r e v b r a s r e u m a t o l . 2017;57(5):491–494
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Brief
communication
Rheumatoid
arthritis
in
elderly
and
young
patients
Artrite
reumatoide
do
idoso
e
do
jovem
Ariane
Carla
Horiuchi,
Luiz
Henrique
Cardoso
Pereira,
Bárbara
Stadler
Kahlow,
Marilia
Barreto
Silva,
Thelma
L.
Skare
∗HospitalUniversitárioEvangélicodeCuritiba,Servic¸odeReumatologia,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16January2014
Accepted24June2015
Availableonline27October2015
Introduction
There isa wide variabilityin the formsofpresentation of
rheumatoid arthritis(RA). Theage ofonset ofthis disease
seems tobe acritical factor in its clinical spectrum.1 It is
considered thata patientsuffers elderly onset rheumatoid
arthritis(EORA) whenthe disease beganat theage of≥60
years.1,2ThisformofRAcontributeswith10–33%ofcasesof
disease.3
TheprevalenceofRAincreaseswithageandisestimated
tooccurinupto2.2%ofthepopulation>55years.4Thegenetic
influence,especiallyofHLAclass2genes,5,6 actsnotonlyin
theincidencerate,accordingtotheageofonset,4,7,8butalsoin
promotingtheappearanceofclinicalpeculiaritiesineachage
group.9Individualswithdiseaseonsetatayoungeragehavea
higherprevalenceofHLADRB1*04;inthosewithalateonset,
HLADRB1*01prevails.8 Onthe otherhand,elderlypatients
withtheseronegative,polymyalgia-likeformshowincreasing
prevalenceofHLADRB1*13/*14.10
In contrast to the disease beginning in young
individ-uals(youngonsetrheumatoidarthritis,orYORA),EORAseem
tofollowamoreacutecourse,inassociationwithsystemic
∗
Correspondingauthor.
E-mail:[email protected](T.L.Skare).
phenomenasuchasfever,fatigueandweightloss,aswellas
withtheinvolvementoflargerjointsandhigherprevalence
ofatypical formsofonsetasRS3PE (remittingseronegative
symmetricalsynovitiswithpittingedema)andpolymyalgia
rheumatica-like forms.1 However,the statement that, with
increasingage,theprognosisbecomesmoresevereoreven
thattherearedifferencesinthecourseofthediseaseforyoung
andelderlypeople,assomeauthorsclaim,1,4,5,11isa
contro-versialmatter,sincetheliteratureisnotunanimousonthis
point.5,8,11ABrazilianstudy couldnotdetectdifferencesin
prognosisforbothgroups.6
ThetreatmentofEORApatientspursuits thesame goals
asthose ofYORApatients, i.e.tocontroltheclinical
mani-festations,preventstructuraldamage,preservefunctionand
autonomyoftheindividual,andalsopreventexcess
mortal-itycausedbythedisease.1Butsomeauthorshaveobserved
thatthetreatmentofelderlypatientsiscarriedoutdifferently,
withlessaggressivenessopposedtothatforYORApatients.2,4
Thisfindingisjustifiedforthefearofprescribing
modifying-disease drugs in more vulnerable people, with greater
possibilityofdruginteractionduetomultipleco-morbidities
towhichtheelderlyindividualisusuallysubject.2,3
http://dx.doi.org/10.1016/j.rbre.2015.06.002
2255-5021/©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
492
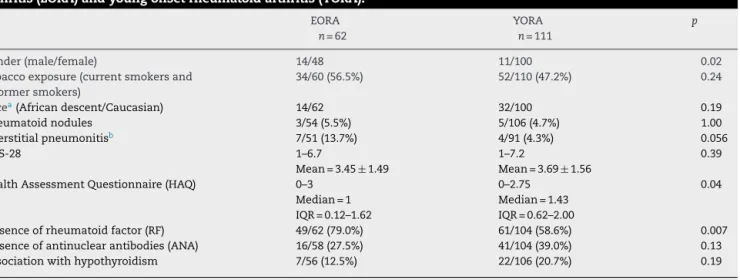
rev bras reumatol.2017;57(5):491–494Table1–Comparisonofdemographic,clinicalandserologicaldatabetweenpatientswithelderlyonsetrheumatoid arthritis(EORA)andyoungonsetrheumatoidarthritis(YORA).
