“W I THOUT MONEY YOU’RE NOTHI NG”: POVERTY AND HEALTH
I N MEXI CO FROM W OMEN’S PERSPECTI VE
I sabel Her n án dez Tezoqu ipa1 Luz Ar enas Monr eal1 Sandr a Tr ev iño- Siller1
Hernández I T, Arenas LM, Treviño- Siller S. “ Wit hout m oney you’re not hing” : pov er t y and healt h in Mexico from w om en’s per spect iv e. Rev Lat ino- am Enfer m agem 2 0 0 5 set em br o- out ubr o; 1 3 ( 5 ) : 6 2 6 - 3 3 .
The obj ect ive of t his qualit at ive st udy was t o get t o know poor Mexican wom en’s experience of povert y in relat ion t o healt h care. Fort y- nine int erviews were carried out wit h poor adult wom en in Mexico ( bet ween 35 and 65 years old) . Three cent ral elem ent s were det ect ed in relat ion t o t he wom en’s experience of povert y and healt h care: t heir socio- econom ic dependence on t heir fam ily; t he not ion of social belonging in t heir experience w it h h ealt h car e r igh t s, r ef lect ed in t h e idea an d accept an ce t h at , du e t o t h eir pov er t y , t h ey can on ly be at t en ded at ph ilan t h r opic in st it u t ion s; an d t h e ex ist en ce of su r v iv al m ech an ism s w h en f acin g an illn ess. I n recovering t he experience of poor wom en in relat ion t o t heir healt h care, we ident ified t hat t here is a clear idea t hat , if wom en had had econom ic resources, t heir healt h problem would have been solved different ly. They are also conv inced t hat , due t o being poor , t hey hav e t o cont ent t hem selv es w it h bad- qualit y m edical car e. This conform it y finally m akes t hem resign t o t he fact of eit her loosing a part of t heir own body, or even j ust wait ing for deat h.
DESCRI PTORS: w om en; healt h; pov er t y ; sur v iv al
“SI N DI NERO NO ERES NADA”: POBREZA Y SALUD EN MÉXI CO
DESDE LA PERSPECTI VA DE LAS MUJERES
El obj et ivo del present e t rabaj o fue conocer la vivencia de la pobreza en relación al cuidado y at ención de la salud en el caso de m uj eres pobres m exicanas. Se desarrolló una invest igación cualit at iva que se llevó a cabo en México. Se realizaron y analizaron cuarent a ent revist as que se aplicaron a m uj eres ent re 35 y 65 años d e ed ad . Se d et ect ar on t r es elem en t os cen t r ales con r elación a la v iv en cia d e la p ob r eza y el cu id ad o y at ención de la salud: la dependencia socioeconóm ica hacia su fam ilia; la noción de una per t enencia social en la vivencia de los derechos de at ención a la salud que se reflej a en la consideración y acept ación de que a ellas d eb id o a su con d ición d e p ob r eza sólo les cor r esp on d e ser at en d id as en las in st it u cion es d e b en ef icen cia pública; y la ex ist encia de m ecanism os de super v iv encia fr ent e a un ev ent o de enfer m edad. Al r ecuper ar la ex per iencia de las m uj er es pobr es en su cuidado de salud se ident ificó lo siguient e: ex ist e una clar a idea de que si se hubier a cont ado con r ecur sos económ icos suficient es su pr oblem a de salud se hubier a r esuelt o de ot ra m anera; t am bién se t iene la convicción de que por ser pobres deben conform arse con una m ala at ención m édica y, est a confor m idad pr ovoca que, finalm ent e, se r esignen al hecho de, o bien per der una par t e de su cuer po, o, inclusiv e, a esper ar la m uer t e.
