www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Experimental
study
on
the
effects
of
bismuth
subgallate
on
the
inflammatory
process
and
angiogenesis
of
the
oral
mucosa
夽
,
夽夽
Eduardo
Vieira
Couto
a,∗,
Carlos
Roberto
Ballin
b,c,
Claudia
Paraguac
¸u
Pupo
Sampaio
b,c,d,
Carlos
Augusto
Seije
Maeda
d,
Carlos
Henrique
Ballin
e,
Camila
Soares
Dassi
e,
Lilian
Yukari
Miura
eaDepartmentofOtorhinolaryngology,HospitalUniversitárioEvangélicodeCuritiba(HUEC),Curitiba,PR,Brazil bDepartmentofSurgery,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
cDepartmentofSurgery,PontifíciaUniversidadeCatólicadoParaná(PUCPR),Curitiba,PR,Brazil dFunctionalRhinology,IrmandadeSantaCasadeMisericórdiadeCuritiba,Curitiba,PR,Brazil
eDepartmentofOtorhinolaryngology,PontifíciaUniversidadeCatólicadoParaná(PUCPR),Curitiba,PR,Brazil
Received15September2013;accepted9December2014 Availableonline27October2015
KEYWORDS Woundhealing; Tonsillectomy; Angiogenesis-inducing agents
Abstract
Introduction:Bismuthsubgallateisasaltderivedfromheavymetal.Theaimofthisstudywas toevaluatetheeffectofthissaltonsomephasesofhealing.
Objectives: To assess the effect of subgallate on mucosa and to evaluate the association betweentheuseofbismuthsubgallateandneogenesisofvesselsinoralmucosalwounds. Methods:Thiswasaprospectiveandexperimentalstudy.Thisstudyusedsixtyrats,whichwere dividedintocontrolandexperimentalgroups.Theanimalsweresubmittedtoasurgical proce-dure,whichcausedoralmucosalinjury.Asalinesolutionwasappliedonthewoundofthecontrol group,andintheexperimentalgroup,asolutionofbismuthsubgallatewasadministrated. Results:The experimental group showed greater inflammatory reaction with increasing monomorphicproliferation.Therewasincreasedvesselproliferationinthecontrolgroup. Conclusion: Bismuthsubgallatehadanegativeinfluenceonthehealingprocess,delayingthe rateofnewvesselformationandoptimalwoundhealing.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:CoutoEV,BallinCR,SampaioCPP,MaedaCAS,BallinCH,DassiCS,etal.Experimentalstudyontheeffectsof
bismuthsubgallateontheinflammatoryprocessandangiogenesisoftheoralmucosa.BrazJOtorhinolaryngol.2016;82:17---25.
夽夽Institution:PontifíciaUniversidadeCatólicadoParaná(PUCPR),Curitiba,PR,Brazil.
∗Correspondingauthor.
E-mail:[email protected](E.V.Couto). http://dx.doi.org/10.1016/j.bjorl.2014.12.009
PALAVRAS-CHAVE Cicatrizac¸ão; Tonsilectomia; Indutoresda angiogênese
Estudoexperimentalsobreosefeitosdosubgalatodebismutonoprocesso inflamatórioedeangiogêneseemmucosabucal
Resumo
Introduc¸ão:Osubgalatodebismutoéumsalderivadodemetalpesado.Aideiadestapesquisa éavaliarsuainterferênciaemalgumadasfasesdacicatrizac¸ão.
Objetivo:Delinearaac¸ãodosubgalato emmucosas. Avaliararelac¸ãoentreautilizac¸ãodo subgalatodebismutoeaneoformac¸ãodevasosnasferidasemmucosaoral,paraevidenciaro possívelbenefícioresultantedoseuuso.
Método: Estudo experimental, prospectivo. Utilizou-se sessenta ratos, que foram divididos igualmenteem grupocontrolee experimento.Foramsubmetidosaum procedimento cirúr-gicoondefoifeitoumalesãonamucosaoraldosanimais,após,umasoluc¸ãodesorofisiológico foiaplicadasobrealesãodogrupocontroleesobreaferidadogrupoexperimentofoiaplicada umasoluc¸ãodesubgalatodebismuto.
Resultados: o grupo experimento apresentou maior reac¸ão inflamatória com crescente proliferac¸ãomonomórfica.Vasos:houvemaiorproliferac¸ãonogrupocontrole.
