w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Sphincteroplasty
and
perineoplasty
with
skin
advancement
flap
in
management
of
traumatic
cloacal
defect
Fakhrolsadat
Anaraki
a,
Omid
Etemad
b,∗aShahidBeheshtiUniversityofMedicalSciences,ColorectalDivisionofSurgeryWard,TaleghaniHospital,Tehran,Iran
bShahidBeheshtiUniversityofMedicalSciences,SurgeryWard,TaleghaniHospital,Tehran,Iran
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6August2016 Accepted31August2016
Availableonline28September2016
Keywords:
Traumaticcloacadefect Sphinctroplasty Prinealreconstruction Skinadvancementflap
a
b
s
t
r
a
c
t
Background:Traumaticcloacaldefect(TCD)istheconditionthatoccursin0.3%ofwomen whohaveexperiencedthethird/fourth-degreeperineallacerationduringtraumaticNatural VaginalDelivery(NVD).Thisconditionhasmanyundesirableeffectsintheirlives.Surgery isthebestwaytorepairthisdeformityandwillimprovethequalityoflifeinthesepatients.
Design:Inthisstudy,weprospectivelystudied19patientswhowerereferredtothehospital withsymptomsofTCDwithinyears2011and2015withthemeanof2.6-yrsfollow-up.They allunderwentsphincteroplastyandperineoplastywithskinadvancementflap.
Results:Ofall19patients,incontinencetosolidfaecesin16patients(84%),incontinenceto liquidstoolin15patients(78%)andincontinencetoflatusin4patients(21%)were com-pletelyresolved.TheFIscorewasdecreasedfromthemeanof12.7to2.6.Sexualfunction wassignificantlyimprovedinallofthemanddyspareuniawascompletelydisappearedin 9patients(50%).Thequalityoflifescorewasincreasedfromthemeanof45to95. Post-operationcomplicationswereoccurredin3ofpatients(woundinfectionin2-casesand recto-vaginalfistulainanother).
Conclusion:Ourfindingsshowthatsphincteroplastyandperineoplastywithskin advance-mentflapisaneffectivesurgicaltechniquetorepairtheperinealbodyduetoitsbenefits andfewcomplications.Inthisstudy,therewassignificantimprovementinqualityoflifeof almostallpatientsafterthisreconstructivesurgery.Consultingwithacolorectalsurgeonis recommendedforthesecases.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](O.Etemad).
http://dx.doi.org/10.1016/j.jcol.2016.08.002
Esfincteroplastia
e
perineoplastia
com
retalho
cutâneo
de
avanc¸o
no
tratamento
de
defeito
cloacal
traumático
Palavras-chave:
Defeitocloacaltraumático Esfincteroplastia
Reconstruc¸ãoperineal Retalhocutâneodeavanc¸o
r
e
s
u
m
o
Experiência: Defeitocloacaltraumático(RCT)éacondic¸ãoqueocorreem0,3%dasmulheres quesofreramlacerac¸ãoperinealdeterceiro/quartograuduranteumpartovaginalnatural (PNV)traumático.Essacondic¸ãocausamuitosefeitosindesejáveisemsuasvidas.Acirurgia éamelhorformaderepararessadeformidade,emelhoraráaqualidadedevidanessas pacientes.
Modelo: Nesseestudo,estudamos prospectivamente 19 pacientesqueforam encamin-hadasaohospitalcomsintomasdeRCTentre2011e2015,comumamediade2,6anosde seguimento.Todasforamsubmetidasaumaesfincteroplastiaeperineoplastia,comretalho cutâneodeavanc¸o.
Resultados:Datotalidadede19pacientes,aincontinênciaparafezessólidasem16pacientes (84%),aincontinênciaparafezeslíquidasem15pacientes(78%)eaincontinênciaparaflatos emquatropacientes(21%)foramcompletamenteresolvidas.Ocorreureduc¸ãonoescoreFI, deumamediade12,7para2,6.Afunc¸ãosexualmelhorousignificativamenteemtodasas pacientes,eadispareuniadesapareceucompletamenteemnovepacientes(50%).Oescore paraqualidadedevidamelhorou,damediade45para95.Ocorreramcomplicac¸ões pós-operatóriasemtrêspacientes(infecc¸ãodaferidaemdoiscasosefistularetovaginalnocaso restante).
