ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Prevalence
of
ischemic
heart
disease
and
associated
factors
in
patients
with
rheumatoid
arthritis
in
Southern
Brazil
Rafael
Kmiliauskis
Santos
Gomes
a,∗,
Ana
Carolina
Albers
b,
Ana
Isadora
Pianowski
Salussoglia
b,
Ana
Maria
Bazzan
b,
Luana
Cristina
Schreiner
b,
Mateus
Oliveira
Vieira
b,
Patrícia
Giovana
da
Silva
b,
Patrícia
Helena
Machado
b,
Cynthia
Mara
da
Silva
b,
Mauro
Marcelo
Mattos
c,
Moacyr
Roberto
Cuce
Nobre
daCentrodeEspecialidadesdosMunicípiosdeBlumenaueBrusque,Blumenau,SC,Brazil
bFundac¸ãoRegionaldeBlumenau,FaculdadedeMedicina,Blumenau,SC,Brazil
cFundac¸ãoRegionaldeBlumenau,DepartamentodeSistemaseComputac¸ão,Blumenau,SC,Brazil
dUniversidadedeSãoPaulo,FaculdadedeMedicina,UnidadedeEpidemiologiaClínica,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31March2016 Accepted8November2016 Availableonline8February2017
Keywords:
Rheumatoidarthritis Cardiovasculardisease Acutemyocardialinfarction Prevalence
a
b
s
t
r
a
c
t
Objective:Toestimatetheprevalenceofischemicheartdiseaseandassociatedfactorsin patientswithrheumatoidarthritis.
Methods:Across-sectionalstudyusingtheAmericanCollegeofRheumatologydiagnostic criteriainordertoselectpatientsseenatprimaryorsecondaryhealthcareunitsin Blu-menau,SantaCatarina,SouthernBrazil,in2014.Thepresenceofischemicheartdisease wasdefinedasanacutemyocardialinfarctionwithpercutaneouscoronaryinterventionor coronaryarterybypassgraftsurgerythathasoccurredafterdiagnosis.Fischer’sexacttest, Wald’slineartrendtest,andmultivariatelogisticregressionanalysiswereusedtotestthe associations.
Results:Among296patients(83.1%female) withamean ageof56.6yearsanda mean rheumatoidarthritisdurationof11.3years,13 reportedhavingacutemyocardial infarc-tionrequiringapercutaneousorsurgicalreperfusionprocedure,aprevalenceof4.4%(95% CI2.0–6.7).DiabetesMellitus(oddsratio[OR]4.9[95%CI1.6–13.8])anddiseaseduration>10 years(OR8.2[95%CI1.8–39.7])weretheonlyfactorsassociatedwithanischemicdisease thatremainedinthefinalmodel,afterthemultivariateanalysis.
Conclusion:Theprevalenceofacutemyocardialinfarctionwassimilartothatobservedin otherstudies.Amongthetraditionalriskfactors,DiabetesMellitus,andamongthe fac-torsrelatedtorheumatoidarthritis,diseaseduration,werethevariablesassociatedwith comorbidity.
©2017ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](R.K.Gomes). http://dx.doi.org/10.1016/j.rbre.2017.01.006
Prevalência
de
doenc¸a
isquêmica
cardíaca
e
fatores
associados
em
pacientes
com
artrite
reumatoide
no
Sul
do
Brasil
Palavras-chave: Artritereumatoide Doenc¸acardiovascular Infartoagudodomiocárdio Prevalência
r
e
s
u
m
o
Objetivo: Estimaraprevalênciadadoenc¸aisquêmicacardíacaeosfatoresassociadosem pacientescomartritereumatoide.
Métodos:EstudotransversalqueusouocritériodiagnósticodoColégioAmericanode Reuma-tologiaparaselecionarpacientesatendidosnasunidadesdesaúdedaatenc¸ãoprimáriaou secundáriaemBlumenau,SantaCatarina,suldoBrasil,em2014.Apresenc¸adedoenc¸a cardíacaisquêmicafoidefinidacominfartoagudodomiocárdiocomintervenc¸ão coronari-anapercutâneaoucirurgiaderevascularizac¸ãodomiocárdioquetenhaocorridodepoisdo diagnóstico.Paratestarasassociac¸õesusou-seotesteexatodeFischer,otestedetendência lineardeWaldeaanálisederegressãologísticamultivariada.
Resultados: Entre296pacientes,83,1%demulheres,commédiade56,6anos,tempomédio deartrite reumatoidede11,3anos,13 relatamtertidoinfartoagudodomiocárdioque necessitoudeprocedimentodereperfusãopercutâneaoucirúrgica,prevalênciade4,4% (IC95%2,0-6,7).Odiabetesmelittus(razãodechancede4,9[IC95%1,6-13,8])eotempo dedoenc¸amaiordoque10anos(razãodechancede8,2[IC95%1,8-39,7])foramosúnicos fatoresassociadoscomadoenc¸aisquêmicaquepermaneceramnomodelofinalapósanálise multivariada.
