1160
anesthesiologists.
95.8%
2.2% 0.5% 1.6%
0% 20% 40% 60% 80% 100%
Without sequelae
With mild/moderate
sequelae
With severe sequelae
With death
Figure8 Evolutionofpatientswithcomplicationsattributed
totheuseofNMB.Totalof1156responses.
MainNMBused
The main NMB used in Brazil for elective surgical pro-cedures are rocuronium, atracurium, and cisatracurium. Results reportedin aprevious studyshowed thattheNMB commonly used 10 years ago were atracurium, pancuro-nium, and succinylcholine.15 In other parts of the world
itsuse is slightly different.Naguib etal.16 reportedthat,
in Europe, the threemost commonly usedneuromuscular blockingagentsarerocuronium(75%),atracurium(49%),and succinylcholine(47%)and,intheUnitedStates,rocuronium (89%), vecuronium (63%), and atracurium (47%). Specifi-cally in France, the most used NMB are atracurium and cisatracurium.18 We could say that, in the USA, there is
a greater tendency toward using steroidal NMB, whereas inFrancearethebenzylisoquinolineneuromuscular block-ing agents. In Brazil there is a more even distribution of bothsteroidalNMBandbenzylisoquinolineagents.Wecould explainthisdifferencebetweencountriesbymarketsupply reasons andthe incidenceof adverse effects,particularly anaphylactic reactions,which seemtobedifferentin dif-ferentpartsoftheworld.19---22
Emergencytrachealintubation
Succinylcholineremainsthedrugofchoicebyrespondents for emergency tracheal intubation, a result similar to that found in a previous study,15 with rocuronium as a
Eldawlatlyetal.23intheMiddleEastandbyNaguibetal.16
inEuropeandtheUSA.Thiscanbeexplainedbytherapid onset of action and the clinical ultrashort duration of succinylcholine.Rocuroniumhasemergedasanoptiondue toitssimilarprofile of onsetof action andespecially the possibilityofrapidreversalwithsugammadex.Sugammadex at a dose of 16mgkg−1 is abletocompletely reverse the
deep neuromuscular blockade induced by rocuroniumin in less time than the spontaneous recovery of 1mgkg−1
dose of succinylcholine.24 With such flexibility of use, it
can be supposed that the introduction of sugammadexin theEuropeanmarketisthecauseofincreasedrocuronium consumptioninFrance.18
Clinicalcriteriatodiagnosetheendofthe blockade
MostBraziliananesthesiologistsremainusingclinical crite-riatodiagnosetheendofmusclerelaxation,15 suchasthe
registered inAustralia andNew Zealand.17 This is a
ques-tionableconduct, asseveralauthors have shown that the clinical testsalone or in combination have low sensitivity and specificity in the diagnosis of residual neuromuscular blockade.
Residualneuromuscularblockademaybepresentdespite theuseofsubjective monitorsofneuromuscularfunction, clinicaltrials,andreversingagents.25,26 Onlytheobjective
monitoringofneuromuscularfunctionisabletodiagnosethe degreeofresidualneuromuscularblockade,andcurrentlyit isconsideredthattheT4/T1ratiobyTOFmustbeequalto or preferablyhigherthan0.9 tobeconsidered absenceof residualneuromuscularblockade.DiMarcoetal.,inastudy of the residual curarization knowledge in Italy, reported thatonly24%of anesthesiologistsresponded thatthesafe T4/T1ratio for trachealextubation was0.9.27 This result
issimilartoothersreportedinAustraliaandNewZealand, where anesthesiologists considered the T4/T1 ratio ≥0.9
asan acceptable criterion for safe tracheal extubation.17
ThepresentsurveyresultsshowthatinBrazilonly4.6%use onlymonitor forthediagnosis ofmusclerelaxation recov-ery. Probably it is notonly due tothe outdatedscientific knowledgebytheanesthesiologist,butalsothelackof neu-romuscularfunctionmonitors.
