w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Genetics
of
rheumatoid
arthritis:
a
new
boost
is
needed
in
Latin
American
populations
Patricia
Castro-Santos
a,
Roberto
Díaz-Pe ˜na
a,b,∗ aFacultaddeCienciasdelaSalud,UniversidadAutónomadeChile,Talca,ChilebDepartmentofImmunology,HospitalUniversitarioCentraldeAsturias,Oviedo,Spain
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27January2015 Accepted30August2015
Availableonline19November2015
Keywords:
Rheumatoidarthritis HLA
Genomewideassociationstudies Geneticsusceptibility
Singlenucleotidepolymorphism
a
b
s
t
r
a
c
t
Rheumatoidarthritis(RA)isanautoimmuneinflammatoryrheumaticdiseasewhichaffects severalorgansandtissue,predominantlythesynovialjoints.Likemanyotherautoimmune diseases,RAisacomplexdisease,wheregeneticvariants,environmentalfactorsand ran-domeventsinteracttotriggerpathologicalpathways.GeneticimplicationinRAisevident, andrecentadvanceshaveexpandedourknowledgeaboutthegeneticfactorsthatcontribute toRA.Anexponentialincrementinthenumberofgenesassociatedwiththediseasehas beendescribed,mainlythroughgenewidescreenstudies(GWAS)involvinginternational consortiawithlargepatientcohorts.However,thereareafewstudiesonLatinAmerican populations.ThisarticledescribeswhatisknownabouttheRAgenetics,thefuturethatis emerging,andhowthiswilldevelopamorepersonalizedapproachforthetreatmentofthe disease.LatinAmericanRApatientscannotbeexcludedfromthisfinalaim,andahigher collaborationwiththeinternationalconsortiamaybeneededforabetterknowledgeofthe geneticprofileofpatientsfromthisorigin.
©2015ElsevierEditoraLtda.Allrightsreserved.
Genética
da
artrite
reumatoide:
é
necessário
um
novo
impulso
em
populac¸ões
latino-americanas
Palavras-chave:
Artritereumatoide HLA
Estudodeassociac¸ãogenômica ampla
Susceptibilidadegenética
Polimorfismodenucleotídeoúnico
r
e
s
u
m
o
A artrite reumatoide (AR)é uma doenc¸a reumática inflamatória autoimune queafeta váriosórgãosetecidos,predominantementeasarticulac¸õessinoviais.Comomuitas out-rasdoenc¸asautoimunes,aARéumadoenc¸acomplexa,emquevariantesgenéticas,fatores ambientaiseeventosaleatóriosinteragemedesencadeiamviaspatológicas.Aimplicac¸ão genéticanaARéevidenteeavanc¸osrecentestêmexpandidonossoconhecimentosobre osfatoresgenéticosquecontribuemparaadoenc¸a.Houveum incrementoexponencial na quantidadedegenes associadosà doenc¸adescritos,principalmentepor estudosde associac¸ãogenômicaampla(GWAS)queenvolveramconsórciosinternacionaiscomgrandes
∗ Correspondingauthor.
E-mail:[email protected](R.Díaz-Pe ˜na).