Conclusão: Aprevalênciadeinfartoagudodomiocárdiofoisemelhantecomaobservada emoutrosestudos.Entreosfatoresderiscotradicionaiseentreosfatoresrelacionadosà artritereumatoide,odiabetesmelittuseotempodedoenc¸aforamasvariáveisassociadasà comorbidade.
©2017ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rheumatoidarthritis(RA)isasystemicinflammatory
autoim-mune disease characterized by the involvement of the
synovialmembraneofperipheraljointsleadingtodestruction andfunctionallimitation.1TheprevalenceofRAvariesfrom 0.24to1%oftheadultpopulation,withapredominanceof womenandahigherincidenceinthe30–50-yearagegroup.2–4 InBrazil,twostudieswerepublished.Thefirststudyshows avariationfrom 0.2to1%,dependingontheregionofthis country,5andtheotherestablishesaprevalenceof0.46%.6
Studiespoint toanincreasedriskofcardiovascular
dis-ease (CVD) in patients with RA compared to the general
population.7–9 CVDexertsagreatimpactandrepresentsan importantmorbidityinpatientswithRA,andacute myocar-dial infarction (MI)is considered to be the most common event.9,10 Studies conducted indifferent countries indicate thattheprevalencecanvaryfrom1to17%.10–12
The greatest number of cardiac ischemic events in RA
patientsisnot entirelyexplainedbythe presenceof tradi-tionalriskfactorsalone.10AstudyinSwedenwithtwocohorts ofRApatientsdemonstratedthatthereisnoincreaseinthe occurrenceofischemicheartdiseasepriortothe rheumato-logicdiagnosis.13Ontheotherhand,soonaftertheonsetof thedisease14andalongitscourse,15 RAplaysanimportant roleintheonsetofMI,aboveallinpatientswithan accumu-lationofseveritymarkers.10Thus,RAwasconsideredasan independentriskfactorfortheoccurrenceofcoronaryartery disease.16,17
Despite the important advancesin diagnosis and avail-abletreatments,thereremainsahighCVDmorbidity.10This isduetothecombinationofthecharacteristicsofachronic inflammatorydisease,whicharepredisposingfactorstothe developmentofcomorbidities;ofthedrugsusedintreatment, forexample,glucocorticoids11;toanincreasedprevalenceof traditionalriskfactorsoverthedurationofdisease18,19;and tothepersistentactivityofthediseaseinitsmostaggressive periods.7
The present study aimed to estimate the self-reported prevalenceofcoronaryischemic eventsand toidentifythe possibleassociatedfactorsinpatientswithRAinBlumenau, SantaCatarina,SouthernBrazil,in2014.
Materials
and
methods
Thisisacross-sectional,population-basedstudyconducted
betweenJuly2014and January2015withmenand women
aged20yearsandolderwithrheumatoidarthritisaccording
to the American College of Rheumatology (1987)
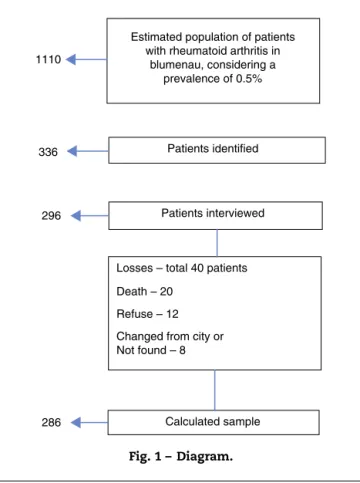
336
296
286 Calculated sample Patients identified
Patients interviewed
Losses – total 40 patients
Death – 20
Refuse – 12 Changed from city or Not found – 8 1110
Estimated population of patients with rheumatoid arthritis in
blumenau, considering a prevalence of 0.5%
Fig.1–Diagram.
Tocalculatethesamplesize,theformulaforestimatingthe prevalenceforasimplerandomsamplewasapplied.The fol-lowingparameterswereconsidered:prevalenceofRA=0.5% (1110 patients), prevalence ofexposure and unknown out-come=50%,samplingerror=5%,andconfidencelevelof95%. Thesamplesizecalculatedwasof286individuals.The sam-plecollectionprocess wascarriedout byreviewingmedical recordsinthebasichealthunitsandinthemedicalspecialty outpatientclinic,aswellasbyidentifyingpatientsinthe wait-ingroomatthehigh-costdrugdispensingpharmacyfromthe city(Fig.1).