Monitoruseandavailabilityofmonitors
This surveyshowedthat only14%of Brazilian anesthesiol-ogistsroutinelyuseobjectivemonitoringofneuromuscular function,aresultquiteclosetothatfoundinAustraliaand NewZealand(17%)17 andmuchlowerthanthepercentage
inFrance,whichis52%whenusingsingledoseofNMBand 74%whenusingmaintenancedoses.28
In this survey, only 18% of the Brazilian respondents’ workplaces have neuromuscular function monitor. These resultsaresimilartothosefoundintheUSA(22%)and dif-ferwidelyfromthosefoundinEurope(70%),16 althoughin
theBrazilianstudythereisnoseparationofqualitativeand quantitativemonitors.InAustraliaandNewZealand, quan-titative neuromuscular function monitors are available in
58%ofhospitalswhere respondentspracticeanesthesia,a numbergreaterthanthatfoundinBrazil.17
ReversingNMB
Regardingthereversalofneuromuscularblockade,wefound thatalmost halftheanesthesiologistsalwaysusesreversal agents,eithersugammadexorneostigmine.Thisfactmaybe aresultoftheunavailabilityofNMTmonitorsinmost Brazil-ianhospitals.However,thisapproachmaybequestionedas theuseofneostigmineafterneuromuscularblockade com-plete recovery may result in muscle weakness. We found thatonly14%statedthattheuseofreversalagentis condi-tionedtotheresultsofTOF.Thispercentageislowerthan thatfoundamonganesthesiologistsintheMiddleEast23and
couldbeexplainedbythelackofNMTmonitorsinBrazil.
ComplicationsofusingNMBandreversal
The complicationsmost often citedinthis surveyarethe residual neuromuscular blockade followed by prolonged neuromuscularblockade.Estevesetal.29foundanincidence
ofresidualneuromuscularblockadeof26%(TOF<0.9).This demonstratesthat,despitethescientificknowledgeofthe problemandthe use ofsugammadex, a high incidenceof thiscomplicationstillremains.30
InBrazil,theuseofclinicalcriteriatomonitortheend ofneuromuscularblockadeandthelackofobjective moni-toringofNMTmaybeoneofthecausesofthisproblem.In AustraliaandNewZealand,71%ofrespondentsinasurvey underestimatetheincidenceofresidualcurarization.17
Residual neuromuscular blockade may result in severe clinicalcomplications.31,32
The data of this survey show that 26% reported aller-gic reactions as a complication of using NMB. Among the agents used in anesthesia, NMB are the ones that cause mostanaphylaxis,withapercentageof 58%.19,33 The
inci-denceofallergicreactionsduringanesthesiaretrievedfrom theFrenchnational databaseis greater thanthe previous estimate.33Chongetal.foundthatNMBwerethecausative
agentsofanaphylaxisduringgeneralanesthesiainaseries of23patientswithanaphylacticshock.34
Prolonged apnea reported by 9% and serious cardiac arrhythmiasby2%ofrespondentstothissurveyarelistedin theresultsofthestudybyKaranovi´cetal.35whoreported
the most common adverse events reported for succinyl-choline:myalgia (47%),prolongedblockade(36%),allergic reaction(13%),andasystole(12%).Asystematicreviewby Abrishamietal.36 demonstratedthatthereis noevidence
ofdifferencesintheprevalenceofadverseeventsbetween sugammadex,placebo,orneostigmine.
Evolutionofpatientswithcomplicationsafterthe useofNMB
Inthissurvey,theconsequencesarisingfromcomplications ofusingNMBwereconsideredseverein 0.5%ofcasesand withdeath1.6%.This resultdemonstratesthatthe useof NMBmaybe relatedtounfavorableoutcomes, as demon-stratedby Naguibetal.,16 Eikermann etal.,5 and Murphy
et al.7,38,39 The justification could be found in the very
resultsofthissurvey:theuseofclinicalcriteriaforresidual neuromuscularblockadediagnosis, low use andlow avail-abilityofquantitativeNMT monitors,inappropriateuseof reversalagents,andpossiblytheproperinadequate diagno-sisandtreatmentofcomplicationscouldexplaintheserious adverseoutcomes.
Studylimitations
Theelectronicmeansuseddidnotreachallrecipients,due tospam typemechanism orsome outdatede-mailsinthe databaseused,whichmayhavehamperedtheparticipation ofalargernumberofanesthesiologists.
