Immunoblotting analyses using two-dimensional gel electr ophor esis
of
Trypan osom a cru zi
excr eted-secr eted antigens
Análise de antígenos excretados-secretados de Trypa no so m a cruzi
por
im m uno blo tting em gel bidimensional
Adr iano Gomes Silva
1, Elisangela Paula Silveir a-Lacer da
2, Jair Per eir a Cunha-Júnior
1,
Mar ia Apar ecida de Souza
1and Silvio Favor eto Junior
1ABSTRACT
Trypano so ma c ruzi trypo m a sti go te s e xc re te - se c re te a c o m ple x m i xtu re o f a n ti ge n i c m o le c u le s. Thi s a n ti ge n i c m i xtu re de n o m in a te d trypo m a stigo te e xc re te d- se c re te d a n tige n s c o n ta in s a 150- 160 k Da b a n d tha t sho ws e xc e lle n t pe rfo rm a n c e i n Ch a ga s’ d i se a se d i a gn o si s b y i m m u n o b lo tti n g. Th e p re se n t stu d y p a rti a lly c h a ra c te ri ze d b y two - d i m e n si o n a l ge l e le c tro pho re sis the im m u n o re a c tivity a ga in st the 150- 160k Da pro te in u sin g se ra sa m ple s fro m c ha ga sic pa tie n ts in diffe re n t pha se s o f the di se a se . Trypo m a sti go te e xc re te d se c re te d a n ti ge n pre pa ra ti o n s we re su b je c te d to hi gh re so lu ti o n two -dim e n sio n a l ( 2D) ge l e le c tro pho re sis fo llo we d b y im m u n o b lo ttin g with se ra fro m c ha ga sic a n d n o n - c ha ga sic pa tie n ts. The 150- 160k Da pro te in pre se n te d fo u r iso fo rm s with iso e le c tric fo c u sin g ra n gin g fro m 6.2 to 6.7. The fo u r iso fo rm s we re re c o gn ize d b y IgM fro m a c u te pha se a n d IgG fro m c hro n ic pha se se ra o f c ha ga sic pa tie n ts. The 150- 160k Da iso fo rm with IF o f a ppro xim a te ly 6.4 b e c a m e the im m u n o do m in a n t spo t with the pro gre ssio n o f the dise a se . No c ro ss- re a c tivity wa s o b se rve d
with n o n - c ha ga sic o r pa tie n ts in fe c te d with Leishmania sp. In this stu dy we pro vide b a sic k n o wle dge tha t su ppo rts the
va lida tio n o f trypo m a stigo te e xc re te d- se c re te d a n tige n s fo r se ro lo gic a l dia gn o sis o f Cha ga s’ dise a se .
Ke y-words: Tr ypano so ma c r uzi. Ex c re te d - se c re te d a n ti ge n s. Two - d i m e n si o n a l ge l e le c tro p h o re si s. Im m u n o b lo tti n g.
RESUMO
Fo rm a s tripo m a stigo ta s de Trypanosoma c ruzi e xcre ta m /se cre ta m um a co m ple xa m istura de m o lé cula s a ntigê nica s. Essa m istura
é cha m a da trypomastigote exc reted-sec retedantigens e co nté m um a b a nda de m a ssa m o le cula r e m to rno de 150- 160k Da q ue
po ssui e xce le nte pe rfo rm a nce pa ra dia gnó stico de do e nça de Cha ga s e m immunoblotting. No pre se nte e studo fo i ca ra cte riza do
pa rcia lm e nte , po r ge l b idim e nsio na l, a pro te ína de 150-160k Da pe la a ná lise da re a tivida de de a ntico rpo s de pa cie nte s cha gá sico s
na s dive rsa s fa se s da do e nça . Pro te ína s do trypomastigote exc reted-sec reted antigens fo ra m se pa ra da s po r e le tro fo re se de a lta
re so luçã o e m dua s dim e nsõ e s ( 2D) e sub m e tida s a immunoblotting co m so ro s de pa cie nte s cha gá sico s e nã o cha gá sico s. A
pro te ína de 150-160k Da fo i ide ntifica da e m q ua tro iso fo rm a s co m po nto s iso e lé trico s va ria ndo e ntre 6,2 a 6,7. As q ua tro iso fo rm a s fo ra m re co nhe cida s po r a ntico rpo s IgM na fa se a guda e po r a ntico rpo s IgG na fa se crô nica da do e nça de Cha ga s. A iso fo rm a de 150- 160k Da , co m po nto iso e lé trico de a pro xim a da m e nte 6,4 to rno u- se im uno do m ina nte de ntre a s de m a is co m a pro gre ssã o da do e nça . Nã o fo i de te cta da re a tivida de cruza da co m o s so ro s de pa cie nte s nã o cha gá sico s o u pa cie nte s infe cta do s
co m Leishmania sp. Os da do s o b tido s ne sse tra b a lho , re fo rça m a im po rtâ ncia da utiliza çã o do trypomastigote exc reted-sec reted
antigens pa ra o dia gnó stico so ro ló gico da do e nça de Cha ga s.
