ABSTRACT
Effect s of cervical m obilizat ion and exercise on
pain, m ovem ent and funct ion in subj ect s w it h
t em por om andibular disor der s: a single gr oup
pre- post t est
Letícia Bojikian CALIXTRE1, Bruno Leonardo da Silva GRÜNINGER1, Melina Nevoeiro HAIK2, Francisco
ALBURQUERQUE-SENDÍN3, Ana Beatriz OLIVEIRA1
1- Universidade Federal de São Carlos, Departamento de Fisioterapia, Laboratório de Cinesiologia Clínica e Ocupacional, São Carlos, SP, Brasil. 2- Universidade Federal de São Carlos, Departamento de Fisioterapia, Laboratório de Avaliação e Intervenção do Complexo do Ombro, São Carlos, SP, Brasil. 3- Universidad de Salamanca, Departamento de Enfermería y Fisioterapia; Instituto de Investigación Biomédica de Salamanca, Salamanca,España.
Corresponding address: Ana Beatriz Oliveira - Universidade Federal de São Carlos, Departamento de Fisioterapia - Via Washington Luis, KM 235 - CP 676 - 13565-905 - São Carlos-SP - Brasil - Phone: +55 16 33519793 - e-mail: [email protected]
6XEPLWWHG-XQH0RGL¿FDWLRQ'HFHPEHU$FFHSWHG0DUFK
O
bj ect iv e: To inv est igat e t he effect of a r ehabilit at ion pr ogram based on cer v icalm obilizat ion and exercise on clinical signs and m andibular funct ion in subj ect s w it h t em porom andibular disorder ( TMD) . Mat erial and Met hods: Single- group pre- post t est , wit h baseline com parison. Subj ect s: Twelve wom en ( 22.08± 2.23 years) wit h m yofascial pain and m ixed TMD according t o t he Research Diagnost ic Crit eria for Tem porom andibular Disorders. Out com e m easures: Subj ect s w ere evaluat ed t hree t im es: t w ice before ( baseline phase) and once aft er int ervent ion. Self- report ed pain, j aw funct ion [ according t o t he Mandibular Funct ional I m pairm ent Quest ionnaire ( MFI Q) ] , pain- free m axim um m out h opening ( MMO) , and pressure pain t hresholds ( PPTs) of bot h m asset er and t em poralis m uscles were obt ained. Baseline and post- int ervent ion differences were invest igat ed, and effect size was est im at ed
WKURXJK&RKHQ¶VGFRHI¿FLHQW5HVXOWV-DZIXQFWLRQLPSURYHGSRLQWVRQWKHVFDOHDIWHUWKH LQWHUYHQWLRQ3 DQGVHOIUHSRUWHGSDLQZDVVLJQL¿FDQWO\UHGXFHG3 3DLQ IUHH002YDULHGIURPPPWRPPDQGVKRZHGVLJQL¿FDQWLPSURYHPHQW
( P= 0.017) w it h m oderat e effect size w hen com pared t o t he baseline phase. PPT also increased w it h m oderat e effect size, and subj ect s had t he baseline values changed from 1.23± 0.2 kg/ cm2 t o 1.4± 0.2 kg/ cm2 in t he left m asset er ( P= 0.03) , from 1.31± 0.28 kg/ cm2
t o 1.51± 0.2 kg/ cm2 in t he right m asset er ( P> 0.05) , from 1.32± 0.2 kg/ cm2 t o 1.46± 0.2 kg/
cm2 in t he left t em poralis ( P= 0.047) , and from 1.4± 0.2 kg/ cm2 t o 1.67± 0.3 kg/ cm2 in t he
ULJKWWHPSRUDOLV3 &RQFOXVLRQV7KHSURWRFROFDXVHGVLJQL¿FDQWFKDQJHVLQSDLQ
free MMO, self- report ed pain, and funct ionalit y of t he st om at ognat hic syst em in subj ect s w it h m yofascial TMD, regardless of j oint involvem ent . Even t hough t hese differences are
VWDWLVWLFDOO\VLJQL¿FDQWWKHLUFOLQLFDOUHOHYDQFHLVVWLOOTXHVWLRQDEOH
Keyw ords: Tem porom andibular j oint . Neck. Physical t herapy specialt y. St om at ognat hic syst em .
I N TRODUCTI ON
Te m p o r o m a n d i b u l a r d i so r d e r s ( TMD ) a r e
GH¿QHG E\ WKH $PHULFDQ $FDGHP\ RI 2URIDFLDO
Pain as a collect ive t erm for a num ber of clinical problem s involving t he m ast icat ory m usculat ure, t he t em por om andibular j oint s ( TMJs) , and t heir
associat ed st r u ct u r es. Th is dy sfu n ct ion im pair s chew ing, swallow ing, and speaking, and t he m ain signs are j oint noises, reduced range of m ot ion, and m andibular deviat ion during TMJ funct ion.
t rigem inal and neck sensory input s24. I n prim at es, t his is caused by t he t opographic arrangem ent of t he t rigem inal caudat e nucleus t hat allow s inform at ion exchange bet ween t he spinal and t rigem inal nerves. Therefore, st im ulat ion of st ruct ures innervat ed by t he t rigem inal nerve m ay produce neck pain and vice- versa6.
The associat ion bet w een neck pain ( NP) and TMD h as b een w id ely in v est ig at ed2. A st r on g r elat ion sh ip w as d em on st r at ed b et w een n eck disabilit y an d j aw dy sf u n ct ion in pat ien t s w it h TMD w it h alt er ed elect r om y ograph ic act iv it y of t h e est er n ocleidom ast oid an d an t er ior scalen e
PXVFOHVGXULQJWKHFUDQLRFHUYLFDOÀH[LRQWHVWZKHQ
com pared w it h healt hy cont rols3. Moreover, TMD pat ien t s pr esen t ed r edu ced en du r an ce of n eck
ÀH[RUV DQG H[WHQVRU PXVFOHV %HYLODTXD*URVVL
et al.7 ( 2007) suggest ed t hat signs and sym pt om s of NP can perpet uat e TMD, but t hey do not appear t o predispose t he subj ect t o t he dysfunct ion. There seem s t o be a posit iv e, y et st ill con t r ov er sial, associat ion bet w een NP and TMD in adult s. The elucidat ion of t his cause and effect associat ion w ill reinforce t he possibilit y for physical t herapist s t o assist pat ient s w it h TMD by approaching t heir cervical spines25,29.