http://dx.doi.org/10.1016/j.rbre.2015.10.004
issovaidesenvolverumaabordagemmaispersonalizadaparaotratamentodadoenc¸a.Os pacienteslatino-americanoscomARnãopodemserexcluídosdesseobjetivofinalepode sernecessáriaumamaiorcolaborac¸ãocomosconsórciosinternacionaisparaseobterum melhorconhecimentodoperfilgenéticodospacientesprovenientesdessaregião.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Rheumatoid
arthritis
Rheumatoidarthritis (RA)is anautoimmune inflammatory rheumatic disease that affects many tissues and organs, mainly synovial joints. This disease leads to progressive destructionofarticularcartilageandankylosisofthejoints.1
Subsequent, pannus formation may lead to destruction of underlyingcartilageandbonyerosions.RAdiagnosisisbased on clinical criteria and laboratory tests.2 Anti-citrullinated
proteinautoantibodies(ACPA)showahighspecificityforRA, evenACPAtestinghasbecomeasubstantialcomponentofthe currentAmerican CollegeofRheumatology(ACR)-European LeagueAgainstRheumatism(EULAR)classificationcriteriafor RA.3Additionally,ithasbeendescribedthatACPAmayplaya
roleindiseasepathogenesis.4
RAaffectsapproximately1%ofthepopulationworldwide.5
Inthelastyears,severalepidemiologicalstudiesofRAhave been published, showing variations in the incidence and prevalenceofRAacrosspopulations.Mostofthestudieshave beendevelopedincountriesfromtheNorthEuropeandNorth America,estimatingprevalencesof0.5–1.1%.5Another
stud-iesmademainlyincountriesfromSouthEuropereporteda lowerprevalencearound0.3–0.7%.6–8 Thelowestprevalence
datahavebeenreportedinareasfromAfricaandAsia,andthe highestinNativeAmericanpopulations.5Infact,the
preva-lence ofRA is10 times higher among Canadianor Native Americans than Europeans (3% and 0.3%, respectively).9,10
Although the disease can develop at any age, RA affects females more frequently than males and it is diagnosed mainlyinage40–60years,althoughthemechanismbywhich genderinfluencesthesusceptibilitytoRAremains unclear. OthercharacteristicofRAisheterogeneity:patientsdonot formahomogenous population and someclinical RA sub-groups,suchasACPAseropositiveversusseronegative,erosive versusnon-erosive,progressiveversusmild-course,havebeen identified.11–13
RA
genetics
and
pathogenesis
Like many autoimmune diseases, the etiology of RA is multifactorial. Genetic susceptibility is evident in familial clusteringand monozygotictwinstudies,witha50%ofRA risk attributable to genetic factors, and heritability of RA has been estimated to be about 60%.4 Moreover, disease
progression, outcome and RA phenotype have been asso-ciatedwith genetic factors.11,14,15 Thus, understanding the
geneticsbasisofRAisrequiredinorder todevelopamore
personalizedapproachforthediseasetreatment.RAgenetic risk factors can be classified into two groups: (1) major histocompatibility complex (MHC) genes and (2) non-MHC regions. Interestingly,HLA and somenon-HLA genes have been linked to the development of antibodies against cit-rullinatedproteins,differentiatingbetweentwoentitieswith distinctive characteristics,ACPA seropositiveand seronega-tiveRA.16Interestingly,severalgeneticpolymorphismshave
been described associated to environmental factors in RA patients, primarilysmoking.17 Smoking and possibly other
environmentalfactorsmaytriggerACPAproductionandthe developmentofACPA seropositiveRA(Fig.1).11,16 Although
theetiologyofRAhasnotbeenelucidatedyet,theirsymptoms developgraduallyindifferentphases.18Inthisdevelopmentof
thediseasehasbeendescribeda“preclinicalphase”,inwhich severalimmunologicalmarkers,asACPAorrheumatoidfactor (RF),becomepositivesometimesyearsbeforeoftheonsetof clinicalsymptoms.Tosumup,RAdevelopsingenetically pre-disposedindividualssubjectedtoanunclearsetoflifeevents, speciallysmoking(Fig.1).
HLAregion
ThegenomicmapofthehumanMHC(HLA)spansabout7.6Mb and contains approximately 421 gene locion acontiguous regiononchromosome6.19TheclassicalHLAloci,whichplay
acentralroleintheimmunesystem,arecalled-A,-B,and-C (classI)and-DRB1,-DQB1,and-DPB1(classII).Particularly, the HLAclassIand classIIgenesencodeforproteinsthat bindtosmallantigenpeptidesandcarrythemintothecell surfacethuspresentingthemtotheimmunesystem. There-fore,thisgenomicregioniscrucialfortheorganismresistance andsusceptibilitytopathogenicfactors.
