w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Anti-Müllerian
hormone
levels
as
a
predictor
of
ovarian
reserve
in
systemic
lupus
erythematosus
patients:
a
review
夽
Andrese
Aline
Gasparin
a,∗,
Rafael
Mendonc¸a
da
Silva
Chakr
a,
Claiton
Viegas
Brenol
b,
Penélope
Ester
Palominos
a,
Ricardo
Machado
Xavier
b,
Lucian
Souza
c,
João
Carlos
Tavares
Brenol
b,
Odirlei
André
Monticielo
b aRheumatologyDepartment,HospitaldeClínicas,PortoAlegre,RS,BrazilbRheumatologyDepartment,UniversidadeFederaldoRioGrandedoSul,PortoAlegre,RS,Brazil cFaculdadedeMedicina,UniversidadeFederaldoRioGrandedoSul,PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29January2014 Accepted2May2014
Availableonline7January2015
Keywords:
Anti-Müllerianhormone Ovarianreserve
Systemiclupuserythematosus
a
b
s
t
r
a
c
t
Theanti-Müllerianhormone(AMH)issecretedfromgranulosacellsofgrowingovarian fol-liclesandappearstobethebestendocrinemarkercapableofestimatingovarianreserve. Systemiclupuserythematosus(SLE)isanautoimmunediseasethatpredominantlyaffects womenofreproductiveageandmaynegativelyaffecttheirfertilityduetodiseaseactivity andthetreatmentsused.Recently,severalstudiesassessedAMHlevelstounderstandthe realimpactofSLEanditstreatmentonfertility.
©2014ElsevierEditoraLtda.Allrightsreserved.
Hormônio
anti-Mülleriano
como
preditor
de
reserva
ovariana
em
pacientes
lúpicas:
uma
revisão
Palavras-chave:
Hormônioanti-Mülleriano Reservaovariana
Lúpuseritematososistêmico
r
e
s
u
m
o
Ohormônioanti-Mülleriano(HAM)ésecretadoapartirdascélulasdagranulosados folícu-losovarianosemcrescimentoepareceseromelhormarcadorendócrinocapazdeestimara reservaovariana.Olúpuseritematososistêmico(LES)éumadoenc¸aautoimunequeacomete predominantementemulheresemidadereprodutivaepodeafetarnegativamentesua fer-tilidadepelaatividadedadoenc¸a,bemcomopelostratamentosusados.Conheceroreal impactodoLESedeseutratamentonafertilidadevemsendooobjetivodeestudosrecentes, osquaistêmusadooHAMparaessefim.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
夽
DepartmentofRheumatologyofHospitaldeClínicasofPortoAlegre. ∗ Correspondingauthor.
E-mail:[email protected](A.A.Gasparin). http://dx.doi.org/10.1016/j.rbre.2014.05.008
Introduction
Bettertreatment conditionsand themanagement of infec-tions havenotonlycontributed to increasethe survivalof systemiclupus erythematosus(SLE) patients, but also pro-videdbetterqualityoflife,sonowadaysmostofthesepatients areabletoworknormally.Withtheincreasingparticipationof womeninthelabormarket,themomenttheydecidetohave theirfirstchildhasbeenincreasinglypostponed.Female fertil-itystartstodeclineatthebeginningofthethirddecadeoflife andcouldbehamperedinSLEpatientsduetodisease activ-ityanditstreatment.Thismakesfertility-relatedproblemsin suchpatientsmoreandmoreimportant,hence theneedto haveeffectivemarkerstopredictovarianreserve.