WeconcludebythissurveyontheuseofNMBinBrazil thatthefollowingaspectsstoodout:succinylcholineisstill themostfrequentlyusedNMBforemergencysituations,the rates of PORC and prolonged muscular block are high, as wellastherecord ofsequelae considered seriousor even deathascomplicationsofusingthesedrugs.Theresidualor prolongedblockadeis possiblyseenasaresultofthehigh rateofusingclinicalcriteriatodiagnosewhetherthepatient hasrecoveredornotfrommotorblockand,asacorollary, thelowuseofNMTmonitorsindailypractice.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BergH,RoedJ,Viby-MogensenJ,etal.Residualneuromuscular blockisariskfactorforpostoperativepulmonarycomplications. A prospective,randomised, and blinded studyof postopera-tivepulmonarycomplicationsafteratracurium,vecuroniumand pancuronium.ActaAnaesthesiolScand.1997;41:1095---103. 2.MathiasLA, daST, de Bernardis RCG.Postoperative residual
paralysis.RevBrasAnestesiol.2012;62:439---50.
3.WarnerMA.Perioperativemortality:intraoperativeanesthetic managementmatters.Anesthesiology.2005;102:251---2. 4.BrullSJ, NaguibM,Miller RD.Residualneuromuscularblock:
rediscoveringtheobvious.AnesthAnalg.2008;107:11---4. 5.EikermannM,VogtFM,HerbstreitF,etal.Thepredispositionto
inspiratoryupperairwaycollapseduringpartialneuromuscular blockade.AmJRespirCritCareMed.2007;175:9---15.
6.ErikssonLI,SatoM,SeveringhausJW.Effectofa vecuronium-induced partial neuromuscular block on hypoxic ventilatory response.Anesthesiology.1993;78:693---9.
7.Murphy GS, Brull SJ. Residual neuromuscular block: lessons unlearned. Part I:Definitions, incidence,and adverse physi-ologiceffectsofresidualneuromuscularblock.AnesthAnalg. 2010;111:120---8.
8.Fuchs-Buder T, Claudius C, Skovgaard LT, et al. Good clinical research practice in pharmacodynamic studies of
neuromuscularblockingagentsII:theStockholmrevision.Acta AnaesthesiolScand.2007;51:789---808.
9.Eikermann M, Groeben H, Hüsing J, et al. Accelerometry of adductor pollicis muscle predicts recovery of respira-tory function from neuromuscular blockade. Anesthesiology. 2003;98:1333---7.
10.MortensenCR,BergH,el-MahdyA,etal.Perioperative moni-toringofneuromusculartransmissionusingacceleromyography preventsresidualneuromuscularblockfollowingpancuronium. ActaAnaesthesiolScand.1995;39:797---801.
11.GätkeMR,Viby-Mogensen J,RosenstockC,et al. Postopera-tive muscle paralysis after rocuronium: less residual block when acceleromyography is used. Acta Anaesthesiol Scand. 2002;46:207---13.
12.SorgenfreiIF,Viby-MogensenJ,SwiatekFA.Doesevidencelead toachangeinclinicalpractice?Danishanaesthetists’andnurse anesthetists’clinicalpracticeandknowledgeofpostoperative residualcurarization.UgeskrLaeger.2005;167:3878---82. 13.Fuchs-BuderT,HofmockelR,GeldnerG,etal.Theuseof
neuro-muscularmonitoringinGermany.Anaesthesist.2003;52:522---6. 14.GraylingM,SweeneyBP. Recoveryfromneuromuscular
block-ade:asurveyofpractice.Anaesthesia.2007;62:806---9. 15.AlmeidaMCS.OusodebloqueadoresneuromuscularesnoBrasil.
RevBrasAnestesiol.2004;54:850---64.
16.Naguib M, Kopman AF, Lien CA, et al. A survey of current managementofneuromuscularblockintheUnitedStatesand Europe.AnesthAnalg.2010;111:110---9.
17.PhillipsS,StewartPA,BilginAB.Asurveyofthemanagement of neuromuscularblockade monitoring in Australia and New Zealand.AnaesthIntensiveCare.2013;41:374---9.