Conclusão: Nossosachadosdemonstramqueaesfincteroplastiaeaperineoplastiacom retalhocutâneodeavanc¸oétécnicacirúrgicaefetivaparaoreparodocorpoperineal,grac¸asa seusbenefícioseàspoucascomplicac¸ões.Nesseestudo,foiobservadamelhorasigana qual-idadedevidadepraticamentetodasaspacientesemseguidaaessacirurgiareconstrutiva. Parataiscasos,érecomendávelumaconsultacomumcirurgiãocolorretal.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Background
Cloacaldeformityistheconditionthatoccursin0.3%ofthe patients with the third or fourth-degree laceration during (NVD).1–4Thisinjuryischaracterizedbydisruptionofthe
peri-nealbodyanddistalportionofrecto-vaginalseptum.1
Patients with cloacal deformity invariably suffer from severe incontinence to flatus, liquid and solid stool and severeurinaryandvaginalinfections.5Difficultiesduring
sex-ualfunctionsuchasdyspareuniainthesepatientsare also annoying.1–5 Theseproblemsmayleadtopsychologicaland
physicaldisorderssuchassocialisolationandsexual dysfunc-tionwhichcoulddecreasethequalityoflife.1–5Forpatients
withhistoryofTCDandsuccessfulsurgicalrepair,Caesarean sectionseemsreasonableforthenextdelivery.5
Todiagnosethisdeformityweshouldhaveacareful obstet-ric history and detailed physical examination of perineal area.1Diminutionorabsenceofprinealbodyandthe
anovagi-nal/rectovaginalseptuminwomenwithhistoryoftraumatic NVDaretheevidencesofcloacaldeformity.
There are also additional diagnostic tests including endoanal ultrasound, manometry and pudendal nerve stimulation.6
SeveralsurgicaltechniquesareavailabletotreatTCDand reconstructperinealbody.Inthisstudy,wewillstudythe con-ditionsof19patientswhowereunderwentsphincteroplasty
andperineoplastywithskinadvancementflaptorepairthe perinealbodybetween2011and2015atthe follow-upplan between3-monthsand4-yrswiththemeanof2.6-yrs.
Objective
Thesphincteroplastyand perineoplastywithskin advance-ment flap were performed for all patients. All data are gatheredformean2.6-yrs offollow-up. Thedatarelatedto incontinencescoreandqualityoflifewerecollectedbyusing WextnerFaecalIncontinenceScore(FIScore)andQualityof Life (QoL) form which are available in Appendix 1 and 2, respectively.
Other data including pre- and post-operation dyspareu-nia,sexualfunctionsatisfaction,satisfactionoftheresultsof surgery,andalsopost-operationcomplicationswerecollected throughinterviewswitheachpatient.
Fig.1showsTCDinoneofthepatients.
Design
Fig.1–Traumaticcloacadefectinoneofthepatients.
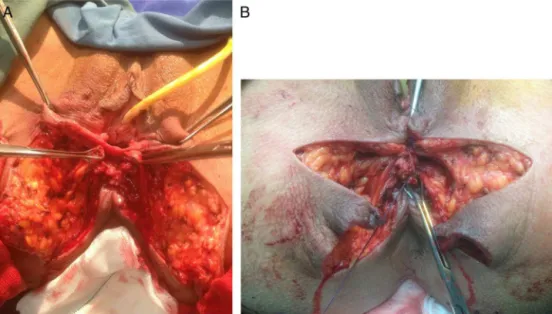
• Identifyingtheskinflapwithapproximatelengthof8–10cm (Fig.2B).
• Separationofano-rectumfromthevaginabydissectingthe recto-vaginalseptum(Fig.3A).
• Performanceofsphincteroplastyinordertooverlappingthe internalandexternalsphincter(Fig.3B).
• Reconstructionofperinealbodybyapproximatingthe bul-bocavernosus,externalsphincterand transverseperineal muscles.
• Reconstruction ofperineal skinwith advancement flaps (Fig.4).