Anti-Müllerian
hormone
as
an
ovarian
reserve
marker
Around the twentieth week of pregnancy, the number of oocytesreachesamaximumofsixtosevenmillionand,in acontinuous process ofatresia/apoptosis, onlyoneto two millionfolliclesreachtheneonatalperiod.1Onlyoogoniathat
entermeiosiswillsurviveatresiainthefetalovarybeforebirth. Atmenarche,around 300thousandare viable.Womenuse around500primordialfolliclesduringthereproductiveyears. Atmenopause,theovaryisformedbydensestromaandrare remainingscatteredoocytes.2
Folliculargrowthstartsinthefetus,inacontinuous pat-tern,and is related tothe total massoffollicles and with factorsreleasedbyatreticovarianfollicles.Folliculargrowth cyclesandsubsequentatresiainitiatebeforebirthand con-tinue through the reproductive years. The viability of the oocytedeclines in olderwomeninreproductive age before they present any measurable serum or intrafollicular hor-moneconcentrationdecrease.3Menopauseisassociatedwith
amarkeddeclineinthenumberofoocytes,whichisattributed totheprogressiveatresiaoftheoriginalpoolofoocytes. How-ever,evidencesofcompletedepletionofoocytesarecurrently limited.3
Theanti-Müllerianhormone(AMH),alsocalled Müllerian-inhibiting substance, is a polypeptide, member of the transforminggrowthfactor-(TGF)family.Itisinvolvedin thesexualdifferentiationofthemaleembryo,inducing regres-sion ofthe Müllerian duct, embryologicalprecursor ofthe female reproductive tract.4 In female individuals, it starts
expressinginthefetalovaryafterthe36thweekofpregnancy. Itisexpressedbythegranulosacellsofgrowingovarian fol-licles:primary,secondary, preantralandsmallantral,being producedathigherlevelsbythelasttwo.5 Ithastwomain
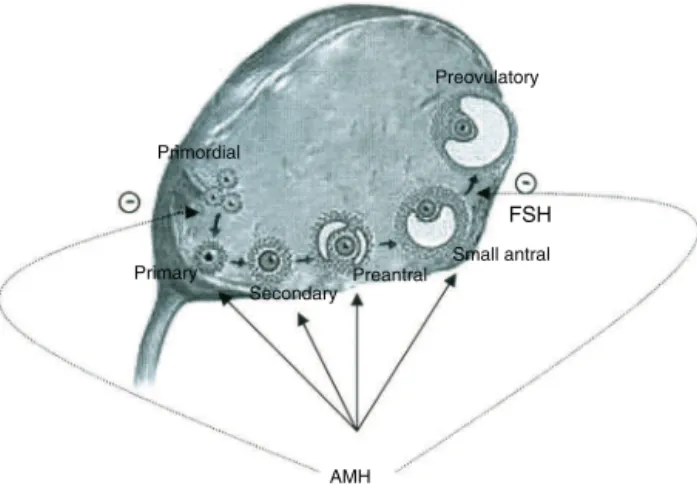
mechanismsofactionintheovary:inhibitstheinitial recruit-mentofprimaryfolliclesfromprimordialfollicles,andinhibits the sensitivityofantralfollicles to follicle-stimulating hor-mone (FSH) during cyclical recruitment (Fig. 1). The AMH prevents the premature depletion of follicles.6 Despite the
“anti”prefix,theAMHhasnoroleintheproductionof anti-bodies.
Theterm“ovarianreserve”describesthenumberand qual-ityoftheremainingoocytesintheovaries. Theamountof
Preovulatory
Primordial
Secondary Preantral Primary
AMH
FSH
Small antral
Fig.1–Anti-Müllerianhormone(AMH)and
folliculogenesis.AMHissecretedbygrowingfolliclesand secretionincreasesoverfolliculardevelopment.Highest levelsaresecretedbypreantralandsmallantralfollicles. AMHinhibitstheinitialrecruitmentofprimaryfollicles fromthepoolofprimordialfolliclesandreducesthe sensitivityofantralfolliclestofollicle-stimulatinghormone (FSH)duringrecruitment.
remainingprimordialfolliclesappearstocorrelatewiththe numberofgrowingfollicles.Asonlygrowingfolliclesproduce AMH,theirplasmalevelsreflecttheamountofremaining pri-mordialfollicles.7 Studiesinmice8 and chimpanzees9 have
shownstrongcorrelationbetweenthelevelsofAMHandthe numberofprimordialfollicles.
Othercurrentteststoestimatetheovarianreserveinclude hormone(FSH,estradiol,inhibinB)andsonographicmarkers (antralfollicle countandmeasurementofovarianvolume). Thesetestsdirectorindirectlyreflectthenumberofremaining antral follicles.Antralfollicle countisadirectsonographic measurement. In the early follicular phase, the levels of inhibinBandestradiolareconsidereddependentonthe num-ber ofantral follicles.FSH levels are regulated bynegative feedbackofthesetwogranulosacellproducts,sothey indi-rectlyreflectthepoolofantralfollicles.Theage-relateddecline of oocytes leadsto reduced levels of estradiol and inhibin Band,consequently,theincreaseofFSH.10Comparedwith
thesehormonalmarkers,AMHplasmalevelsappearto asso-ciatebetterwiththelongitudinaldeclineofoocytes/follicles overtime,evenbeforetheoccurrenceofirregularcycles.11As
opposedtothecyclicfluctuationsofFSH,estradiolandinhibin B,theAMHhassmallorabsentintracyclicfluctuation. There-fore,theAMHreflectsthecontinuedgrowthofsmallfollicles. AMHlevelsarerelativelyunaffectedbyconditionsthat sup-press late stagesofFSH-dependent follicular development, likepregnancy,12theuseofhormonalcontraceptives13andthe
treatmentwithGnRHagonists.Inadditiontothat,theAMH doesnotappeartobeaffectedbythebodymassindex(BMI)or smoking.14ThepredictivevalueoftheAMHtoestimate
Table1–Summaryofpublishedarticles.