DESCRI PTORES: m u j er es; salu d; pobr eza; su per v iv en cia
“SEM DI N HEI RO VOCÊ N ÂO É N ADA”: POBREZA E SAÚDE N O MÉXI CO
A PARTI R DA PERSPECTI VA DAS MULHERES
O obj et iv o do pr esent e t r abalho foi conhecer a v iv ência da pobr eza em r elação à assist ência à saúde no caso de m ulher es pobr es m ex icanas. Desenv olv eu- se um a pesquisa qualit at iv a no Méx ico, r ealizando 4 0 ent r ev ist as com m ulher es ent r e 35 e 65 anos de idade. Det ect ar am - se t r ês elem ent os cent r ais a r espeit o da v iv ência da pobr eza e da assist ência à saúde: a dependência socioeconôm ica par a com a fam ília; a noção de um a pert ença social na vivência dos direit os de at enção à saúde, que se reflet e na consideração e aceit ação de qu e, dev ido a su a con dição, som en t e podem ser at en didas em in st it u ições f ilan t r ópicas; e a ex ist ên cia de m ecan ism os d e sob r ev iv ên cia d ian t e d e u m ev en t o d e d oen ça. Ao r ecu p er ar a ex p er iên cia d as m u lh er es p ob r es com r elação à assist ên cia à saú d e, id en t if icou - se q u e ex ist e u m a id éia clar a d e q u e, se t iv essem cont ado com recursos econôm icos suficient es, seus problem as de saúde t eriam sido resolvidos de out ra m aneira. Tam bém t êm a conv icção de que, por ser em pobr es, dev em se confor m ar com um a at enção m édica de m á qu alidade, e est a con for m idade fin alm en t e pr ov oca su a r esign ação com o fat o de per der em u m a par t e dos seus cor pos, ou ainda m ais esper ar em a chegada da m or t e.
DESCRI TORES: m u lh er , saú de, pobr eza, sobr ev iv ên cia
1
I NTRODUCTI ON
W
om en const it ut e a lit t le m ore t han half t he world’s populat ion. However, in spit e of effort s carriedou t in past decades, in gen er al, w om en liv e u n der
condit ions of inequalit y and w it h few er oppor t unit ies.
Th er ef or e, pov er t y * con t in u es t o be m or e acu t e in
t h e c a s e o f w o m e n , w h o r e p r e s e n t t h e g r e a t e r
percent age of t he world’s populat ion living in absolut e
povert y. Som e world- wide dat a show t hat 70% of t he
people t hat live in condit ions of ext r em e pover t y ar e
w om en and t hat 2/ 3 of t hem ar e illit er at e ( 1). I n t he
r u r al ar eas, m or e t h an 5 5 0 m illion w om en liv e in
p o v e r t y ( m o r e t h a n 5 0 % o f t h e w o r l d ’ s r u r a l
populat ion) . Tw o- t hir ds of t he 1 0 0 0 m illion illit erat e
adult s in t he world are wom en and a t hird of t he hom es
ar e headed by a w om an. As far as em ploy m ent , all
r egion s of t h e w or ld dem on st r at e a gr eat er r at e of
unem ploym ent am ong t he w om en t han t he m en and
in Lat in Am er ica and t he Car ibbean, bet w een 7 and
11% of t he t ot al beneficiaries of credit are wom en ( 2).
Many w om en aut hor s point out t hat pov er t y
and inequalit y acquir e differ ent m odalit ies w hen t hey
a r e a n a l y z e d f r o m t h e p e r s p e c t i v e o f g e n d e r.
Ther efor e, t he populat ion t hat liv es in im pov er ished
condit ions is t he principal vict im of chronic illness and
in fect ion s an d h av e t h e low est lev els of h ealt h an d
t he great est indices of healt hy life years lost( 3- 4). But ,
w hen one analyzes t he pr oblem accor ding t o gender,
it is observed t hat fem inine povert y is a far reaching
phenom ena t hat affect s m en as m uch as wom en and
t hat has r eper cussions for t he w hole fam ily in t er m s
of healt h car e and ser v ices.
I n t h e specif ic case of Mex ico, r ecen t dat a
indicat e t hat t here are a t ot al of 40.7 m illion poor and
2 2 m illion ex t r em ely p oor p eop le( 5 ). Th e d at a also
in dicat e t h at as of 1 9 9 2 , t h e r u r al poor h av e been
in cr easin g f r om 2 . 7 t o 3 . 4 t im es m or e t h an w h en
com par ed w it h t he ur ban ar eas in 2000. I n addit ion,
t he indicat ors associat ed wit h povert y and m arginalit y
su g g est m or e p r ecar iou s con d it ion s in t h e sp ecif ic
case of wom en; in relat ion t o t he illit erat e populat ion
15 years of age and older, it is observed t hat 7.4 %
ar e m en v s. 11. 3 w om en; in r elat ion t o econom ics:
70. 3 % of m en v s. 29. 9 % of w om en par t icipat e in
som e for m of incom e gener at ion ( 6).