Overlappingsphincteroplastywasperformedbyusing2/0 vicryl separated sutures. Perineal body was reconstructed byapproximatingbulbocavernosus,transverse perinealand externalsphinctermuscles.Finallyskinreconstructionwas donewithadvancementflapandhemovacdrainwasplaced under the flap. The patienst left NPO for three days and loperamidewasadministeredforthemandthewoundwas dresseddaily.Thedrainwasremovedafter3–4days.
Outcome
measures
WeconsideredthenumberofNVDs,BMI,ageandthe inter-valbetweenthetraumaticNVDandreconstructiveoperation. ThisinformationistabulatedinTable1.
Alsoasyou canfindfrom Table2,wecollectedthedata
ofall19patientsincludingtheFaecalIncontinence(FI)score (accordingtotheWexnerFIscoreinAppendix1),Qualityof Life(QoLforminAppendix2),dyspareunia,lifesatisfaction in pre- and post-operation, post-op complicationssuch as woundinfection,recto-vaginalfistulaandflapnecrosisand satisfactionbytheresultsofthesurgery.Foreasyanalyzing, weallocatedanumbertoeachpatient.
Results
AccordingtoTable1,themeanageofpatientsatthetimeof surgerywas35-yrs-oldandthemeanintervalyearsbetween thetraumaticNVDandthereconstructivesurgerywas5.9-yrs. ThemeanBMIofthepatientsatthetimeofsurgerywas26.63. AsitcanbefoundfromTable2,of19patientswhosuffered from faecalincontinence,3ofthem(15%)were completely curedwiththepost-opscoreof0/20,andthereisasignificant improvementinothers.Incontinencetothe solidstoolwas treatedin16patients(84%)and4patients(21%)stillsuffered fromincontinencetotheliquidstool.Theincontinencetothe gaswascompletelycuredin3patients(15%).Consequently thefaecalincontinencescorewassignificantlydecreasedin
Fig.3–(A)Separationofano-rectumfromthevaginabydissectingtherecto-vaginalseptum;(B)performanceof sphincteroplastyinordertooverlappingtheinternalandexternalsphincter.
Fig.4–Reconstructionofperinealskinwithadvancement flaps.
allpatients.ThemeanFIscorewasdecreasedfrom12.7/20to 2.6/20(Fig.5).
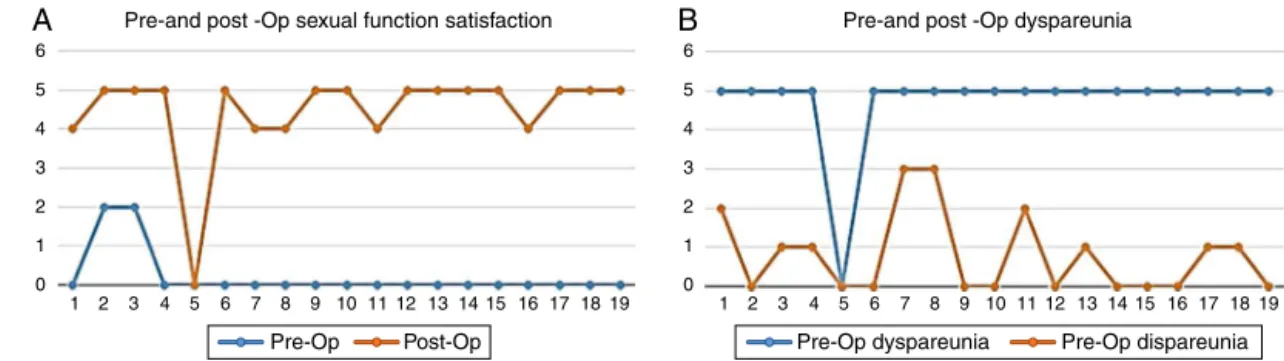
Of18patientswhohadsexualfunctionaftersurgery,sexual functiondissatisfactioninallofthepatientswascompletely resolved(Fig.6A).
Of18patientswhohadsexualfunction,thedyspareunia was cured in 9 patients. The score of this parameter was decreasedfromthemeanof5tolessthan1(Fig.6B).