Ph y siot h er ap y t ech n iq u es in v olv in g m an u al therapy, active and passive stretching, strengthening of involved m uscles, and post ural exercises seem t o be effect ive for TMD t reat m ent28. According t o a syst em at ic review, m anual t herapy has been applied direct ly on TMJ st ruct ures, indirect ly on t he cervical or t horacic spine, or on bot h regions or st ruct ures w h en co m p o si n g m a n u a l t h er a p y p r o t o co l s9. Therapeut ic approaches using m anual t herapy and
H[HUFLVHVRQWKHFHUYLFDOVSLQHKDYHVKRZQEHQH¿WV
for pain, m ax im um m out h opening ( MMO) , and pressure pain t hresholds ( PPTs)24. However, st udies exam ining physical t herapy int ervent ions are st ill required t o st rengt hen t he evidence of t heir effect on com plem ent ing TMD t reat m ent28.
Th e h ig h est m et h od olog ical q u alit y st u d ies provide evidence support ing t he use of high-velocit y and low - am plit ude t hr ust m anipulat ions on t he upper cervical spine t o im prove PPT and MMO on TMD pat ient s27,29. How ever, such evidence is not available w hen considering nonm anipulat ive and exer cise t echniques. La Touche, et al.24 ( 2009) applied m anual t herapy and exercise t o t he cervical spines of pat ient s wit h m yofascial TMD and report ed im p r ov em en t of clin ical sig n s an d sy m p t om s, alt hough t he lack of a cont rol group, placebo, or baseline phase com prom ises t he evidence of t heir result s. I t is also unclear how subj ect s wit h m ixed TMD ( com bining m yofascial wit h j oint involvem ent ) w ould respond t o t his t reat m ent .
Th e r e f o r e , t h e a i m o f t h i s st u d y w a s t o inv est igat e t h e ef f ect s of a pr ot ocol based on
cervical m obilizat ion and exercise on m andibular f u n ct ion , PPTs, self- r epor t ed pain an d MMO in subj ect s w it h m yogenic or m ixed TMD com pared t o a wait- and- see period ( baseline) . The hypot hesis of t he st udy is t hat t hese out com es w ill im prove aft er int ervent ion when com pared t o t he baseline phase.
METHODOLOGY
St udy design
This single- group pre- post t est was conduct ed over a 9- week period. The baseline phase consist ed of t w o evaluat ions ( E1 and E2) perform ed w it h a 3- w eek int er val, dur ing w hich t im e t he subj ect s r eceiv ed n o t r eat m en t . Th e in t er v en t ion ph ase consist ed of 10 sessions of physical t herapy over
DZHHNSHULRGWKH¿UVWVHVVLRQRFFXUULQJXSWR
7 days aft er E2) , and a t hird evaluat ion ( E3) was perform ed 3–5 days aft er t he last session.
Alt hough m et hodological lim it at ions are inherent t o sin gle- gr ou p pr e- post t est st u dies ( i. e., t h e inabilit y t o cont rol t hreat s t o int ernal validit y) , t he use of a baseline phase was proposed t o st rengt hen t he st udy design. Consequent ly, t he st abilit y of t he out com e m easures was assessed and allow ed subj ect s t o act as t heir ow n cont rols5.
Subj ect s
Part icipant s w ere eligible t o part icipat e if t hey w ere older t han 18 years of age and had a prim ary d i ag n o si s o f m y o f asci al p ai n w i t h o r w i t h o u t lim it at ion of m out h opening according t o Axis I of t he Resear ch Diagnost ic Cr it er ia for TMD ( RDC/ TMD) . They could also be eligible w hen t here was u n ilat er al or bilat er al j oin t im pair m en t or disc displacem ent associat ed t o m iofascial pain. These crit eria dem onst rat ed good reliabilit y ( I CC 0.51- 0.60) , especially on m yofascial pain diagnoses20. Su bj ect s w er e ex clu ded if t h ey pr esen t ed w it h any of t he follow ing: a diagnosis of isolat ed disc displacem ent , ar t hr osis, or ar t hr it is of t he TMJ accor d in g t o t h e RDC/ TMD w it h ou t associat ed m yofascial com m it m ent ; a hist ory of m andibular
RUQHFNWUDXPDWLFLQMXULHV¿EURP\DOJLDV\QGURPH
a d i ag n o si s o f sy st em i c d i sease ( r h eu m at o i d a r t h r i t i s, sy st e m i c l u p u s e r y t h e m a t o su s, o r psor iat ic ar t hr it is) ; t he pr esence of neur ological disorders; and a hist ory of any form of t reat m ent ( phy siot herapy, splint t herapy, or acupunct ur e) w it hin t he 3 m ont hs before t he st udy. They w ere ask ed n o t t o u se p ai n m ed i cat i o n o r m u scl e relaxant s at least 24 hours before t he evaluat ions and during t he t reat m ent period.
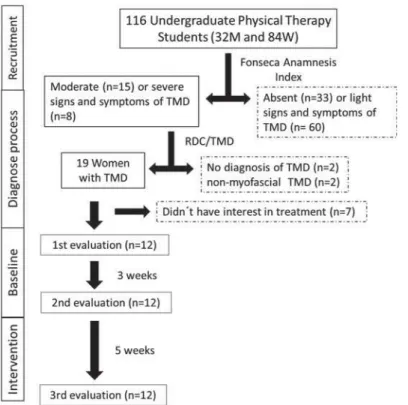
low- cost alt ernat ive t o screen subj ect s displaying signs and sym pt om s of t he disorder, as w ell as t o classify t he severit y of t he sym pt om s ( absent , light , m oderat e, or severe) . I t is validat ed t o Brazilian Port uguese language and has a regular reliabilit y ( I CC 0.55)10.
Tw e n t y - t h r e e st u d e n t s sh o w e d m o d e r a t e ( n= 15) or severe ( n= 8) signs and sym pt om s of t he disorder, according t o t he Fonseca Anam nest ic I ndex, and t hey w ere invit ed t o part icipat e in t he diagnost ic pr ocess. The evaluat ion pr oposed by RDC/ TMD w as per f or m ed by a phy siot h er apist w ho had recent ly graduat ed and was t rained and supervised by t wo physiot herapist s wit h at least 10 years of experience in physical t herapy t reat m ent and evaluat ion. Elev en subj ect s w er e ex cluded because of t he absence of m yofascial pain ( n= 2) ; a lack of a TMD diagnosis ( n= 2) ; and a lack of int erest in part icipat ing in t he int ervent ion ( n= 7) .