Ithasbeen35yearssinceitwaspublishedthattheHLA regioncontributestoRAsusceptibility,specificallyHLA-DR4 allele,20buttheexactmechanismthatdeterminesthe
predis-positionisunknown.AmongtheHLAgenes,theHLA-DRB1 sharedepitope(SE)allelesthatencodeforacommonamino acidsequence,isthemostimportantriskfactordescribedfor RAsusceptibilityandprogression.21ThepresenceofSE
sug-gestthattheHLAallelescontainingitbindthesameantigen, postulatingthepresentationofarthritogenicself-peptidesor molecular mimicry withforeign antigens,22,23 and/or
shap-ing the T-cell-antigenrepertoire.24 HLA-DRB1SE alleles are
APC cell (HLA-DR)
T cell
B cell
ACPA-positive
Immune response
Genetic and epigenetic risk
Asymptomatic autoimmunity and inflammation
Symptoms of autoimmunity and inflammation (undetectable by physical examination)
Undifferentiated synovitis
Clasical RA
Evolution of chronic Autoimmunity and inflammation
Perpetuation of the immflamation
“Preclinical” RA
RA evolution
T cell B cell
Fc Receptors
Synovial macrophages
Fig.1–HypotheticalmodelforinitiationofRAinACPA-positiveindividuals.Inaninductionphase,environmentalfactors couldcontributetostimulatetheinnateimmunity.Apoptosis,necrosis,orbothofsomecellscouldcausecitrullinationin certainproteinsinthelungs(duetotheincreaseintheactivityofpeptidylargininedeiminasesenzymes,PAD).Someof thesemodifiedproteinsbindspecificallytoHLA-DRmoleculesondendriticcellsormacrophagesresultinginhightitersof ACPA.Citrullinationproteinsinthejointsduetoinfection,trauma,exercise,etc.,couldleadtoimmunecomplexformation betweenmodifiedproteinsandACPA,whichfurtherbindtoFcreceptorsonthesurfaceofsynovialmacrophages,
contributingtotheperpetuationofinflammation.
andACPAinthepathogenesisofRAhasbeenexplainedby cit-rullinatedpeptidebindingintothepocketofDRB1molecules containingthe shared epitope,and the consequent activa-tion of CD4+ T cells and polarization to Th17 cells, a Th
subpopulationinvolvedprimarilyinautoimmuneprocesses.16
HLA-DRB1 SE alleles are present in64–70% ofRA patients and in 55% of their first-degree relatives; this frequency is significantly higher to the one observed in control
Worldwide
PTPN22 CTLA4 PAD14
STAT4 TNFAIP3 TRAF1/C5
IL2/IL21
CD40 IL2RA IL2RB TNFRSF14
PRKCQ AFF3
1987
Candidate genes and SNP genotyping
GWAS studies GWAS studies and meta-analysis High density SNP genotyping and
meta-analysis
High density SNP genotyping
2003-2005 2007 2008-2011 2012
ENOX1 NNA25 and moderate RA associations
with loci previously reported: PTPN22, STAT4, IRF5, CCL21, SPRED2, IL2RA
2013
Latin America
populations
HLA
“shared eptitope”
hypothesis
REL TAGAP
CD28 TRAF6 PTPRC CD2/CD58
CCR6 IRF5 SPREAD2 ANKRD55 IL6ST
GIN1
TYK2 IL6R RUNX1 GATA3 IRF8 ARID5B
IRAK1 PTPN2 B3GNT2
Caucasian and Asia
n
populations