Conclusões:concluiu-se queosubgalatodebismutoteveuma ac¸ãonegativanoprocessode cicatrizac¸ão,atrasandoavelocidadedeformac¸ãodosneovasoseacicatrizac¸ãoidealdaferida operatória.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Bismuthsubgallateorbismuthoxygallateisayellowish sub-stance,whichpresentsasan odorlesspowderthat suffers discoloration in the presence of sunlight.1 It is a heavy metalsaltthatispoorlyabsorbed,andhasstrongastringent power.2
Dermatol,anothernameforthesalt,hasbeen increas-inglyusedbyprofessionalsfromtheotorhinolaryngologyand dentistryareas.Duetoitshemostaticandastringent proper-ties,thesubstancemaybeusedinmanyways;amongthem, astopicaltreatmentforopenwounds,treatmentof gastro-duodenalulcers,diarrhea,odorcontrolincolostomies, in dental surgeries, epistaxis management and, empirically, inadenotonsillectomies.
The literature is not in unified opinion about the ben-efitsofsubgallatein hemostasisorthe healingeffectand therearediscrepanciesamongstudies.Itdoesnotaddress whethertherearebeneficialeffectsonhealing,andthere arefew studies with comparisonor control groups. How-ever, Arroyo Júnior et al.2 found that bismuth subgallate hasaneffectonfactor12activation,whichacceleratesthe intrinsicpathwayinthecoagulationcascade,contributingto thehemostaticcharacteristicofthiscompound.Theauthors alsodiscussedthepossibilitythatbismuthsubgallatemight inhibitfibrinolysisand,thereby,increasefibrosis.
AccordingtoHernández-Pazetal.3(fromthe otolaryn-gologyservice ofthe outpatientsurgery centerISSSTE, in Mexico City, Mexico), some methods are currently being investigatedtoreduceorpreventintraoperativeor postop-erativebleedingduringadenotonsillectomy.Forthisreason, severalmeanshave beencompared,suchasalaser, elec-trodissection, cold ablation, harmonic scalpel, or radio frequency.However,noneofthesetechniquesshowed100% efficacy.Inthissearchforanidealmethod,twosubstances
derived frombismuth (subgallate, and bismuth subsalicy-late)havebeenreported,whichexhibithemostaticeffects thatactivatefactorXIIviatheintrinsiccoagulationpathway. Whenappliedtopicallytothewound,immediatelyafter tis-sueremoval,bleedingissignificantlydecreased.
Padilla et al.4 (from the department of otorhinolaryn-gology of Centro Médico Nacional La Raza, IMSS, Mexico City,Mexico)describedbismuthsubgallateasaheavymetal that accelerates clot formation and improves hemostasis. Theyalsoreportedthatsomeauthorshave suggestedonly adrenalineonlyastheactiveingredientthathelps hemosta-sis,due toitsvasoconstrictor effect.Accordingto Padilla etal.,therehavebeenfewstudiesusingbismuthsubgallate alone (without adrenaline) todemonstrate itshemostatic effectand,considering that,theyproposedaclinicaltrial comparingthehemostaticeffectofsubgallatein adenoton-sillectomies, comparedto a control group that used only drygauze.Inthepresentstudy,bismuthsubgallateshowed noactivityasahemostaticagenttoreduce intraoperative bleeding.
The goal of this study was to assess whether bismuth subgallate interferes in any of the healing stages. As it is an inexpensiveeasy-to-handle powder, itsuse couldbe beneficialfromthe perspectiveof healing,ifcase studies documentthatbenefit.
Many otorhinolaryngology services do not use bismuth subgallate, reporting that the immediate postoperative results ofitsuse shownobenefits, whereasothersreport that ithelps tocontrolbleeding. The studies, in general, focus on its use in relation to immediate postoperative bleedingcontrol.
proliferation, contraction, andremodeling.1 The phaseof proliferationissubdividedintore-epithelialization, fibropla-sia,andangiogenesis.
Asangiogenesisisanimportanthealingphase,ifbismuth subgallateinducesincreasedangiogenicactivity,earlyand increasedneovascularizationisexpected,culminatinginan optimizationofthehealingprocess.
Angiogenesisoccursfrompreexistingvessels, inserum, andintheextracellularmatrix.Thesenewvesselsassistin granulationtissueformation,aswellasbysupplying nutri-ents and oxygen to tissues, thus they are crucial for the healingprocess,correspondingto60%oftissuerepair.5,6
Theformationofnewvesselsisessentialfortissue regen-eration and,therefore,localfactors,chemical mediators, extracellularmatrix,andmetabolicgradientsshow concom-itantdevelopment.7
Amongtheobjectivesofthisstudy,thegeneralonewas outliningsubgallateactiononmucosaltissueandasa spe-cificobjective,theassessmentoftheassociationbetween the use of bismuth subgallate and the formation of new vesselsin oral mucosa wounds, thus showing thepossible resultingbenefitsofitsuse,sothatnewprotocolscanfinally beutilizedinotorhinolaryngologyservicesinvolvingtheuse ofthissalt,mainlyinoralcavitysurgeries.