Various st udies( 7- 8) wit h a fem inist perspect ive
h a v e f o cu se d o n g i v i n g v i si b i l i t y t o t h e so ci a l l y
disadv ant ageous condit ions t hat char act er ize a w ide
num ber of sit uat ions which wom en have experienced,
am on g ot h er s, t h ose r elat ed t o p ov er t y, in eq u alit y
a n d h e a l t h . A s a r e s u l t , g e n d e r i n e q u i t i e s a r e
m an if est ed in div er se aspect s: t h e div ision of w or k
b e t w e e n t h e se x e s, t h e l a ck o f o p p o r t u n i t i e s f o r
educat ion and em ploy m ent , t he pr ev alence of low er
levels of well- being and healt h, t he lim it ed part icipat ion
socially and in fam ily decisions, w hich lim it s personal
au t on om y. Th ese in eq u alit ies g en er at e a ser ies of
disadvant ages for wom en t hat are int erconnect ed wit h
ot her social asym m et ries, et hnic or int ergenerat ional,
t h at ex pose t h em an d m ak e t h em m or e v u ln er able
t o sit uat ions charact erized by lim it at ions and povert y.
Fem in ism an d socio- st r u ct u r al an aly sis ar e
fundam ent al t ools t o be able t o underst and t he healt h
of “ poor w om en”. The pr em ise of t hese per spect ives
i s t h a t t h e u n d e r l y i n g s t r u c t u r e i n s o c i e t y h a s
p r o d u ced a sy st em o f st r at i f i cat i o n t h at p r esen t s
en or m ou s in equ alit ies in w om en ’s lif e opt ion s. Th is
inequalit y has effect s on t he healt h of poor wom en as
f ar as t h eir b eh av ior, m or b id it y an d m or t alit y an d
a cce ss t o h e a l t h ca r e se r v i ce s. Fo r a n a d e q u a t e
concept of healt h in poor w om en, it is necessar y t o
go deeper in t he analysis of t he healt h sit uat ion, int o
t he social cont ex t w it hin w hich it occur s, t ak ing int o
accou n t t h e posit ion of poor w om en in societ y, t h e
com m unit ies in which t hey live and t he st ressful event s
in t heir lives. The socio- st ruct ural analysis em phasizes
t h at , cu r r en t ly, as a con seq u en ce of an econ om ic
m odel t hat widens social differences, one can observe
what is called t he polarizat ion of wealt h: few rich and
m any poor( 9) .This sit uat ion, specifically in t he case of
w o m en , h as b een r ep o r t ed m ai n l y i n q u an t i t at i v e
st udies( 1 0 ), w it h ou t ex plor in g t h e daily dim en sion of
h o w w o m en l i v e a n d ex p er i en ce p o v er t y a n d t h e
healt h- illness condit ion.
Therefore, t he obj ect ive of t his st udy w as t o
b e c o m e f a m i l i a r w i t h p o o r M e x i c a n w o m e n ’ s
ex per ience of pov er t y in r elat ion t o healt h car e.
METHODOLOGY
We used a qualit at ive design t o ex plor e and
descr ibe t he Mex ican w om en’s ex per ience of pov er t y
i n r e l a t i o n t o h e a l t h ca r e . Qu a l i t a t i v e d a t a w e r e
obt ained using t aped sem i st r uct ur ed int er v iew s. We
a n a l y zed t h e q u a l i t a t i v e d a t a i n Sp a n i sh t h r o u g h
gr ounded t heor y pr ocedur es and t echniques( 11- 13).
Par t icipan t s
The unit of analysis of t his st udy w er e adult
wom en ( ranging in age from 25 t o 65 years old) users
an d n on - u ser s of h ealt h ser v ices. Wer e 4 9 w om en
int er v iew ed, fiv e belonged t o t he 25 t o 29 y ear old
age group, four t o t he 30- 34 year old age group, 15
t o t he 35 t o 49 year old age group, nine t o t he 40 t o
44 year old group, five t o t he 45 t o 49 year old group,
four t o t he 50 t o 54 year old group, four t o t he 55 t o
59 year old group and t hree were older t han 60 years
of age. Wit h respect t o place of residence: 15 wom en
w er e f r om t h e sou t h er n r eg ion , 1 1 w er e f r om t h e
n or t h er n r eg ion , six w er e f r om t h e cen t r al r eg ion ,
and eight were from t he region considered t o be highly
m ar g in alized .
