ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Influence
of
periodontal
treatment
on
rheumatoid
arthritis:
a
systematic
review
and
meta-analysis
夽
Débora
Cerqueira
Calderaro
a,∗,
Jôice
Dias
Corrêa
b,
Gilda
Aparecida
Ferreira
c,
Izabela
Guimarães
Barbosa
d,
Carolina
Castro
Martins
e,
Tarcília
Aparecida
Silva
f,
Antônio
Lúcio
Teixeira
gaUniversidadeFederaldeMinasGerais,HospitaldasClínicas,Servic¸odeReumatologia,BeloHorizonte,MG,Brazil
bUniversidadeFederaldeMinasGerais,InstitutodeCiênciasBiológicas,ProgramadePós-Graduac¸ãoemBiologiaCelular,Belo
Horizonte,MG,Brazil
cUniversidadeFederaldeMinasGerais,FaculdadedeMedicina,DepartamentodoAparelhoLocomotor,BeloHorizonte,MG,Brazil dHospitaldoInstitutodePrevidênciadosServidoresdoEstadodeMinasGerais,Servic¸odePsiquiatria,BeloHorizonte,MG,Brazil eUniversidadeFederaldeMinasGerais,FaculdadedeOdontologia,DepartamentodeOdontopediatriaeOrtodontia,BeloHorizonte,MG,
Brazil
fUniversidadeFederaldeMinasGerais,FaculdadedeOdontologia,DepartamentodeClínica,PatologiaeCirurgiaOdontológicas,Belo
Horizonte,MG,Brazil
gUniversidadeFederaldeMinasGerais,FaculdadedeMedicina,DepartamentodeMedicinaInterna,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received19May2016 Accepted24October2016 Availableonline4January2017
Keywords:
Periodontal-systemicdisease interactions
Periodontitis Rheumatoidarthritis Meta-analysis
a
b
s
t
r
a
c
t
Objective:Toevaluatetheinfluenceofperiodontaltreatmentonrheumatoidarthritis activ-ity.
Methods:MEDLINE/PUBMED,TheCochraneLibrary,ClinicalTrials,SciELOandLILACSwere searchedforstudiespublisheduntilDecember2014.Includedarticleswere:prospective studies;includingpatientsolderthan18years,diagnosedwithperiodontitisandrheumatoid arthritissubmittedtonon-surgicalperiodontaltreatment;withacontrolgroupreceivingno periodontaltreatment;withoutcomesincludingatleastonemarkerofrheumatoidarthritis activity.MethodologicalqualityofthestudieswasassessedusingPEDroscale.Quantitative datawerepooledinstatisticalmeta-analysisusingReviewManager5.
Results:Fourarticles wereincluded.Non-surgicalperiodontaltreatmentwasassociated withasignificantreductionofDAS28(OR:−1.18;95%CI:−1.43,−0.93;p<0.00001). Erythro-cytesedimentationrate,C-reactiveprotein,patient’sassessmentofrheumatoidactivity usingvisualanalogicalscale,tenderandswollenjointcountsshowedatrendtoward reduc-tion(notstatisticallysignificant).
夽
StudyconductedatUniversidadeFederaldeMinasGerais,FaculdadedeOdontologiaeFaculdadedeMedicina,Departamentodo AparelhoLocomotor,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](D.C.Calderaro).
http://dx.doi.org/10.1016/j.rbre.2016.11.011
2255-5021/© 2016 Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND license (http://
Conclusions: ThereductionofDAS28inpatientswithrheumatoidarthritisafterperiodontal treatmentsuggeststhattheimprovementofperiodontalconditionisbeneficialtothese patients.Furtherrandomizedcontrolledclinicaltrialsarenecessarytoconfirmthisfinding. ©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Influência
do
tratamento
periodontal
na
artrite
reumatoide:
revisão
sistemática
e
metanálise
Palavras-chave: Interac¸õesdoenc¸a periodontal-sistêmica Periodontite
Artritereumatoide Metanálise
r
e
s
u
m
o
Objetivo: Avaliarainfluênciadotratamentoperiodontalsobreaatividadedadoenc¸ana artritereumatoide.