Methods
Surgicalprocedure
The experimentswere carried out from September 24 to October 1, 2012. A total of 60 young adult male Wistar rats(Rattusnorvegiccusalbinus),aged110daysandmean weightbetween250gand300g,wereassessed.Thesample sizewasestimatedaccordingtostudiesintheliteratureand theprojectfollowedtheguidelinesofLaw11,797of Octo-ber8,2008,regulatedbyDecreeNo.6899of15July2009 andtherecommendationsoftheBrazilianCollegeofAnimal Experimentation.The studywasperformedafterapproval bytheethicscommitteeonanimalstudiesunderNo.666.
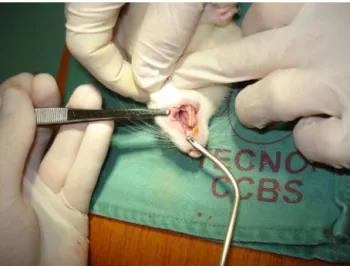
The animals wereanesthetizedwith0.1mL/100gbody weightwithamixtureof1mLofketamine(50mg)and1mL xylazine2%(20mg),IM,intheposteriorportionofthethigh. Subsequently,theywere placedin theprone positionand hadthelowerandupperlimbsattachedtoawoodensupport (Fig.1).Withtheaidofasuitablemouthopener,awound ofapproximately0.7cmindiameterwasmadeontheleft sideoftheoralmucosa,byusingabiopsyforceps.
At this point, it wasdecidedtocreate a singlewound to reduce the aggression to the animals and tofacilitate theirrecovery;theleftsidewaschosentostandardizethe study.Itwasdecidedtousethebiopsy forcepsinsteadof apunch biopsy devicedue tothechance that thesecond toolwouldcompletelypiercetherat’soralcavitywall.After the surgery, the animals received dipyrone (at a dose of 10mg/kg)IMforanalgesia,accordingtowhatwasproposed toandacceptedbyCEUA.
The animals were randomly marked and divided into threegroupsof10animals,whichreceived0.5mgoftopic bismuthsubgallateafter woundwithbiopsy forceps.Each group was reoperated for wound removal and evaluation after24h(GII),threedays(GIII),andsevendays(GIV)after
Figure1 Surgicalwoundinduction.
Figure2 WoundremovalonD7.
thelesion(Fig.2).Theremaining30animalscomprisedthe controlgroup(GI),whichwasalsodividedintothreegroups oftenanimals,whichwerealsoevaluatedafter24h,three days,andsevendays(Table1).
The control group was treated by washing the wound with0.9%NaClsolution,asrecommendedbytheliterature. Thefragmentwasremovedwithamarginofapproximately 0.5cm around the entire mucosal lesion, which went as deep as the buccal musculature of the rat. Immediately after the end of each surgery, the animals were eutha-nizedbyalethalintraperitonealdoseofthiopentalsodium (120mg/kg).There wasonlyonelossduring thestudy,an animal fromthe control group,number 57 (Table 2),five dayspost-operatively.
Histologicalandimmunohistochemicalanalysis
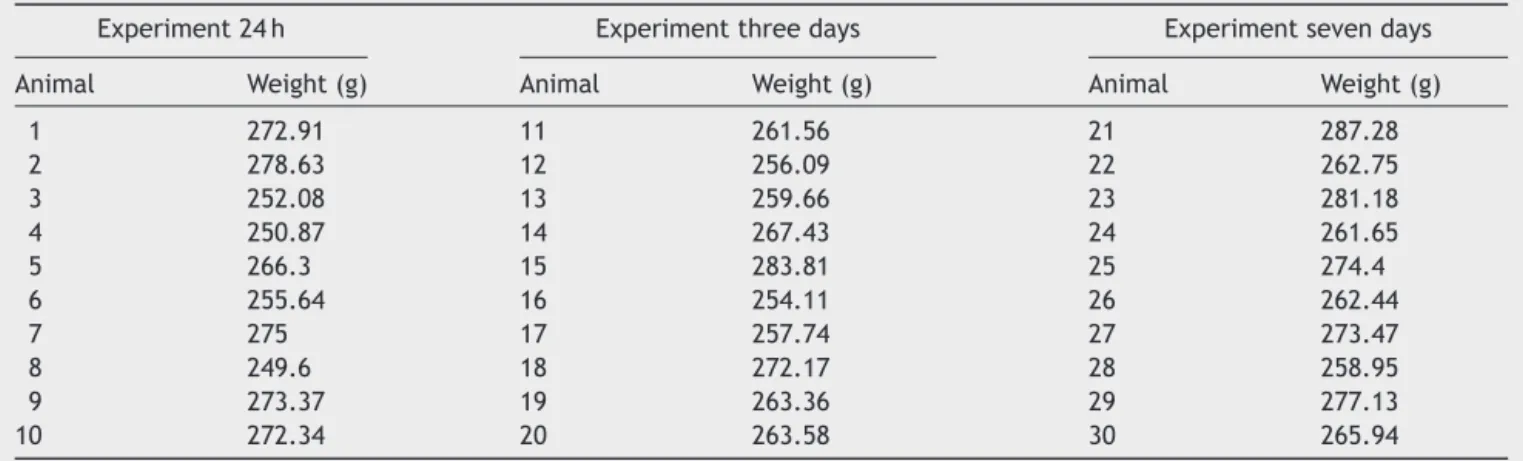
Table1 Identificationofstudiedsampleswithbismuthsubgallate.