haveSE.Thisinteractionamonggeneticriskfactorsandthe presenceofautoantibodiesincreasetheriskofdevelopingRA infirst-degreerelativesofRApatients.27,28
The SE hypothesis remains controversial, because sug-gest the existence of an autoantigenic peptide that has not identified yet. Several other diseases, like Type I dia-betes,psoriaticarthritis,lupus,early-onsetchroniclymphoid leukemia,and otherconditions,29 andthis promiscuity are
incongruous with tenets of MHC-restricted antigen pre-sentation theory. Although HLA-DRB1 alleles containing the epitope are established genetic risk factors in RA, the precise immunological implications of their expres-sion are not clear. Furthermore,it has been reported that sharedepitope alleles atthe HLA-DRB1locus donot com-pletelyexplaintheassociation ofthe MHCregionwiththe disease.30–32
Non-HLAgeneticassociations
ThepathogenesisofRAhasapolygenicbasis.About50%of RArisk isthoughtto begeneticand one-third of this risk belongs to the HLA locus.4 Thus, genetic variation can be
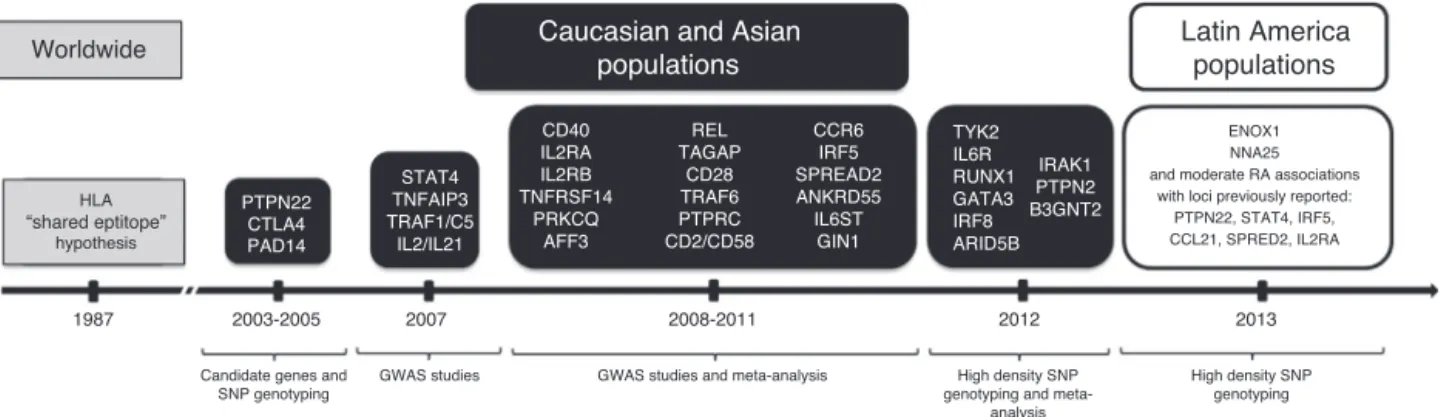
explainedbyRAriskallelesinnon-HLAlocus.Therehasbeen anexponentialincreaseinthe numberofgenesassociated withRAinthelastseveralyears,asshowninFig.2. Specifi-cally,inadditiontotheHLA-DRBlocus,over46non-HLARA risklocihaveemergedfromgenome-wideassociation stud-ies (GWAS) and subsequent GWASmeta-analysis ofGWAS datasets,33,34 all oftheminindividuals ofEuropean
ances-try.Anothermeta-analysisofGWASinJapanesepopulation wasreported,whichidentifiedninenovellociassociatedwith RA.35Thecitedstudyprovidedevidenceofsignificant
over-lapintheRAgeneticrisksbetweenJapaneseandEuropean population,contributingtofurtherunderstandingoftheRA etiology.GWASareconsideredtobeoneoftheprimarytools for determining genetic links to diseases. These analyses havebeenabundantinrecentscientificresearches.Ineach ofthesestudies atleast100,000singlenucleotide polymor-phisms (SNPs) are genotyped, taking an unbiased view of the wholegenome andtherefore havea higherprobability ofdetecting an association witha genetic marker, provid-ingthestudieswithsufficientpower.Fig.2capturesthetop regionsofRAassociationsthatarestatisticallysignificant.A recentstudydiscovered42novelRArisklociatagenome-wide levelofsignificance,bringingthetotalto101.36Thesestudy
genotypedaround10millionSNPsonatotalofover100,000 subjectsofEuropeanandAsianancestry,29,880RApatients and73,758controls.Insummary,theresearcherswereable toestablish98genesthatcouldpotentiallycontributetothe onset ofRA. Manyofthese genesalsoplayarole inother diseases,including humanprimary immunodeficiency dis-ordersandbloodcancers.Theydiscoveredmanygenesthat overlaptocontributetotheconditionthatarealreadybeing targetedbyexistingdrugs,butwasnotknownwhenthedrugs weredeveloped.Thisstudyprovidesevidencesthatgenetic ofdiseases could contribute to biological insightand drug discovery.