Métodos: Pesquisaram-se as bases de dados MEDLINE/PubMed, The Cochrane Library, ClinicalTrials, SciELOeLILACSembuscadeestudospublicados atédezembrode2014. Incluíram-seestudosprospectivosqueavaliarampacientescommaisde18anos diagnos-ticadoscomperiodontiteeartritereumatoidesubmetidosatratamentoperiodontalnão cirúrgico;osestudosdeveriamtertambémumgrupocontrolenãosubmetidoatratamento periodontal.Osresultadosdosestudosdeveriamcontarcompelomenosummarcadorda atividadedadoenc¸anaartritereumatoide.Aqualidademetodológicadosestudosfoi avali-adautilizandoaescalaPEDro.Reuniram-seosdadosquantitativosemumametanálise estatísticausandooReviewManager5.
Resultados:Incluíram-sequatroartigos.Otratamentoperiodontalnãocirúrgicoesteve asso-ciadoaumareduc¸ãosignificativanoDAS-28(OR:-1,18;IC95%:-1,43a-0,93;p<0,00001). Avelocidadedehemossedimentac¸ão,aproteínaC-reativa,aavaliac¸ãodaatividade reuma-toide pelaescala visualanalógicae ascontagens de articulac¸ões sensíveis einchadas apresentaramumatendênciadereduc¸ão(reduc¸ãonãoestatisticamentesignificativa). Conclusões: Areduc¸ãonoDAS-28empacientescomartritereumatoideapóstratamento periodontalsugerequeamelhoranacondic¸ãoperiodontalébenéficaaestespacientes.São necessáriosmaisensaiosclínicosrandomizadoscontroladosparaconfirmaresteachado.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Previousclinicalandexperimentalstudieshavesuggestedan associationbetweenperiodontaldisease(PD)andrheumatoid arthritis(RA).1–9 Thisassociationisbasedoncommon
envi-ronmental,inflammatoryandgeneticpathwayssharedbyRA andPDthatincludesmoking,HLA-DRantigens,inflammatory pattern,tissuedestructionpathways.Furthermore,the possi-bleroleofperiodontopathicbacteriaPorphyromonasgingivalis, thatproducesapeptidylargininedeiminasecapableof citrulli-nationofhumanproteins,wasdemonstratedinRA.Apossible roleforPDinhamperinganti-tumornecrosisfactortreatment responseinRAhasalsobeensuggested.10–21
Aseriesofintervention trialsto assessthe effectofPD treatmenton RAhavebeen performed. Thesetrials exam-ineddifferentRAactivityparameters,suchasDiseaseActivity Score (DAS 28), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP),patient’s assessment ofrheumatoid activityusingvisualanalogicalscale(VAS),tender(TJC)and swollen (SJC) joint counts, cytokines (Interleukin (IL) 1-, tumornecrosisfactor(TNF)-␣),antibodies(rheumatoidfactor, anti-cycliccitrullinatedproteinantibodies,antibodiesanti-P. gingivalis)and/ormeasuresofqualityoflife.Theresultswere quitecontroversial,withpositive,negativeorneutralfindings
regarding the effect ofPD treatment on RAoutcomes.22–31
Therefore,theimpactofPDtreatmentonRAactivityremains tobedetermined.
Thepresentsystematicreviewandmeta-analysisaimedto investigatetheeffectsofPDnon-surgicaltreatmentin inflam-matory parameters and clinical measuresofRAactivity in adultpatients.Thisreviewwasconductedaccordingtothe QUOROMstatement forimproving thequality ofreportsof meta-analysesofrandomizedcontrolledtrials.32
Methods
Searchstrategy
Records identified through database search
(n=217)
Additional records identified through hand
search (n=4)
Records after duplicates removed screened (n=210)
Records excluded (n=202)
Records screened (n=210)
Included
Elegibility
Screening
Identification
Final exclusion of articles – Intervention studies with
no control group (n=3)
Exclusion (numerical data not provided)
(n=1) – Basic science, rheumatic
diseases other than RA, case reports (n=68) – No therapeutic intervention (n=52) – Reviews, editorials, comments, letters (n=44)
– Incomplete trials (n=3) –Trials with RA intervention (n=4)
Full-text articles assessed for elegibility (n=8)
Studies included in qualitative synthesis (n=5)
Studies included in quantitative synthesis (meta-analysis) (n=4)
Fig.1–Flowdiagramforstudiesretrievedthroughthesearchingandselectionprocess.RA,rheumatoidarthritis.
ThesearchstrategyforLILACSandSciELOwas:((Chronic Periodontitis) OR (Periodontitis Crónica) OR (Periodontite Crônica))AND ((Arthritis, Rheumatoid)OR(Artritis Reuma-toide)OR(ArtriteReumatoide)).