Study Design Follow-up Mainresults
Lawrenzetal.28 Case–control(33patientsin eachgroup)
February2009toMay2010, Germany
SLEpatientshavesignificantlylowerAMH levelsthanhealthycontrols.
Moketal.29 Cohortstudy,216SLE patients
JunetoOctober,2009,China ThemeanAMHlevelwassignificantly lowerinpatientswhohadbeen
previouslyexposedtocyclophosphamide. Moreletal.30 Case–control(56patientsin
eachgroup)
2012,France LowAMHlevelsinSLEpatients,with significantdecreaseassociatedwithage andprioruseofcyclophosphamide. Malheiroetal.31 Case–control(27patientsin
eachgroup)
Brazil Themeanvaluesofovarianreservewere
similarinbothgroups.SLEpatients showedwiderdistributionofAMHvalues.
TheAMHappearstobeanearly,reliableanddirect pre-dictor of declining ovarian function. However, there is no consensusregardingappropriatethresholdvalues.Literature datashowedsignificantdispersionofserumAMH concentra-tionsincomparablepopulationsobtainedfromtwodifferent ultrasensitiveimmunoassaysavailableinthemarket–AMH BeckmanCoulterELISAandAMHDiagnosticSystemlaboratories (DSL)ELISA.Apreviousstudy foundAMHlevelsaround 4.6 timeslowerwiththeDSLkit,showingthatthecut-offvalue variesaccording to theassay being used.16 Instudies that
assessedthesuccessrateofinvitrofertilization,serumAMH levelsbelow0.5ng/mLstronglysuggestedfolliculardepletion, whileserumlevels≥1.26ng/mLwereconsistentwithagood ovarianreserve.15,17
Howcanlupussystemicerythematosusimpairfertility?
Infertilityisdefinedasthefailuretoconceiveafter12months ofregularunprotectedintercourse.Autoimmunitycan inter-fere with many aspects associated with fertility, causing, forexample,tubalfunctionchanges,ovarianfailure,embryo implantationfailureandmiscarriages.
Acase–controlstudyconductedin2009inFinlandassessed thereproductivehistoryofSLEwomencomparedwithhealthy controls. The authors found no difference in the mean age atmenarcheand the frequencyof infertility.However, menopauseoccurredearlieramongSLEpatients.18
Around10–30%ofwomenwithprematureovarianfailure (POF) have a concomitant autoimmune disease.19
Autoim-mune reactions against ovaries can be general or partial, leading to a fluctuating course of POF. The evidence of an autoimmune basis forPOF is givenby the presence of antibodiesagainststeroid-producingcellsinaround80%of patientsandoophoritiswithinfiltrationofCD4+andCD8+T lymphocytes.20
It is suggested that fertility in some patients could be reduced due to menstrual irregularities and anovulatory cycles during disease activity and the administration of highdosesofcorticosteroids.21Atleast53%ofSLEpatients
under the age of 40 present some degree of menstrual irregularity,while menstrualalterations are more frequent among patients with greater disease activity.22 The
ovar-ianfunction can bereduced by autoimmune oophoritis in SLE, leading to POF, while a reduced ovarian reserve is associatedwithreducedAMH levels.23 Lupusnephritiscan
resultinendstagerenal disease andamenorrhea together
withhyperprolactinemia.24AroundonethirdofSLEwomen
presentantiphospholipidantibodies,whichcouldexplainthe SLE/miscarriageassociation.25
TherapeuticagentsprescribedtotreatSLEmayimpair fer-tility,suchasisthecaseofhighdoses ofsteroids,NSAIDs and cyclophosphamide, which, in particular, influence the ovarianfunction,especiallyatolderages.Astudypublished in 2006found 39% of prevalenceofovarian failure among patients treated with cyclophosphamide under the age of 30 and 59% of patients aged 30–40.26 A cohort study
per-formed from September 2010 to July 2011 in the United States,comparingthereproductivehistoryofyoungwomen withrheumaticdiseases,withorwithoutpriorexposureto cyclophosphamide,concludedthatmorewomenwithprior exposure tocyclophosphamide had amenorrhea, infertility andnulliparity.27