Householdsvisitedatleasttwicewithouttheinterviewer meetingtheperson,includingaweekendvisitandanother nighttimevisit,orinthecaseofachangeofaddress,orevenin casesofrefusalontwooccasions,wereconsideredas“losses”.
Theteamwascomposedof8medicalstudentsfromthe
medicalschooloftheFundac¸ãoUniversidadeRegionalde Blu-menau(FURB),previouslytrainedtocarryoutapre-structured interviewand,ifnecessary,toconducttheinterviewby tele-phone in another occasion, and also by a local professor
supervisor. Quality control was performed in 20% of the
respondentswhentheywereinterviewedforasecondtime, throughtheapplicationofashortquestionnaire.
The dependent variable was the presence of a
posi-tivehistory ofa coronaryischemic event after adiagnosis
of rheumatoid arthritis, defined by an acute myocardial
infarctiondiagnosedbythephysicianandrequiringcardiac catheterization for angioplasty or stent implantation, or a coronaryarterybypassgraftsurgery.
The independent variables were defined as (a)
demo-graphicvariables:gender,ageincompletedyears,categorized
in a group of 20–59 years for adults and of 60 years or
morefortheelderly;(b)traditionalcardiovascularriskfactors reported in the interview: previous diagnosis of hyperten-sion,diabetesmellitusordyslipidemia,oruseofmedications for such diseases; previous or current smoking; prior and current practice of leisure-time physical activity; positive family historyforheartattack orcardiaccatheterizationat any age (mother, father, brothers or sisters); dichotomous categorization;currentbodymassindex–BMI(kg/m2) accord-ing to weightand height and categorized accordingto the
World Health Organization recommendations (low/normal
weight ≤24.9kg/m2, overweight 25–29.9kg/m2, and obesity ≥30kg/m2);and(c)RA-relatedvariables:diseasedurationin years and presenceofrheumatoid factor, both categorized respectively between 0–10 or 11 or moreyears of disease, andrheumatoidfactor<60(negativeorlowtiter)or>60(high titers).
Thedatawereenteredinasystemdevelopedforthisstudy withtheir outputintheExcel® tableformat;subsequently, the finalfilewas exportedtotheStata 10.0program(Stata Corp.,CollegeStation,UnitedStates).Thevariablesof inter-estwereanalyzedfortheirdistributions;forthisend,mean, standarddeviationandmedianwereusedforcontinuous vari-ables,andfrequencyandpercentagewereusedforcategorical variables.Totesttheassociationbetweenhistoryofacoronary ischemiceventandindependentvariables,theFisher’sexact testand,whereappropriate,theWald’slineartrendtestwere used.Afterthat,amultivariatelogisticregressionanalysiswas performed,aimingtoverifytheassociationofthefactors stud-iedwiththedependentvariable,withestimatesofgrossand adjustedoddsratios(OR)andoftherespective95%confidence intervals.
For the entry into the final multivariate model, all the variables with a p-value<0.20 in the univariate analysis were taken into account. Those variables that maintained a p-value≤0.05 or which were adjustedtothe final model remainedinthemultivariateregressionmodel.Forthe inclu-sion of the variables in the logistic regression model, the investigatorsoptedsequentiallybytheinclusion,inthefirst place,ofthedemographicvariables;then,thetraditionalrisk factorsforcoronaryarterydisease,andfinallythevariables relatedtothediseasewereincluded.Thisresearchwas sub-mittedtotheResearchEthicsCommitteeoftheUniversidade de SãoPaulo (USP)andFURB (protocols339/13and 133/12, respectively),havingobtainedapproval.Allparticipantsinthis studysignedaninformedconsentform.
Results
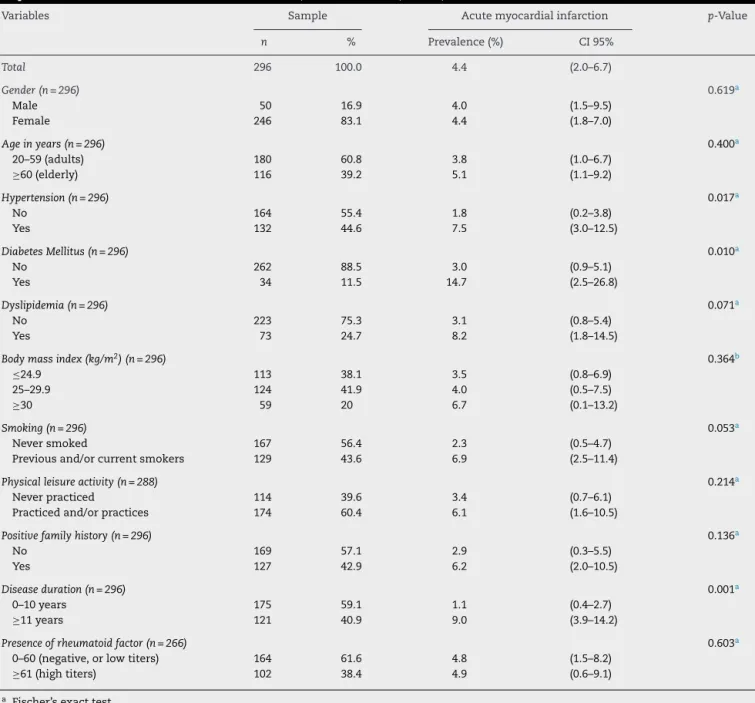
Table1–Descriptionofthesampleandprevalenceofacutemyocardialinfarctionaccordingtotheindependentvariables inpatientswithrheumatoidarthritis.Blumenau,SantaCatarina,Brazil,2014.