Palavr as-chave s:Tr ypano so ma c r uzi. An tí ge n o s e xc re ta do s/se c re ta do s. Ele tro f o re se e m du a s di m e n sõ e s. Immuno b lo tting.
1 . Lab o r ató r io de Imuno lo gia do Instituto de Ciê nc ias B io mé dic as da Unive r sidade Fe de r al de Ub e r lândia, Ub e r lândia, MG. 2 . Instituto de Ciê nc ias B io ló gic as da Unive r sidade Fe de r al de Go iás, Go iânia, GO. 3 . De par tame nto de Ciê nc ias B io ló gic as da Unive r sidade Estadual de Santa Cr uz, Ilhé us, B A, B r asil
Apo io financ e ir o : CNPq .
Addr e ss to: Dr. Silvio Favo r e to J unio r. R. Espír ito Santo 3 1 4 /2 1 , 3 8 4 4 0 - 6 6 0 Ub e r lândia, MG, B r asil. Te l: 5 5 3 4 3 2 3 2 - 4 2 3 9
Chagas’ disease caused by Trypa no so m a cruzi, is still a major
health problem in Latin America. Despite the decrease in incidence and prevalence in endemic areas2 6 2 7, the World Health Organization
has estimated 1 6 -1 8 million infected people and approximately
9 0 million individuals undeniably living at risk of c ontac t with
T. cruzi2 0. The debilitating morbidity among these infected persons
remains a serious obstacle to health and economic development
in Latin America, particularly in poor rural areas.
Currently, the procedures available for control of Chagas’ disease
are limited. There are no vaccines available and curative measures
are restricted to two drugs. Chemotherapy is most effective during the acute and early chronic phase of infection, but has several adverse
effects and may not always eliminate the parasite6.
The ac ute phase of Chagas’ disease follows the introduc tion
of infec tive forms by vec tor transmission or c ontaminated blood
tr ansfusio n. High numb e r o f par asite s in the b lo o dstr e am, fe ve r, adenomegaly and presenc e of spec ific IgM antibodies
c har ac te r ize this phase . Ho we ve r, the se sympto ms ar e no t
frequently observed in endemic areas, where the infection usually
has a benign clinical course leading to an indeterminate phase1 9 2 4. Late r in life , 1 5 - 2 0 % o f individuals in this inde te r m inate
asymptomatic phase evolve to a severely inc apac itating c hronic
phase, the triggering fac tors for this outc ome remain unknown8.
Serological diagnosis of american trypanosomiasis currently
relies upon indirect immunofluorescence, indirect hemagglutination and enzyme-linked immunosorbent assay ( ELISA) . Most of the
commercial tests currently available use whole or semi-purified
fractions of T. cruzi epimastigotes as the source of antigen. Despite
a high sensitivity for antibody detec tion in c hronic patients, epimastigote antigens produce false positive reactions and produce
cross-reactivity with sera from patients with other infections, mainly
leishmaniasis5. Thus, several authors have used recombinant antigens
for Chagas’ disease sc reening1 6 2 8 2 9. However, the variation in sensitivity, specificity, antigenic preparation and standardization of
reagents and procedures reported by different laboratories leads to
a considerable percentage of unsatisfactory results that need to be
confirmed by other methods3 11. This is a critical issue for blood banks, as none of the methods available can be considered sufficiently
sensitive for an efficient donor screening of Chagas’ disease21.
Trypomastigote forms of the parasite sec rete several antigens
into the supernatant of infec ted c ells in c ulture that inc ludes
glyc osidases2 3, glyc osyltransferases4 and proteases2 1 3 3 3. This
mixed group of molec ules is rec ognized by antibodies produc ed
during the ac ute and c hronic phase of Chagas’ disease1 4 9 and
generally is named trypomastigote exc reted– sec reted antigens
( TESA)3 0. When these sec reted antigens are used to identify
antibody populations present in the serum of c hronic patients
by immunoblotting, a 1 5 0 -1 6 0 kDa protein is rec ognized from
1 0 0 % of c hronic c hagasic sera and displays no c ross-reac tivity
with other parasitic diseases2 1 3 0. Rec ent reports have shown that
TESA utilized in ELISA assays result in exc ellent sensitivity and
spec ific ity for Chagas’ diagnostic , in both ac ute and c hronic
patients3 1.
Our aim in this study was to par tially c har ac te r ize the
1 5 0 1 6 0 k Da c o mpo ne nt o f TESA using high r e so lutio n two
-dime nsio nal e le c tr o pho r e sis fo r pr o te in se par atio n and se r a
fr o m patie nts in diffe r e nt phase s o f T. c ru zi infe c tio n as pr o b e s. We ho pe to pr o vide b a sic k no wle dge tha t c o uld
suppo r t the validatio n o f TESA fo r se r o lo gic al diagno sis o f
Chagas’ dise ase .