OvarianreserveassessmentinpremenopausalSLE patientsthroughanti-Müllerianhormone– state-of-the-art
Few studies using AMH to assess ovarian reserve in SLE patientshavebeen publishedtodate.Acase–controlstudy conductedinGermanyfromFebruary2009toMay2010 ana-lyzed the influence of SLE in ovarian reserve considering diseaseactivityanddiseaseduration.Theovarianreservewas determinedthroughserumAMHlevelsin33premenopausal SLEpatientswithoutpriorexposuretocyclophosphamideand in33age-matchedcontrolpatients.AMHlevelsinSLEpatients weresignificantlylowerthaninhealthycontrols.No signifi-cantdifferenceswerefoundbetweenthegroupsinrelationto thenumberofchildrenandabortions,andtherewasno corre-lationbetweentheAMHlevelandthedurationofthedisease orSLEDAIasadiseaseactivityindex.Despitepresentingmild diseaseactivity,theovarianreserveofSLEpatientswas signif-icantlysmallerthanthatofage-matchedhealthycontrols.28
Acase–controlstudy conductedin2012inFrancefound low AMH levels in SLE patients with significant decrease associatedwithageandprioruseofcyclophosphamide. Nev-ertheless,theriskofpregnancyfailurewaslow(15.8%).The prioruseofcyclophosphamidewasa predictorwhileAMH levelswerenot.30
Acase–controlstudywithasmallnumberofpatients(27in eachgroup)conductedinBrazilfoundsimilarmeanovarian reservevaluesinbothgroups.However,SLEpatientsshowed broaderdistributionofAMHlevels.Theovarianfunctionwas morecompromisedinpatientswithhighercumulativedose ofcyclophosphamideandhigherdiseasedamagescore.31The
summaryofthemainarticlespublishedtodatecanbeseen inTable1.
Conclusion
AMHhasbeenincreasinglyreportedasareliablemarkerof ovarianreserve.Theroleofcyclophosphamideasthecauseof infertility,evidencedbylowerlevelsofAMHinage-matched andpreviouslyexposedpatients,iswellestablished.However, furtherstudies,withlargernumberofpatients,arenecessary toassessdifferences inthe ovarianreserveofSLEpatients whencomparedwithcontrols,andtheimplications of dis-easeactivityonthefertilityofthesepatients.Agentswithless ovariantoxicitycouldbeofferedtopatientswithreducedAMH levelsandtothosewhowishtobecomepregnant.
Funding
FundodeIncentivoàPesquisaeEventos(FIPE/HCPA),Brazil.
Conflict
of
interest
Theauthorsdeclarenoconflictofinterest.
r
e
f
e
r
e
n
c
e
s
1. PetersH,ByskovAG,GrinstedJ.Folliculargrowthinfetaland prepubertalovariesinhumansandotherprimates.JClin EndocrinolMetab.1978;7:469–85.
2. Freitas,Menke,Rivoir,Passos.Rotinasemginecologia.6thed. PortoAlegre:Artmed;2011.
3. RichardsonSJ,SenikasV,NelsonJF.Folliculardepletionduring themenopausaltransition:evidenceforacceleratedlossand ultimateexhaustion.JClinEndocrinolMetab.1987;65:1231–7. 4. LeeMM,DonahoePK.Mullerianinhibitingsubstance:a
gonadalhormonewithmultiplefunctions.EndocrRev. 1993;14:152–64.
5. LaMarcaA,StabileG,ArtenisioAC,VolpeA.Serum anti-Müllerianhormonethroughoutthehumanmenstrual cycle.HumReprod.2006;21:3103–7.
6. VisserJA,DeJongFH,LavenJS,ThemmenAP.Anti-Müllerian hormone:anewmarkerforovarianfunction.Reproduction. 2006;131:1–9.
7. FaddyMJ,GosdenRG,GougeonA,RichardsonSJ,NelsonJF. Accelerateddisappearanceofovarianfolliclesinmid-life: implicationsforforecastingmenopause.HumReprod. 1992;7:1342–6.
8.KevenaarME,MeerasahibMF,KramerP,VandeLang-Born BM,DeJongFH,GroomeNP,etal.Serumanti-Müllerian hormonelevelsreflectthesizeoftheprimordialfolliclepool inmice.Endocrinology.2006;147:3228–34.
9.ApptSE,ClarksonTB,ChenH,AdamsMR,ChristianPJ,Hoyer PB,etal.Serumanti-Müllerianhormonepredictsovarian reserveinamonkeymodel.Menopause.2009;16:597–601. 10.BurgerHG,CahirN,RobertsonDM.SeruminhibinsAandB
falldifferentiallyasFSHrisesinperimenopausalwomen.Clin Endocrinol(Oxf).1998;48:809–13.