7KH¿QDOVDPSOHZDVFRPSRVHGRIZRPHQ
w it h a m ean age of 22.08± 2.23 years ( Figure 1) . They w er e diagnosed w it h m yofascial pain w it h lim it at ion of m out h opening ( n= 2) , or m ixed TMD ( n= 10) - com bining m yofascial pain eit her w it h j oint im pairm ent ( n= 7) or disc displacem ent ( n= 3) . All subj ect s had bilat eral m yofascial involvem ent , alt hough m ost j oint or disc disorders were unilat eral ( six left sided, t w o right sided) .
All r esear ch p r oced u r es w er e ap p r ov ed b y t he local Et hics Com m it t ee on Hum an Resear ch ( Au t h o r i z a t i o n # 1 4 5 / 2 0 1 2 ) . Th e st u d y w a s regist ered on ClinicalTrials.gov ( NCT01954511) .
Evaluat ion prot ocol
Evaluat ion of m andibular funct ion
Man dibu lar fu n ct ion w as evalu at ed w it h t h e
Mandibular Funct ional I m pairm ent Quest ionnaire
( MFI Q). Th is q u est ion n air e h as 1 7 q u est ion s, each one scoring bet w een 0 and 4. The higher t he score, t he great er t he funct ional im pairm ent . The sum of t he responses was used in t he st at ist ical analysis. The Port uguese version used in t his st udy has shown good reliabilit y11 it was applied t o 62 indiv iduals w ho com plet ed t he quest ionnair e on t wo occasions. Validit y and reliabilit y of t he dat a gat hered w it h MFI Q w ere evaluat ed in a sam ple of 2 4 9 pat ien t s. Con st r u ct - r elat ed validit y w as assessed t hrough fact orial validit y ( by m eans of a
FRQ¿UPDWRU\IDFWRUDQDO\VLV
Evaluat ion of clinical signs of TMD
Clinical signs of TMD w ere evaluat ed according t o RDC/ TMD ( h t t p: / / w w w. r dc- t m din t er n at ion al. or g) . Pain- fr ee MMO was m easur ed w it h a 0.05 m m precision analog vernier caliper. Part icipant s were seat ed while t he assessor asked t hem t o open t heir m out hs as m uch as possible w it hout causing pain. At t he lim it of pain- free m out h opening, t he dist ance bet w een t he upper- low er cent ral incisors ( not considering t he overbit e) was m easured.
Self- report ed pain was evaluat ed t hrough t he num er ic scale pr esent ed in RDC/ TMD. Subj ect s w ere asked t o report t heir pain at t he m om ent on a scale ranging from 0 ( no pain) t o 10 ( w orst pain
ever experienced) , w it h a 1- point int erval.
Evaluat ion of PPTs
Masset er and ant er ior t em poralis PPTs w er e bilat erally assessed using an analog algom et er ( Pain Diagnosis and Treat m ent I nc., Great Neck, NY, USA) . The m easurem ent s were report ed in kg/ cm2. According t o lit erat ure, t he reliabilit y of t his m et hod
LVKLJK>,&& FRQ¿GHQFHLQWHUYDO
0.97) ] for healt hy subj ect s13 at a rat e of 5 Newt ons, and m oderat e ( I CC= 0.64) for TMD pat ient s17. The point s were always evaluat ed in t he sam e order and repeat ed t hree t im es, wit h a 1- m inut e int erval. The average of t he t hree m easurem ent s was considered for each point .
The m asset er m uscle was evaluat ed at 1 cm above and 2 cm ant erior t o t he m andibular angle. The ant erior t em poralis m uscle was evaluat ed at 2 cm above t he zygom at ic arch, bet w een t he lat eral
HGJHRIWKHH\HDQGWKHDQWHULRUSDUWRIWKH¿EHUV24.
I nt ervent ion
The pr ot ocol r epor t ed by La Touche, et al.24 ( 2 0 0 9 ) w a s u sed a s a r ef er en ce. Th er ef o r e, m uscle- condit ioning t echniques, m anual t herapy, and st r et ching w er e applied for 1 0 sessions of appr ox im at ely 35 m inut es each: 20 m inut es of m anual t herapy, 10 m inut es of m uscle condit ioning exercises, and 5 m inut es of m uscle st ret ching.
The t echniques w er e applied in t he follow ing order:
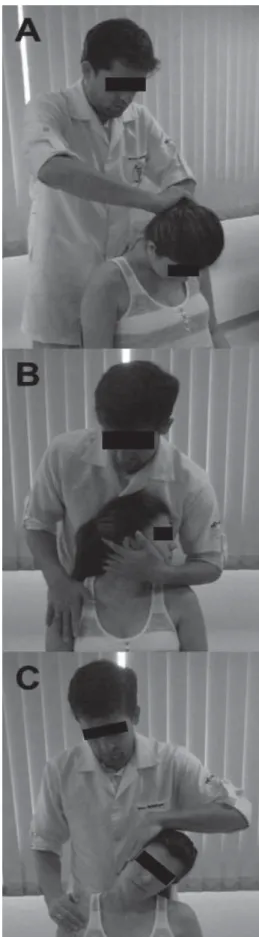
8SSHUFHUYLFDOÀH[LRQPRELOL]DWLRQWKHVXEMHFW
lay dow n in t he supine posit ion ( Figure 2A) w hile t he t herapist kept one hand in cont act w it h t he occipit al bone, exert ing t ract ion force, and placed t he ot her on t he front al region of t he subj ect ’s head, apply ing caudal pr essur e. The com bined for ces
SURPRWHGÀH[LRQRQWKHXSSHUFHUYLFDOUHJLRQZLWK
t he m obilizat ion being applied at a slow rat e of 2 seconds per oscillat ion for a t ot al t im e of 10 m in24.
C5 cent ral post erior- ant erior m obilizat ion: t he subj ect lay down in t he prone posit ion, wit h neut ral cervical spine posit ion ( Figure 2B) . The t herapist placed t he t ips of his t hum bs on t he post er ior surface of t he C5 spinous process w hile t he ot her
¿QJHUV ZHUH JHQWO\ UHVWHG DURXQG WKH VXEMHFW¶V
neck. The oscillat ions w ere conduct ed in t he t hird grade of t he Mait land scale at t he fr equency of 2 oscillat ion s per secon d an d per f or m ed f or 9 m inut es, divided int o 3 set s of 3 m inut es, w it h a 1- m inut e int erval.