Pr o ced u r es
Healt h ser v ices in Mex ico ar e or gan ized as
follow s: t he social secur it y ones, w hich include t hat
p o p u l a t i o n w h o h a s a f o r m a l j o b a n d t h e o p e n
populat ion ser v ices w hich at t end t he populat ion w ho
doesn’t have a form al j ob and has no social securit y.
Th i s l a st ca se w a s t h e t a r g et p o p u l a t i o n f o r t h i s
research. An analysis was m ade of t he dat abase t hat
corresponds t o t he Nat ional Healt h Survey ( “ Encuest a
Nacional de Salud” or “ ENSA I I ” ) in Mex ico* , w hich
was carried out in 1994.A fundam ent al com ponent of
t h e s u r v e y w a s t h e i n c l u s i o n o f a q u a l i t a t i v e
com p on en t .
Th e t ot al f ed er al st at es w er e g r ou p ed in t o
five st udy regions: Met ropolit an Zone, Cent ral, Nort h,
S o u t h e a s t a n d t h e Gu l f . I n t o t a l , 1 9 2 i n - d e p t h
in t er v iew s w er e car r ied ou t w it h f iv e g r ou p s f r om
w it hin t he populat ion: a) sick per sons w ho r eceiv ed
m ed ical car e, b ) sick p er son s w h o d id n ot r eceiv e
m e d i ca l ca r e , c) p e r so n s w h o w e r e n o t si ck a n d
received m edical care ( e.g. vaccines, fam ily planning,
b ir t h con t r ol, ear ly can cer d et ect ion an d scr een in g
e t c. ) a n d , d ) ch r o n i ca l l y si ck w o m e n . Of a l l t h e
in t er v iew s car r ied ou t ( 1 9 2 ) , on ly 4 9 cor r espon ded
t o wom en bet ween t he ages of 25 and 65.
Th e i n t e r v i e w s c o n t a i n e d t h e f o l l o w i n g
t h e m e s: 1 ) No t i o n a n d p e r ce p t i o n o f h e a l t h a n d
illness, 2) Sick wom en’s career 3) Percept ion of healt h
services and t he econom y of healt h, 4) Hospit alizat ion.
Ea c h o n e o f t h e t h e m e s i n v e s t i g a t e d s p e c i f i c
charact erist ics of t hree t ypes of users, a sick w om an
w h o d i d or d i d n ot r ecei v e car e, n on - si ck u ser, a
ch r on ically sick w om an .
Dat a an aly sis
Th e p r o p o sal w as ap p r o v ed b y t h e Et h i cs
Com m it t ee of t he Nat ional I nst it ut e of Public Healt h.
Th e in t er v iew s w er e t aped w it h t h e appr ov al of all
t hose int er view ed. They w er e t r anscr ibed, coded and
p r ocessed u sin g t h e p r og r am Et h n og r ap h 4 . 0 . Th e
infor m at ion w as or ganized using t he follow ing codes:
Ca r e t o o t h e r s , Pr i v a t e a r e n a , Pu b l i c a r e n a ,
Socioeconom ic fact or s, Gender, Suppor t Net w or k s as
t o al l ow f or t h e i d en t i f i cat i on of ot h er cod es t h at
em erged during t he analysis. The em erging code was
“ f e e l i n g p o o r ”, w h i ch w a s d e f i n e d a s t h e f a ct o f
considering t hat in due of t he social st at us t he wom en
only have right t o one kind of healt h care: public, not
enough and of bad qualit y.
Scien t if ic adequ acy
We u sed sev er al st r at egies in t h e st u dy t o
ad d r ess q u alit at iv e r ig or : cr ed ib ilit y, d ep en d ab ilit y,
confir m abilit y, t ransfer abilit y( 14). Specifically, We used
t he follow ing st rat egies: ( a) verbat im t ranscript ion of
audiot ape recordings; ( b) det ailed observat ional not es
in clu ded in t h e dat a an aly sis; ( c) docu m en t at ion of
personal feelings and em ot ions and react ions included
in t h e dat a an aly sis an d codin g; ( d) docu m en t at ion
on aut hor s ow n behav ior and ex per iences in r elat ion
t o t h e i n f o r m an t ’s ex p er i en ces ( e) f eed b ack f r o m
wom en of a shared experience aft er t he result s were
pr esent ed ( f ) our long- t er m com m it m ent t o w or k ing
wit h wom en’s groups in im poverished areas of Mexico
a n d t o t h e f i e l d o f g e n d e r a w a r e p e r s o n a l
em p ow er m en t .