Thesearchwasindependentlyperformedbytwo review-ers(DCC,JDC).Disagreementsweresolvedbydiscussion.The Kappa between the two reviewers that independently per-formedthesearchwas0.764.
In addition to the online search, a hand search of the bibliographiesofreviews,comments,letters,casereports, edi-torialsandotherpapersaddressingtherelationshipbetween RAandPDwasconducted.
Theflowchartofthesearchandselectionprocessisshown inFig.1.
Methodological quality of the included studies was assessedusingthePEDroscale33bytwoindependent
review-ers(DCCand JDC)and disagreements weresolvedthrough discussion.
Selectioncriteria
Inclusioncriteria
Interventionstudies;inclusionofadultpatients(olderthan18 years)diagnosedwithbothPDandRA;interventioncomprised ofnon-surgicalperiodontaltreatment;presenceofacontrol groupreceivingnoperiodontaltreatmentforthelengthofthe study;outcomeforRAthatincludedatleastoneofthe follow-ing:erythrocytesedimentationrate(ESR),C-reactiveprotein (CRP),DiseaseActivityScore(DAS28),tender(TJC)andswollen (SJC)jointcountsandpatient’sassessmentofRAactivityusing
a100mm-visualanalogicalscale(VAS);follow-upofatleastsix 6weeks.
Exclusioncriteria
Case reports, review articles, editorials, comments, letters totheeditor,experimentalstudies/basicscience,articleson RAtherapeuticinterventionsandreportsaboutpatientswith rheumaticdiseasesotherthanRAwereexcluded.
Datacollection
Dataabstractionwasperformedinduplicate,bytwo indepen-dent reviewers(DCC,JDC). Attemptswere madetocontact originalauthorsformissingdata,butonlytheauthorsofone articleprovidedustheinformationrequired(TJCandSJCmean andstandarddeviationinperiodontaldiseasefortreatedand non-treatedgroupsatbaselineandafterfollow-up).29
Methodologicalqualityassessment
Thequalityofthestudieswaspeer-reviewed(DCC,JDC)by usingamodifiedversionofthePEDroscaleforclinicaltrials.33
Disagreementswereresolvedbyconsensus(Table1).
Quantitativedatasynthesis
Table1–Estimatesofreliabilityfromincludedstudiesforeachofthe11itemsofthePEDroscale.32
PEDroscaleitem Al-Katmaetal.,200725 Pinhoetal.,200926 Ortizetal.,200927 Okadaetal.,201329
Eligibilitycriteriaspecified 1 1 1 1
Randomallocation 1 0 1 1
Concealedallocation 0 0 0 0
Groupssimilaratbaseline 1 1 1 1
Subjectblinding 0 0 0 0
Therapistblinding 0 0 0 0
Assessorblinding 1 0 0 0
Lessthan15%dropouts 0 1 1 1
Intention-to-treatanalysis 1 1 1 1
Between-groupstatisticalcomparisons 1 0 1 1
Pointmeasuresandvariabilitydata 1 1 1 1
Total 7 5 7 7
Toassessoverallefficacyfromallthestudiesincludedin themeta-analysis,wecalculatedmeandifferenceusingboth fixed-effectsand random-effects models, reporting hetero-geneity and overall p-values.When I2>50% indicated high
heterogeneitybetweenstudies,therandom-effectmodelwas adopted,andwhenI2<50%thefixedeffectmodelwasused.
Studiesthatdidnotreportstandarddeviationwereexcluded fromthemeta-analysis.Theeffectsizesforeachstudyand overallpooledeffectsizeswerecalculatedwitha95% confi-denceinterval.Statistical significancewasdeclaredifthe p valuewaslessthan0.05.
Results
Four articles25–27,29 were included in the meta-analysis
(Table2).
Theyweresingle-centerinterventionalcontrolledstudies. Thecriteriausedforthediagnosisofperiodontitisvaried. Al-Katma et al.25 included patients with generalized
mild-to-moderatechronic periodontitisaccording to Armitage35;
Pinhoet al.26 definedPD accordingtoMachtei et al.36: the
presence of at least two teeth with CAL≥ 6mm and at
least one tooth with probing depth≥ 5mm. Ortiz et al.27
includedpatientswithgeneralizedseverechronic periodon-titis according to Löe and Sillness,37 while Okada et al.29
definedperiodontitisasthepresenceofatleastonesitewith CAL≥ 4mm.
