w w w . r b o . o r g . b r
Original
article
Experimental
trial
on
surgical
treatment
for
transverse
fractures
of
the
proximal
phalanx:
technique
using
intramedullary
conical
compression
screw
versus
lateral
compression
plate
夽
Daniel
Schneider
Ibanez
∗,
Fabio
Lucas
Rodrigues,
Rafael
Salmeron
Salviani,
Fernando
Augusto
Reginatto
Roberto,
Jose
Roberto
Pengo
Junior,
Marcio
Aurelio
Aita
LaboratóriodeEnsaiosMecânicoseMetalográficos(LEMM),Jaú,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17June2014 Accepted25August2014 Availableonline1August2015
Keywords:
Bonefixation
Internalfixationoffractures Handinjuries
Fingerinjuries
a
b
s
t
r
a
c
t
Objective:Tocomparethemechanicalparametersbetweentwomethodsforstabilization throughcompression:1.5mmaxialcompressionplateversusconicalcompressionscrew usedasanintramedullarytutor.
Methods:Polyurethanemodels(Sawbone®)thatsimulatedtransversefracturesofthe
prox-imalphalanxwereused.Themodelsweredividedintothreegroups:lateralplate,conical screwandnoimplant.
Results:Greater force was needed to result in fatigue in the synthesis using an intramedullaryplate.Thus,thismodelwasproventobemechanicallysuperiortothemodel withthelateralplate.
Conclusion: StabilizationusingtheAcutrak®screwfortreatingfracturesinthemodelused
inthistrialpresentsmechanicalresultsthatarestatisticallysignificantlysuperiortothose fromtheaxialcompressiontechniqueusingthelateralplate(AptusHand®).
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Ensaio
experimental
para
tratamento
cirúrgico
das
fraturas
transversas
da
falange
proximal
–
Técnica
com
parafuso
intramedular
cônico
de
compressão
versus
placa
de
compressão
lateral
Palavras-chave:
Fixac¸ãoóssea
Fixac¸ãointernadefraturas
r
e
s
u
m
o
Objetivo:Compararosparâmetrosmecânicosentredoismétodosdeestabilizac¸ãopor com-pressão:placadecompressãoaxialde1,5mmcomoparafusocônicodecompressãousado comotutorintramedular.
夽
WorkdevelopedintheLaboratóriodeEnsaiosMecânicoseMetalográficos(LEMM),Jaú,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.S.Ibanez).
http://dx.doi.org/10.1016/j.rboe.2014.12.009
Traumatismosdamão Traumatismosdosdedos
Métodos: Foramusadosmodelosde poliuretano(Sawbone®)quesimulama fraturada falangeproximaltransversa,divididosemtrêsgrupos(placalateral,parafusocônico,sem implante).
Resultados: Hánecessidadedeumamaiorforc¸apararesultarnafadigada síntesecom parafusointramedular.Comprova-se,assim,asupremaciamecânicadessesobreomodelo comaplacalateral.
Conclusão: Aestabilizac¸ãocomoparafusoAcutrak®,notratamentodasfraturasnomodelo adotadonesteensaio,apresentaresultadosmecânicossuperioreseestatisticamente sig-nificativosemcomparac¸ãocomatécnicadecompressãoaxialcomousodaplacalateral (AptusHand®).
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Fractureofthephalangesarefrequentinjuriesandaccount for6%ofallfractures.1,2 Theproximalphalanxisfractured morefrequentlythanthemiddleordistalphalanges.3,4
Indicationsforsurgicaltreatmentforthesefracturesneed to take into consideration the type of fracture line, the displacement between the fragment and the difficulty in maintainingclosedreductionofthefracture.3Theaimof sur-gicaltreatmentistorestoretheanatomyandfunctionofthe affectedfinger.4,5
Thetechniquesthathavebeendescribedrangefrom seek-ingrelativestability totheprincipleofabsolutestability. A combinationofmethodsissometimesnecessary,6 andthis dependsonthenatureofthefractureline,theavailabilityof implantsandthesurgeon’spreference.