RESULTS
Based o n t h e an al y si s o f t h e r ead i n g an d
codifying of t he int erviews, t hree elem ent s were clearly
ident ified in t he w ay in w hich t he w om en w ho w er e
i n t er v i ew ed ex p er i en ced h eal t h i n p o v er t y : so ci al
d e p e n d e n ce o n t h e i r f a m i l y, t h e n o t i o n o f so ci a l
b elon g in g - f r om p ov er t y - in t h eir ex p er ien ce w it h
healt h car e r ight s, and t he dev elopm ent of differ ent
st r at egies t o sur v iv e illness.
Social d ep en d en ce
A form of social inequalit y for wom en of t his
age an d especially w om en ov er 5 0 y ear s of age is
t he econom ic dependence on t heir spouses and t heir
children. Nine out of t he 14 wom en in t his st udy live
in t his sit uat ion, six of whom live in a region considered
t o be highly m ar ginalized. I f t he spouses or childr en
ar e u n em ploy ed, t h e f am ily in com e dim in ish es, t h e
q u alit y of lif e f or t h e w h ole f am ily is af f ect ed an d
t h er ef or e, t h ey h av e pr oblem s r elat ed t o access t o
h e a l t h c a r e o r h e a l i n g . A w o m a n , s h a r e s h e r
ex p er i en ce:
Now unfort unat ely, m y husband, when he can work, he
works, and when he can’t , he doesn’t ... because since we are old
now, see how t hey don’t give work t o old people as t hey like no?
when t here is w ork, ok, but w hen t here isn’t , no. That is w hy I
haven’t gone t o t he doct or now . [ Because you didn’t have { t he
m eans} ?] Yes, because I haven’t had { t he m eans} ( I nt erview
215) .
Th e pov er t y sit u at ion is also m an if est ed in
t he dependence on one’s children for access t o healt h
car e, t he follow ing t est im ony is an ex am ple:
No, now m y children are giving m e m oney, t he son t hat
works, I t ell you, he is giving m e a lit t le bit , he is helping m e,
when t hey pay him he gives m e 200 [ pesos] every 15 days, t hat
is what I use for m edicines. Where can I t ake [ m oney] , because
what if I acquire debt , where will I get t he m oney so t hat I can
replace t hat m oney, you see, now a good am ount of m oney is
needed. ( I nt erview 235) .
Dependency on t heir children for healt h care
becom es a cent ral w orry in t he life of t he w om en:
Well, t hat is what I oft en t hink, t he day t hat I am very
ill and don’t have insurance, where will I go? Well, I do t hink t hat
because now t he only son t hat support s us is t he 20 year old
son, he is t he only one t hat helps us and t his I t ell you is t o t hink
about , but , well God is great and God will know... ( I nt erview
164) .
The cent ral point is how t o resolve t he illness
ev ent –an ur gency or unex pect ed ev ent - , and how
t o st rengt hen healt h. These wom en don’t like t he fact
t hat t hey depend on t heir spouses or childr en. They
don’t want t o be an econom ic burden t o ot hers, t hey
don’t feel t hey hav e t he r ight t o ask for m oney for
t heir healt h car e consult s needs.
N o t i o n o f s o c i a l b e l o n g i n g - f r o m p o v e r t y - a n d
ex per ience of healt h car e r ight s
Anot her one of t he fact ors which was clearly
id en t if ied in t h e in t er v iew s is t h e con cep t t h at t h e
wom en give t o healt h care in relat ion t o povert y. The
w om en consider t hat t her e is a specific healt h car e
t hat corresponds t o t he poor; t hese m ay be t he social
s e c u r i t y s e r v i c e s , t h e s e r v i c e s f o r t h e g e n e r a l
p op u lat ion w h ich t h e Secr et ar y of Healt h p r ov id e,
Fam ily Healt h Services ( Cent ros de Desarrollo I nt egral
d e l a Fam i l i a, o r “ D I F” ) an d t h e Red Cr o ss. Po o r
w om en com e t o t hink t hat giv en t heir im pov er ished
condit ions, only cert ain t ypes of services are for t hem .