Studies were conducted from 2007 to 2013 in different countries: Brazil,26 Japan29 and USA25,27 with participants
fromdifferentethnicandculturalbackgrounds.
SubjectsofthesestudiespresentedbothRAandPD,and weredivided intwo groups:onesubmittedto non-surgical periodontaltreatmentconsistingofscaling/rootplanningand plaqueremovalandhygiene instructions(treatmentgroup) andoneother groupthat wasonlyfollowed upduringthe periodofthestudy(controlgroup),withoutperiodontal treat-mentororalhygieneinstruction.
Thefollow-up periodwas6-weeks,25 8-weeks27,29 or six
months.26
PEDroscoresofthestudiesincludedinthismeta-analysis areshowninTable1.Qualityassessmentvariedfrom7to5 points.
Analysisofthepooleddatafortheoutcomesevaluatedon thismeta-analysisisshowninTable3.
DAS28isacompositediseaseactivityscorethathasbeen largely used tomeasure RA activity.38 A reduction of DAS
28 means that RA has improved. The pooled data of the two studies included in the meta-analysis suggests a dis-crete, but significant reduction in DAS 28 score following non-surgicalperiodontaltreatment(OR:−1.18;95%CI:−1.43, −0.93;p<0.00001)(Table3;Fig.2).25,27
Therewasnoevidenceforaneffectofperiodontal ther-apyinthebloodlevelsofCRP(OR:−0.16;95%CI:−0.64,0.33; p=0.53)and ESR(OR:−6.68;95% CI:−28.57,15.21; p=0.55);
patient’sglobalVAS(OR:−1.56;95%CI:−8.14,5.02;p=0.84);
TJC(OR:−2.97;95%CI:−8.76,2.82;p=0.31)orSJC(OR:−2.53;
95%CI:−5.89,0.83,p=0.14)(Table3).25,26,29
Discussion
RAandPDsharesimilarpathogenicmechanisms,i.e. inflam-matory cells and pro-inflammatory cytokines that drive chronic bone erosion in RA and chronic gum destruction in PD are similar.A role forPD on initiation and mainte-nanceofRAautoimmuneinflammatoryresponses,eveninRA patientsreceivingconventionalsyntheticdiseasemodifying anti-rheumaticdrugsorbiologics(specificallyTNFinhibitors), hasbeensuggested.6,10,12–15,21
The control of local periodontal infection and inflam-mation bynon-surgical periodontal therapy isexpected to attenuate systemic inflammatory response which in turn wouldcontributetoimproveRAactivity.Accordingly,the cur-rentmeta-analysisshowsthat,afternon-surgicalperiodontal treatment,thereisreductionofDAS28inRApatientswithPD, corroboratingtheimpactofperiodontalconditiononRA.
In contrast, evaluation of the other variables failed to demonstratetheeffectofPDtreatmentinRAactivity.A possi-bleexplanationisregardingthecomplexnatureofRA,which diseaseactivityisbetterevaluatedbyacompositescorelike DAS28insteadofindividualanalysisofinflammatoryand clin-icalmarkers.
Corroborating thesefindings,recently,Kaur etal.22
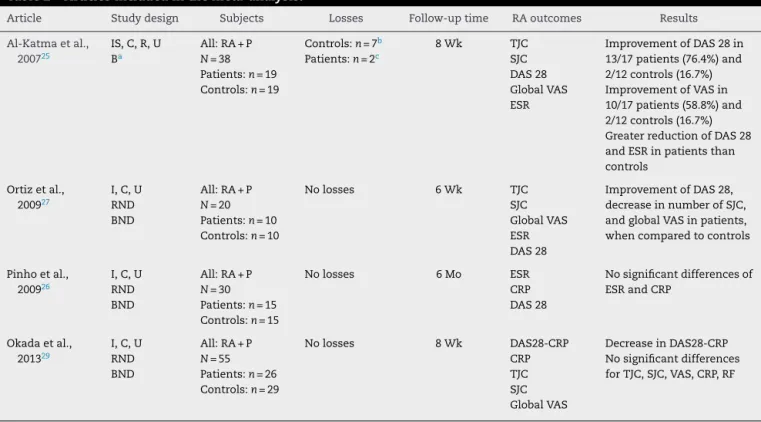
Table2–Articlesincludedinthemeta-analysis.
