Braz. Dent. J. vol.14 número2
Texto
Imagem

Documentos relacionados
Foram incluídos todos os estudos encontrados na estratégia de busca que preencheram os critérios de inclusão, listados a seguir: a) estudos primários que realizaram ensaios clínicos
Conforme as respostas de grande parte das participantes, a vida sexual também não está satisfatória e isso mostra que a qualidade de vida após uma gravidez precoce e
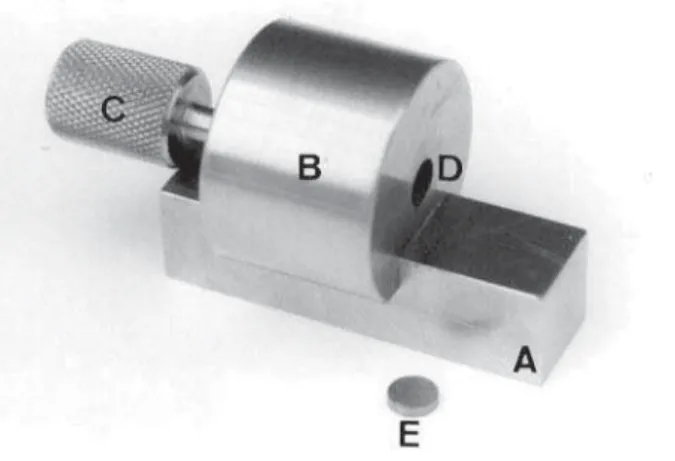
This study evaluated the effect of chemical and mechanical surface treatments for cast metal alloys on the bond strength of an indirect composite resin (Artglass) to commercially
The aim of this study was to evaluate the shear bond strength (SBS) of metallic orthodontic brackets bonded to bovine teeth using light-activated or chemically activated composite
This study evaluated the masking ability of different porcelain thicknesses and combination of enamel and/or dentin porcelain layers over simulated background dental substrates
materials were based on literature data (Table 1); and GIE - mechanical properties of resin cement, composite resin core, metal coping and porcelain were determined by the
This study evaluated the effects of three metal primers and one multi-mode adhesive system on the shear bond strength (SBS) of a flowable composite resin to nickel-chrome metal
Normalização contabilística - neste último grupo, estendido por sete questões, o nosso objetivo é saber se o respondente conhecia o SNC-ESNL; em que medida concorda com a