Experiment24h Experimentthreedays Experimentsevendays
Animal Weight(g) Animal Weight(g) Animal Weight(g)
1 272.91 11 261.56 21 287.28
2 278.63 12 256.09 22 262.75
3 252.08 13 259.66 23 281.18
4 250.87 14 267.43 24 261.65
5 266.3 15 283.81 25 274.4
6 255.64 16 254.11 26 262.44
7 275 17 257.74 27 273.47
8 249.6 18 272.17 28 258.95
9 273.37 19 263.36 29 277.13
10 272.34 20 263.58 30 265.94
Table2 Identificationofstudiedsamplesfromthecontrolgroup.
Control24h Controlthreedays Controlsevendays
Animal Weight(g) Animal Weight(g) Animal Weight(g)
31 271.06 41 274.35 51 284.02
32 268.96 42 278.96 52 284.6
33 257.99 43 282.05 53 265.88
34 281.5 44 272.44 54 254.1
35 268.2 45 256.63 55 282.46
36 251.8 46 262.35 56 261.76
37 271.26 47 245.71 57 236.3
38 249.7 48 249.17 58 244.34
39 278.79 49 247.94 59 276.49
40 271.49 50 262.56 60 249.1
consideredstatisticallysignificant.Datawereanalyzedusing theSPSSv.20.0software.
Thesectionusedforthehistologicalanalysiswasplaced onidentified cardboard and secured withcolored pins to schematizewoundpositionintherat.Subsequently,itwas dippedinacontainerwith10%formaldehydefor24h.After that,itwasembeddedinparaffinblocks,andsectionedat 5-mthicksections.
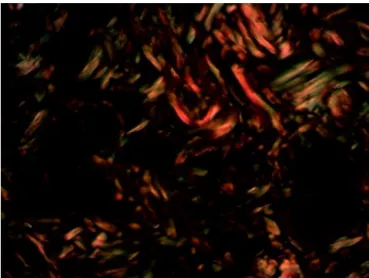
Thehistologicalsectionswerestainedwith hematoxylin-eosin and picrosirius. For each slide, the reading was performedin threefields forboth stains, with200× mag-nification,overthelesionarea(Figs.3and4).
Withhematoxylin-eosinstain,theinflammatoryprocess wasassessed, countingmonomorphonuclear and polymor-phonuclearcellsandthenumberofvessels.Thepicrosirius stain assesses collagen through its specific birefringence, identifyingthefiberorientationthroughapolarizingoptical microscope.Thethickerfibers,withgreaterbirefringence, willappearcoloredinorangeandredtones,identifyingthe typeIcollagen;thethinnerfibers,withlowerbirefringence, willdisplayagreencolor,identifyingtypeIIIcollagen.
An Olympus BX50 microscope witha 3CCD Pro-S series capturecameraswasusedtogetherwiththeImage-ProPlus program,v.4.5,byCybernetics.Theimageswerecaptured usingaDino-Litecameraandwereanalyzedusingthe appli-cationImagePlus4.5forWindowsinPentiumIIIcomputer. Afterthereading, theareas withgreater cellularitywere
Figure3 MaskusedforthereadingofPicrosiriusstaining.
defined, which were submitted to a punch, in order to preparethetissuemacroarray(TMA)for immunohistochem-istryanalysis(Fig.5).
Figure4 SlideshowingPicrosiriusstainingofintegra.
Figure5 Finishedslidesand paraffin afterpunch was per-formed.
antigenisasingle-chaintransmembraneglycoprotein asso-ciatedwithhumanhematopoieticprogenitorcells(Fig.6). The antigen-antibody reaction is defined by a brownish chemicalreaction,allowing thequantificationand qualifi-cationofthehealingprocess(Fig.7).