Article Studydesign Subjects Losses Follow-uptime RAoutcomes Results
Al-Katmaetal., 200725
IS,C,R,U Ba
All:RA+P N=38 Patients:n=19 Controls:n=19
Controls:n=7b
Patients:n=2c
8Wk TJC
SJC DAS28 GlobalVAS ESR
ImprovementofDAS28in 13/17patients(76.4%)and 2/12controls(16.7%) ImprovementofVASin 10/17patients(58.8%)and 2/12controls(16.7%) GreaterreductionofDAS28 andESRinpatientsthan controls
Ortizetal., 200927
I,C,U RND BND
All:RA+P N=20 Patients:n=10 Controls:n=10
Nolosses 6Wk TJC
SJC GlobalVAS ESR DAS28
ImprovementofDAS28, decreaseinnumberofSJC, andglobalVASinpatients, whencomparedtocontrols
Pinhoetal., 200926
I,C,U RND BND
All:RA+P N=30 Patients:n=15 Controls:n=15
Nolosses 6Mo ESR
CRP DAS28
Nosignificantdifferencesof ESRandCRP
Okadaetal., 201329
I,C,U RND BND
All:RA+P N=55 Patients:n=26 Controls:n=29
Nolosses 8Wk DAS28-CRP
CRP TJC SJC GlobalVAS
DecreaseinDAS28-CRP Nosignificantdifferences forTJC,SJC,VAS,CRP,RF
RA,rheumatoidarthritis;P,periodontitis;DAS28,diseaseactivityscore;DAS28-CRP,diseaseactivityscoreusingC-reactiveprotein;ESR, erythro-cytesedimentationrate;CRP,C-reactiveprotein;TJC,tenderjointcount;SJC,swollenjointcount;VAS,visualanalogicalscale;IS,intervention study;C,controlled;R,randomized;U,unicentric;RND,randomizationnotdescribed;B,blinded;BND,blindingnotdescribed;Wk,weeks;Mo, months.
a Rheumatologistblindedtoperiodontaltreatment.Patients:thosesubmittedtonon-surgicalperiodontaltreatment.Controls:Thosenot
submittedtoperiodontaltreatment.
b Four:absencetoevaluations;three:changesinmedicationsforRA.
c One:absencetoevaluations;one:inabilitytomaintaingoodleveloforalhygiene.
Table3–Meta-analysisforoutcomesevaluated.
Outcome OR[95%CI] I2;p-value Numberofpatients(periodontal
treatment/notreatment)
Numberofstudies(References)
DAS28 −1.18[−1.43,−0.93] 0%;<0.00001 27/22 2(Al-Katmaetal.25;Ortizetal.27)
CRP −0.16[−0.64,0.33] 77%;0.53 41/44 2(Okadaetal.29;Pinhoetal.26)
ESR −6.68[−28.57,15.21] 97%;0.55 32/27 2(Al-Katmaetal.25;Pinhoetal.26)
TJC −2.97[−8.76,2.82] 97%;0.31 43/41 2(Al-Katmaetal.25;Okadaetal.29)
SJC −2.53[−5.89,0.83] 96%;0.14 43/41 2(Al-Katmaetal.25;Okadaetal.29)
GlobalVAS −1.56[−8.14,5.02] 84%;0.84 43/41 2(Al-Katmaetal.25;Okadaetal.29)
DAS28,diseaseactivityscore;CRP,C-reactiveprotein;ESR,erythrocytesedimentationrate;TJC,tenderjointcount;SJC,swollenjointcount; VAS,visualanalogicalscale;OR,oddsratio;CI,confidenceinterval.