Cr an iocer v ical f lex or st ab ilizat ion ex er cise: ly in g dow n in t h e su pin e posit ion , t h e su bj ect
ZDV LQVWUXFWHG WR SHUIRUP FUDQLRFHUYLFDO ÀH[LRQ
( Figur e 2C) . The head was kept in cont act w it h t he suppor t ing sur face t o facilit at e act ivat ion of
GHHS QHFN ÀH[RUV ZLWK PLQLPDO DFWLYLW\ RI WKH VXSHU¿FLDOQHFNÀH[RUPXVFOHV21. This cont ract ion
was m onit ored using a pressure sensor ( St abilizer; Ch a t t a n o o g a Gr o u p , I n c., Ch a t t a n o o g a , TN, USA) . The t herapist m onit ored any cont ract ion of
VXSHU¿FLDOQHFNÀH[RUVPXVFOHVZLWKSDOSDWLRQRI
t he ant erior neck region t o ensure t hat t he exercise was being correct ly perform ed. Each craniocervical
ÀH[LRQSURGXFHGDSUHVVXUHUDQJLQJIURPWR
m m Hg. The subj ect s w ere inst ruct ed t o m aint ain t hat pressure using visual feedback for 10 seconds
Figure 2- Positioning of patient and therapist during
$ XSSHU FHUYLFDO ÀH[LRQ PRELOL]DWLRQ % & FHQWUDO
posterior-anterior mobilization, and (C) craniocervical
ÀH[RU VWDELOL]DWLRQ H[HUFLVH 7KH DUURZV LQGLFDWH WKH
w it h n o con t r act ion of su p er f icial n eck f lex or m uscles. This procedure was repeat ed 10 t im es. Load increase was used t o progress t he exercise. The num ber of r epet it ions and durat ion of each cont ract ion was const ant21.
St ret ching exercises: w hile seat ed, t he subj ect p er f or m ed st r et ch in g ex er cises f or t h e u p p er t r apeziu s, scalen e, sem ispin al m u scle of h ead, splenius capit is, and st ernocleidom ast oid m uscles ( Figure 3) . These m uscles are direct ly involved wit h head posit ioning and t heir shor t ening pr oduces m isalignm ent in head and neck segm ent s1. Each st r et ch w as applied for 25- 30 seconds, at high int ensit y, accor ding t o t he subj ect s’ per cept ions ( score of 8 on a 0- 10 scale, for w hich 0 m eans no st ret ching and 10 m eans a m axim um elongat ion of t hat m uscle) .
St at ist ical analysis
Sam ple size was calculat ed considering PPT as t he m ain out com e, w it h dat a from t he lit erat ure24, f o r a r e p e a t e d m e a su r e s d e si g n . To d e t e ct
VLJQL¿FDQW GLIIHUHQFHV RI NJFP2 on t he PPTs, w it h st andard deviat ion of 1 kg/ cm2DVLJQL¿FDQFH level of 0.05, and pow er of 0.80, t he sam ple size was calculat ed as at least 10 subj ect s w it h TMD. Spanish soft war e was used for calculat ion ( Ene 3.0, Aut onom a Barcelona Universit y & Glaxo Sm it h Kline, Spain) . Tw elve subj ect s w er e included t o cont rol a w it hdrawal rat e of 20% .
Sh a p i r o - W i l k a n d Lev en e t est s w er e u sed t o r esp ect i v el y ev al u at e t h e d i st r i b u t i o n an d h o m o sce d a st i ci t y o f t h e n u m e r i ca l v a r i a b l e s ( pain- fr ee MMO and PPTs) . One- fact or r epeat ed m easures ANOVA was used t o com pare pain- free MMO and PPTs am ong evaluat ions E1, E2, and E3, considering evaluat ion as wit hin- subj ect fact or. The Tukey t est was used for post - hoc analysis t o locat e t he difference ( E1xE2 or E2xE3) . For int erpret ing t hose t est s, alfa was considered = 0.05 ( 5% ) . The com parison bet w een E1 and E3 was not perform ed because it was considered irrelevant t o answ er t he research quest ion.
Fr iedm an t est w as applied t o com par e pain and funct ion acr oss evaluat ions E1, E2, and E3 for num erical ordinal and nonparam et ric variables ( MFI Q and pain scor es) consider ing alfa = 0. 05 ( 5 % ) . Mor eov er, i sol at ed p ai r ed com p ar i son s w ere m ade ( E1xE2 or E2xE3) w it h Wilcoxon t est .
%RQIHUURQL FRUUHFWLRQ ZDV DSSOLHG Į WR
count eract t he pr oblem of m ult iple com par isons ( high risk of t ype I error) . Analyses w ere carried out using t he st at ist ical package Sigm aPlot ( v.11.0) .
Fin ally, ef f ect size ( ES) w as calcu lat ed f or norm ally dist ribut ed variables t hrough t he relat ive
&RKHQ¶VGFRHI¿FLHQW(6KDVEHHQGH¿QHGDV³WKH
degree at w hich t he phenom enon is present in t he populat ion”. Therefore, t he larger t he effect size,
“ t he higher t he degree at w hich t he phenom enon u n der st u dy m an if est s”1 4. ES is t h e dif f er en ce in m ean scor es div ided by t he pooled st andar d deviat ion of t he evaluat ions ( evaluat ions E1 and E2, t hen evaluat ions E2 and E3)4. Values bet w een 0.2 and 0.49 were int erpret ed as sm all effect ; t hose bet w een 0. 5 and 0. 79 as m oderat e effect ; and values great er t han 0.8 as large effect .
RESULTS
The m andibular funct ion scor e w as differ ent am ong evaluat ions ( P= 0.019) . Post - hoc analysis
r e v e a l e d s i g n i f i c a n t m a n d i b u l a r f u n c t i o n im provem ent from E2 t o E3 ( P= 0.02) but not from E1 t o E2 ( P= 0.47) , as report ed in Table 1. Only t w o subj ect s present ed w it h w orsened funct ion aft er int er vent ion, w hile seven show ed im pr ovem ent , and t hree displayed t he sam e previous MFI Q score.
Pain- free MMO also changed with tim e ( P= 0.002) .
Post - hocDQDO\VLVUHYHDOHGDVLJQL¿FDQWLQFUHDVHRI
5.7 m m ( p= 0.009) in MMO, from E2 t o E3, w it h m od er at e ef f ect size ( d = 0 . 6 4 ) . Th er e w as n o
VLJQL¿FDQWGLIIHUHQFH3 DQGORZHIIHFWVL]H
( d= 0.09) bet w een E1 and E2 ( Table 1) .