Pre-and post-Op FI score (Wextner)
Pre-Op FI score Post-Op FI score
25 20 15 10 5 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Fig.5– Comparisonofpre-andpost-opfaecalincontinence score.
Thequalityoflifehadasignificantimprovementandwas increasedfromthemeanof45/119to95/119(Fig.7).
17patients(89.47%)weresatisfiedand2patients(10.52%) wererelativelysatisfiedfromtheresultsofsurgery(Fig.8).
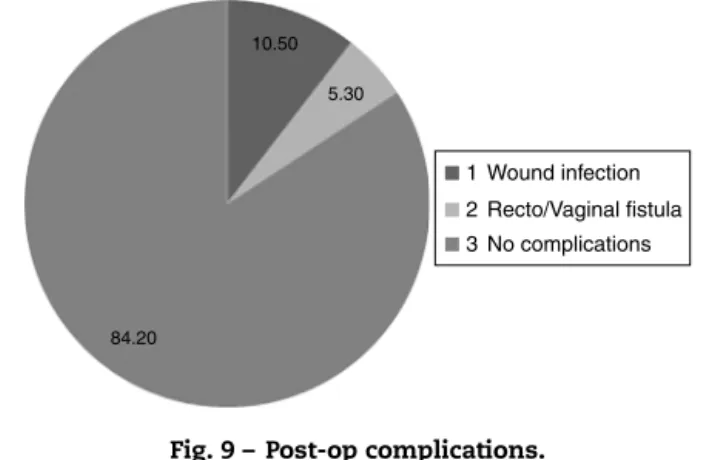
Asit canbe foundfromFig. 9, recto/vaginalfistulawas occurredinonepatient(5%)andwoundinfectionin2patients (10%)whichallofthemweremanagedconservatively.There wasnocomplicationreportedintheothers.
Alsowehaveinvestigatedifthereareanysignificant dif-ferencesbetweenthepre/postopvaluesofthegivenvariables byusingSPSSver.20.
Table1–Patientsdata.
Patients 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Age 25 29 33 30 71 58 20 37 32 39 42 33 41 27 27 30 33 38 32
BMI 25 23 29 27 30 20 25 31 23 27 26 28 30 34 26 30 22 27 25
Interval(-yrs) 4 2 4 1.5 20 10 8 5 2 1 20 3 10 4 1 10 3 3 2
Pre-and post -Op sexual function satisfaction Pre-and post -Op dyspareunia
Pre-Op Post-Op Pre-Op dyspareunia Pre-Op dispareunia
6 5 4 3 2 1
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 0
6 5 4 3 2 1 0
A
B
Fig.6–Changesinpre-opandpost-opsexualfunctionsatisfaction(A)anddyspareunia(B).
Table2–Dataofpre-andpost-op.
Patients Pre-op FI
Post-op FI
Pre-op dyspareunia
Post-op dyspareunia
Pre-opsexual function satisfaction
Post-opsexual function satisfaction
Pre-op QoL
Post-op QoL
Complication Satisfaction
1 8/20 3/20 5/5 2/5 0/5 4/5 48/119 100/119 Wound
infection Yes
2 4/20 1/20 5/5 0/5 2/5 5/5 81/119 116/119 – Yes
3 4/20 1/20 5/5 1/5 2/5 5/5 87/119 100/119 – Yes
4a 15/20 0/20 5/5 1/5 0/5 5/5 34/119 98/119 – Yes
5 10/20 7/20 – – – – 37/119 79/119 – Relatively
6 4/20 0/20 5/5 0/5 0/5 5/5 82/119 102/119 Wound
infection Yes
7 16/20 5/20 5/5 3/5 0/5 4/5 36/119 87/119 – Relatively
8 16/20 4/20 5/5 3/5 0/5 4/5 36/119 72/119 – Yes
9 20/20 11/20 5/5 0/5 0/5 5/5 34/119 60/119 – Yes
10 10/20 4/20 5/5 0/5 0/5 5/5 36/119 72/119 – Yes
11 16/20 2/20 5/5 2/5 0/5 4/5 38/119 99/119 – Yes
12 16/20 3/20 5/5 0/5 0/5 5/5 38/119 85/119 – Yes
13 10/20 1/20 5/5 1/5 0/5 5/5 43/119 98/119 – Yes
14 20/20 0/20 5/5 0/5 0/5 5/5 38/119 108/119 R.V.F.b Yes
15 12/20 1/20 5/5 0/5 0/5 5/5 45/119 98/15 – Yes
16 13/20 2/20 5/5 0/5 0/5 4/5 47/119 106/119 – Yes
17 15/20 2/20 5/5 1/5 0/5 5/5 43/119 95/119 – Yes
18 16/20 1/20 5/5 1/5 0/5 5/5 49/119 98/119 – Yes
19 15/20 2/20 5/5 0/5 0/5 5/5 38/119 105/119 – Yes
a Thepatientwhosehusbandisdeadanddidnothavesexualactivity.