EORA n=62
YORA n=111
p
Gender(male/female) 14/48 11/100 0.02
Tobaccoexposure(currentsmokersand formersmokers)
34/60(56.5%) 52/110(47.2%) 0.24
Racea(Africandescent/Caucasian) 14/62 32/100 0.19
Rheumatoidnodules 3/54(5.5%) 5/106(4.7%) 1.00
Interstitialpneumonitisb 7/51(13.7%) 4/91(4.3%) 0.056
DAS-28 1–6.7
Mean=3.45±1.49
1–7.2
Mean=3.69±1.56
0.39
HealthAssessmentQuestionnaire(HAQ) 0–3
Median=1 IQR=0.12–1.62
0–2.75 Median=1.43 IQR=0.62–2.00
0.04
Presenceofrheumatoidfactor(RF) 49/62(79.0%) 61/104(58.6%) 0.007
Presenceofantinuclearantibodies(ANA) 16/58(27.5%) 41/104(39.0%) 0.13
Associationwithhypothyroidism 7/56(12.5%) 22/106(20.7%) 0.19
a Accordingtothepatient’sself-declaration.
b Foundbyhigh-resolutionCTofthechest.
Withincreasinglongevity and growth ofthepopulation
over60years,itisimportanttorecognizethecharacteristics
ofthelocalpopulationwithEORAtoimprovethequalityof
healthcareofferedtothesepatients.Inthisstudy,wesought
toevaluatethedemographic,clinical,serologicaland
treat-mentprofilesofthelocalpopulationwithEORAcomparedto
patientswithYORA.
Patients
and
methods
This is a study approved by the Research Ethics
Commit-tee.RApatientswho met atleastfourofthe classification
criteriaoftheAmericanCollegeofRheumatology(1987)for
RA12 and being diagnosed with EORA1 who attended to a
singlerheumatologyoutpatientclinicofatertiarycare
cen-ter during the period of one year (August 2012 to August
2013)werestudied.Thisisanobservational,analytical,
cross-sectionalstudyofaconveniencesamplewherepatientswith
EORA(n=62) andwithYORA(n=111)properlymatchedfor
diseasedurationwerecompared.Dataaboutdemographics,
presenceofnodules,extra-articularmanifestationsofRA,the
presence of autoantibodies as rheumatoid factor (RF) and
antinuclear antibody (ANA), and use of medications were
obtainedretrospectively through a reviewof their medical
records.InflammatoryactivityindexessuchasDAS(Disease
ActivityScore)2813and offunctionalcapacitymeasuredby
HAQ(HealthAssessmentQuestionnaire)14wereobtained
dur-ingthestudyperiod.
Dataweregatheredinfrequencyandcontingencytables;
Chi-squaredandFischertestswere usedforcomparisonof
nominal data; and Mann–Whitney and non-paired t tests
wereappliedtonumericaldata.Thesampledistributionwas
studiedbyD’Agostinoand Persontest. Measuresofcentral
tendency were expressed as mean and standard deviation
for Gaussian variables; and as median and interquartile
range(IQR)fornon-Gaussianvariables.Resultswithp≤0.05
were considered statistically significant. The calculations
weremadewiththeaidoftheGraphPadPrism(version5.0)
software.
Results
At disease onset, YORA patients (n=111) were aged 32–58
(median=45,IQR=39.0–51.0)years;andEORApatients(n=62)
wereaged60–83(median=63.0,IQR=60.7–70.0)years.InEORA
group, the disease duration time was 1–16 (median=3.0;
IQR=1.0–6.5)years;andinYORAgroup,thediseaseduration
timewas1–13(median=5.0;IQR=2.0–8.0)years(p=0.21).In
Table1,onecanobservethecomparisonbetweenthesetwo
groupsregardingdemographic,serologicalandclinical
char-acteristics;itisworthnotingthedifferencefoundforgender,
HAQandRFbetweenthegroups.InEORAgrouptherewere
41.6%patientswithlowactivityorremissionbyDAS28(<3.2)
asopposedto38.7%inYORAgroup(p=0.85).Asregardsthe
useofmedications,nodifferencewasfoundbetweengroups,
ascanbeseeninTable2.