I n addit ion t o t he low level of self- report ed pain
Mean (SD) ANOVA (P-value)
post-hoc Tukey
(P-value)
ES
Maximum Mouth Opening (mm)
1st Evaluation 31.5 (9.17) 0.002* 1x2 0.88 0.09
2nd Evaluation 32.3 (8.80)
3rd Evaluation 38.0 (8.82) 2x3 0.009* 0.64
Median (25%-75%) Friedman (P-value)
post-hoc :LOFR[RQƇ
(P-value)
Pain Scale - RDC/TMD
1st Evaluation 1 (1-3) 0.013* 1x2 0.888
2nd Evaluation 1 (0-3)
3rd Evaluation 0 (0-1) 2x3 0.017*
Mandibular Function – MFIQ
1st Evaluation 18.5 (11.75 - 24.25) 0.019* 1x2 0.47
2nd Evaluation 15 (10 - 26.25)
3rd Evaluation 8.5 (7 - 14.25) 2x3 0.020*
VWDWLVWLFDOO\VLJQL¿FDQWYDOXHV(6HIIHFWVL]HƇDOSKD %RQIHUURQLFRUUHFWLRQ[&RPSDULVRQEHWZHHQ¿UVWDQG
second evaluations; 2x3: Comparison between second and third evaluations
Table 1- Data of Mandibular Function Impairment Questionnaire, self-reported pain, and pain-free Maximum Mouth Opening
Pressure Pain Thresholds - kg/cm2
Muscle Evaluations ANOVA post-hoc Tukey Effect Size 1st
mean (SD)
2nd
mean (SD)
3rd
mean (SD)
(P-value) P-value)
Left masseter 1.25 (0.21) 1.23(0.20) 1.40 (0.27) 0.028* 1x2 2x3
0.896 0.033*
-0.13 0.71
Right masseter
1.41 (0.27) 1.31 (0.28) 1.51 (0.28) 0.105 1x2 2x3
N/A N/A
-0.30 0.65
Left temporalis
1.28 (0.23) 1.32 (0.21) 1.46 (0.20) 0.008* 1x2 2x3
0.714 0.047*
0.19 0.67
Right temporalis
1.64 (0.24) 1.40 (0.24) 1.67 (0.36) 0.003* 1x2 2x3
0.013* 0.060
-1.03 0.91
VWDWLVWLFDOO\VLJQL¿FDQWYDOXHV1$QRWDSSOLHG[FRPSDULVRQEHWZHHQ¿UVWDQGVHFRQGHYDOXDWLRQV[FRPSDULVRQ
between second and third evaluations
am ong subj ect s ( t w o of t hem report ed no pain at
WKH PRPHQW RI ( D VLJQL¿FDQW GLIIHUHQFH ZDV
also found for pain score ( P= 0.013, Table 1) . Self-report ed pain decreased in E3 when com pared t o E2
3 ZLWKQRVLJQL¿FDQWGLIIHUHQFHEHWZHHQ
E1 an d E2 ( P= 0 . 8 8 ) . Sev en su b j ect s sh ow ed im provem ent in t his sym pt om .
6LJQL¿FDQWGLIIHUHQFHVLQ337VZHUHIRXQGLQERWK
left t em poralis and m asset er m uscles, and t he post -hoc DQDO\VLV VKRZHG D VLJQL¿FDQW LQFUHDVH DIWHU
int ervent ion ( P= 0.033 and P= 0.047, respect ively) , bot h w it h m oderat e effect size. The com par ison bet w een E1 and E2 for PPT dat a has not show n a st at ist ical difference, and t he effect size was low ( Table 2) .
1R VLJQL¿FDQW GLIIHUHQFH ZDV IRXQG RQ ULJKW
m asset er PPT, bu t t h e in cr easin g effect of t h is m e a su r e m e n t w a s m o d e r a t e ( d = 0 . 6 5 ) a f t e r t reat m ent . However, right t em poralis PPT present ed
DVLJQL¿FDQWGHFUHDVHEHIRUHLQWHUYHQWLRQ3
d= - 1.03) and high effect size aft er int er vent ion
G ZLWKQRVWDWLVWLFDOVLJQL¿FDQFH3
DI SCUSSI ON
Accor d in g t o t h e r esu lt s, t h e t r eat m en t of t he cer v ical spine based on j oint m obilizat ions, segm en t al st abilizat ion , an d m u scle st r et ch in g
SURGXFHGVWDWLVWLFDOO\VLJQL¿FDQWFKDQJHVLQVXEMHFWV
w i t h TMD. Th e t r eat m en t p r o t o co l d ecr eased self- report ed pain, increased pain- free MMO, and im proved m andibular funct ion. There was also a
VLJQL¿FDQW LPSURYHPHQW LQ PDVWLFDWRU\ PXVFOH
sensit ivit y on t he left side.
Pain and m andibular funct ion
7KHUHZDVDVWDWLVWLFDOO\VLJQL¿FDQWLPSURYHPHQW
in self- report ed pain aft er int ervent ion, w it h som e subj ect s achieving a m edian of 0 on t he pain scale. Pain was m easured by m eans of t he graduat e scale included in t he RDC/ TMD prot ocol. Even t hough it is not t he m ost w idely used t ool for m easuring pain, t his scale was sensit ive t o pain var iat ions aft er int ervent ion. These result s agree w it h t he current lit erat ure24.
The Visual Analogue Scale ( VAS) is com m only used in TMD st udies. I t has been st at ed t hat t he st at ist ic an d clin ical su ccess of t h e t r eat m en t requires at least t he sm allest det ect able difference ( from 15 t o 43 m m , depending on t he m et hodology) and 38% of t he init ial average pain level23. Alt hough all subj ect s had been diagnosed w it h TMD, t heir pain levels were low, causing a ceiling effect . Hence, t he clinical relevance for t his out com e could not be achieved.
How ev er, p ain r ed u ct ion af t er in t er v en t ion w as con sist en t am on g su b j ect s. Ev en t h ou g h t he m echanism associat ed w it h t his result is not
fully underst ood, t he st im ulat ion of t he inhibit ory downward pat h t hrough t he cervical spine has been ex pect ed t o r educe pain in t he t r igem inal ar ea. Nevert heless, because signs and sym pt om s of neck dysfunct ion were not evaluat ed in t he present st udy, a relat ionship bet ween t he cervical spine t reat m ent and TMD sym pt om s cannot be est ablished. Pain r ed u ct ion is su g g est ed t o b e associat ed w it h increased MMO.