Among the surgical complications, the following can be highlighted: joint stiffness, adherence and/or tearing of the extensor tendon,1 functional loss of the finger2 or, additionally, skewed consolidation, pseudarthrosis and osteomyelitis.5–7
Thesecomplicationsareoftencausedbypoorknowledge ofthebiomechanicsofthisorgan;anunfoundedbeliefthat allfracturesofthehandcanberesolvedthroughconservative treatment;orpoorcooperationfromthepatient.8
Inseekingtominimizethesecomplications,Mantovanni etal.9describedlateralpositioningoftheplateinwhichthe extensortendon wasleft untouched soasto avoidtendon adherenceandjointstiffness.Anotheroptionwouldbetouse theprincipleofanintramedullaryinternaltutor,10,11suchas aconicalcompressionscrew(Acutrak®),tobeplaced percuta-neously.Wedescribethisnoveltechniqueinthepresentstudy. Theobjectiveofthisstudywastocomparethemechanical parameters of two methods of stabilization through com-pression:a1.5mmaxialcompressionplateversusaconical compressionscrewusedasanintramedullarytutor.Bothof thesemethodswereusedonfracturesofthediaphysisofthe proximalphalanxthatfollowedatransverseline.
Methods
Thisstudy was conductedin the Mechanical and Metallo-graphicTestingLaboratory(LEMM), inthe city ofJaú,state
Fig.1–GroupImodelbeforethemechanicaltest.
Fig.2–GroupIImodelbeforethemechanicaltest.
ofSão Paulo,Brazil,inMay 2012.Thislaboratoryhas been certifiedbyINMETRO.
Fifteenpolyurethanemodelssimulatingtheproximal pha-lanx(Sawbone®),ofdimensions10mm
×8mm×60mmand density 40poundsper cubicfoot (lb/ft3)were used. Simple transversefractureswithasinglelineataninclinationofless than30◦weremade.12
Thesemodelsweredividedintothreegroups:fivemodels foreachgroupwithsynthesismaterial(groupsIandII);and threemodelsforagroupwithoutsynthesismaterial(group III).
GroupI–witha1.5mmcompressionplateandfour corti-calscrews(AptusHand®),placedinthelateralregionofthe model(Fig.1).
Group II – one conical compression screw (Acutrak®) of standardtype,positionedintramedullarily(Fig.2).
GroupIII–modelsofthephalanxwithoutanimplantand withoutafracture(Fig.3).
Placement technique for the lateral plate in the polyurethanemodel(Fig.1):
Placementof1.5mmplatepositionedlaterallyinthemodel and,afterreduction,placementoffourbicorticalscrews(two
Load
h
Test body
Support bearings
L
Load bearing
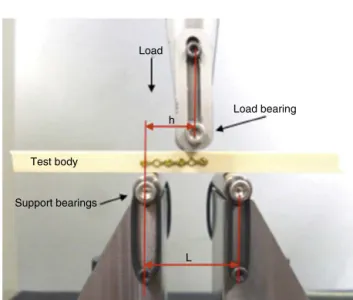
Fig.4–Illustrativeschematicphotooftheflexiontestwith load-bearingatthreepoints:distanceL:40mm;distanceh:
15mm;forceapplied:5mm.
distallyandtwoproximallytothefracturefocus)thatpromote compressionaxiallytothefractureline.
Placementtechniquefortheintramedullaryconical com-pressionscrewinthepolyurethanemodel(Fig.2):
Reductionofthefractureinthepolyurethanemodeland passageofthe guidewirefrom theupper face towardsthe lowerface,acrossthefracture.Thisisfollowedby measure-mentofthesizeoftheimplant,drillingofanopeninginboth corticesandinstallationofaconicalcompressionscrewjust belowtheuppersurfaceintheregionproximaltothefracture andadjacenttothedistallowersurfaceofthismodel.
Application ofthe mechanical test inthe polyurethane models:flexiontestatthreesupportpoints(Fig.4).
Thepolyurethanemodels(testbodies) wereplacedin a machine(EMIC apparatus,model DL10000)withthree con-tactpoints:oneloadbearingandtwosupportbearings.Inthis manner,theloadwasappliedsoastogenerateaconstantly increasingflexionforceuntilthesynthesismaterialreached fatigue.