Statisticalanalysis
The analysiswasperformed takingintoaccountthestudy results, described as mean, median, minimum, maxi-mumvalues, and standard deviations. The nonparametric Mann---Whitneytestwasusedforthecomparisonofthestudy andcontrolgroups.Comparisonsofthedaysofassessment withineachgroupwereperformedusingthenonparametric Kruskal---Wallistest.
Results
Collagen is the main component of tissue extracellular matrix.Itisstructuredintoadenseanddynamicnetwork, resultingfromitsconstantdepositionandresorption. Col-lagendegradationstartsearlyandisveryactiveduringthe
Figure6 MaskusedforthereadingofCD34marker.
Figure7 SlideshowingCD34markerofintegra.
inflammatoryprocess;duringthisprocess,itispossible to evaluate the healing activity, mainly by investigating its immatureform,collagentypeIII,whichcomprises approxi-mately40%ofthegranulationtissue.
Maturecollagen
Table3 Comparison inrelation to mature collagen. The table shows mean, median, minimum, maximum, andstandard deviation.Italsoshowsthep-valuesofstatisticaltests.
Day Group n Mean Median Minimum Maximum SD p-Valuea
1 StudyControl 1010 82.388.3 86.595.0 59.655.2 95.599.1 12.213.9 0.143
3 StudyControl 1010 86.292.2 87.592.6 63.482.0 99.298.2 10.05.2 0.123
7 StudyControl 109 91.794.7 93.796.2 82.280.3 100.097.9 5.26.1 0.079
SD,standarddeviation.
aNonparametricMann---Whitneytest,p<0.05.
Table4 Comparison inrelationtoimmaturecollagen.The tableshows mean,median,minimum, maximum,andstandard deviation.p-Valuesofthestatisticaltestsarealsogiven.
Day Group n Mean Median Minimum Maximum SD p-Valuea
1 StudyControl 1010 17.711.7 13.55.0 4.50.9 40.444.8 12.213.9 0.143
3 StudyControl 1010 13.87.8 12.57.4 0.81.8 36.618.0 10.05.2 0.123
7 StudyControl 109 8.35.3 6.33.8 2.10.0 17.819.7 5.26.1 0.079
SD,standarddeviation.
aNonparametricMann---Whitneytest,p<0.05.
Table5 Comparisoninrelationtoinflammatorycellgrowth.Thetableshowsmedian,minimum,andmaximumvalues.p-Values ofstatisticaltestsarealsogiven.
Day Group n Median Minimum Maximum p-Valuea
1 StudyControl 1010 00 −1 0
−2 0 0.684
3 StudyControl 1010 00 −1 2
−2 1 0.481
7 StudyControl 109 10 0 3
−1 1 0.043
aNonparametricMann---Whitneytest,p<0.05.
Immaturecollagen
Initially,oneach assessmentday (one,three, andseven), thenullhypothesisthatimmaturecollagenpercentagewas equalinbothgroupswastestedvs.thealternative hypoth-esisofdifferentimmaturecollagenpercentages(Table4). Then, withineach group, the null hypothesis that imma-turecollagen percentagewasthesameonthe threedays ofassessmentwastestedvs.thealternativehypothesisthat thepercentageswerenotallthesame.Theresultsof imma-ture collagen assessment showed no differenceregarding its their percentage on the days assessed in the control (p=0.326)andexperimentalgroups(p=0.180).
Inflammatoryprocesscellcount
Initially,oneach assessmentday (one,three, andseven), the null hypothesis that the cell count score of the
inflammatoryprocesswasequalinboth groupswastested vs.thealternativehypothesisofdifferentscores(Table5). Then,within each group, the null hypothesis that the scores were the same on the three days of assessment was tested vs. the alternative hypothesis that the scores were not all the same. For the study group, the test resultsindicatedrejectionofthenullhypothesis(p=0.016). Consideringthatasignificantdifferencewasfoundbetween thedays,theywerecomparedtwo-by-two(Table6).
Table6 p-Valueassessment.Thetableshowsp-valuesof statisticaltests.
Compareddays p-Value
Table7 Comparisoninrelationtothenumberofvessels.Thetableshowsmedian,minimum,andmaximumvalues.p-Values ofstatisticaltestsarealsogiven.
Day Group n Mean Median Minimum Maximum SD p-Valuea
1 StudyControl 1010 22.320.2 19.519.0 7.02.0 38.050.0 13.49.4 0.529
3 StudyControl 1010 28.743.2 29.039.5 15.012.0 41.070.0 18.69.1 0.052
7 StudyControl 109 62.953.8 68.048.5 10.011.0 148.0120.0 47.931.2 0.968
SD,standarddeviation.
a NonparametricMann---Whitneytest,p<0.05.