I n addit ion t o reduced pain, subj ect s present ed
VLJQL¿FDQW LPSURYHPHQW LQ PDQGLEXODU IXQFWLRQ
aft er t r eat m ent , w hich m ay be r elat ed t o bot h r edu ced pain an d in cr eased MMO becau se t h e MFI Q a d d r e sse s t h e m a j o r f u n ct i o n s o f t h e st om at ognat hic syst em ( eat ing different kinds of food, com m unicat ing, yawning, and sm iling) , which require m out h opening and proper perform ance of t his syst em11. Therefore, it is im port ant t o consider t hat t he im pairm ent of m andibular funct ion was low am ong subj ect s, and t he ceiling effect was probably achieved.
Low levels of pain and sm all im pair m ent s of m andibular funct ion are not able charact erist ics of t he college populat ion for w hich t he prevalence of TMD is high12 and should not be neglect ed. Even
ZLWK ORZ LPSDLUPHQW WKHLU GLI¿FXOW\ WR SHUIRUP
som e im por t ant act iv it ies is com m on in clinical pract ice. Furt herm ore, t he invest igat ion of subj ect s w it h sm all severit y helps w it h underst anding t heir sym pt om s and prevent s t hem from becom ing m ore serious.
Pain- free MMO
MMO incr eased an av erage of 5. 7 m m aft er i n t er v en t i o n , co r r esp o n d i n g t o 1 7 . 5 % o f t h e in it ial v alu e w it h m od er at ed ef f ect size. Th is im provem ent agrees w it h st udies t hat have used m anual t herapy on t he cervical spine in subj ect s w it h TMD. A m anipulat ive t herapy applied t o t he upper cer v ical r egion of pat ient s w it h m yogenic
70'SURGXFHGVLJQL¿FDQWLPSURYHPHQWRIPP
in MMO im m ediat ely aft er int ervent ion27. Moreover, La Touche et al.24 ( 2009) report ed an im provem ent of 4.5 m m aft er 10 sessions of m anual t herapy t o t he cervical spine. Bot h st udies observed clinically im port ant result s, alt hough t he sm allest det ect able d if f er en ce f or MMO w as r ep or t ed as 6 - 9 m m , depending on t he evaluat ion procedure22.
A p r ev iou s st u d y t h at ap p lied a m y of ascial r e l e a se t e ch n i q u e o n t h e m a sse t e r m u scl e s pr esen t ed im m ediat e im pr ov em en t s of 4 m m1 9 in MMO. Our pr ot ocol induced im pr ovem ent s in j aw opening sim ilar t o t hose observed w it h local t reat m ent of t he m asset er m uscle. Therefore, an indirect approach focusing on t he upper cervical
VSLQHPD\EHEHQH¿FLDOWRSDWLHQWVZLWKDOORG\QLF UHVSRQVHVLQWKHRURIDFLDOUHJLRQZKR¿QGPDQXDO
Th er e seem s t o b e a f u n ct ion al in t eg r at ion bet w een j aw an d at lan t o- occipit al m ov em en t s. Previous st udies16,18 show ed t hat during chew ing act iv it ies, t h er e ar e m ov em en t s on t h e u p p er cer v i cal sp i n e r el at ed t o m o u t h o p en i n g an d closing, and t hey depend on t he coordinat ion of t he m ast icat ory and cervical m uscles. Consequent ly, t he im m obilizat ion or alt erat ion of head posit ion can affect m andibular m ovem ent s18.
Mor eov er, m ou t h open in g is closely r elat ed t o upper cervical ext ension16. Pat ient s w it h TMD
KDYH VKRZQ VLJQL¿FDQW OLPLWDWLRQV LQ PRYHPHQWV of t he upper cervical segm ent w hen com pared t o asym pt om at ic subj ect s15. Therefore, TMJ alt erat ions can cause neck dysfunct ion and vice versa. Manual t h er apy applied t o t h e cer v ical spin e pr obably cont ribut es t o cervical range of m ot ion, facilit at ing and increasing m out h opening.
Finally, accor ding t o Leandr i, et al.26 ( 2001) , n ocicep t iv e im p u lses f r om t h e u p p er cer v ical spin e cau se r ef lex con t r act ion s in m ast icat or y m uscles, w hich can cont ribut e t o t he developm ent of TMD sym pt om s. Thus, j oint m obilizat ion t oward t h e u p p er cer v i ca l r eg i o n a p p ea r s t o r ed u ce
PXVFXODUUHÀH[FRQWUDFWLRQVDQGWRDOORZPXVFOH
relaxat ion, especially in m asset er m uscles, and m ay consequent ly increase MMO.
Alt hough t he im provem ent on MMO did not reach t he clinically m eaningful difference22WKHVLJQL¿FDQW change and t he good effect size of t he t herapy su ggest gr eat t en den cy t ow ar ds r est or at ion of norm al values for MMO, even aft er few int ervent ion se ssi o n s o f m a n u a l t h e r a p y t e ch n i q u e s a n d segm ent al st abilizat ion applied direct ly t o cervical spine. Lim it ed MMO is one of t he m ain com plaint s r epor t ed by TMD pat ient s because of funct ional lim it at ions. Ther efor e, pr olonged pr ot ocols and ot her m anual t herapy t echniques t o t he cervical spine should be considered and invest igat ed for t he t reat m ent of TDM pat ient s.
PPTs
PPTs m easu r ed on m asset er an d t em por alis
PXVFOHVZHUHVLJQL¿FDQWO\KLJKHUDIWHULQWHUYHQWLRQ
part icularly on t he left side. Moreover, t he effect size f or b ot h m u scles w as m od er at e or lar g e aft er int ervent ion, but sm all or nonexist ent at t he baseline phase. I n general, t he m ean differences w er e p r ed om in an t ly n eg at iv e ( i. e., t h er e w as a r ed u ct i o n i n PPTs f r o m t h e f i r st t o seco n d evaluat ion) , alt hough t hose bet w een t he m ean values before and aft er int ervent ion ranged from 0.14 t o 0.28 kg/ cm2, what is lower t han t he m inim al det ect able change t hat varies from 0.45 t o 1.13 kg/ cm2 report ed by Walt on, et al31. Different result s w ere report ed by La Touche, et al.24 ( 2009) , w ho
IRXQGDVLJQL¿FDQWLQFUHDVHJUHDWHUWKDQNJ
cm2) in PPTs on bot h m asset er and t em poralis
m uscles aft er a sim ilar t reat m ent . Anot her st udy27 t hat approached TMD pat ient s w it h upper cervical
PDQLSXODWLRQ YHUL¿HG 337 RQ WKH VSKHQRLG ERQH 7KHDXWKRUVUHSRUWHGVLJQL¿FDQW\HWQRWFOLQLFDOO\
relevant , result s.