18.BenyK, PiriouV,DussartC,etal.Impactofsugammadexon neuromuscularblockingagentsuse:amulticentric, pharmaco-epidemiologicstudyinFrenchuniversityhospitalsandmilitary hospitals.AnnFrAnesthReanim.2013;32:838---43.
19.Sadleir PHM, Clarke RC, Bunning DL, et al. Anaphylaxis to neuromuscularblocking drugs: incidenceand cross-reactivity in Western Australia from 2002 to 2011. Br J Anaesth. 2013;110:981---7.
20.MertesPM,TajimaK,Regnier-KimmounMA,etal.Perioperative anaphylaxis.MedClinNorthAm.2010;94:761---89.
21.Dewachter P, Mouton-Faivre C, Emala CW. Anaphylaxis and anesthesia: controversies and new insights. Anesthesiology. 2009;111:1141---50.
22.DongSW,MertesPM,PetitpainN,etal.Hypersensitivity reac-tionsduringanesthesia.Resultsfrom theninthFrenchsurvey (2005---2007).MinervaAnestesiol.2012;78:868---78.
23.Eldawlatly A, El-Tahan MR. A survey of the current use of neuromuscularblockingdrugsamongtheMiddleEastern anes-thesiologists.SaudiJAnaesth.2013;7:146---50.
24.Sørensen MK, Bretlau C, Gätke MR, et al. Rapid sequence inductionandintubation withrocuronium---sugammadex com-paredwithsuccinylcholine:arandomizedtrial.BrJAnaesth. 2012;108:682---9.
25.BaillardC.Incidenceandcomplicationsofpostoperative resid-ualparalysis.AnnFrAnesthReanim.2009;28Suppl.2:S41---5. 26.KotakeY,OchiaiR,SuzukiT,etal.Reversalwithsugammadex
intheabsenceofmonitoringdidnotprecluderesidual neuro-muscularblock.AnesthAnalg.2013;117:345---51.
27.Di Marco P, Della Rocca G, Iannuccelli F, et al. Knowledge ofresidual curarization: anItalian survey. Acta Anaesthesiol Scand.2010;54:307---12.
28.Fuchs-Buder T, Meistelman C. Monitoring of neuromuscular block and prevention of residual paralysis. Ann Fr Anesth Reanim.2009;28Suppl.2:S46---50.
30.Kaan N, Kocaturk O, Kurt I, et al. The incidence of resid-ual neuromuscular blockade associated with single dose of intermediate-actingneuromuscularblockingdrugs.MiddleEast JAnesthesiol.2012;21:535---41.
31.KumarGV,NairAP,MurthyHS,etal. Residualneuromuscular blockadeaffectspostoperativepulmonaryfunction. Anesthesi-ology.2012;117:1234---44.
32.Cedborg AIH, Sundman E, Bodén K, et al. Pharyngeal func-tionandbreathingpatternduringpartialneuromuscularblock inthe elderly:effects onairway protection. Anesthesiology. 2014;120:312---25.
33.MertesPM,AllaF,TréchotP,etal.Anaphylaxisduringanesthesia inFrance:an8-yearnationalsurvey. JAllergyClinImmunol. 2011;128:366---73.
34.ChongYY,Caballero MR,LukawskaJ, etal.Anaphylaxis dur-inggeneralanaesthesia:one-yearsurveyfromaBritishallergy clinic.SingapMedJ.2008;49:483---7.
35.Karanovi´cN,CarevM,KardumG,etal.Succinylcholineusein adultanesthesia ---a multinationalquestionnairesurvey. Coll Antropol.2011;35Suppl.1:183---90.
36.Abrishami A, Ho J, Wong J, et al. Sugammadex, a selec-tivereversalmedicationforpreventingpostoperativeresidual neuromuscular blockade. Cochrane database Syst Rev. 2009. CD007362.
37.HopkinsPM.Malignanthyperthermia:pharmacologyof trigger-ing.BrJAnaesth.2011;107:48---56.
38.MurphyGS,SzokolJW, AvramMJ,etal.Postoperative resid-ualneuromuscularblockadeisassociatedwithimpairedclinical recovery.AnesthAnalg.2013;117:133---41.