Table8 p-Valuesofthestatisticaltests.
Compareddays p-Value
Dayone×daythree 0.007 Dayone×dayseven 0.001 Daythree×dayseven 0.480
Forthecontrolgroup,thetestresultsindicatedthe non-rejection of the null hypothesis (p=0.289). Thus, in this group,therewasnosignificantdifferencebetweenthedays ofassessmentinrelationtothecellcountscore.The exper-imental group showed higher inflammatory reaction with increasingmonomorphicproliferation(p=0.016).
Numberofvessels
Hematoxylineosinstaining
Initially,oneachdayofassessment(one,three,andseven), the nullhypothesis in which the numberof vessels is the sameinbothgroupswastestedvs.thealternative hypoth-esisofdifferentnumbersofvessels(Table7).
Then, within each group, the null hypothesis that the scoreswerethesameonthethreedaysofassessmentwas testedvs. thealternativehypothesis thatthescores were notallthesame.Therewasagreaterproliferationof ves-selsinthecontrolgroup(p=0.006).Theexperimentalgroup showed nosignificant vessel proliferation onthe assessed days(p=0.119;Table8).
CD34marker
Initially,oneachdayofassessment(one,three,andseven), thenullhypothesisthattheCD34resultwouldbethesame inbothgroupswastestedvs.thealternativehypothesisof differentresults(Table9).Then,withineachgroup,thenull hypothesisthattheCD34resultwasthesameonthethree daysofassessmentwastestedvs.thealternativehypothesis thattheresultswerenotallthesame.
Therewasgreater proliferationinthecontrolgroupon dayseven(p=0.036),whereastherewasnosignificant pro-liferationofvesselsintheexperimentalgroup.
Discussion
Since bismuth subgallateis commonly used in medical practice,especiallybyotorhinolaryngologistsand dermato-logists,wedesignedthisstudytoclarifythebenefitsofthe saltinsurgical procedures.Currently it is usedcommonly in tonsillectomies in several services, mainly in southern Brazil.The authorscertainly haveobserved itsbenefitsin theirservice;itprovidesclearervisualizationofthe bleed-ingpointsinoropharyngeallesions,inadditiontoproviding possiblebeneficialeffectsonhealingandhemostasis.
Thehealingprocessinvolvesseveralreactionsoccurring simultaneously;thus,itisnotpossibletoseparatethe begin-ningandendofeachstage.Intheory,however,thereaction is divided into steps: coagulation, inflammation, prolifer-ation,contraction, andremodeling.1 This process hasthe ultimategoaloftissuerepair,butthatrequiresallstepsto occursatisfactorily.
Coagulation starts a few seconds after the creation of the wound. The clot and the extracellular matrix are
Table9 Comparisoninrelationtoangiogenesis.Thetableshowsmedian,minimum,andmaximumvalues.p-Valuesofstatistical testsarealsogiven.
Day Group n Mean Median Minimum Maximum SD p-Valuea
1 StudyControl 108 67429371 59497737 13483341 13,10621,206 36265981 0.460
3 StudyControl 109 58469406 49378188 21313814 13,49315,493 37353999 0.079
7 StudyControl 98 43477575 44196799 2437619.8 15,7507590 22813843 0.036
SD,standarddeviation.
formed;theycontainchemicalcompounds(growthfactor) andinflammatorymediators(cytokines) thatcontributeto there-epithelializationandwoundcontractionprocesses.
Theinflammatoryprocessischaracterizedbyhemostasis, cellmigration,andprovisionalmatrixdeposition.Platelets are essential for the formation of the hemostatic plug that secretes multiple mediators, including growth fac-torsreleasedintothedamagedarea.Inducedbythrombin, theyalsoundergoplatelet degranulationand release sev-eralgrowthfactors,suchasplatelet-derivedgrowthfactor (PDGF),transforming growth factor  (TGF-),epidermal growthfactor(EGF),thetransforminggrowthfactor␣ (TGF-␣),and the vascular endothelial growthfactor (VEGF), in additiontoadhesiveglycoproteins,suchasfibronectinand thrombospondin, which areimportant constituents of the provisionalextracellularmatrix.5,6,8
Themacrophageisthemostimportantcellinthehealing process.Inadditiontoaprominentroleinphagocytosisof cellulardebris,macrophagesalsosecretechemotactic fac-torsthatattractotherinflammatorycellstothewoundsite andproduceprostaglandins,which actaspotent vasodila-torsaffecting the permeabilityof microvessels.They also preparethewoundfortheproliferative phase.The prolif-erationinhealingscarformationpromoteswoundclosure. Thisphaseconsistsofre-epithelialization,fibroplasia,and angiogenesis.