PPT of m ast icat ory m uscles in TMD pat ient s has been described as lower t han t hose in asym pt om at ic su b j e ct s3 0. Va l u e s f o r m a sse t e r m u scl e s a r e a p p r ox i m a t el y 1 . 5 k g f / cm2 a n d 2 . 3 k g f / cm2, and for t he t em poralis m uscle, 2.1 kgf/ cm2 and 3.5 kgf/ cm2 in TMD and asym pt om at ic subj ect s, r esp ect iv ely. Ou r sam p le sh ow ed a sig n if ican t incr ease aft er t r eat m ent w it h a m oderat e/ lar ge effect from t he int ervent ion. How ever, PPT values for t he m asset er and t em poralis did not r each norm al values aft er t reat m ent . This result suggest s som e t endency t owards im provem ent t hat should be bet t er invest igat ed w it h prolonged prot ocols, in addit ion t o ot her m anual t herapy t echniques and cont rol groups.
Fi n al l y, PPT o f m u scl es f r o m t h e l ef t si d e present ed great er im provem ent s t han t hose from t he right side. I t is im port ant t o highlight t hat t he left side was m ost ly involved in pat ient s present ing j oint degenerat ions or disc displacem ent s associat ed
WRP\RIDVFLDOSDLQ6RWKHVLJQL¿FDQWLQFUHDVHRQ
PPT of t he m uscles in t he left side aft er int ervent ion and not in t he right one m ay be relat ed t o t hose associat ed im pairm ent s.
St udy lim it at ions
Sam ple size est im at ion was based on PPT dat a,
DQGVWDWLVWLFDOO\VLJQL¿FDQWGLIIHUHQFHVZHUHIRXQG
w h en co m p ar i n g ev al u at i o n s; h o w ev er, m o st differ ences w er e low er t han t he est im at ed ones an d did n ot sh ow clin ical r elevan ce ( com par ed w it h m inim al clinical difference) . Therefore, using changes of anot her out com e t o est im at e sam ple si ze co u l d h av e p r ov i d ed b i g g er sam p l e si ze est im at ion and different result s.
The AB design was support ed by t he lit erat ure5 t o provide result s t hat could be useful on t he clinical decisions for one pat ient . The design show ing t he proposed prot ocol was m ore effect ive t han t im e it self because no im port ant changes were observed
EHWZHHQ¿UVWDQGVHFRQGHYDOXDWLRQV+RZHYHUWKH
effect iveness of t he prot ocol should be invest igat ed t hrough a random ized cont rolled t rial, considering eit her a cont rol or a sham group.
Mo r eov er, 5 w eek s o f i n t er v en t i o n can b e consider ed as associat ed t o shor t - t er m r esult s. However, high qualit y st udies invest igat ing m anual t herapy on subj ect s wit h TMD show posit ive effect s w it h few sessions8. We believe t hat furt her st udies should consider a follow- up perform ed som e weeks aft er t he last evaluat ion. I t can help t o underst and t he perpet uat ion of t he result s along t im e.
according t o t he RDC/ TMD prot ocol, t hey present ed w it h low levels of pain and sm all im pairm ent s of m andibular funct ion. Sam ples w it h m or e sever e im pairm ent m ay have revealed different result s. Conver sely, t he high pr evalence of TMD am ong st u d en t s an d t h e f act t h at t h ey ar e com m on pat ient s in t he daily pract ice of physiot herapy lead our result s t o help m ake t he right clinical decision w hen dealing w it h t his kind of pat ient .
CON CLUSI ON S
Th e cer v ical sp in e t h er ap y ap p r oach u sin g neck j oint m obilizat ion, m uscle st r et ching, and
VHJPHQWDOVWDELOL]DWLRQVHHPVWRFDXVHVLJQL¿FDQW
im p r ov em en t in p ain - f r ee MMO, self- r ep or t ed pain, and m andibular funct ionalit y in subj ect s wit h m yofascial pain or m ixed TMD. Changes show ed m oderat e- t o- large effect sizes but sm all m agnit ude and no clinical relevance. How ever, t he t endency of t he result s indicat es t hat furt her st udies should co n t i n u e i n v est i g at i n g t h e ef f ect s o f cer v i cal t reat m ent in subj ect s w it h TMD. I t w ill bring up st ronger evidence about t he indirect approach of TMD by physical t herapist s.
FUN DI N G
Th is w or k w as su ppor t ed by t h e São Pau lo Research Foundat ion ( FAPESP) - Grant 2014/ 05276-7.
REFEREN CES
1- Andrade AV, Gom es PF, Teixeira- Salm ela LF. Cer vical spine alignm ent and hyoid bone posit ioning w it h t em porom andibular disorders. J Oral Rehabil. 2007; 34: 767- 72.
2- Arm ij o- Olivo S, Magee D. Cervical m usculoskelet al im pairm ent s a n d t em p o r o m a n d i b u l a r d i so r d er s. J Or a l Ma x i l l o f a c Res. 2012; 3: e4.
3- Ar m ij o- Olivo S, Silvest r e RA, Fuent es JP, Cost a BR, Maj or PW, Warren S, et al. Pat ient s w it h t em porom andibular disorders hav e incr eased fat igabilit y of t he cer v ical ex t ensor m uscles. 2012; 28: 55- 64.
4 - Ar m ij o- Oliv o S, War r en S, Fu en t es J, Magee DJ. Clin ical
UHOHYDQFH YV VWDWLVWLFDO VLJQL¿FDQFH XVLQJ QHFN RXWFRPHV LQ
pat ient s w it h t em porom andibular disorders as an exam ple. Man Ther. 2011; 16: 563- 72.
5- Backm an CL, Harris SR, Chisholm JA, Monet t e AD. Single-subj ect research in rehabilit at ion: a review of st udies using AB, wit hdrawal, m ult iple baseline, and alt ernat ing t reat m ent s designs. Arch Phys Med Rehabil. 1997; 78: 1145- 53.
6- Bart sch T, Goadsby PJ. I ncreased responses in t rigem inocervical nocicept ive neurons t o cervical input aft er st im ulat ion of t he dura m at er. Brain. 2003; 126: 1801- 13.