ThestudyofgeneticsinLatinAmerican populationsisnot a trivial topic. The expressionof genetic variants is mod-ified by many environmental factors, and the significance of ethnicity in geneticsis controversial.37 Latin Americans
have been wrongly designated as “Hispanics” and consid-eredhomogenous.Actually,theorigins anddestinationsof non-Amerindianpopulationshavedependedonthetimeand reasonsforthemigration,andthedegreeofadmixturevaries between Latin American countries according to the major ancestrypopulationcomponent.38
There are importantchallenges in finding susceptibility genesforRAinthesepopulations.TheHispaniccommunityis anadmixedpopulation,andtheallelicfrequencydifferences across ethnicgroups caninterferewithassociation studies andleadtofalse-positiveresults.Thus,inGWAS,candidate genesandreplicationstudiesofGWAS,differencesfoundin theallelefrequenciesmaybeoriginatedmorebydifferences in thepopulations structurethan bythe phenotype ofthe disease. However, thereare approaches to overcoming the problemofpopulationstructure,like touseancestry infor-mative markers(AIMs),39 or include structured association
test(structure)andprincipalcomponentanalysisforadjusting populationstratificationsinthestudies.40,41
Althoughahighprogresshasbeenmadeindetectingthe genes implicatedinRAsusceptibility,little isknown about genetic susceptibility in the “Hispanic” populations of the Americas. This is largely due to the difficulty of perform-ingassociationstudiesinadmixedpopulationsandthefact that the power requiredto identifygeneticassociations in thesepopulationsisgreaterthaninmorehomogeneous popu-lations. SomeARassociation studies havebeen previously reportedinAmerindianandmixedHispanicpopulations,and the strongestassociation observed wasin theHLA classII region.Specifically,geneticassociationsofRAwithHLA-DRB1 alleles have been reported in Native Americans, Mexican American ancestry, Colombianpopulation, Chilean popula-tion,Peruvianpopulation,BrazilianpopulationandMexican Mestizo population with a larger proportion of European ancestry.42–48Ameta-analysiscarriedoutacrossLatin
Ameri-canpopulationsestimatedtherelevanceofHLA-DRB1alleles on RA susceptibility, confirming a significant association betweenRAandHLA-DRB1geneandrevalidatingtheshared epitopehypothesisinLatinAmericanpopulations.49Arecent
studyexaminedsusceptibilitylociforRAinLatinAmerican individualswithadmixedEuropeanandAmerindiangenetic ancestry.50Thesestudygenotyped196.524markers,covering
thepreviouslyassociatedlociwithvariousautoimmune dis-eases,in1.475RApatientsand1.213controls.Astronggenetic association ofRAwiththe MHCregion wasobserved,with threeindependenteffects,probablyduetothediverseorigin ofthesamples.Inthesamestudy,50RAassociationspreviously
perspectives into the RAgenetic basis in Latin-Americans individuals.Severalofthesefindingsrequirereplicationand supplyanimpetusforfuturestudies.Moreover,theyprovide interestingconclusionsoftheobservedcomplexityofRA asso-ciationswithHLAregion,probablyasaconsequenceofthe origindiversity.
Genetic analyses undertaken in the recent years have revealedanewpictureforRApathogenesisandmadeusaware ofheterogeneityamongindividualsandpopulations.
Genomicsresearchisadvancingrapidly,throughSNP geno-typingandthenextgenomesequencing,twotechniquesthat areimproving ourunderstanding oftheRA etiopathogene-sis.Thefinalgoalinthecomingyearsistoidentifygenetic variantsinvolvedinthedifferentclinicalmanifestationsand RA-associatedfeatures,andtherebypredicttheevolutionof thedisease,and finally,toestablish newtreatmentsforRA basedontheprognosisofindividuals,enablingthe develop-mentofpersonalizedtherapiesforRA.Otheraspectssuchas epigeneticsandpharmacogenetics,51,52requirefurther
inves-tigationinordertoestablishanyroletheymayhaveinRA. Regardingthislastpoint,thefinalobjectiveof pharmacoge-neticsinrheumatologyistodefinegeneticallydistinctpatient subsets,whichhavedifferentialresponsestothevarious ther-apiesusedtotreatrheumaticdiseases.Avastgrowingbody ofliteraturedescribesthepharmacogeneticsofdrugsusedin RAtreatment.52–54However,therearenodataaboutRA
phar-macogeneticinLatin-Americanpopulations.
Variationsinthefrequencyofcertaingenotypesacross eth-nicgroups may occur,and dueto this,geneticassociation studiesconductedinLatinAmericanmusthaveapowerful “controlpopulation”.ThelargeanddiversepopulationofLatin America isa powerful resource forelucidating the genetic basisofcomplextraitsasRA.55
Conclusions
Multicentricstudieshaveshownahighrelevanceinthe under-standing of the risk genetic factors in complex diseases. Therefore, an additional effort in the search forunknown geneticpredispositionsandclarifydifferencesinrolesamong ethnic groups, including Latin American populations, is needed. Investigation ingenomics area hasadvanced very quicklythroughSNPsgenotypingandGWAS,andwilladvance evenmorewiththenewmassivesequencingtechniques.In thisway,abetterknowledgeaboutgeneticbasisofRAinLatin Americanpopulationsundoubtedlywouldcontributetoa bet-terunderstandingofthisdiseasepathology.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgment
ThisworkwassupportedbyFondecyt,grantno.11130198.
r
e
f
e
r
e
n
c
e
s
1.LeeDM,WeinblattME.Rheumatoidarthritis.Lancet. 2001;358:903–11.