Fig.5–Illustrativedetailedschematicphotooftheflexion testwithload-bearingatthreepoints:groupII.
120
100
80
60
40
20
0
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0
Deflection (mm)
Source: Mechanical and metallographic testing laboratory (LEMM)
Force/Load (N)
TB 1 TB 2 TB 3 TB 4 TB 5
Fig.6–Flexiontestcurves,withload-bearingatthree points,forgroupI.
GroupI–forceappliedfromabovetobelow,withthe com-pressionplatepositionedlaterally.
GroupII–forceappliedfromabovetobelow,withthe com-pression screwalso placedfrom above to below,inclined accordingtothetransversefractureline(Fig.5).
GroupIII–forceappliedfromabovetobelow,ontheentire testbody.
Inallthegroupsevaluated,thedistanceLbetweenthe sup-portbearingswasthesame.IngroupsIandII,theflexionforce appliedbytheloadbearingwaskeptconstantatadistanceh
of15mmfromthebeginningofthesynthesisandat5mm fromthefractureline.
All the data were sent for statistical analysis. The Kruskal–Wallistestwasusedandthesignificancelevelwas takentobe5%(0.050).TheStatisticalPackagefortheSocial Sciences (SPSS) software, version 21.0,was used to aid in obtainingtheresults.
The Kruskal–Wallis test was applied to ascertain the possible differences between the three groups, compared simultaneously,forthevariablesofinterest.
Results
Ingroup I(lateralcompression plate),themean maximum flexionforcewithstoodwas81.23N,witharangefrom97.13 to73.35N.Themeanrigidityunderflexionwas90.80N,with arangefrom116to70N(Table1andFigs.6and7).
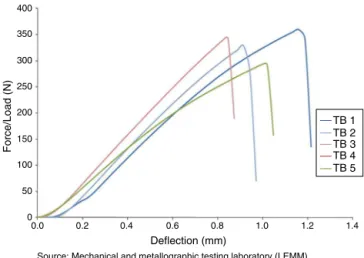
GroupII(intramedullaryconicalcompressionscrew) with-stoodameanmaximumflexionforceof320.40N,witharange from 360.08 to 278.85N. The mean stiffness under flexion was427.48N,witharangefrom455Nto385N(Table2and
Figs.8and9).
GroupIII(entiretestbody)withstoodamean maximum flexionforceof537.50N,witharangefrom545.61to528.68N. Themeanstiffnessunderflexionwas492N,witharangefrom
499Nto480N(Table3andFig.10).
Description and comparisonof the variables of interest betweenthethreegroupsstudied(Table4).
Table1–ResultsobtainedfromflexiontestforgroupI.
Item K(N/mm) Ele(Nm2) Q(mm) P(N) R(Nm) Fmax(N)
1 96.0 0.05 0.03 54 0.41 79.05
2 70.0 0.04 47 0.35 73.35
3 116.0 0.07 52 0.39 97.13
4 86.0 0.05 47 0.35 71.36
5 86.0 0.05 49 0.37 85.05
Mean 90.8 0.052 0.030 49.8 0.4 81.2
Standarddeviation 16.89 0.01 3.11 0.02 10.39
Source:MechanicalandMetallographicTestingLaboratory(LEMM).
K,rigidityunderflexion;Ele,structuralrigidityunderflexion;P,plasticflowload;R,momentofflow(resistancetoflexion);q,displacementat
0.2%ofthedistancebetweentheexternalandinternalbearings;Fmax,maximumtestforce.
Table2–ResultsobtainedfromflexiontestforgroupII.
Sample K(N/mm) Ele(Nm2) q(mm) P(N) R(Nm) Fmax(N)
1 434.0 0.24 0.03 250 1.88 360.08
2 455.0 0.26 265 1.99 328.09
3 467.0 0.26 320 2.40 342.55
4 398.0 0.22 250 1.88 278.85
5 385.0 0.22 190 1.43 292.45
Mean 427.8 0.2 0.03 255.0 1.9 320.4
Standarddeviation 35.48 0.02 46.37 0.35 34.03
Source:MechanicalandMetallographicTestingLaboratory(LEMM).