No treatment Mean difference
SD Mean
–0.6 0.49 17 0.5 0.43 12 54.3% –1.10 [–1.44,–0.76] –1.58 0.47 10 –0.31 0.36 10 45.7% –1.27 [–1.64,–0.90]
Mean
Total SDTotal IV, Fixed, 95%Cl
Mean difference Periodontal treatment
Study or subgroup
Total (95% Cl)
Heterogeneity: Chi2 = 0.45, df = 1 (P=.50); l2 = 0%
Test for overall effect:Z = 9.30 (P<.00001)
27 22
Periodontal treatment No treatment –100 –50 0 50 100
–1.18 [–1.43, –0.93]
Ortiz el al., 2007 Al-katma el al., 2007
IV, Fixed, 95%Cl
100.0%
Weight
markerswereincreasedinRApatientswithPD(CRP,IL-1and serumantibodiestoP.gingivalis),incomparisonwithpatients withoutPD.Although,nodifferencesinotherparameters(ESR, anti-cycliccitrullinated proteinantibodies,rheumatoid fac-tor,TNF-␣) were observed comparingboth groups, a trend towardadecreaseinESRinRApatientsafterPDtreatment wasreported.22
In another systematic review with meta-analysis, Kaur etal.23havealsoevaluatedtheinfluenceofPDtreatmenton
RAactivity.Intheirpooleddatameta-analysis,DAS28wasnot influencedbyPDnon-surgicaltherapy.Kauretal.23included,
inthepooledmeta-analysisofDAS28,thedatafromthestudy ofOkadaetal.,29thatanalyzedDAS28-CRP,anotherRAactivity
compositescore,slightlydifferentfromDAS28(insteadofESR, itincludesCRP),thatpresentsgoodcorrelation,but underes-timatesdiseaseactivitywhencomparedtoDAS28.39Forthis
reason,theresultsofKauretal.23mighthavebiasedthe
pos-sibleinfluenceofPDtreatmentonDAS28andinthepresent meta-analysis,thedataonDAS28-CRPwereexcludedfromthe analysis.TheyhavealsofoundasignificantreductionofESR inPDtreatedpatients,whatmightbeexplainedthroughthe inclusionofthedatafrom Ortizetal.,27sinceKauret al.23
transformedinter-quartilerangesorrangesinstandardized mean difference,assuming anormaldistribution curve for thisstudy,increasingthenumberofpatientsandimproving thedetectionofsmalldifferences.
Thefourstudieseligibleforthismeta-analysisevaluateda smallnumberofsubjects.Randomizationwaswelldescribed in one,25 cited in two27,29 and not mentioned in one.26
RegardingPDtreatment,blindingofpatientsandtherapists, isnotpossible.Toovercomethislimitation,onealternative isblinding the evaluator. Thiswas mentioned inonly one study.25Onestudy25hadahighnumberofdropouts.
Partic-ipantshadPDdiagnosedaccordingtodifferentclassification systems. The follow-up period ranged from 6-weeks to 8-weeksinthreestudies,25,27,29whichisarelativelyshorttime
toassesstheimpactoftherapeuticstrategiesinRAactivity. Allstudiesreportedanobjectiveimprovementin periodon-talclinicalparameters,suggestingthatthefollow-upperiod wassufficienttoobservereductionininfectionand inflam-mationassociatedwithPD.Theheterogeneityamongstudies washighformostoutcomesevaluated.Thesefeaturesmustbe weightedaspossiblelimitationsofthepresentmeta-analysis. Thecurrentmeta-analysissuggeststhatnon-surgical peri-odontaltreatmentmighthaveabeneficialeffectonRAactivity asevaluatedbyDAS28.Furtherrandomizedcontrolledclinical trialsincludingalarger numberofpatients,with appropri-ateblindingandlongerperiodsoffollow-uparenecessaryto confirmthisfinding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CantleyMD,HaynesDR,MarinoV,BartoldPM.Pre-existing
periodontitisexacerbatesexperimentalarthritisinamouse
model.JClinPeriodontol.2011;38:532–41.
2.ChrysanthakopoulosNA,ChrysanthakopoulosPA.
Associationbetweenindicesofclinically-defined
periodontitisandself-reportedhistoryofsystemicmedical
conditions.JInvestigClinDent.2016;7:27–36.
3.JosephR,RajappanS,NathSG,PaulBJ.Associationbetween
chronicperiodontitisandrheumatoidarthritis:a
hospital-basedcase–controlstudy.RheumatolInt.
2013;33:103–9.
4.ChenHH,HuangN,ChenYM,ChenTJ,ChouP,LeeYL,etal.
Associationbetweenahistoryofperiodontitisandtheriskof
rheumatoidarthritis:anationwide,population-based,
case–controlstudy.AnnRheumDis.2013;72:1206–11.
5.DissickA,RedmanRS,JonesM,RanganBV,ReimoldA,
GriffithsGR,etal.Associationofperiodontitiswith
rheumatoidarthritis:apilotstudy.JPeriodontol.
2010;81:223–30.
6.MikulsTR,PayneJB,YuF,ThieleGM,ReynoldsRJ,Cannon
GW,etal.PeriodontitisandPorphyromonasgingivalisin
patientswithrheumatoidarthritis.ArthritisRheumatol.
2014;66:1090–100.