MATERIAL AND METHODS
Human ser a. We collected sera samples from 2 5 chagasic seropositive patients and 2 0 non-chagasic seronegative patients from Brazil. Among the selected chagasic patients, ten were in
chronic phase, with positive serology for Chagas’ disease following
the c r ite r ia utilize d fo r b lo o d do no r s sc r e e ning ( indir e c t
immunofluorescence and ELISA) . All chronic patients’ presented negative results for specific IgM and both tests were positive for
IgG; physical examination and electrocardiography were performed
for clinical assessment. Early acute patients included one case of
ac c ide ntal lab o r ato r y infe c tio n and fo ur c ase s o f ve c to r ial transmission. Clinical symptoms, parasitological tests and presence
of specific IgM established the presence of acute disease. These
five patients had either absent or low levels of spec ific IgG as
detected by conventional serology, which in addition to clinical and epidemiological data, allowed their classification as early acute
infection. Ten cases of vectorial transmission presenting with high
titers of specific IgM and IgG were classified as late acute infection
irrespective of the presence or absence of clinical symptoms. The twenty non-chagasic seronegative patients consisted of ten cases
of cutaneous leishmaniasis and ten healthy blood donors included
as negative controls. All sera samples were preserved in pH 7 .2
buffered glycerol ( v/v) and aliquots were stored at -2 0 ° C to avoid protein degradation2 8. The research protocol presented in this
manusc ript and the c onsent forms for sample c ollec tion and
utiliza tio n we r e a ppr o ve d b y th e Co m m itte e fo r Hum a n
Researc h – Federal University of Uberlandia and Hemominas.
Antigen pr epar ation. TESA were obtained essentially as de sc r ib e d3 0. B r ie fly, tr ypo m astigo te s o f the Y str ain we r e
maintained by serial passages in Swiss mic e. The blood c ollec ted
on the seventh day after inoc ulation was used to infec t HEP-2
c ell monolayers maintained in DMEM enric hed with 1 0 % fetal c alf serum ( FCS) . Following inc ubation for three days at 3 7 ° C in
5 % CO
2, the c ulture was gently rinsed three times with DMEM and the medium was c hanged to DMEM 1 % FCS. The c ulture
supernatants ( TESA) were c ollec ted on post-infec tion day 6 ( ~ 1 07 parasites.ml-1 ) then c entrifuged at 2 8 0 0 xg for 1 0 min at
4oC and filtered through a 0 .2 2 µm pore size c ellulose ac etate
membrane. Protease inhibitors cocktail ( 1 mM PMSF, 0 .5 mg.ml-1
aprotinin, and 0 .5 mg.ml-1 leupeptin) was added to TESA and aliquots were stored at -7 0oC. The spec ific c onc entration of TESA
in our preparations c ould not be determined by c onventional
assays due the c ontent of proteins present in the medium, suc h
as albumin.
One a nd two - dime nsio n ge l e le ctr o pho r e sis. The TESA were prepared fo r o ne-dimensio n SDS-PAGE ( 1 D) by
mixing 1 5 0 µl of c ulture supernatant with equal volume of
6 . 8 ] , 5 % 2 - m e r c a pto e th a n o l, 1 0 % glyc e r o l a n d 0 . 0 1 %
bromophenol blue) . The samples were boiled for 5 min at 1 0 0 ° C a nd lo a de d in a pr e pa r a tive 7 % po lya c r yla m ide ge l. Fo r
two-dimensional gel elec trophoresis ( 2 D) , the supernatants
were diluted ( 1 :3 ) in isoelec tric foc using sample buffer ( 8 M
ur e a , 4 % CHAPS, 1 8 m M DTT, 2 % Phar m alite 3 - 1 0 ) . The first-dimension isoelec tric foc using ( IEF) was c arried out using
Immobiline Dry Strip ( pH 4 -7 L, 7 c m long, Pharmac ia Biotec h)
in a Multiphor II elec trophoresis system ( Pharmac ia Biotec h,
New Jersey, USA) . The isoelec tric foc using was performed at 2 0 ° C with the following program: 5 0 0 V for 1 min, 5 0 0 - 3 ,5 0 0 V rising
gradient over 9 0 min, and 3 ,5 0 0 V for 4 h. After c ompletion of
the first dimension proc edure, the gel strips were inc ubated in
equilibration buffer at room temperature for 1 5 min ( 5 0 mM Tris-HCl [ pH 6 .8 ] , 6 M urea, 2 % [ w/v] SDS, 3 0 % glyc erol, 0 .0 1 %
bromophenol blue and 1 3 0 mM dithiothreitol ( DTT) . This was
fo llo wed by ano ther inc ubatio n in equilibr atio n buffer that
contained 1 5 0 mM iodoacetamide instead of DTT. The equilibrated gel strips were placed on top of 7 % SDS-polyac rylamide gels and
the elec trophoresis was c onduc ted at 6 0 V and 1 0 ° C.