Discussion
TheresultsofthisstudydemonstratethatEORAinBrazilis
morecommoninmaleindividuals,andthatpatientswiththis
formofRAhavebetterHAQthatofpatientswithYORAwith
thesamediseaseduration.Thefindingthatmalesaremore
affectedinolderagegroupsisafactalreadywidelyrecognized
intheliterature.1,15 TheNorfolkArthritisRegister,11i.e. the
Englisharthritisregistry,showsthat theincidenceofRAin
mengraduallyincreaseswithage,whileinwomenitincreases
from45years,reachingaplateauat75years,fromwhichthe
incidencestartstodecline.Bajocchietal.16describedagender
distributionratioof1.5–2womento1manintheelderlyversus
4–4.5womenfor1maninyoungerpeople.
Itwasalsoobservedinthepresentstudythatthefunctional
statemeasuredbyHAQhadlowervaluesinelderly
individu-als.Thisfactisinterestingandisopposedtotheideathatolder
people, despitewhether or notsufferingfrom arheumatic
disease,mayshowfunctionalimpairmentrelatedtothe
weak-nessinherenttoolderpeople.Thiscanbeexplained,ifahigher
rev bras reumatol.2017;57(5):491–494
493
Table2–Comparisonoftreatmentsusedinpatientswithelderlyonsetrheumatoidarthritis(EORA)versusyoungonset rheumatoidarthritis(YORA).
EORA n=62
YORA n=111
p
Corticosteroiduse(numberofpatients) 48/62(77.4%) 85/103(82.5%) Doseofcorticosteroidmg/day(prednisoneor
equivalent)
2.5and20.0 Median=10.0 IQR=5.0–10.0
2.50–20.00 Median=5.0 IQR=5.0–10.0
0.17
Methotrexate 49/62(79.0%) 82/105(78.0%) 0.88
Antimalarials 32/62(51.6%) 44/105(41.0%) 0.22
Leflunomide 15/62(16.1%) 28/105(26.2%) 0.72
Anti-TNF␣ 4/62(6.4%) 6/104(5.7%) 1.00
thatpatientswithEORAhadabetterprognosisandachieved easierand faster remission. Onthe other hand, aSpanish study18 shows thatpatients withelderlyonset rheumatoid
arthritishaveworsefunctionalandanatomicalindexesversus
correspondingyoungersubjects.Data fromthisstudy favor
theconceptthatRAintheelderlyisnotamoreserious
condi-tionthaninyoungsubjects.However,Nazetal.19showedthat
olderageatthetimeofdiagnosisisassociatedwithincreased
cardiovascularmortality,suggestingtheneedforan
aggres-sivetreatmenttoavoidprematuredeath.
Tutuncu et al.7 investigating prescribing habits of 192
rheumatologists, describe that patients with EORA receive
less treatmentthan those with YORA,despite anidentical
durationofdiseaseandcomparableactivityandseverity.As
alreadymentioned,olderpeople havemoreco-morbidities,
areathigherriskofpolypharmacyandaresubjecttoahigher
prevalenceofsideeffectsbychanges indrug
pharmacody-namicsandpharmacokinetics.1,2 TherecognitionthatRAis
adisease withapoorprognosisandthatthecontrolofthe
inflammatoryprocessimpactsdecisivelyonfunctional
capac-ityandsurvivalofthepatient,mayhavebeenresponsiblefor
achangeofattitudetowardthisagegroupinrecentyears.In
thisstudy,wecouldnotdetectdifferencesintheuseofdrugs
inthetwodiseaseonsetranges,showingthatcurrentlythe
aggressivenessintreatmentdoesnotvaryaccordingtothe
ageofonset,andasimilarcontrolofinflammation,measured
byDAS28,wasobtainedinbothpopulations.