Variables Sample Acutemyocardialinfarction p-Value
n % Prevalence(%) CI95%
Total 296 100.0 4.4 (2.0–6.7)
Gender(n=296) 0.619a
Male 50 16.9 4.0 (1.5–9.5)
Female 246 83.1 4.4 (1.8–7.0)
Ageinyears(n=296) 0.400a
20–59(adults) 180 60.8 3.8 (1.0–6.7)
≥60(elderly) 116 39.2 5.1 (1.1–9.2)
Hypertension(n=296) 0.017a
No 164 55.4 1.8 (0.2–3.8)
Yes 132 44.6 7.5 (3.0–12.5)
DiabetesMellitus(n=296) 0.010a
No 262 88.5 3.0 (0.9–5.1)
Yes 34 11.5 14.7 (2.5–26.8)
Dyslipidemia(n=296) 0.071a
No 223 75.3 3.1 (0.8–5.4)
Yes 73 24.7 8.2 (1.8–14.5)
Bodymassindex(kg/m2)(n=296) 0.364b
≤24.9 113 38.1 3.5 (0.8–6.9)
25–29.9 124 41.9 4.0 (0.5–7.5)
≥30 59 20 6.7 (0.1–13.2)
Smoking(n=296) 0.053a
Neversmoked 167 56.4 2.3 (0.5–4.7)
Previousand/orcurrentsmokers 129 43.6 6.9 (2.5–11.4)
Physicalleisureactivity(n=288) 0.214a
Neverpracticed 114 39.6 3.4 (0.7–6.1)
Practicedand/orpractices 174 60.4 6.1 (1.6–10.5)
Positivefamilyhistory(n=296) 0.136a
No 169 57.1 2.9 (0.3–5.5)
Yes 127 42.9 6.2 (2.0–10.5)
Diseaseduration(n=296) 0.001a
0–10years 175 59.1 1.1 (0.4–2.7)
≥11years 121 40.9 9.0 (3.9–14.2)
Presenceofrheumatoidfactor(n=266) 0.603a
0–60(negative,orlowtiters) 164 61.6 4.8 (1.5–8.2)
≥61(hightiters) 102 38.4 4.9 (0.6–9.1)
a Fischer’sexacttest.
b Wald’slineartrendtest.
relatedtoRA,durationofdiseaseover10yearswastheonly variabletodemonstrateastatisticallysignificantassociation (Table1).
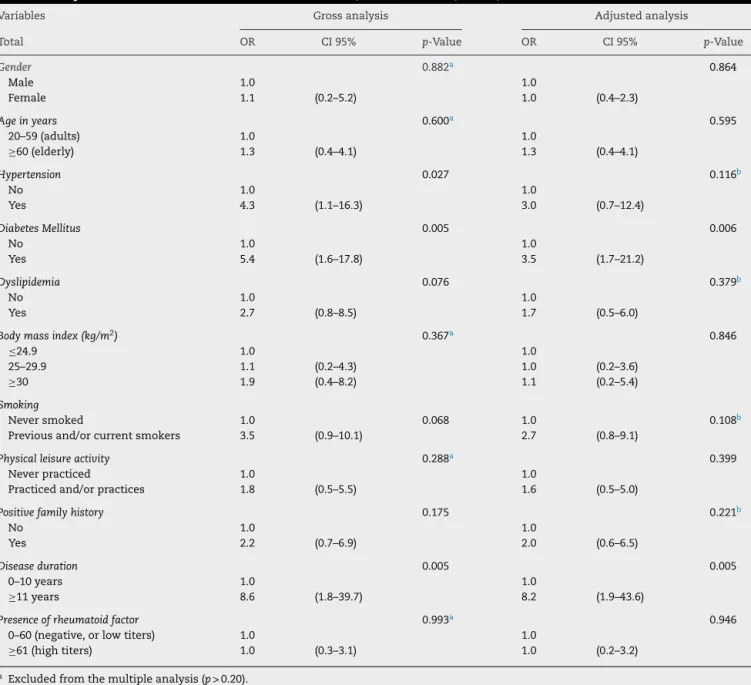
Inthegrossanalysis,it wasverifiedthatthedependent variablepresentedatendency ofassociationwith
dyslipid-emia and smoking; on the other hand, significance was
observedwithhypertension,diabetes mellitus,and disease duration.Intheadjustedanalysis,thevariablehypertension lostthepower ofassociation;thus,itwassuppressedfrom thefinalmodel,composedofdiabetesmellitusanddisease duration.Thesetwovariablespresented,respectively,3.5-and 8.2-fold increases in the chance of showing the outcome, comparedtonon-diabeticpatientswithlessthan10yearsof disease(Table2).Together,thesetwovariablesestablisheda coefficientofdeterminationof17%.