Immuno blo tting. The proteins separated in the 1 D and 2 D PAGE gels were transferred onto polyvinylidene difluoride
membrane ( PVDF, millipore) . The membranes were bloc ked with 5 % de fatte d milk in PB S fo r 2 ho ur s, the n inc ub ate d
overnight at 4oC with patient sera diluted 1 :5 0 in PB S c ontaining
1 % defatted milk ( PB S-M1 % ) . After washing, the blots were
probed with goat anti-human IgG-peroxidase or anti-human IgM-peroxidase ( Sigma) in PB S-M1 % for 2 hours followed by
a c yc le of washes. Antigen-antibody reac tions were observed
a fte r d e te c ti o n o f p e r o x i d a s e a c ti vi ty b y H
2O2 a n d diaminobenzidine ( Sigma) .
RESULTS
In our one dimension immunoblotting assays with sera from
early ac ute patients, IgM antibodies c onsistently rec ognized TESA proteins in a range of 8 0 -2 0 0 kDa in a ladder-like pattern ( Figure
1 a) . TESA-blot for spec ific IgG in these patients showed reac tivity
to proteins below 1 0 0 kDa with a weaker overall intensity when
c ompared to IgM assays ( Figure 1 b) .
The patients grouped as late ac ute phase showed similarities on their TESA-blot pattern for spec ific IgM ( Figure 1 c ) and IgG
( Figure 1 d) . The 8 0 -2 0 0 kDa ladder-pattern was present in both
assays. Interestingly, most of the patients in this group presented
one band with approximately 1 6 0 kDa, inc luded in the ladder pattern, that showed inc reased intensity when c ompared to the
others at the same range of molec ular weight.
Serological analysis of the chronic patients by one dimension
TESA-blot showed an intense IgG reaction at 1 5 0-1 6 0 kDa in all
tested samples ( Figure 1f) . Some patient samples showed a few bands above this area and most of them recognized bands in the range of
8 0-1 2 0 kDa. IgM specific assays with samples from these patients
failed to recognize any TESA proteins as shown in Figure 1 e.
No antib o dy r e ac tivity was o b se r ve d in TESA-b lo t using
samples fro m healthy blo o d do no rs o r patients with c utaneo us
le ishmaniasis ( data no t sho wn) .
Se r um sample s fr o m e ar ly ac ute infe c tio n whe n analyze d b y 2 D TESA-b lo t sho we d a sc atte r e d IgM r e ac tio n r anging
fr o m pI 5 .8 to 6 .7 and 8 0 to 2 0 0 k Da. The ladde r-lik e patte r n
o b se r ve d in 1 D TESA-b lo t r e ve ale d a lar ge r numb e r o f spo ts in 2 D analysis. IgM r e ac tivity against the 1 5 0 -1 6 0 k Da pr o te in
was o b se r ve d with po o r de finitio n to war ds the alk aline side
a b c d e f
2 0 5
9 7
6 6
Gr o up I
Gr o up II
Gr o up III
1 6 0
o f the b lo tting, as sho wn b y the ar r o w he ads ( Figur e 2 a) . A
s im ila r I gM pr o file wa s o b s e r ve d in la te a c ute infe c tio n ( Figur e 2 b ) .
The IgG detec ted in the late ac ute infec tion also presented
a scattered reaction ranging from pI 5.8 to 6.7 and 70 to 180kDa.
However, IgG showed a slightly distinct pattern when compared to
IgM. In the late acute infection four defined spots, with pI 6.2-6.7, were recognized by IgG in the 150-160kDa region, as shown by the
arrow heads ( Figure 2c) . Serum samples from chronic patients, when
analyzed for specific IgG in 2D immunoblotting showed strong reaction
against the four spots described above. Among these dots, a dominant responsiveness was observed against the spot located at pI 6.2 - 6.4 in
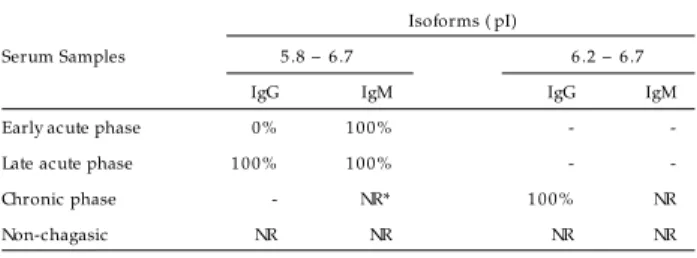
most of the chronic patient samples ( Figure 2d) . The frequency of
bands recognized in all sample sera were similar ( Table 1) .
showed that the four spots loc ated at the range of 1 5 0 -1 6 0 kDa
and pI 6 .2 -6 .7 were equally immuno stained by the 1 6 0 kDa spec ific antibody ( data not shown) .
DISCUSSION
In this study, we grouped the infected patients into early acute,
late acute and chronic phases of T. cruzi infection. This classification
serves for academic purposes and does not necessarily represent
the epidemiological scenario of the disease. Approximately 5 0 % of the chagasic population in endemic areas have the indeterminate
form of Chagas’ disease. The acute phase frequently goes unperceived
due to a lack of clinical symptoms, the majority of the infected
population is unaware of their health condition25.