2.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
3.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham CO3rd,etal.Rheumatoidarthritisclassificationcriteria:an AmericanCollegeofRheumatology/EuropeanLeagueAgainst Rheumatismcollaborativeinitiative.AnnRheumDis. 2010;69:1580–8.
4.MacGregorAJ,SniederH,RigbyAS,KoskenvuoM,KaprioJ, AhoK,etal.Characterizingthequantitativegenetic contributiontorheumatoidarthritisusingdatafromtwins. ArthritisRheum.2000;43:30–7.
5.TobónGJ,YouinouP,SarauxA.Theenvironment, geo-epidemiology,andautoimmunedisease:rheumatoid arthritis.JAutoimmun.2010;35:10–4.
6.CarmonaL,VillaverdeV,Hernández-GarcíaC,BallinaJ, GabrielR,LaffonA,etal.Theprevalenceofrheumatoid arthritisinthegeneralpopulationofSpain.Rheumatology (Oxford).2002;41:88–95.
7.GuilleminF,SarauxA,GuggenbuhlP,RouxCH,FardelloneP, LeBihanE,etal.PrevalenceofrheumatoidarthritisinFrance: 2001.AnnRheumDis.2005;64:1427–30.
8.AndrianakosA,TrontzasP,ChristoyannisF,KaskaniE,Nikolia Z,TavaniotouE,etal.Prevalenceandmanagementof rheumatoidarthritisinthegeneralpopulationofGreece–the ESORDIGstudy.Rheumatology(Oxford).2006;45:1549–54.
9.MolokhiaM,McKeigueP.Riskforrheumaticdiseasein relationtoethnicityandadmixture.ArthritisRes. 2000;2:115–25.
10.El-GabalawyHS,RobinsonDB,DahaNA,OenKG,SmolikI, EliasB,etal.Non-HLAgenesmodulatetheriskofrheumatoid arthritisassociatedwithHLA-DRB1inasusceptibleNorth AmericanNativepopulation.GenesImmun.2011: 568–74.
11.SzodorayP,SzabóZ,KapitányA,GyetvaiA,LakosG,SzántóS, etal.Anti-citrullinatedprotein/peptideautoantibodiesin associationwithgeneticandenvironmentalfactorsas indicatorsofdiseaseoutcomeinrheumatoidarthritis. AutoimmunRev.2010;9:140–3.
12.DahaNA,ToesRE.Rheumatoidarthritis:areACPA-positive andACPA-negativeRAthesamedisease?NatRevRheumatol. 2011;7:202–3.
13.LakiJ,LundströmE,SnirO,RönnelidJ,GanjiI,CatrinaAI, etal.Veryhighlevelsofanti-citrullinatedproteinantibodies areassociatedwithHLA-DRB1*15non-sharedepitopeallele inpatientswithrheumatoidarthritis.ArthritisRheum. 2012;64:2078–84.
14.vanderHelm-vanMilAH,WesolyJZ,HuizingaTW. Understandingthegeneticcontributiontorheumatoid arthritis.CurrOpinRheumatol.2005;17:299–304.
15.vanderHelm-vanMilAH,ToesRE,HuizingaTW.Genetic variantsinthepredictionofrheumatoidarthritis.Ann RheumDis.2010;69:1694–6.
16.ArendWP,FiresteinGS.Pre-rheumatoidarthritis: predispositionandtransitiontoclinicalsynovitis.NatRev Rheumatol.2012;8:573–86.
17.PadyukovL,SilvaC,StoltP,AlfredssonL,KlareskogL.A gene–environmentinteractionbetweensmokingandshared epitopegenesinHLA-DRprovidesahighriskofseropositive rheumatoidarthritis.ArthritisRheum.2004;50:3085–92.
NatRevGenet.2004;5:889–99.
20.StastnyP.AssociationoftheB-cellalloantigenDRw4with rheumatoidarthritis.NEnglJMed.1978;298:869–71.
21.GregersenPK,SilverJ,WinchesterRJ.Thesharedepitope hypothesis.Anapproachtounderstandingthemolecular geneticsofsusceptibilitytorheumatoidarthritis.Arthritis Rheum.1987;30:1205–13.