Th ey in t er n alize belon gin g t o a cer t ain social class,
a s a c o n s e q u e n c e , t h e y a u t o m a t i c a l l y p l a c e
t hem selv es in cer t ain ar enas. This is ex pr essed by a
w om an, in t he follow ing w ay:
Well, you can see t hat when one is poor, one always
goes t o t he Red Cross because it is t he m ain provider because
t hat is what one as a poor person does ( I nt erview 234) .
This per cept ion t hat t her e is a specific place
for t hem because t hey are poor is accom panied by a
series of inconveniences and barriers in t he care and
at t ent ion t o t heir healt h: not having m oney t o pay for
a specialist or t o sim ply see a general physician; not
t o be able t o have a sur gical int er vent ion; not t o be
able t o m aint ain a special diet ; not t o be able t o have
m oney t o buy m edicine or special t r eat m ent ; not t o
be able t o carry out cont inuous t reat m ent , not t o be
able t o be at t ended t o im m ediat ely. This sit uat ion is
ex pr essed in t he follow ing t est im ony :
No, well I say, about one’s econom ic st at e, well if [ you
go] t o a healt h cent er, because if you had, well you would go t o a
privat e one and quick, t hey would at t end t o you and everyt hing.
Never, for t hat reason he is as he is, because I know for sure if I
was being t reat ed by a doct or or a specialist t hey would have
m oney, because w it hout m oney you’re not hing ( I nt erview 248) .
Pu r ch asin g pow er is cen t r al f or t h e w om en
so t h at t h ey can access h ealt h ser v ices t h at t h ey
consider t o be good qualit y.
Fr om t h e social per spect iv e, social ser v ices
ar e con sider ed t o ex ist for people of few r esou r ces
and t o be t he w ay t o r esolv e t heir healt h pr oblem s.
The pr oblem is t hat it is not sufficient t o offer car e
b ecau se t h e p eop le d o n ot h av e r esou r ces t o b u y
m edicine or bet t er t o pay for t heir t ransport at ion, and
m uch less for t heir diet s or special care, t he following
ex per ien ce con fir m s t h is:
Your illness is in a crit ical phase, such t hat you can no
longer support yourself on your own feet and t end t o fall, and for
t hat reason you approached t he healt h cent er and t hey have been
seeing you but at t im es, for econom ic reasons, you don’t go, or
you don’t buy t he m edicine, it is t hen when you resort t o oint m ent s
or unguent s ( I nt erview 41) .
Qu alit y of car e is an ot h er asp ect w h ich is
linked t o t he social not ion of what corresponds t o being
poor. Th e w om en k n ow t h at a w or ld of h ealt h car e
ex ist s w hich does not belong t o t hem , t his sense of
bein g dist an t an d n ot belon gin g is t ak en t o absu r d
lev els:
Well, I didn’t t end t o m yself for t hat reason, for lack of
m oney, because if I had had m oney, of course I would have been
at t ended t o by a privat e physician and as m y sist er did, m y
sist er, well everyt hing was t hrough a privat e physician, unt il I
t hink t hat best t hat I didn’t have t he need t o have m y breast
rem oved, I say no and t hey rem oved it , but t hat ’s t he way it is,
so it is, not even crying is good. I f I had had a way t o pay for a
specialist , or t o pay for som e st udies, if I had done it …, because
t o lose a piece of your body hurt s a lot , we suppose t hat t here is
no pain once you are calm ing down, but t o rem ain like t hat , it
em barrasses m e t o walk around like t hat , I can’t even put on a bra
( I nt erview 23) .
Am ong t he poor, t he sensat ion of nor m alit y
w it h r espect t o healt h car e r ight s w hich cor r esponds
t o t hem because t hey belong t o a cert ain social class,
f o r m p a r t o f a n i d e o l o g y o f s u b m i s s i v e / p a s s i v e
accept ance. The wom en also observe t hat t here is an
inaccessible w or ld for t heir car e because t hey k now
t hat alt er nat ive m edicines exist t hat could help t hem
find relief from t heir healt h ailm ent s but t hey cannot
a cce ss t h e m b e ca u se t h e y a r e n o t e co n o m i ca l l y
solv en t .
These experiences of inaccessibilit y t o healt h
care, can reach such a level, t hat t hey are lived wit h
a cert ain sense of conform it y, while wait ing for deat h.