K,rigidityunderflexion;Ele,structuralrigidityunderflexion;P,plasticflowload;R,momentofflow(resistancetoflexion);q,displacementat
0.2%ofthedistancebetweentheexternalandinternalbearings;Fmax,maximumtestforce.
Table3–ResultsobtainedfromflexiontestforgroupIII.
Sample K(N/mm) Ele(Nm2) q(mm) P(N) R(Nm) Fmax(N)
1 480.0 0.27 0.030 430 3.23 528.68
2 499.0 0.28 0.030 420 3.15 545.61
3 497.0 0.28 0.030 410 3.08 538.12
Mean 492.0 0.3 0.030 420.0 3.2 537.5
Standarddeviation 10.44 0.01 0.030 10.00 0.08 8.48
Source:MechanicalandMetallographicTestingLaboratory(LEMM)
K,rigidityunderflexion;Ele,structuralrigidityunderflexion;P,plasticflowload;R,momentofflow(resistancetoflexion);q,displacementat
0.2%ofthedistancebetweentheexternalandinternalbearings;Fmax,maximumtestforce.
Fig.7–IllustrativephotoofgroupIafterthemechanical test.
400
350
300
250
200
150
100
50
0
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4
Deflection (mm)
Source: Mechanical and metallographic testing laboratory (LEMM)
Force/Load (N)
TB 1 TB 2 TB 3 TB 4 TB 5
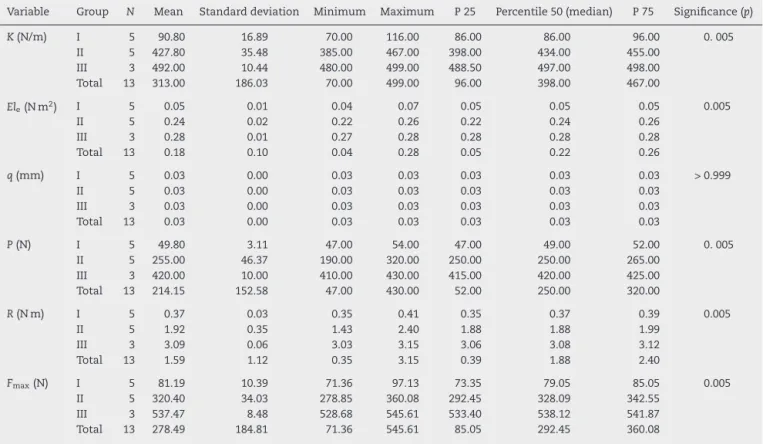
Table4–ApplicationofKruskal–Wallistest.
Variable Group N Mean Standarddeviation Minimum Maximum P25 Percentile50(median) P75 Significance(p)
K(N/m) I 5 90.80 16.89 70.00 116.00 86.00 86.00 96.00 0.005 II 5 427.80 35.48 385.00 467.00 398.00 434.00 455.00
III 3 492.00 10.44 480.00 499.00 488.50 497.00 498.00 Total 13 313.00 186.03 70.00 499.00 96.00 398.00 467.00
Ele(Nm2) I 5 0.05 0.01 0.04 0.07 0.05 0.05 0.05 0.005
II 5 0.24 0.02 0.22 0.26 0.22 0.24 0.26
III 3 0.28 0.01 0.27 0.28 0.28 0.28 0.28
Total 13 0.18 0.10 0.04 0.28 0.05 0.22 0.26
q(mm) I 5 0.03 0.00 0.03 0.03 0.03 0.03 0.03 >0.999
II 5 0.03 0.00 0.03 0.03 0.03 0.03 0.03
III 3 0.03 0.00 0.03 0.03 0.03 0.03 0.03
Total 13 0.03 0.00 0.03 0.03 0.03 0.03 0.03
P(N) I 5 49.80 3.11 47.00 54.00 47.00 49.00 52.00 0.005 II 5 255.00 46.37 190.00 320.00 250.00 250.00 265.00
III 3 420.00 10.00 410.00 430.00 415.00 420.00 425.00 Total 13 214.15 152.58 47.00 430.00 52.00 250.00 320.00
R(Nm) I 5 0.37 0.03 0.35 0.41 0.35 0.37 0.39 0.005
II 5 1.92 0.35 1.43 2.40 1.88 1.88 1.99
III 3 3.09 0.06 3.03 3.15 3.06 3.08 3.12
Total 13 1.59 1.12 0.35 3.15 0.39 1.88 2.40
Fmax(N) I 5 81.19 10.39 71.36 97.13 73.35 79.05 85.05 0.005
II 5 320.40 34.03 278.85 360.08 292.45 328.09 342.55 III 3 537.47 8.48 528.68 545.61 533.40 538.12 541.87 Total 13 278.49 184.81 71.36 545.61 85.05 292.45 360.08
K,rigidityunderflexion;Ele,structuralrigidityunderflexion;P,plasticflowload;R,momentofflow(resistancetoflexion);q,displacementat
0.2%ofthedistancebetweentheexternalandinternalbearings;Fmax,maximumtestforce.