The epidemiologic al features and pec uliarities of the disease in endemic areas represent a c hallenge for sc reening healthy
blood donors. In Uberlândia, MG, Brazil, a well c harac terized
endemic area, up to 4 % of the volunteers for blood donation are
rejec ted due to inc onc lusive c onventional serology for Chagas’ disease. This data enc ouraged us to searc h for more effic ient
diagnostic tools, espec ially in those c ases where c onventional
tec hniques c an not provide a definitive result.
Tryp a n o so m a c ru zi as we ll as o the r tr ypano so matids
synthesize and secrete a broad variety of molecules with biological
ac tivity during their lifec yc le. The fac t that T. cruzi is transmitted by an insec t vec tor and is able to invade several c ell types within
the host indic ates the requirement of a very versatile adaptive
system or systems. The spec ialized c oat of glyc o pr o te ins and
Ta ble 1 - Frequency fo r reco gnitio n in 2D gel o f 160 k Da pro tein, a cco rding to cha ga sic a nd no n-cha ga sic serum sa m ples.
Isoforms ( pI)
Serum Samples 5 .8 – 6 .7 6 .2 – 6 .7
IgG IgM IgG IgM
Early acute phase 0 % 1 0 0 % - -Late acute phase 1 0 0 % 1 0 0 % - -Chronic phase - NR* 1 0 0 % NR
Non-chagasic NR NR NR NR
* Non reactivity
As a c o mple me ntar y e xpe r ime nt, 2 D me mb r ane s we r e
probed with polyc lonal antibodies generated against a fragment
o f T. c ru zi 1 6 0 kDa rec ombinant protein ( kindly provided by
Dr. Eufrozina S. Umezawa, IMT-USP, São Paulo) . Our results
IEF
7 .0
PAGE
5 .8 7 .0 5 .8
1 6 0
1 6 0
IgM
IgG
a
b
d
c
glyc o lipis o n the pa r a site sur fa c e to ge the r with se c r e te d
pro teins all have a c ruc ial ro le in this enviro nmental transitio n and adaptatio n1 8.
Many of these sec reted molec ules belong to the T. c ru zi
transialidase ( TS) family7. During the early stage of infec tion
an intense shedding of TS molec ules ( also c alled shed ac ute
phase antige ns [ SAPA] ) , e lic its the pr o duc tio n o f spe c ific antibodies that func tion as markers of ac ute infec tion1. Rec ent
public ations have supported that transialidase family antigens
are assoc iated to c ellular invasion, due to their c apac ity to bind
c ell rec eptors and extrac ellular matrix proteins1 0 1 7. TS proteins have also been implic ated in immune respo nse mo dulatio n
leading to a down regulation of T c ells ac tivity1 2. Later in the
dise ase c o ur se , a c le ar de te c tio n o f antib o die s against the
1 6 0 kDa sec reted protein is c onsidered indic ative of c hronic Chagas’ disease3 2.
Following the criteria described above, the pattern of specific IgM
produced during the early acute infection suggests that these antibodies
are directed against TS repeats contained in SAPA complex15. During
the early acute phase, most samples contained IgG that weakly recognized antigens below 100kDa. Further investigations will focus
on the characterization of this antibody population.
In the late ac ute phase IgM and IgG r evealed str o ng b ands
of approximately 1 5 0 -1 6 0 kDa. A lower intensity of reac tion was
observed in other bands above and below the 1 5 0 -1 6 0 kDa range that pro bably represents antibo dies against TS repeats present
in SAPA mo le c ule s.
As e xpe c te d, no IgM was de te c te d in the c hr o nic infe c tio n
a n d th e 1 6 0 k Da pr o te in b e c a m e th e do m in a n t a n tige n
r e ve ale d b y the IgG immuno assay.
Two-dimensional analysis of ES antigens immunolabeled by human chagasic serum revealed several spots in the 8 0 -1 1 0 kDa
region with a wide range of isoelectric points ( pI between 5 .4 -6 .7 )22. I n the pr e se nt wo r k , the I gG pr o file displaye d do m inant
responsiveness against the dot located at 1 6 0 kDa and pI 6 .2 -6 .4 ,
which was the major immunological target in secreted antigens during the chronic infection ( Figure 2 d) . Five out of ten samples
from chronic patients remained reactive to TS repeats in various degrees. These data suggest that TS immune stimuli can remain active
through the course of the disease leading to a long-lasting specific antibody production.
The combined analysis of 1 D and 2 D immunoblots during the
early and late acute phase revealed a high level of complexity in
the T. cruzi excreted-secreted antigen recognition. The
ladder-like pattern, usually containing six bands, observed in 1 D blots
exposed approximately thirty immunoreactive spots when analyzed by 2 D blots. This data in addition to the lack of clear definition in
the spots’ shape indicate a considerable degree of modification in
this group of antigens. The uniformity and definition of these spots suggest the presence of a highly repetitive protein motif and may
also indicate that this group of antigens undergoes a considerable degree of post-translational modifications.