Thisstudyhassomelimitations.Duetotheretrospective
natureofthestudy,itwasnotpossibletoaccesscertain
infor-mation such as, for instance, the prevalence ofsecondary
Sjögrensyndromeinbothgroups.Interestingly,weobserved
alowertendencyforinvestigationofsuchkindofsymptoms
in the older age group. Itmay be that such fact occurred
byattributing the sicca symptoms to their own age, or to
the concomitant use ofother drugs, such asdiuretics and
antidepressants,commoninolderpeople.Anotherlimitation
isthefactthatonlyindividualswhoalreadyhavecompleted
fourACR (1987)classificationcriteriaforRAwere included.
Thischoicewasmadebecausethisisaretrospectivestudy;
thus,thequalityofinformationisdependentonthecorrect
completionofmedicalrecords.Itistherefore importantto
stressthattheabovefindingsareonlyvalidforthistypeof
patients.Subjectswithatypical formsofRA,suchasthose
with preferential involvement of large joints, polymyalgia
rheumatica-likeformsandRS3PEhavenotbeenstudied.On
theotherhand,thissameselectiveprocessallowedthe
inclu-sionofindividualswithamoreaccuratediagnosis,withthe
exclusionofotherdiseasesthat,intheelderly,maysimulate
RA,suchasmicrocrystallinediseases.Thestrategyusedfor
ourinclusioncriterionofpatientsmayalsohavebeen
respon-sibleforthehigherprevalenceofpositiveRFinEORAfoundin
thisstudy,sincemostauthorshavedescribedthisvariableas
beinglowerthanthatfoundinyoungsubjects.1,11Although
theliteraturementionsthathealthyelderlyarelikelytohave
ahigherprevalenceofRF,afactattributedsolelytoage,itis
interestingtonotethatthisfindingcouldnotbeprovenina
studyof336healthypatientsinourregion.20Therefore,the
higher prevalenceofthis autoantibodyfoundin thisstudy
cannot be justifiedby immunesystem changes associated
withtheagingprocess.Furthermore,itisworthnotingthat
thecutoffpointusedfordefiningEORAinthisstudywas60
years,1whichmakesthispopulationsomewhatyoungerand
lesssubjecttoimmunosenescencethanthatfromother
stud-ies,wherethecutoffpointof65yearswasadopted.8
Moreover,inthisstudyacomparisongroupmatchedfor
diseasedurationwasincluded,whichallowedamorerealistic
analysisoftheeffectsofthediseaseonthefunctionalcapacity
ofthedifferentgroups.
An interesting observation was the finding of a trend
toward theappearance ofinterstitialpneumonitisinEORA
individuals.Althoughthisextra-articularmanifestationwas
notassociatedwithageatdiseaseonset,ithasbeenfound
morefrequentlyinmaleindividuals21who,inturn,aremore
commoninEORAgroups.Oneshouldtakeintoaccountthat
this finding may be influenced by the fact that this study
wasperformedinatertiarycenter,withaheavierreferralof
patientswithmoreseveredisease.
Inconclusion,itcanbesaidthat,inourregion,patients
withEORAhavehigherprevalenceofmaleindividuals and
that, despiteequaltreatment and control ofinflammatory
activityinbothgroups,patientswithYORAhaveaworse
func-tionalperformance.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
494
rev bras reumatol.2017;57(5):491–4942. TutuncuT,KremerG,KavanoughA.Dopatientswitholder onsetrheumatoidarthritisreceivelessaggressivetreatment. AnnRheumDis.2006;65:1226–9.
3. OlivieriI,PalazziC,PeruzG,PadulaA.Managementissue withelderlyonsetrheumatoidarthritis:anuptodate.Drugs Aging.2005;22:809–22.
4. Villa-BlancoJI,Calvo-AlénJ.Elderlyonsetrheumatoid arthritisdifferentialdiagnosisandchoiceoffirst-lineand subsequenttherapy.DrugsAging.2009;26:739–50.