synthesismaterials(Tables1and2)andfracturingofthetest bodyingroupIII(Table3).
The study described here did not present any statisti-callysignificantdifferencesincomparingthedifferentmodels simultaneouslyand withineachgroup.For thisreason,the Mann–Whitneytestwasapplied(Table5)toidentifywhich groupsdifferedfromtheothers,whencomparedaspairs.
Withtheexceptionofthevariableq(mm),whichremained constantinthethreegroups,itcanbestatedthatreal differ-encesbetweenthegroupswerepresentinrelationtotheother variablesofinterest.
Fig.9–IllustrativephotoofgroupIIafterthemechanical test.
600
500
400
300
200
100
0
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6
Deflection (mm)
Source: Mechanical and metallographic testing laboratory (LEMM)
Force/Load (N)
TB 1 TB 2 TB 3 TB 4 TB 5
Fig.10–Flexiontestcurves,withload-bearingatthree points,forgroupIII.
Table5–ApplicationofMann–Whitneytest.
Variable Pairofgroups
Ivs.II Ivs.III IIvs.III
K(N/m) 0.009 0.024 0.025
Ele(Nm2) 0.008 0.021 0.023
P(N) 0.009 0.024 0.024
R(Nm) 0.009 0.024 0.024
Discussion
Fracturesoftheproximalphalanxaremostprevalentamong malesbetweentheagesof10and40years.Theyareusually treatedasinsignificantinjuries,butthisresultsinfunctional limitation4inaneconomicallyimportantpopulation.
Evolution in treatments for fractures of the proximal phalanx is a necessity in our setting, given that the inci-dence of this fracture has been increasing exponentially andthepublishedresultsfromtheestablishedmethodsare unconvincing.10Theideal,inseekingtodiminishthe postop-erativecomplications,istocombinelessinvasivetechniques withbetterimplantstability,inordertoenableearly mobiliza-tionofthefracturedfinger.
Thenewdesignoflockedplatesandspecificallythoseof 1.5mmwithathicknessof2mm,alongwiththe accompany-inginstruments(preciseguidesandtweezersforperforming reduction),facilitatestheintraoperativeprocedure.
TheuseofanAcutrak®conicalcompressionscrew(which wasdesignedfortreatingfracturesofthescaphoid),described forthefirsttimeinthisstudy,showsthepossibilityof apply-ingthistofracturesoftheproximalphalanxwiththestability thatisnecessaryforgood postoperativerecovery.However, forthistobeundertaken,mechanicalproofthatthesynthesis would withstandtheloadingneeded duringthe rehabilita-tion,andwouldnotimpairrecoveryorbringanyharmtothe patient,wasrequired.Thisreasonencouragedustoconduct thepresentstudy.
Neither the percutaneous approach using the Acutrak® screwinthedorsalregionofthefinger(asaninternaltutor) northe placementofalateral plate (usingtheprinciple of axialcompression)reachedtheextensortendon,and adher-enceofthe tendontothe implantwas avoided.Therewas alsolessriskofjointstiffness,sincethehypothesiswasthat thesemethodswouldbesufficientlystabletoenable metacar-pophalangealand interphalangealjointmobilityduringthe immediatepostoperativeperiod.