It is noteworthy that IgM and/or IgG antibodies rec ognized
four dots at 1 6 0 kDa through all phases of Chagas’ disease in all
infec ted patient samples, as observed in 2 D analysis ( Figure 2 ,
arrowheads) . These dots represent isoforms of 1 6 0 kDa protein, as
indicated by specific polyclonal antibody reaction. In contrast to sera from chronically infected patients the 1 6 0 kDa immunoreaction
was not clearly visible in 1 D immunoblot during the acute phase
( Figure 1 a) , this is probably due to a massive antibody response
against TS repeats that masked the 1 6 0 kDa band.
No variation in mass was observed between the four isoforms of the 1 6 0 kDa protein. However, eac h isoform has a partic ular
i s o e l e c tr i c fo c u s i n g p o i n t, wh i c h m i gh t b e r e l a te d to
modific ations, suc h as phosphorylation that alter the proteins’
elec tric c harge.
It is interesting to observe how the immune system shifts the response direc ted to sec reted antigens. The SAPA responsiveness
slowly dec reased during the progress of disease1 4, while 1 6 0 kDa
c omplex bec ame the major exc reted-sec reted immunogen.
In summary, we have shown that T. cruzi exc reted-sec reted
a n ti ge n s c o m p r i s e a c o m p l e x m i x tu r e o f a n ti ge n s , a s demonstrated by high-resolution 2 D immunoblotting. Our data,
although analyzing a small number of patients, c orrelated with
other studies indic ating that TESA is a highly effic ient tool for
Chagas’ disease diagnosis in either ac ute or c hronic stages.
ACKNOWLEDGMENTS
We ar e inde b te d to Dr. Eufr o zina S. Ume zawa fr o m the
Institute o f Tr o pic al Me dic ine o f São Paulo , fo r the he lp with antige n pr o duc tio n and standar dizatio n and to Dr. Samantha
Do nne lly fo r c r itic ally r e ading this manusc r ipt.
REFERENCES
1 . Affr anc hino J L, Ib ane z CF, Luq ue tti AO, Rassi A, Re ye s MB , Mac ina RA, Aslund L, Pe tte r sso n U, Fr asc h AC. Ide ntific atio n o f a Tryp a n o so m a c ru zi antige n that is she d dur ing the ac ute phase o f Chagas’ dise ase . Mo le c ular and B io c he mic al Par asito lo gy 3 4 : 2 2 1 - 2 2 8 , 1 9 8 9 .
2 . An d r e ws NW. T h e a c i d - a c ti ve h e m o l ys i n o f Tr yp a n o s o m a c r u z i. Expe r ime ntal Par asito lo gy 7 1 : 2 4 1 - 2 4 4 , 1 9 9 0 .
3 . Camar go ME, SG, CE, Silve ir a AC. [ Se r o lo gic al sur ve y o f the pr e vale nc e o f Chagas’ infe c tio n in B r azil, 1 9 7 5 /1 9 8 0 ] . Re vista do Instituto de Me dic ina Tr o pic al de São Paulo 2 6 : 1 9 2 - 2 0 4 , 1 9 8 4 .
4 . Ca m pe te lla O, Ma r tin e z J , Ca zzulo J J . A m a j o r c ys te in e pr o te in a s e is de ve lo pm e ntally r e gulate d in Tryp a n o so m a c ru zi. FEMS Mic r o b io lo gy Le tte r s 5 5 : 1 4 5 - 1 4 9 , 1 9 9 0 .
5 . Ch i l l e r T M, S a m u d i o MA, Zo u l e k G. I gG a n ti b o d y r e a c ti vi ty wi th Tryp a n o so m a c ru zi and Le i sh m a n i a antige ns in se r a o f patie nts with Cha ga s ’ dis e a s e a nd le is hm a nia s is . The Am e r ic a n J o ur na l o f Tr o pic a l Me dic ine and Hygie ne 4 3 : 6 5 0 - 6 5 6 , 1 9 9 0 .
6 . Co he n J E, Gur tle r RE. Mo de ling ho us e ho ld tr a ns m is s io n o f Am e r ic a n tr ypano so miasis. Sc ie nc e 2 9 3 : 6 9 4 - 6 9 8 , 2 0 0 1 .
7 . Co lli W. Tr a n s - s ia lida s e : a un iq ue e n zym e a c tivity dis c o ve r e d in th e pr o to zo an Tryp a n o so m a c ru zi. The FASEB Jo ur nal 7 : 1 2 5 7 -1 2 6 4 , 1 9 9 3 . 8 . Gazzine lli G, B r e ne r Z. Immuno lo gic al aspe c ts o f the mo r b idity o f human
Chagas’ dise ase . Re se ar c h in Immuno lo gy 1 4 2 : 1 6 7 -1 6 9 , 1 9 9 1 .