7- Bevilaqua- Grossi D, Chaves TC, Oliveira AS. Cervical spine sign s an d sy m pt om s: per pet u at in g rat h er t h an pr edisposin g fact ors for t em porom andibular disorders in w om en. J Appl Oral Sci. 2007; 15: 259- 64.
8- Calixt re LB, Grüninger BL, Chaves TC, Oliveira AB. I s t here an associat ion bet w een anxiet y/ depression and t em porom andibular disorders in college st udent s? J Appl Oral Sci. 2014; 22: 15- 21.
9- Calixt re LB, Moreira RF, Franchini GH, Alburquerque- Sendín F, Oliveira AB. Manual t herapy for t he m anagem ent of pain and lim it ed range of m ot ion in subj ect s w it h signs and sym pt om s of t em porom andibular disorder: a syst em at ic review of random ised cont rolled t rials. J Oral Rehabil. 2015; 22: 15- 21.
10- Cam pos J, Gonçalves J, Cam paris D, Speciali C. Reliabilit y of a quest ionnaire for diagnosing t he severit y of t em porom andibular disorder. Rev Bras Fisiot er. 2009; 13: 38- 43.
11- Cam pos JD, Carrascosa C, Maroco J. Validit y and reliabilit y of t he Por t uguese ver sion of Mandibular Funct ion I m pair m ent Quest ionnaire. J Oral Rehabil. 2012; 39: 377- 83.
1 2 - Casan ov a- Rosado JF, Medin a- Solís CE, Vallej os- Sán ch ez AA, Casan ov a- Rosad o AJ, Her n án d ez- Pr ad o B, Av ila- Bu r g os L. Pr evalen ce an d associat ed fact or s for t em por om an dibu lar disorders in a group of Mexican adolescent s and yout h adult s. Clin Oral I nvest ig. 2006; 10: 42- 9.
1 3 - Ch est er t on LS, Sim J, Wr igh t CC, Fost er NE. I n t er r at er reliabilit y of algom et ry in m easuring pressure pain t hresholds in healt hy hum ans, using m ult iple rat ers. Clin J Pain. 2007; 23: 760- 6. 14- Cohen J. St at ist ical pow er analysis for behavioural sciences. 2nd ed. Hillsdale: Law rence Eribaum Associat es; 1988.
15- De Laat A, Meulem an H, St evens A, Verbeke G. Correlat ion bet w een cervical spine and t em porom andibular disorders. Clin Oral I nvest ig. 1998; 2: 54- 7.
16- Eriksson PO, Zafar H, Nordh E. Concom it ant m andibular and head- neck m ovem ent s during j aw opening- closing in m an. J Oral Rehabil. 1998; 25: 859- 70.
17- Gom es MB, Guim arães JP, Guim arães FC, Neves AC. Palpat ion and pressure pain t hreshold: reliabilit y and validit y in pat ient s wit h t em porom andibular disorders. Cranio. 2008; 26: 202- 10. 18- Häggm an- Henrikson B, Nordh E, Zafar H, Eriksson PO. Head im m obilizat ion can im pair j aw funct ion. J Dent Res. 2006; 85: 1001-5.
19- I báñez- García J, Alburquerque- Sendín F, Rodríguez- Blanco C, Girao D, At ienza- Meseguer A, Planella- Abella S, et al. Changes in m asset er m uscle t rigger point s follow ing st rain- count erst rain or neuro- m uscular t echnique. J Bodyw Mov Ther. 2009; 13: 2- 10. 2 0 - Jo h n MT, Dw o r k i n SF, Man cl LA. Rel i ab i l i t y o f cl i n i cal t em porom andibular disorder diagnoses. Pain. 2005; 118: 61- 9. 21- Jull GA, Falla DL, Treleaven JM, M SM, O’Leary SP. A t herapeut ic ex er cise appr oach f or cer v ical disor der s. 3r d ed. Edin bu r gh :
Churchill Livingst one/ Elsevier Science; 2004.
22- Kropm ans T, Dij kst ra P, St egenga B, St ewart R, de Bont L. Sm allest det ect able differ ence of m ax im al m out h opening in pat ient s wit h painfully rest rict ed t em porom andibular j oint funct ion. Eur J Oral Sci. 2000; 108: 9- 13.
23- Kropm ans TJ, Dij kst ra PU, St egenga B, St ewart R, de Bont LG. Repeat ed assessm ent of t em porom andibular j oint pain: reasoned decision- m aking wit h use of unidim ensional and m ult idim ensional pain scales. Clin J Pain. 2002; 18: 107- 15.
24- La Touche R, Fernández- de- las- Peñas C, Fernández- Carnero J, Escalan t e K, An gu lo- Díaz- Par r eñ o S, Par is- Alem any A, et al. The effect s of m anual t herapy and exercise direct ed at t he cervical spine on pain and pressure pain sensit ivit y in pat ient s w it h m yofascial t em por om andibular disor der s. J Oral Rehabil. 2009; 36: 644- 52.
25- La Touche R, París- Alem any A, Mannheim er JS, Angulo- Díaz-Parreño S, Bishop MD, Lopéz- Valverde- Cent eno A, et al. Does m obilizat ion of t he upper cer vical spine affect pain sensit ivit y and aut onom ic nervous syst em funct ion in pat ient s w it h cervico-craniofacial pain?: A random ized- cont r olled t r ial. Clin J Pain. 2013; 29: 205- 15.
2 6 - Lean d r i M, Got t lieb A, Cr u ccu G. Head ex t en sor r ef lex evoked by t rigem inal st im ulat ion in hum ans. Clin Neurophysiol. 2001; 112: 1828- 32.
2 8 - McNeely ML, Ar m ij o- Oliv o S, Mag ee DJ. A sy st em at ic review of t he effect iveness of physical t herapy int ervent ions for t em porom andibular disorders. Phys Ther. 2006; 86: 710- 25. 29- Oliveira- Cam pelo NM, Rubens- Rebelat t o J, Mar t í N- Vallej o FJ, Albu r qu er qu e- Sen dí NF, Fer n án dez- de- Las- Peñ as C. Th e im m ediat e effect s of at lant o- occipit al j oint m anipulat ion and suboccipit al m uscle inhibit ion t echnique on act ive m out h opening an d pr essu r e pain sen sit iv it y ov er lat en t m y of ascial t r igger point s in t he m ast icat ory m uscles. J Ort hop Sport s Phys Ther. 2010; 40: 310- 7.