b Recto-VaginalFistula.
By assuming that the acceptable ofthe (sig.) p-value is
p<0.05,theresultsshowasignificantdifferencebetween pre-andpostopFIscore,pre-andpostopdyspareunia,pre-and post opsexual functionsatisfaction,and pre- and post op qualityoflife.p-valuerangeofeach parameteristabulated
inTable3.
Quality of life score
140 120 100 80 60 40 20 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Pre-Op Post-Op
Fig.7–Post-surgicalimprovementofqualityoflife.
Discussion
TCD is a rare complication of traumatic NVD which may lead to faecal incontinence, stress, social isolation and
10.53
89.47
Satisfied Relatively satisfied Dissatisfied
10.50 5.30
Wound infection
Recto/Vaginal fistula
No complications 1
2
3
84.20
Fig.9–Post-opcomplications.
physiologicaldamagesinapatient.Repairandreconstruction ofperineal bodyanddeformedorgans forthesepatientsis efficient.Thevitalpartofsuchtheseproceduresisprecision whiledissectingand dividingthe ano-vaginal/recto-vaginal septum.There are several surgical techniques totreat the TCD and almost all of them have a significant impact to improve the physical and physiological conditions of the patients.
Thereareseveralarticlesinwhichthedeformityofcloaca hasbeentreatedbyusingdifferenttechniquesof reconstruc-tivesurgery.3,7–9Inordertoanalyzetheoutcomesoftheother
surgeonswithours, wehavecompared ourmainvariables withtheothersasfollows.
Pre/postopFIscore
Inthisstudy,faeces,liquidstoolandgasincontinencywas resolvedin84%,78%and15%ofthepatients,respectively.Also themeanFIscorewasdecreasedfrom12.7to2.6.
In the Spanos’sstudy on 4patients, the mean FIscore was decreased from 18 to 1.5 In the Hollingshead’s study
on 29 patients, incontinence to faeces, liquid stool and gas was resolved in 100%, 50% and 40% of the patients, respectively.2
Pre/postopdyspareunia
Inourstudy,fromall18patientswhohadsexualfunctionafter thesurgery,dyspareuniawascompletelyresolvedin9ofthem (50%).Thisparameterwasdecreasedfromthemeanof5to0.8 aftertherepairsurgery.
InSpanos’sstudyon4patients,onepatientsufferedfrom dyspareunia afterthe repairsurgery.5 InVenkatesh’s study
on44patients,27%ofthemstillsufferedfromdyspareunia.4
InAbcarian’sstudyon43patients,dyspareuniawasresolved
Table3–p-Valueofeachvariable.
Variable p-Value
Pre-andpost-opFI <0.05
Pre-andpost-opQoL <0.05
Pre-andpost-opdyspareunia <0.05
Pre-andpost-opsexualfunctionsatisfaction <0.05
in15%ofthem.1 InHollinshead’sstudyon29patients,
dys-pareuniawasresolvedin9patients.2InValente’sstudy,this
parameterwasresolvedinall4patientswhowereunderwent thestudy.8
Pre/postopsexualfunctionsatisfaction
Inourstudy,thesexualfunctionsatisfactionwasimproved fromthemeanscoreof0.2to4.7.
Hollingshead reported the improvementofsexual func-tion satisfactionscorein9patients from29patientsinhis study.2Spanosreportedtheimprovementofsexualfunction
satisfactioninall4patientsofhisstudy.5
Pre/postopqualityoflife
Inourstudy,thequalityoflifescorewasincreasedfromthe meanof45to95.