Discussion
ThestudyidentifiedagreaterchanceofMIdefinedbycardiac catheterization forangioplastyor stentimplantationorfor coronaryarterybypassgraftinginRApatientswithdiabetes mellitusandover10yearsofdisease.
InBrazil,thisisthefirststudytoestablishtheprevalenceof MI(4.4%)inthispopulation.Previousstudieshaveshownthat
European countrieshave aprevalence between2% (United
Table2–Grossandadjustedlogisticregressionanalysisofpatientswithacutemyocardialinfarctionandindependent variablesinpatientswithrheumatoidarthritis.Blumenau,SantaCatarina,Brazil,2014.
Variables Grossanalysis Adjustedanalysis
Total OR CI95% p-Value OR CI95% p-Value
Gender 0.882a 0.864
Male 1.0 1.0
Female 1.1 (0.2–5.2) 1.0 (0.4–2.3)
Ageinyears 0.600a 0.595
20–59(adults) 1.0 1.0
≥60(elderly) 1.3 (0.4–4.1) 1.3 (0.4–4.1)
Hypertension 0.027 0.116b
No 1.0 1.0
Yes 4.3 (1.1–16.3) 3.0 (0.7–12.4)
DiabetesMellitus 0.005 0.006
No 1.0 1.0
Yes 5.4 (1.6–17.8) 3.5 (1.7–21.2)
Dyslipidemia 0.076 0.379b
No 1.0 1.0
Yes 2.7 (0.8–8.5) 1.7 (0.5–6.0)
Bodymassindex(kg/m2) 0.367a 0.846
≤24.9 1.0 1.0
25–29.9 1.1 (0.2–4.3) 1.0 (0.2–3.6)
≥30 1.9 (0.4–8.2) 1.1 (0.2–5.4)
Smoking
Neversmoked 1.0 0.068 1.0 0.108b
Previousand/orcurrentsmokers 3.5 (0.9–10.1) 2.7 (0.8–9.1)
Physicalleisureactivity 0.288a 0.399
Neverpracticed 1.0 1.0
Practicedand/orpractices 1.8 (0.5–5.5) 1.6 (0.5–5.0)
Positivefamilyhistory 0.175 0.221b
No 1.0 1.0
Yes 2.2 (0.7–6.9) 2.0 (0.6–6.5)
Diseaseduration 0.005 0.005
0–10years 1.0 1.0
≥11years 8.6 (1.8–39.7) 8.2 (1.9–43.6)
Presenceofrheumatoidfactor 0.993a 0.946
0–60(negative,orlowtiters) 1.0 1.0
≥61(hightiters) 1.0 (0.3–3.1) 1.0 (0.2–3.2)
a Excludedfromthemultipleanalysis(p>0.20).
b Excludedfromthefinalmodel(p>0.05).
CVDlimitedtoLatinAmericancountriesfoundamore impor-tantprevalence(9%)ofcoronaryarterydisease.24InOceania, astudyusingthehospitaldatabaseofthecityofChristchurch establishedaprevalenceof8.3%.15
TheCORONNA10studyfoundasignificantdifferenceinthe riskofischemiceventsamongwomen(RR3.1)versusmen(RR 6.5).Thesampleconsistedof75%ofwomen,which differs fromourstudy,with83%ofwomen.Thiscouldexplainthe differenceinresultsbetweengenders.Theagefactorshowed atendencyofgreaterchanceamongtheelderly,butwithout significance.In this study,resultswere obtainedthat were commontothoseintheQUEST-RAstudy,12which,afterthe multivariateanalysisforMI,showednodifferenceinrelation toage.