Itwasdecided inthis studytofocusonthe processof angiogenesis,asitiscrucialforhealingandaccountsfor60% oftherepairtissue.5,6Stashaketal.,citedbySouzaetal.9 reportedthatangiogenesisshortenshealingtimeby increas-ingthesupplyofnutrientsandcellentryintotheaffected area,thusdecreasingwoundretractiontime.Balbinoetal.10 reportedthemigrationofendothelialcellsthroughthe ves-selwall where theythen travelthroughthe extracellular matrixtoward thesiteof injury.Oncein theouter region of the vessel, theyundergo a differentiation processand acquirethecapacitytoformnewcapillarytubules. Migrat-ingendothelialcells formacapillarysproutoutsideofthe vessel,whichjoinstheoriginatingcapillary,restoringblood flow.
Theformationofthenewvesselbeginswithtissueinjury, withtheactivationofmacrophagesandthesubstancesthey produce.The proteases (plasmin and collagenases)digest thebasementmembraneandallow endothelialcells stim-ulatedby angiogenic cytokines to form the new vascular bundle,which invadesthe wound.Angiogenesisceases by apoptosis.11,12
Thespecificmechanismresponsibleforcontractionmay beduetomovementofmyofibroblaststhroughthe extracel-lularmatrix. The latterhave contractileactinand myosin fibers in their cytoplasm that originate from mesenchy-malstemcells,circulatingmononuclearcellsorfibrocytes situatedaroundtheadventitiaoflocalbloodvessels,a pro-cessfacilitatedbyTGF-.Fibroblastsonthewoundmargins showachange inphenotypetomyofibroblasts,with func-tional characteristics similar to those of smooth muscle. Thesecellsarealignedarounddepositsofnewextracellular matrix,establishingcell-to-cellconnectionsandgenerating tensilestrength.10
Collagen modeling is a balance between the synthe-sisand degradation of collagen. This process is mediated by proteolytic enzymes (metalloproteinases), epidermal
cells, endothelial cells,and fibroblasts.11 During remodel-ing,thereareseveralstagesofproduction,digestion,and orientation of thecollagen fibers. The fibers aredigested by collagenase, resynthesized, rearranged according to the array of adjacent connective tissue fibers, and con-nectedlaterallybycovalentbonds.Theamountofcollagen increases during the first week, and by 21 days, there is abalancebetweenproductionanddegradation.Scar resis-tanceisgivenbytheamountofdepositedcollagenandthe manner in which the fibers are arranged, with resistance beinggreater than itwould beexpectedonly by collagen deposition.Thisprocessbeginsaroundthethirdweekafter theinjuryandpersistsformonthsoryears.10,13
The objective for surgical recovery is for faster and more effective tissue recovery. The present study aimed toevaluatebismuthsubgallateonwoundhealing,hopingto improvetheresponsetotrauma.Bismuthsubgallateor bis-muthoxygallateisayellowishsubstance,whichpresentsas an odorless powder thatsuffers discolorationin the pres-enceofsunlight.1Itisaheavymetalsalt,littleadsorbed, andhasstrongastringentpower.2
This compound has been used to containhemorrhages in tonsillectomy, turbinectomy, andpartial hepatectomy.2 Bismuthsubgallate,aheavymetal,relativelyinsoluble,and poorlyabsorbedfromthesurgical bed,is inexpensiveand easy touse, andis effective asalocal hemostaticagent. Itsmechanism of action is attributed tothe activation of clottingfactor12,inadditiontoapresumedlocalastringent effect.14
Arroyo Júnior et al.2 also stated that bismuth subgal-lateacts intheactivation offactor 12,whichaccelerates the intrinsic coagulation cascade pathway, contributing to the hemostatic characteristic of this compound. The authorsdiscussedthepossibilitythatbismuthsubgallatecan inhibitfibrinolysisand,thereby,increasefibrosis.This state-mentpromptedustodesignthisstudytodemonstratethe contribution of bismuth subgallate tothe healing process and,consequently,toincreasedformationofnewvessels.
Withrespectto theinflammatory processasmeasured by the number of mononuclear and polymorphonuclear cells,thestudydemonstratedthattheexperimentalgroup hadreducedinflammatoryprocesstime,i.e.,thetissuewas exposed toa faster inflammatory reaction,which did not resultintheexpectednewcellformation.
The study demonstrated that bismuth subgallate pro-motedasignificantdifferenceininflammatorypattern,and on the seventh day, the bismuth subgallate promoted a reduction inthe inflammatory process,leading toa more markedchronicstatusthaninthecontrolgroup.