11.DeVetA,LavenJS,DeJongFH,ThemmenAP,FauseBC. Anti-Müllerianhormoneserumlevels:aputativemarkerfor ovarianaging.FertilSteril.2002;77:357–62.
12.LaMarcaA,GiuliniS,OrvietoR,DeLeoV,VolpeA.
Anti-Müllerianhormoneconcentrationsinmaternalserum duringpregnancy.HumReprod.2005;20:1569–72.
13.LiHW,WongCy,YeungWS,HoPC,NgEH.Serum
anti-Müllerianhormonelevelisnotalteredinwomenusing hormonalcontraceptives.Contraception.2011;83:582–5. 14.ShawCM,StanczykFZ,EglestonBL,KahleLL,SpittleSC,
GodwinAK,etal.Serumanti-Müllerianhormoneinhealthy premenopausalwomen.FertilSteril.2011;95:2718–21. 15.BroekmansFJ,KweeJ,HendriksDJ.Asystematicreviewof
testspredictingovarianreserveandIVFoutcome.Hum Reprod.2006;12:685–718.
16.FréourT,MiralliéS,Bach-NgohouK,DenisM,BarrièreP, MassonD.Measurementofserumanti-Müllerianhormoneby BeckmanCoulterElisaandDSLElisa:comparisonand relevanceinassistedreproductiontechnology(ART).Clin ChimActa.2007;375:162–4.
17.GnothC,SchuringAN,FriolK,TiggesJ,MallmannP, GodehardtE.Relevanceofanti-Müllerianhormone measurementinaroutineIVFprogram.HumReprod. 2008;23:1359–65.
18.Ekblom-KullbergS,KautiainenH,AlhaP,HelveT,
Leirisalo-RepoM,JulkunenH.Reproductivehealthinwomen withsystemiclupuserythematosuscomparedtopopulation controls.ScandJRheumatol.2009;38:375–80.
19.NelsonLM.Clinicalpractice,primaryovarianinsufficiency.N EnglJMed.2009;360:606–14.
20.HoekA,SchoemakerJ,DrexhageHA.Prematureovarian failureandovarianautoimmunity.EndocrVer.1997;18:107–34. 21.GayedM,GordonC.Pregnancyandrheumaticdiseases.
Rheumatology(Oxf).2007;46:1634–40.
22.ShabanovaSS,AnanievaLP,AlekberovaZS,GuzovII.Ovarian functionanddiseaseactivityinpatientswithsystemiclupus erythematosus.ClinExpRheumatol.2008;26:436–41. 23.CarpHJA,SelmiC,ShoenfeldY.Theautoimmunebasesof
infertilityandpregnancyloss.JAutoimmun.2012;38:J266–74. 24.GomezF,DelaCuevaR,WautersJP,Lemarchand-BeraudT.
Endocrineabnormalitiesinpatientsundergoinglong-term hemodialysis.Theroleofprolactin.AmJMed.1980;68:522–30. 25.BizarroN,TonuttiE,VillaltaD,TampoiaM,TozzoliR.
Prevalenceandclinicalcorrelationof
anti-phospholipid-bindingproteinantibodiesin anticardiolipin-negativepatientswithsystemiclupus erythematosusandwomenwithunexplainedrecurrent miscarriages.ArchPatholLabMed.2005;129:61–8. 26.MangerK,WildtL,KaldenJR,MangerB.Preventionof
gonadaltoxicityandpreservationofgonadalfunctionand fertilityinYoungwomenwithsystemiclupuserythematosus treatedbycyclophosphamide:thePregostudy.Autoimmun Rev.2006;5:269–72.
27. HarwardLE,MitchellK,PieperC,CoplandS, Criscione-SchreiberLG,ClowseMEB.Theimpactof cyclophosphamideonmenstruationandpregnancyin womenwithrheumatologicdisease.Lupus.2013;22:81–6. 28.LawrenzJC,HenesM,HenesE,NeunhoefferM,SchmalzingT,
ovarianreserveinpremenopausalwomen:evaluationby usinganti-Müllerianhormone.Lupus.2011;20:1193–7. 29.MokCC,ChanPT,ToCH.Anti-Müllerianhormoneand
ovarianreserveinsystemiclupuserythematosus.Arthritis Rheum.2013;65:206–10.
30.MorelN,BachelotA,Ghillani-DalbinP,AmouraZ,GalicierL. Studyofanti-Müllerianhormoneandtherelationshipwith
subsequentprobabilityofpregnancyin112systemiclupus erythematosuspatientsexposedornottocyclophosphamide. The10thInternationalCongressonSLE.Lupus.2013;22:16. 31.MalheiroOB,RezendeCP,FerreiraGA,ReisFM,Federal