Amongthetraditionalriskfactors,patientswithahistory ofhypertensionordyslipidemiadidnotshowagreaterchance
ofMIbecause,aftertheanalysisadjustedforgenderandage in the final model, theylost an association withoutcome, althoughthisassociationwaspointedoutbyother interna-tionalstudies.25,26
Diabetes mellitus presents a direct association with an ischemicevent,afindingalsoobservedinotherstudies.12,25 Asystemicreviewandmeta-analysisontheimpactof car-diovascularriskfactorsforMIinpatientswithRAperformed in 2014indicated that diabetic individuals demonstrated a propensity 1.9 times higher versus non-diabetic patients,26 while inthe present study a 3.5 timeshigher chance was found.
outcome.28Theinvestigatorsfoundthattherewasno associ-ationwithCVD,afindinginlinewiththeresultsofourstudy. Therewasaprevalenceof43%forpositivefamilyhistoryinthe sample,butwithnostatisticalsignificancewiththeoutcome, whiletwootherstudiesindicatedanopposedrelationship.29,30 Patientswithdiseasedurationover10yearshadan8.2-fold higherchanceofMIversuspatientswithashorterduration oftheirdisease.Thisassociationwas maintainedafterthe adjustedanalysisandremainedinthefinalmodel.AJapanese studyincludingafollow-upof571patientsinauniversity hos-pitaloveradecadeconcludedthatdiseaseduration(>10years) wasanindependentriskfactorforcardiovascularevents.31 Thisfindingresultsfromthelongerdurationofthe inflam-matoryprocessforthegenerationofconsequencessuchas atherosclerosisandendothelialdysfunction.32 Ontheother hand,astudyconductedintheNetherlandsdidnotindicate adifferenceintheriskforanischemiceventduetoadisease durationoflessthanorgreaterthan10years.33
Inthisstudy,thevalueoftherheumatoidfactor(RF)inhigh titerswasusedasamarkerofpoorprognosis(RF>60),because RFisapredictorofcardiovasculardisease34andalsobecause it could promote instability and rupture of atherosclerotic plaqueintothecoronaryartery.35Somestudieshaveshown thatthe presenceofRF inbothnon-diseasedindividuals36 and in patients with RA37 confers a higher chance of MI. However,theresultsofthisstudydidnotshowany associ-ationofRFwiththeoutcome,asalreadyindicatedinanother study.14
In the present study, some limitations must be taken
intoaccount.Thecross-sectionaldesignofthestudymakes
it impossible to determine cause and effect between the
exploratoryvariablesandtheoutcome.Basedontheresults obtained, the possibility of reverse causality, characteristic incross-sectionalstudies, ishighlighted.Another factor to consideristhepossibility ofmemory biasinthecollection
ofsome information,which is attenuated bythe common
characteristicofRAbeingachronicillness.Finally,the self-reporteddataoncomorbiditieshavenotbeenconfirmedby aphysician.On theother hand,health surveysrevealthat theinformationobtainedonthe prevalenceofchronic
dis-easespresentsgoodagreement,whencomparedtomedical
recordsorclinicalexams,especiallyforsomechronicdiseases suchashypertensionanddiabetesmellitus(DM).38,39Itshould furtherbeconsideredthat thedatarelatedtoRAwere col-lectedaccordingtotheEuropeanLeagueAgainstRheumatism (EULAR)recommendationsforannualdetectionand monitor-ingforcardiovascularrisk.40
ThisisthefirstBrazilianstudytoestablishaprevalenceof MIamongRApatients.Amongthetraditionalriskfactors, dia-betesmellitus,andamongfactorsrelatedtoRA,disease dura-tion, were the associated variables. New population-based studies are needed inorder toincrease the consistency of informationoncoronaryarterydiseaseinRApatientsandalso toinvestigateassociatedfactorsinotherBrazilianregions.
Funding
Fundac¸ãodeAmparoàPesquisadoEstadodeSãoPaulo, pro-cessFAPESP2013/12979-1.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ToDrs.AnaMariaGallo,JoãoEliasdeMouraJúniorand Jeron-imoS.Benites Júnior,therheumatologistswhocontributed withpatientstoobtainthestudysample.
r
e
f
e
r
e
n
c
e
s
1.KayJ,UpchurchKS.ACR/EULAR2010Rheumatoidarthritis classificationcriteria.Rheumatology.2012;51Suppl.6:5–9. 2.GuilleminF,SarauxA,GuggenbuhlP,RouxCH,FardelloneP,
LeBihanE,etal.PrevalenceofrheumatoidarthritisinFrance: 2001.AnnRheumDis.2005;64:1427–30.
3.CrossM,SmithE,HoyD,CarmonaL,WolfeF,VosT,etal.The globalburdenofrheumatoidarthritis:estimatesfromthe globalburdenofdisease2010study.AnnRheumDis. 2014;73:1316–22.