22.WucherpfennigKW,StromingerJL.Selectivebindingofself peptidestodisease-associatedmajorhistocompatibility complex(MHC)molecules:amechanismforMHC-linked susceptibilitytohumanautoimmunediseases.JExpMed. 1995;181:1597–601.
23.LaCavaA,NelsonJL,OllierWE,MacGregorA,KeystoneEC, ThorneJC,etal.Geneticbiasinimmuneresponsestoa cassettesharedbydifferentmicroorganismsinpatientswith rheumatoidarthritis.JClinInvest.1997;100:658–63.
24.BhayaniHR,HedrickSM.Theroleofpolymorphicamino acidsoftheMHCmoleculeintheselectionoftheTcell repertoire.JImmunol.1991;146:1093–8.
25.vanderWoudeD,Houwing-DuistermaatJJ,ToesRE,Huizinga TW,ThomsonW,WorthingtonJ,etal.Quantitative
heritabilityofanti-citrullinatedproteinantibody-positiveand anti-citrullinatedproteinantibody-negativerheumatoid arthritis.ArthritisRheum.2009;60:916–23.
26.ÄrlestigL,MullazehiM,KokkonenH,RocklövJ,RönnelidJ, DahlqvistSR.Antibodiesagainstcycliccitrullinatedpeptides ofIgG,IgAandIgMisotypeandrheumatoidfactorofIgMand IgAisotypeareincreasedinunaffectedmembersofmulticase rheumatoidarthritisfamiliesfromnorthernSweden.Ann RheumDis.2012;71:825–9.
27.KolfenbachJR,DeaneKD,DerberLA,O’DonnellC,Weisman MH,BucknerJH,etal.Aprospectiveapproachtoinvestigating thenaturalhistoryofpreclinicalrheumatoidarthritis(RA) usingfirst-degreerelativesofprobandswithRA.Arthritis Rheum.2009;61:1735–42.
28.vanVenrooijWJ,vanBeersJJ,PruijnGJ.Anti-CCPantibodies: thepast,thepresentandthefuture.NatRevRheumatol. 2011;7:391–8.
29.deAlmeidaDE,LingS,HoloshitzJ.Newinsightsintothe functionalroleoftherheumatoidarthritissharedepitope. FEBSLett.2011;585:3619–26.
30.DingB,PadyukovL,LundströmE,SeielstadM,PlengeRM, OksenbergJR,etal.Differentpatternsofassociationswith anti-citrullinatedproteinantibody-positiveand
anti-citrullinatedproteinantibody-negativerheumatoid arthritisintheextendedmajorhistocompatibilitycomplex region.ArthritisRheum.2009;60:30–8.
31.LeeHS,LeeAT,CriswellLA,SeldinMF,AmosCI,CarulliJP, etal.Severalregionsinthemajorhistocompatibilitycomplex conferriskforanti-CCP-antibodypositiverheumatoid arthritis,independentoftheDRB1locus.MolMed. 2008;14:293–300.
32.VignalC,BansalAT,BaldingDJ,BinksMH,DicksonMC, MontgomeryDS,etal.ArthritisRheum.2009;60:53–62.
33.StahlEA,RaychaudhuriS,RemmersEF,XieG,EyreS, ThomsonBP,etal.Genome-wideassociationstudy
meta-analysisidentifiessevennewrheumatoidarthritisrisk loci.NatGenet.2010;42:508–14.
34.EyreS,BowesJ,DiogoD,LeeA,BartonA,MartinP,etal. High-densitygeneticmappingidentifiesnewsusceptibility lociforrheumatoidarthritis.NatGenet.2012;44:1336–40.
35.OkadaY,TeraoC,IkariK,KochiY,OhmuraK,SuzukiA,etal. Meta-analysisidentifiesninenewlociassociatedwith rheumatoidarthritisintheJapanesepopulation.NatGenet. 2012;44:511–6.
drugdiscovery.Nature.2014;506:376–81.
37.CaulfieldT,FullertonSM,Ali-KhanSE,ArbourL, BurchardEG,CooperRS,etal.Raceandancestryin
biomedicalresearch:exploringthechallenges.GenomeMed. 2009;1:8.
38.SansM.AdmixturestudiesinLatinAmerica:fromthe20thto the21stcentury.HumBiol.2000;72:155–77.