7.MonsarratP,VergnesJN,BlaizotA,ConstantinA,deGradoGF,
RamambazafyH,etal.Oralhealthstatusinoutpatientswith
rheumatoidarthritis:theOSARAstudy.OralHealthDent
Manag.2014;13:113–9.
8.FarahVakarF,SyedAfrozA,AtherSA.Evaluationof
correlationbetweenperiodontitisandrheumatoidarthritisin
anIndianpopulation.JClinDiagRes.2010;4:3654–8.
9.WolffB,BergerT,FreseC,MaxR,BlankN,LorenzHM,etal.
Oralstatusinpatientswithearlyrheumatoidarthritis:a
prospective,case–controlstudy.Rheumatology(Oxford).
2014;53:526–31.
10.RamamurthyNS,GreenwaldRA,CelikerMY,ShiEY.
Experimentalarthritisinratsinducedbiomarkersof
periodontitiswhichareamelioratedbygenetherapywith
tissueinhibitorofmatrixmetalloproteinases.JPeriodontol.
2005;76:229–33.
11.MirrielessJ,CroffordLJ,LinY,KryscioRJIII,DawsonDR,
EbersoleJL,etal.Rheumatoidarthritisandsalivary
biomarkersofperiodontaldisease.JClinPeriodontol.
2010;37:1068–74.
12.MareszKJ,HellvardA,SrokaA,AdamowiczK,BieleckaE,
KozielJ,etal.Porphyromonasgingivalisfacilitatesthe
developmentandprogressionofdestructivearthritisthrough
itsuniquebacterialpeptidylargininedeiminase(PAD).PLoS
Pathog.2013;9:e1003627.
13.QuirkeAM,LugliEB,WegnerN,HamiltonBC,CharlesP,
ChowdhuryM,etal.Heightenedimmuneresponseto
autocitrullinatedPorphyromonasgingivalispeptidylarginine
deiminase:apotentialmechanismforbreaching
immunologictoleranceinrheumatoidarthritis.AnnRheum
Dis.2014;73:263–9.
14.GümüsP,BuduneliE,BiyikogluB,AksuK,Sarac¸F,NileC,etal.
Gingivalcrevicularfluid,serumlevelsofreceptoractivatorof
nuclearfactor-Bligand,osteoprotegerin,andinterleukin-17
inpatientswithrheumatoidarthritisandosteoporosisand
withperiodontaldisease.JPeriodontol.2013;84:
1627–37.
15.TémoinS,ChakakiA,AskariA,El-HalabyA,FitzgeraldS,
MarcusRE,etal.IdentificationoforalbacteriaDNAin
synovialfluidofarthritispatientswithnativeandfailed
prostheticjoints.JClinRheumatol.2012;18:117–21.
16.BiyikogluB,BuduneliN,KardeslerL,AksuK,OderG,
Kütükc¸ülerN.Evaluationoft-PA,PAI-2,IL-1betaandPGE(2)in
gingivalcrevicularfluidofrheumatoidarthritispatientswith
peridontaldisease.JClinPeriodontol.2006;33:605–11.
17.BiyikogluB,BuduneliN,KardeslerL,AksuK,PitkalaM,Sorsa
T.GingivalcrevicularfluidMMP-8and-13andTIMP-1levels
inpatientswithrheumatoidarthritisandinflammatory
18.NilssonM,KoppS.Gingivitisandperiodontitisarerelatedto
repeatedhighlevelsofcirculatingtumornecrosis
factor-alphainpatientswithrheumatoidarthritis.J
Periodontol.2008;79:1689–96.
19.BozkurtFY,BerkerE,AkkusS,BulutS.Relationshipbetween
interleukin-6levelsingingivalcrevicularfluidand
periodontalstatusinpatientswithrheumatoidarthritisand
adultperiodontitis.JPeriodontol.2000;71:1756–60.
20.BozkurtFY,YetkinAyZ,BerkerE,TepeE,AkkusS.
Anti-inflammatorycytokinesingingivalcrevicularfluidin
patientswithperiodontitisandrheumatoidarthritis:a
preliminaryreport.Cytokine.2006;35:180–5.
21.SavioliC,RibeiroAC,FabriGM,CalichAL,CarvalhoJ,SilvaCA,
etal.Persistentperiodontaldiseasehampersanti-tumor
necrosisfactortreatmentresponseinrheumatoidarthritis.J
ClinRheumatol.2012;18:180–4.