4.GabrielSE.Theepidemiologyofrheumatoidarthritis.Rheum DisClinNorthAm.2001;27:269–81.
5.MarquesNJF,Gonc¸alvesET,BarrosEFO,CunhaMFL, RadominskiS,OliveiraSM,etal.Estudomulticêntricoda prevalênciadaartritereumatoidedoadultoemamostrasda populac¸ãobrasileira.RevBrasReumatol.1993;33:169–73. 6.SennaER,DeBarrosAL,SilvaEO,CostaIF,PereiraLV,Ciconelli
RM,etal.PrevalenceofrheumaticdiseasesinBrazil:astudy usingtheCOPCORDapproach.JRheumatol.2004;31:594–7. 7.LévyL,FautrelB,BarnetcheT,SchaeverbekeT.Incidenceand
riskoffatalmyocardialinfarctionandstrokeeventsin rheumatoidarthritispatients.Asystematicreviewofthe literature.ClinExpRheumatol.2008;26:673–9.
8.Maradit-KremersH,CrowsonCS,NicolaPJ,BallmanKV,Roger VL,JacobsenSJ,etal.Increasedunrecognizedcoronaryheart diseaseandsuddendeathsinrheumatoidarthritis:a population-basedcohortstudy.ArthritisRheum. 2005;52:402–11.
9.BergströmU,JacobssonLT,TuressonC.Cardiovascular morbidityandmortalityremainsimilarintwocohortsof patientswithlong-standingrheumatoidarthritisseenin1978 and1995inMalmö,Sweden.Rheumatology(Oxford). 2009;48:1600–5.
10.SolomonDH,KremerJ,CurtisJR,HochbergMC,ReedG,Tsao P,etal.Explainingthecardiovascularriskassociatedwith rheumatoidarthritis:traditionalriskfactorsversusmarkers ofrheumatoidarthritisseverity.AnnRheumDis.
2010;69:1920–5.
11.DougadosM,SoubrierM,AntunezA,BalintP,BalsaA,Buch MH,etal.Prevalenceofcomorbiditiesinrheumatoidarthritis andevaluationoftheirmonitoring:resultsofan
international,cross-sectionalstudy(COMORA).AnnRheum Dis.2014;73:62–8.
12.NaranjoA,SokkaT,DescalzoMA,Calvo-AlénJ,
Hørslev-PetersenK,LuukkainenRK,etal.Cardiovascular diseaseinpatientswithrheumatoidarthritis:resultsfrom theQUEST-RAstudy.ArthritisResTher.2008;10:R30.
14.HolmqvistME,WedrénS,JacobssonLT,KlareskogL,NybergF, Rantapää-DahlqvistS,etal.Rapidincreaseinmyocardial infarctionriskfollowingdiagnosisofrheumatoidarthritis amongstpatientsdiagnosedbetween1995and2006.JIntern Med.2010;268:578–85.
15.KhanEA,StampLK,O’DonnellJL,ChapmanPT.
Cardiovascularmorbidityinrheumatoidarthritispatientsin NorthCanterbury,NewZealand1999–2008.IntJRheumDis. 2013;16:19–23.
16.KaplanMJ.Cardiovascularcomplicationsofrheumatoid arthritis:assessment,prevention,andtreatment.RheumDis ClinNorthAm.2010;36:405–26.
17.delRincónID,WilliamsK,SternMP,FreemanGL,EscalanteA. Highincidenceofcardiovasculareventsinarheumatoid arthritiscohortnotexplainedbytraditionalcardiacrisk factors.ArthritisRheum.2001;44:2737–45.
18.Tiippana-KinnunenT,KautiainenH,PaimelaL,Leirisalo-Repo M.Co-morbiditiesinFinnishpatientswithrheumatoid arthritis:15-yearfollow-up.ScandJRheumatol.2013;42:451–6. 19.KapetanovicMC,LindqvistE,SimonssonM,GeborekP,Saxne
T,EberhardtK.Prevalenceandpredictivefactorsof comorbidityinrheumatoidarthritispatientsmonitored prospectivelyfromdiseaseonsetupto20years:lackof associationbetweeninflammationandcardiovascular disease.ScandJRheumatol.2010;39:353–9.
20.ProgramadasNac¸õesUnidas–PNUD.Atlasdo
DesenvolvimentoHumanonoBrasil2003.Accessed11/13. Availableat:http://www.pnud.org.br/atlas.
21.InstitutoBrasileirodeGeografiaeEstatística-IBGE.Sinopsedo CensoDemográficode2010/2011.Accessed11/13.Available at:http://www.ibge.gov.br/home/estatistica/populacao/ censo2010.