Collagen activity was another factor evaluated in the presentstudy.Itwasaffirmedthatcollagenisthemost abun-dantconnectivetissueproteininthehealingphase.15 This proteinprimarily comprisestheextracellularmatrixandis partoftheremodelingphaseofhealing.
TypeIcollagenisthemostcommoncollagentype;itis synthesized by fibroblasts andis most prevalent in bones andtendons.TypeIIIismostcommonlyfoundinsofttissues, suchasbloodvessels,dermis,andfascia.Thehealthydermis containsapproximately80%oftypeIcollagenand20%type IIIcollagen.Granulationtissueexpresses30---40%oftypeIII collagen,immaturecollagen.15
There wasnodifferenceincollagen production,asthe control and experimental groups showed the same effi-ciency.
Conclusion
Apossiblenegativeeffectofbismuthsubgallateonthe heal-ingprocessinthemucosalwoundsoftheassessedanimals wasobserved.The saltresulted in lesstissue exposureto theinflammatoryprocess,leadingtoanearlychronicstatus withsome stabilizationin the numberof vessels, thereby evendelayingthephysiologicalhealingprocessand impair-ingangiogenesis.
Thebismuthsubgallatestimulustofibroplasiawas indif-ferent,asitdidnotinterfereincollagenformation,either initsimmatureormatureform.
But when considering the entirety of the healing pro-cess,wedemonstratedthatthesubgallatedoesnotimprove thequalityofhealing,andtheheavymetalalsointerferes bydelaying the rateof newvesselformation and optimal healingofthesurgicalwound.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MandelbaumSH,DiSantisEP,MandelbaumMHS.Cicatrizac¸ão: conceitosatuaiserecursosauxiliares/ParteI.AnBrasDermatol. 2003;78:393---410.
2.ArroyoJúniorPC,SilvaRCMA,SantiNetoD,SantanaJúniorD, FerreiraFD,SilvaRF.Usodosubgalatodebismutopara hemosta-sialocalemhepatectomisasparciaisderatos.RevColBrasCir. 2004;31:165---71.
3.PazSHH,ReyesAO,GuzmánCMG.Estudiocomparativodedos agentes hemostáticos adicionados con epinefrina en la ade-noamigdalectomía.RevEspMédQuir.2012;17:3---7.
4.Padilla RM, Valdés CM, Asato JR, Márquez M, Gutiérrez SC, GonzálezYA,et al. Eficaciadelsubgalato debismuto,como agente hemostático tópico, en el sangrado transoperatorio de la adenoamigdalectomía o amigdalectomía. An Orl Mex. 2012;57:65---8.
5.ArnoldF,WestDC.Angiogenesisinwoundhealing.Pharmacol Ther.1991;52:407---22.
6.Mendonca RJ, Coutinho-Netto J. Aspectos celulares da cicatrizac¸ão.AnBrasDermatol.2009;84:257---62.
7.FonsecaVRCD,MalafaiaO,RibasFilhoJM,NassifPAN,Czeczko NG, Marcondes CAP, et al. Angiogenesis, fibrinogenesis and presence of synechiae after exeresis of a swine vocal fold mucosal microflap and use oftopical mitomycin-C. Acta Cir Bras.2010;25:80---5.
8.StreitM,VelascoP,RiccardiL,SpencerL,BrownLF,JanesL, etal.Thrombospondin-1suppresseswoundhealingand granu-lationtissueformationintheskinoftransgenicmice.EMBOJ. 2000;19:3272---82.
9.SouzaDW,MachadoTSL,ZoopaALV,CruzRSF,GáragueAP,Silva LCLC.Ensaiodaaplicac¸ãodecremeàbasedeTriticumvulgare nacicatrizac¸ãodeferidascutâneasinduzidasemeqüinos.Rev BrasPlMed.2006;8:9---13.
10.Balbino CA, Pereira LM, Curi R. Mecanismos envolvidos na cicatrizac¸ão: uma revisão. Rev Bras Cienc Farm. 2005;41: 27---51.
11.Hanson D, Langemo D, Thompson P, Anderson J, Hunter S. Understandingwoundfluidandthephasesofhealing.AdvSkin WoundCare.2005;18:360---2.
12.SingerAJ,ClarkRA.Cutaneouswoundhealing.NEnglJMed. 1999;341:738---46.
13.BaumCL,ArpeyCJ.Normalcutaneouswoundhealing:clinical correlationwithcellularandmolecularevents.DermatolSurg. 2005;31:674---86.
14.Molina FD, Maniglia JV, Magalhães FP, Dafico SR, Rezende RS. A eficácia do subgalato de bismuto em tonsilectomias comoagentehemostático.RevBrasOtorrinolaringol.2000;66: 194---7.