1 0 . Gio r dano R, Fo uts DL, Te war i D, Co lli W, Manning J E, Alve s MJ . Clo ning o f a s ur fa c e m e m b r a n e glyc o pr o te in s pe c ific fo r th e in fe c tive fo r m o f Tryp a n o so m a c ru zi having adhe sive pr o pe r tie s to laminin. The J o ur nal o f B io lo gic al Che mistr y 2 7 4 : 3 4 6 1 - 3 4 6 8 , 1 9 9 9 .
1 1 . Go m e s YM. P CR a n d s e r o - d i a gn o s i s o f c h r o n i c Ch a ga s ’ d i s e a s e . B io te c h n o lo gic a l a dva n c e s . Applie d B io c h e m is tr y a n d B io te c h n o lo gy 6 6 : 1 0 7 -1 1 9 , 1 9 9 7 .
1 2 . Go r e lik G, Cr e masc hi G, B o r da E, Ste r in- B o r da L. Tryp a n o so m a c ru zi a n ti ge n s d o wn - r e gu l a te T l ym p h o c yte p r o l i fe r a ti o n b y m u s c a r i n i c c h o lin e r gic r e c e p to r- de p e n de n t r e le a s e o f PGE2 . Ac ta Ph ys io lo gic a Phar mac o lo gic a at The r ape utic a Latino ame r ic ana 4 8 : 1 1 5 -1 2 3 , 1 9 9 8 .
1 3 . Gr e ig S, As h a ll F. Ele c tr o ph o r e tic de te c tio n o f Tr yp a n o s o m a c r u z i pe ptidase s. Mo le c ular and B io c he mic al Par asito lo gy 3 9 : 3 1 - 3 7 , 1 9 9 0 .
1 4 . J azin EE, Luq ue tti AO, Rassi A, Fr asc h AC. Shift o f e xc r e to r y- se c r e to r y im m un o ge n s o f Tryp a n o so m a c ru z i dur in g h um a n Ch a ga s ’ dis e a s e . Infe c tio n and Immunity 5 9 : 2 1 8 9 - 1 9 1 , 1 9 9 1 .
1 5 . Ke s p e r NJ , AK, S t o l f AM , Um e za wa E S . I m m u n o b l o t a n a l ys i s o f tr ypo mastigo te e xc r e te d-se c r e te d antige ns as a to o l fo r the c har ac te r izatio n o f Tryp a n o so m a c ru zi str ains and iso late s. The J o ur nal o f Par asito lo gy 8 6 : 8 6 2 -8 6 7 , 2 0 0 0 .
1 6 . Kr autz GM, Galvao LMC, Canç ado JR, Gue var a-Espino za A, Ouaissi A, Kr e ttli AU. Use o f a 2 4 - k ilo dalto n Tryp a n o so m a c ru zi r e c o mb inant pr o te in to mo nito r c ur e o f human Chagas’ dise ase . J o ur nal o f Clinic al Mic r o b io lo gy 3 3 : 2 0 8 6 -2 0 9 0
1 7 . Magde sian MH, Gio r dano R, Ulr ic h H, J uliano MA, J uliano L, Sc humac he r RI, Co lli W, Alve s MJ . Infe c tio n b y Tryp a n o so m a c ru zi. Ide ntific atio n o f a pa r a s ite liga n d a n d its h o s t c e ll r e c e pto r. Th e J o ur n a l o f B io lo gic a l Che mistr y 2 7 6 : 1 9 3 8 2 - 1 9 3 8 9 , 2 0 0 1 .
1 8 . Mc Co nville MJ , Mullin KA, Ilgo utz SC, Te asdale RD. Se c r e to r y pathway o f tr ypano so matid par asite s. Mic r o b io lo gy and Mo le c ular B io lo gy Re vie ws 6 6 : 1 2 2 -1 5 4 , 2 0 0 2 .
1 9 . Medr ano NM, Luz MR, Cabello PH, Tapia GT, Van LF, Ar auj o JT. Ac ute Chagas’ dise ase : plasma le ve ls o f alpha- 2 - mac r o glo b ulin and C- r e ac tive pr o te in in c hildr e n unde r 1 3 ye ar s in a high e nde mic ar e a o f B o livia. J o ur nal o f Tr o pic al Pe diatr ic s 4 2 : 6 8 - 7 4 , 1 9 9 6 .
2 0 . Mo nc ayo A. Pr o gr e ss to war ds the e liminatio n o f tr ansmissio n o f Chagas dise ase in Latin Ame r ic a. Wo r ld He alth Statistic s Quar te r ly 5 0 : 1 9 5 - 1 9 8 , 1 9 9 7 .
2 1 . Nak azawa M, Ro sa DS, Pe r e ir a VR, Mo ur a MO, Fur tado VC, So uza WV, B a r r o s MN, Ab a th FG, Go m e s YM. E x c r e to r y- s e c r e to r y a n ti ge n s o f Tryp a n o so m a c ru zi ar e po te ntially use ful fo r se r o diagno sis o f c hr o nic Chagas’ dise ase . Clinic al and Diagno stic Lab o r ato r y Immuno lo gy 8 : 1 0 2 4 -1 0 2 7 , 2 0 0 -1 .