22.PanafidinaTA,KondratyevaLV,GerasimovaEV,Gorbunova YN,PopkovaTV,NasonovEL.Characteristicsand
cardiovascularcomorbiditiesinpatientswithrheumatoid arthritisinalocalpatientcohortinRussia.AnnRheumDis. 2013;72Suppl.3:A865–6.
23.Villafrádez-DíazM,Santiago-CasasY,Nieves-PlazaM, MoralesM,RodríguezV,RíosG,etal.Associationoftheuseof statinswithdiseaseactivityandfunctionalstatusinPuerto Ricanswithrheumatoidarthritis.PRHealthSciJ.2014;33:3–8. 24.Sarmiento-MonroyJC,Amaya-AmayaJ,Espinosa-SernaJS,
Herrera-DíazC,AnayaJM,Rojas-VillarragaA.Cardiovascular diseaseinrheumatoidarthritis:asystematicliteraturereview inLatinAmerica.Arthritis.2012;371909:1–17.
25.ChungWS,LinCL,PengCL,ChenYF,LuCC,SungFC. Rheumatoidarthritisandriskofacutemyocardialinfarction– anationwideretrospectivecohortstudy.IntJCardiol. 2013;168:4750–4.
26.BaghdadiLR,WoodmanRJ,ShanahanEM,MangoniAA.The impactoftraditionalcardiovascularriskfactorson cardiovascularoutcomesinpatientswithrheumatoid arthritis:asystematicreviewandmeta-analysis.PLOSONE. 2015;10:1–18.
27.GonzalezA,MaraditKremersH,CrowsonCS,BallmanKV, RogerVL,JacobsenSJ,etal.Docardiovascularriskfactors conferthesameriskforcardiovascularoutcomesin rheumatoidarthritispatientsasinnon-rheumatoidarthritis patients?AnnRheumDis.2008;67:64–9.
28.AssousN,TouzéE,MeuneC,KahanA,AllanoreY.
Cardiovasculardiseaseinrheumatoidarthritis:single-center hospital-basedcohortstudyinFrance.JointBoneSpine. 2007;74:66–72.
29.Rojas-VillarragaA,Ortega-HernandezOD,GomezLF,Pardo AL,López-GuzmánS,Arango-FerreiraC,etal.Riskfactors associatedwithdifferentstagesofatherosclerosisin Colombianpatientswithrheumatoidarthritis.Semin ArthritisRheum.2008;38:71–82.
30.Ortega-HernandezOD,Pineda-TamayoR,PardoAL, Rojas-VillarragaA,AnayaJM.Cardiovasculardiseaseis associatedwithextra-articularmanifestationsinpatients withrheumatoidarthritis.ClinRheumatol.2009;28: 767–75.
31.MasudaH,MiyazakiT,ShimadaK,TamuraN,MatsudairaR, YoshiharaT,etal.Diseasedurationandseverityimpactson long-termcardiovasculareventsinJapanesepatientswith rheumatoidarthritis.JCardiol.2014;64:366–70.
32.FullLE,RuisanchezC,MonacoC.Theinextricablelink betweenatherosclerosisandprototypicalinflammatory diseasesrheumatoidarthritisandsystemiclupus erythematosus.ArthritisResTher.2009;11:217–27.
33.ArtsEE,FransenJ,denBroederAA,PopaCD,vanRielPL.The effectofdiseasedurationanddiseaseactivityontheriskof cardiovasculardiseaseinrheumatoidarthritispatients.Ann RheumDis.2015;74:998–1003.
34.HeliövaaraM,AhoK,KnektP,AromaaA,MaatelaJ,Reunanen A.Rheumatoidfactor,chronicarthritisandmortality.Ann RheumDis.1995;54:811–4.
35.MedeirosAM,vonMühlenCA,GidlundMA,BodaneseR, GottliebMG,BodaneseLC.AntibodiesagainstoxLDLand acutecoronarysyndrome.ArqBrasCardiol.2010;95:47–54. 36.LiangKP,KremersHM,CrowsonCS,SnyderMR,Therneau
TM,RogerVL,etal.Autoantibodiesandtheriskof cardiovascularevents.JRheumatol.2009;36:2462–9. 37.GabrielSE.Cardiovascularmorbidityandmortalityin
rheumatoidarthritis.AmJMed.2008;121:S9–14.
38.MartinLM,LeffM,CalongeN,GarrettC,NelsonDE.Validation ofself-reportedchronicconditionsandhealthservicesina managedcarepopulation.AmJPrevMed.2000;18:215–8. 39.HaapanenN,MiilunpaloS,PasanenM,OjaP,VuoriI.
Agreementbetweenquestionnairedataandmedicalrecords ofchronicdiseasesinmiddle-agedandelderlyFinnishmen andwomen.AmJEpidemiol.1997;145:762–9.