39.YangN,LiH,CriswellLA,GregersenPK,Alarcon-Riquelme ME,KittlesR,etal.Examinationofancestryandethnic affiliationusinghighlyinformativediallelicDNAmarkers: applicationtodiverseandadmixedpopulationsand implicationsforclinicalepidemiologyandforensicmedicine. HumGenet.2005;118:382–92.
40.SattenGA,FlandersWD,YangQ.Accountingforunmeasured populationsubstructureincase-controlstudiesofgenetic associationusinganovellatent-classmodel.AmJHum Genet.2001;68:466–77.
41.PriceAL,PattersonNJ,PlengeRM,WeinblattME,ShadickNA, ReichD.Principalcomponentsanalysiscorrectsfor
stratificationingenome-wideassociationstudies.NatGenet. 2006;38:904–9.
42.delRincónI,EscalanteA.HLA-DRB1allelesassociatedwith susceptibilityorresistancetorheumatoidarthritis,articular deformities,anddisabilityinMexicanAmericans.Arthritis Rheum.1999;42:1329–38.
43.El-GabalawyHS,RobinsonDB,HartD,EliasB,MarklandJ, PeschkenCA,etal.Immunogeneticrisksofanti-cyclical citrullinatedpeptideantibodiesinaNorthAmericanNative populationwithrheumatoidarthritisandtheirfirst-degree relatives.JRheumatol.2009;36:1130–5.
44.AnayaJM,CorreaPA,MantillaRD,Arcos-BurgosM.
RheumatoidarthritisassociationinColombianpopulationis restrictedtoHLA-DRB1*04QRRAAalleles.GenesImmun. 2002;3:56–8.
45.GonzálezA,NicovaniS,MassardoL,AguirreV,CervillaV, LanchburyJS,etal.InfluenceoftheHLA-DRbetashared epitopeonsusceptibilitytoandclinicalexpressionof rheumatoidarthritisinChileanpatients.AnnRheumDis. 1997;56:191–3.
46.CastroF,AcevedoE,CiusaniE,AnguloJA,WollheimFA, Sandberg-WollheimM.Tumournecrosisfactor
microsatellitesandHLA-DRB1*,HLA-DQA1*,andHLA-DQB1* allelesinPeruvianpatientswithrheumatoidarthritis.Ann RheumDis.2001;60:791–5.
47.UsnayoMJ,AndradeLE,AlarconRT,OliveiraJC,SilvaGM, BendetI,etal.StudyofthefrequencyofHLA-DRB1allelesin Brazilianpatientswithrheumatoidarthritis.RevBras Reumatol.2011;51:474–83.
48.Ruiz-MoralesJA,Vargas-AlarcónG,Flores-VillanuevaPO, Villarreal-GarzaC,Hernández-PachecoG,Yamamoto-Furusho JK,etal.HLA-DRB1allelesencodingthesharedepitopeare associatedwithsusceptibilitytodevelopingrheumatoid arthritiswhereasHLA-DRB1allelesencodinganasparticacid atposition70ofthebeta-chainareprotectiveinMexican Mestizos.HumImmunol.2004;65:262–9.
49.Delgado-VegaAM,AnayaJM.Meta-analysisofHLA-DRB1 polymorphisminLatinAmericanpatientswithrheumatoid arthritis.AutoimmunRev.2007;6:402–8.
50.LópezHerráezD,Martínez-BuenoM,RibaL,GarcíadelaTorre I,SacnúnM,Go ˜niM,etal.RheumatoidarthritisinLatin AmericansenrichedforAmerindianancestryisassociated withlociinchromosomes1,12,and13,andtheHLAclassII region.ArthritisRheum.2013;65:1457–67.
52.DavilaL,RanganathanP.Pharmacogenetics:implicationsfor therapyinrheumaticdiseases.NatRevRheumatol.
2011;7:537–50.
53.Umi˙cevi˙c MirkovM,CuiJ,VermeulenSH,StahlEA,ToonenEJ, MakkinjeRR,etal.Genome-wideassociationanalysisof anti-TNFdrugresponseinpatientswithrheumatoidarthritis. AnnRheumDis.2013;72:1375–81.
54.PlantD,BowesJ,PotterC,HyrichKL,MorganAW,WilsonAG, etal.Genome-wideassociationstudyofgeneticpredictorsof
anti-tumornecrosisfactortreatmentefficacyinrheumatoid arthritisidentifiesassociationswithpolymorphismsatseven loci.ArthritisRheum.2011;63:645–53.