2 2 . Ouaissi MA, Taib i A, Co r ne tte J , Ve lge P, Mar ty B , Lo ye ns M, Este va M, Rizvi FS, Capr o n A. Char ac te r izatio n o f maj o r sur fac e and e xc r e to r y-se c r e to r y immuno ge ns o f Tryp a n o so m a c ru zi tr ypo mastigo te s and ide ntific atio n o f po te ntial pr o te c tive antige n. Par asito lo gy 1 0 0 : 1 1 5 - 1 2 4 , 1 9 9 0 .
2 3 . Pe r e i r a ME. A de ve l o p m e n ta l l y r e gu l a te d n e u r a m i n i da s e a c ti vi ty i n Tryp a n o so m a c ru zi. Sc ie nc e 2 1 9 : 1 4 4 4 -1 4 4 6 , 1 9 8 3 .
2 4 . Ple ss M, J ur ane k D, Ko zar sk y P, Ste ur e r F, Tapia G, B e r m ude z H. The e pide mio lo gy o f Chagas’ dise ase in a hype r e nde mic ar e a o f Co c hab amb a, B o livia: a c linic al study inc luding e le c tr o c ar dio gr aphy, se r o r e ac tivity to Tr yp a n o s o m a c r u z i, x e n o d i a g n o s i s , a n d d o m i c i l i a r y tr i a to m i n e distr ib utio n. Ame r ic an J o ur nal o f Tr o pic al Me dic ine and Hygie ne 4 7 : 5 3 9 -5 4 6 , 1 9 9 2 .
2 5 . Pr ata A. Clinic al and e pide mio lo gic al aspe c ts o f Chagas dise ase . The Lanc e t Infe c tio us Dise ase s 1 : 9 2 - 1 0 0 , 2 0 0 1 .
2 6 . Sc hmunis GA, Zic k e r F, Pinhe ir o F, B r andling B D. Risk fo r tr ansfusio n-tr ansmitte d infe c tio us dise ase s in Ce nn-tr al and So uth Ame r ic a. Eme r ging Infe c tio us Dise ase s 4 : 5 - 1 1 , 1 9 9 8 .
2 7 . Segura EL, Cura EN, Estani SA, Andrade J, Lansetti JC, RA, Campanini A, Blanc o SB, Gurtler RE, Alvarez M. Long-term effec ts of a nationwide c ontrol program on the seropositivity for Trypa no so m a cruzi infection in young men from Argentina. Americ an Journal of Tropic al Medic ine and Hygiene 6 2 :3 5 3 -3 6 2 , 2 0 0 0 .
2 8 . Ume zawa ES, B asto s SF, Camar go ME, Yamauc hi LM, Santo s MR, Go nzale z A, Zingale s B , Le vin MJ , So usa O, Range l AR, Silve ir a J F. Evaluatio n o f r e c o mb inant antige ns fo r se r o diagno sis o f Chagas’ dise ase in So uth and Ce ntr al Ame r ic a. J o ur nal o f Clinic al Mic r o b io lo gy 3 7 : 1 5 5 4 - 1 5 6 0 , 1 9 9 9 .
2 9 . Ume zawa ES, B asto s SF, Co ur a JR, Le vin MJ, Go nzale z A, Range l AR, Zingale s B , Luq ue tti AO, Silve ir a J F. An impr o ve d se r o diagno stic te st fo r Chagas’ dise ase e mplo ying a mixtur e o f Tryp a n o so m a c ru zi r e c o mb inant antige ns. Tr ansfusio n 4 3 : 9 1 - 9 7 , 2 0 0 3 .
3 0 . Ume zawa ES, Nasc ime nto MS, Ke spe r NJ, Co ur a JR, B o r ge s PJ, Junq ue ir a AC, Camar go ME. Immuno b lo t assay using e xc r e te d-se c r e te d antige ns o f Tryp a n o so m a c ru zi in se r o diagno sis o f c o nge nital, ac ute , and c hr o nic Chagas’ dise ase . J o ur nal o f Clinic al Mic r o b io lo gy 3 4 : 2 1 4 3 - 2 1 4 7 , 1 9 9 6 .
3 1 . Ume zawa ES, Nasc ime nto MS, Sto lf AM. Enzyme - link e d immuno so r b e nt assay with Tryp a n o so m a c ru zi e xc r e te d-se c r e te d antige ns ( TESA-ELISA) fo r s e r o dia gn o s is o f a c ute a n d c h r o n ic Ch a ga s ’ dis e a s e . Dia gn o s tic Mic r o b io lo gy and Infe c tio us Dise ase 3 9 : 1 6 9 - 1 7 6 , 2 0 0 1 .
3 2 . Umezawa ES, Shikanai YM, Stolf AM. Changes in isotype c omposition and antigen rec o gnitio n o f anti-Trypa n o so m a c ru zi antibo dies fro m ac ute to c hro nic Chagas disease. Journal of Clinic al Laboratory Analysis 1 0 :4 0 7 -4 1 3 , 1 9 9 6 .