5. ChoSK,SungY-K,ChoiC-B,ChaH-S,ChoeJ-Y,ChungWT, etal.Patientswithelderly-onsetrheumatoidarthritishave severefunctionaldisability.SeminArthritisRheum. 2012;42:23–31.
6. LimaRA,PaulaAp,SilvaJA,MotaLM,CostaGP,SimaanCK, etal.Artritereumatoide:estudocomparativotransversal entreadoenc¸adoidosoedoadultojovem.RevBras Reumatol.2002;41:S31.
7. TutuncuZ,KavanaughA.Rheumaticdiseaseintheelderly: rheumatoidarthritis.RheumDisClinNorthAm.
2007;33:57–70.
8. Spinel-BejaranoN,QuintanaG,HerediaR,YunisJJ,Caminov JE,GarcésMF,etal.Comparativestudyofelderlyonset rheumatoidarthritisandyoungonsetrheumatoidarthritisin aColombianpopulation:clinical,laboratoryandHLADRB1 findings.ClinExpRheumatol.2013;31:40–6.
9. FarragherTM,GoodsonNJ,NaseemH,SilmanAJ,Thomson W,SymmonsD,etal.AssociationofHLA–DRB1genewith prematuredeath,particularlyfromcardiovasculardisease,in patientswithrheumatoidarthritisandinflammatory polyarthritis.ArthritisRheum.2008;58:359–69.
10.Gonzalez-GayMA,HajeerAH,DababnehA,MakkiR, Garcia-PorruaC,ThomsonW,etal.Seronegativerheumatoid arthritisinelderlyandpolymyalgiarheumatichavesimilar patternsofHLAassociation.JRheumatol.2001;28:122–5.
11.SymmondsDOM,BarretEM,BankheadCR,ScottDG,Silman AJ.TheincidenceofrheumatoidarthritisintheUnited Kingdom:resultsfromaNorfolkArthritisRegister.BrJ Rheumatol.1994;33:735–9.
12.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
13.FransenJ,vanRielPLCM.DASremissioncutpoints.ClinExp Rheumatol.2006;24Suppl43:S29–32.
14.FerrazMB[thesis]Traduc¸ãoparaoportuguêsevalidac¸ãodo questionárioparaavaliaracapacidadefuncional“Stanford HealthAssessmentQuestionnaire”.SãoPaulo:Universidade FederaldeSãoPaulo;EscolaPaulistadeMedicina;
1990.
15.TurkcaparN,DemirO,AtliT,KopukM,TurgayM,KinikliG, etal.Lateonsetrheumatoidarthritis:clinicalandlaboratory comparisonswithyoungeronsetpatients.ArchGerontol Geriatr.2006;42:225–31.
16.BajocchiG,LaCorteR,LocaputoA,GovoniM,TrottaF.Elderly onsetrheumatoidarthritis:clinicalaspects.ClinExp Rheumatol.2000;18Suppl20:S49–50.
17.PeaseCT,BhaktaBB,DevlinJ,EmeryP.Doestheageofonset ofrheumatoidarthritisinfluencephenotype?Aprospective studyofoutcomeandprognosticfactors.Rheumatology (Oxford).1999;38:228–34.
18.Calvo-AlénJ,CorralesA,Sánchez-AndradaS,
Fernández-EchevarríaMA,Pe ˜naJL,Rodríguez-ValverdeV. Outcomeoflate-onsetrheumatoidarthritis.ClinRheumatol. 2005;24:485–9.
19.NazSM,FarragherTM,BunnDK,SymmonsDP,BruceIN.The influenceofageatsymptomonsetandlengthoffollow-upon mortalityinpatientswithrecent-onsetinflammatory polyarthritis.ArthritisRheum.2008;58:985–9.
20.NisiharaR,KubisMM,RodriguesPC,SkareT,MocelinV, UtiyamaS.Antinuclearantibodiesandrheumatoidfactor positivityinhealthyelderlyadults:across-sectionalstudyin 336individuals.JAmGeriatrSoc.2013;61:2044–6.