InValenete’sstudyon4patients,thequalityoflifeinall patientswassignificantlyimproved.8 InAltomar’sstudy on
onepatientwith20-yrsfollow-upplan,therewasreporteda significantimprovementinqualityoflife.10
Post-opcomplications
Wereportedcomplicationsin3patientsincludewound infec-tion intwo patients (10%) and recto/vaginal fistulain one patient(5%).All3patientswerecuredbyconservative treat-ment.
InHarjeet’sstudy,woundinfection wasreportedinall4 patients.7InKaiser’sstudyon12patients,therewasreported
therecto/vaginalfistulain5patients.3InSpanos’sstudyon
4 patients, there was no complication reported.5
Holling-sheadreportedtherecto/vaginalfistulain3patients(10%)and woundinfectionin4patients(14%)ofall29patients.2
Conclusion
Wehavestudied19 patientswhowerereferredtothe hos-pital with symptoms of TCD between 2011 and 2015 at 3-monthsto4-yrswiththemeanof2.6-yrsfollow-up.They allunderwentsphincteroplastyandperineoplastywithskin advancementflap.Accordingtothesignificantimprovements ofFIscore,dyspareunia,sexualfunctionsatisfactionand qual-ityoflifeandalsominimalcomplicationsinallpatientsofour study,thistechniqueisrecommendedasaneffectivesurgical methodtotreattheTCDinsuchpatients.Forpatientswith successfulsurgicalrepairofTCD,Caesarseansectionseems reasonableforthenextdelivery.
Insuchthesecases,consultingwithacolorectalsurgeon mayimprovequalityoflifeofthepatients.
Conflicts
of
interest
Acknowledgements
ThisarticlehasbeenextractedfromthethesiswrittenbyDr. OmidEtemadinSchoolofMedicineShahidBeheshti Univer-sityofMedicalSciences(RegistrationNo.:467).
Appendix
A.
Supplementary
data
Supplementarydataassociatedwiththisarticlecanbefound, intheonlineversion,atdoi:10.1016/j.jcol.2016.08.002.
r
e
f
e
r
e
n
c
e
s
1. AbcarianH,OrsayCP,PearlRK,NelsonRichardL,BrileySusan
C.Traumaticcloaca.DisColonRectum.1989;32:783–7.
2. HollingsheadJRF,WarusavitarneJ,VaizeyCJ,NorthoverJMA.
Outcomesfollowingrepairoftraumaticcloacaldeformities.
BrJSurg.2009;96:1082–5.
3.KaiserAM.Cloaca-likedeformitywithfecalincontinence
aftersevereobstetricinjury-techniqueandfunctional
outcomeofano-vaginalandperinealreconstructionwith
X-flapsandsphincteroplasty.ColorectalDis.2008;10:827–32.
4.VenkateshKS,RamanujamP.Surgicaltreatmentoftraumatic
cloaca.DisColonRectum.1996;39:811–6.
5.SpanosCP,MikosT,KastaniasE.Surgicaltreatmentof
traumaticcloaca.ArchGynecolObstet.2012;286:815–8.
6.KiffES,SwashM.Slowed,“conductioninthepudendalnerves
inidiopathic(neurogenic)fecalincontinence”.BrJSurg.
1984;71:614–6.
7.NarulaHS,WadhawanH,ShorthouseAJ,BrownSR.Traumatic
cloacaldefect,theWarrenflaprevisitedadescriptionofthe
technique.PolishJournalofSurgery.2010:687–93.
8.ValenteMA,KhandujaKS.Layeredsurgicalrepairof
traumaticcloacaldeformities:technicaldetailsand
functionaloutcomes.Springer;2011.p.153–6.
9.DraganicB,SolomonMJ.Islandflapperineoplastyfor
coverageofperinealskindefectsafterrepairofcloacal
deformity.ANZJSurg.2001;71:487–90.
10.AltomareDF,RinaldiM,BucariaV,MarinoF,LobascioP,
SallustioPL.Overlappingsphincteroplastyandmodifiedlotus
petalflapfordelayedrepairoftraumaticcloaca.Tech