22.KaurS,WhiteS,BartoldPM.Periodontaldiseaseand
rheumatoidarthritis:asystematicreview.JDentRes.
2013;92:399–408.
23.KaurS,BrightR,ProudmanSM,BartoldM.Doesperiodontal
treatmentinfluenceclinicalandbiochemicalmeasuresfor
rheumatoidarthritis?Asystematicreviewandmeta-analysis.
SeminArthritisRheum.2014;44:113–22.
24.LeãoJ,LeãoA,NovaesAB.Periodontalinfectionasapossible
severityfactorforrheumatoidarthritis.JClinPeriodontol.
2005;32:412–6.
25.Al-KatmaK,BissadaNF,BordeauxJM,SueJ,AskariAD.
Controlofperiodontalinfectionreducestheseverityofactive
rheumatoidarthritis.JCR.2007;13:134–7.
26.PinhoMN,OliveiraRDR,NovaesJRAB,VoltarelliFJ.C.
Relationshipbetweenperiodontitisandrheumatoidarthritis
andtheeffectofnon-surgicalperiodontaltreatment.Braz
DentJ.2009;20:355–64.
27.OrtizP,BissadaNF,PalomoL,HanYW,Al-ZahraniMS,
PanneerselvamA,etal.Periodontaltherapyreducesthe
severityofactiverheumatoidarthritisinpatientstreated
withorwithouttumornecrosisfactorinhibitors.J
Periodontol.2009;80:535–40.
28.RanadeSB,DoiphodeS.Istherearelationshipbetween
periodontitisandrheumatoidarthritis?JIndianSoc
Periodontol.2012;16:22–7.
29.OkadaM,KobayashiT,ItoS,YokoyamaT,AbeA,MurasawaA,
etal.Periodontaltreatmentdecreaseslevelsofantibodiesto
Porphyromonasgingivalisandcitrullineinpatientswith
rheumatoidarthritisandperiodontitis.JPeriodontol.
2013;84:e74–84.
30.BiyikigluB,BuduneliN,AksuK,NalbantsoyA,LappinDF,
EvrenosogluE,etal.Periodontaltherapyinchronic
periodontitislowersgingivalcrevicularfluid
interleukin-1betaandDAS28inrheumatoidarthritispatients.
RheumatolInt.2013;33:2607–16.
31.ErciyasK,SezerU,ÜstünK,PehlivanY,KisacikB,SenyurtSZ,
etal.Effectsofperiodontaltherapyondiseaseactivityand
systemicinflammationinrheumatoidarthritispatients.Oral
Dis.2013;19:394–400.
32.MoherD,CookDJ,EastwookS,OlkinI,RennieD,StroupDF,
fortheQUOROMGroup.Improvingthequalityofreportsof
meta-analysesofrandomisedcontrolledtrials:theQUOROM
statement.Lancet.1999;354:1896–900.
33.VerhagenAP,deVetHC,deBieRA,KesselsAG,BoersM,
BouterLM,etal.TheDelphilist:acriterialistforquality
assessmentofrandomizedclinicaltrialsforconducting
systematicreviewsdevelopedbyDelphiconsensus.JClin
Epidemiol.1998;51:1235–41.
34.ReviewManager(RevMan)[Computerprogram].Version5.3.
Copenhagen:TheNordicCochraneCentre,TheCochrane
Collaboration;2014.
35.ArmitageGC.Developmentofclassificationsystemfor
periodontaldiseasesandconditions.AnnPeriodontol.
1999;4:1–6.
36.MachteiEE,ChristerssonLA,GrossiSG,DunfordR,ZambonJJ,
GencoRJ.Clinicalcriteriaforthedefinitionof“Established
Periodontitis”.JPeriodontol.1992;63:207–15.
37.LöeH,SilnessJ.Periodontaldiseaseinpregnancy.I.
Prevalenceandseverity.ActaOdontolScand.1963;21:533–51.
38.PrevooML,van’tHofMA,KuperHH,vanLeeuwenMA,vande
PutteLB,vanRielPL.Modifieddiseaseactivityscoresthat
includetwenty-eight-jointcounts.Developmentand
validationinaprospectivelongitudinalstudyofpatientswith
rheumatoidarthritis.ArthritisRheum.1995;38:44–8.
39.InoueE,YamanakaH,HaraM,TomatsuT,KamataniN.
ComparisonofDiseaseActivityScore(DAS)28-erythrocyte
sedimentationrateandDAS28-C-reactive-proteinthreshold