Wedecidedtouseasyntheticbonemodel,ratherthanan animalphalanx(suchasfromapig),becausethedensityinthe modelwouldbeaconstant.Thisminimizedthebiasrelating tovariationsinbonedensityandconcentratedthetestingon theimplants.Westandardizedonasimpletransversefracture linesincethisisthebestlineforobtainingaxialcompression ofthefragments,giventhatweweregoingtotesttechniques thatappliedcompression.
In making horizontal comparisons of the mechanical resultsbetweenthegroups, itwasobservedthattherewas astatisticallysignificantdifferencebetweengroupsIandII. Thus,greaterforcewasneededtoreachfatigueofthe syn-thesismaterialconsistingofanintramedullaryscrew.Itwas thereforeshownthatthismaterialwasmechanicallysuperior tothemodelwiththelateralplate.
Sincethe meanmaximum forceingroupIII(Fig.3)was 167.8%greaterthanthatofgroupIand662.9%greaterthan thatofgroupII,thisshowsthatthetestmachine(Fig.1)didnot influencethefracture,butonlytheimplants.Thecomparative mechanicaltestperformedinthepresentstudywastherefore certified.
The results obtained from this study encourage us to proceedfurtherintheseinvestigations,nowinaclinical man-ner.Inadditiontothemechanicaladvantageofconicalscrews, theyareappliedpercutaneouslyandthismayavoid compli-cations relating tothe surgical access that isnecessary in osteosynthesisusingaplate.
Conclusion
StabilizationusingAcutrak®screws,intreatingthefractures inthemodelusedinthistrial,presents mechanicalresults thatarestatisticallysignificantlysuperiortothosefromthe axial compression technique using a lateral plate (Aptus Hand®).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PackerGJ,ShaheenMA.Patternsofhandfracturesand
dislocationsinadistrictgeneralhospital.JHandSurgBr.
1993;18(4):511–4.
2.EmmettJE,BreckLW.Areviewandanalysisof11,000
fracturesseeninaprivatepracticeoforthopaedicsurgery,
1937–1956.JBoneJointSurgAm.1958;40(A(5)):
1169–75.
3.DeJongeJJ,KingmaJ,VanderLeiB,KlasenHJ.Fracturesofthe
metacarpals.Aretrospectiveanalysisofincidenceand
aetiologyandareviewoftheEnglish-languageliterature.
Injury.1994;25(6):365–9.
4.KamathJB,Harshvardhan,NaikDM,BansalA.Current
conceptsinmanagingfracturesofmetacarpaland
phalangess.IndianJPlastSurg.2011;44(2):203–11.
5.BartonN.Internalfixationofhandfractures.JHandSurgBr.
1989;14(2):139–42.
6.Margi´cK.Externalfixationofclosedmetacarpaland
phalangealfracturesofdigits.Aprospectivestudyofone
hundredconsecutivepatients.JHandSurgBr.
2006;31(1):30–40.
7.HenryMH.Fracturesoftheproximalphalanxand
metacarpalsinthehand:preferredmethodsofstabilization.J
AmAcadOrthopSurg.2008;16(10):586–95.
8.OuelletteEA,DennisJJ,LattaLL,MilneEL,MakowskiAL.The
roleofsofttissuesinplatefixationofproximalphalanx
fractures.ClinOrthopRelatRes.2004;418:213–8.
9.MantovaniG,FukushimaWY,ChoAB,AitaMA,LinoWJr,
FariaFN.Alternativetothedistalinterphalangealjoint
arthrodesis:lateralapproachandplatefixation.JHandSurg
Am.2008;33(1):31–4.
10.ZylukA,Budzy ´nskiT.Treatmentofmetacarpaland
phalangealfractures–areview.ChirNarzadowRuchuOrtop
Pol.2006;71(4):299–308.
11.OrbayJL,TouhamiA.Thetreatmentofunstablemetacarpal
andphalangealshaftfractureswithflexiblenonlockingand
lockingintramedullarynails.HandClin.2006;22(3):
279–86.
12.FitoussiF,LuW,IpWY,ChowSP.Biomechanicalpropertiesof
absorbableimplantsinfingerfractures.JHandSurgBr.