Th e f ollow in g t est im on y is an ex am p le of k n ow in g
t hat one day deat h w ill finally com e because w om en
can’t r eceiv e car e for t heir illness:
Look, when I am walking around wit h m y abdom en
swollen, at t im es I t hink t o m yself, oh m y God! , if at any m om ent
I ’m going t o bust because an infect ion in m y abdom en, an ulcer,
t he bile, t he gall bladder, I t ell you t hat I am going t o die, well
w hat do I ? ( I nt erview 227) .
The w om en liv e in ex t r em e sit uat ions w hich
ar e asso ci at ed w i t h access t o m ed i cal car e, t h ei r
discou r se con st an t ly r ef er s t o t h e lack of econ om ic
r esour ces t o be able t o t ak e car e of t hem selv es, or
t heir fam ily, t he follow ing t est im ony confir m s t his:
Yes, because t here isn’t any m oney; we have t he case
of m y brot her. [ What does he have ?] We don’t know, because
t here isn’t any m oney. We haven’t been able t o t ake him t o a
doct or. We t reat him wit h what we can, not hing m ore. I t m ust be
about a m ont h and a half since he arrived, but now not hing else,
he j ust lays t here, like he doesn’t have any defenses. [ Did t hey
inj ect him wit h vit am ins ?] The t rut h is t hat som et im es we don’t
have m oney for t he appoint m ent ( I nt erview 19) .
Poor w om en ent r ust t he final decision about
t heir healt h in t heir religious fait h and divine help, as
a last r esor t . Sev er al t est im on ies associat e pov er t y
a n d Go d ’ s h e l p a s t h e i r r e co u r se ; t h e f o l l o w i n g
succinct ly expresses t he relat ionship bet ween povert y,
w ait ing for deat h and divine help:
That is why, it is bet t er t hat we get sm art , because
wit hout t he help of t he Social Securit y or anyt hing, and wit hout
m oney, well, if we get sick, t here, we are left only wit h t he help of
God. I f t he person get s up, good; if not , well, t hat ’s t he way it is
( I nt erview 74) .
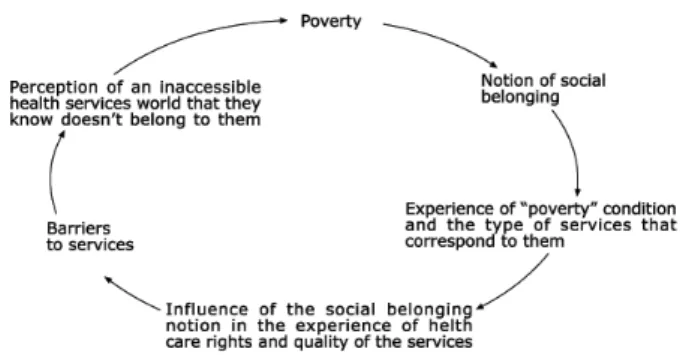
Life or deat h in povert y becom e elem ent s of
daily life. The following schem e sum m arizes t hat which
has been ex plained in t he pr ev ious par agr aphs.
Experience of “poverty”” condition and the type of services that correspond to them
Barriers To services Perception of an inaccessible health services world that they know doesn’t belong to them
Notion of social belonging
Influence of the social belonging notion in the experience of health care rights and quality of the services
Poverty
Figu r e 1 – Per cept ion of adu lt w om en of t h e social world in healt h services: a cyclical perspect ive on how pov er t y r epr odu ces it self
Sur v iv al st r at egies for illness
t he econom ic r esour ces t o pay for t he m edical car e
or at t ent ion t hey need, t hey develop m echanism s and
st r at eg i es t o o v er co m e t h e p o v er t y si t u at i o n an d
healt h care and t hey approach t heir social net work t o
obt ain t he econom ic and m oral support of t he parent s
of t heir godchildr en ( “ com padr es” ) , t heir godpar ent s,
br ot her s, sist er s, par ent s, fr iends. Besides, loans ar e
a n o t h e r m e ch a n i sm t o so l v e t h e i r i l l n e ss- r e l a t e d
p r o b l e m s , t o p a y w i t h i n t e r e s t , s i g n i n g c r e d i t
d o c u m e n t s o r s e e k i n g l o a n s f r o m r e l a t i v e s a r e
com m on st rat egies in t hese sect ors of t he populat ion.
The follow ing t est im ony is an ex am ple:
Yes, t o him also, t he adm inist rat ion of t he DI F [ social
services agency] helped us, t hey gave us t he m edicine for him ,
because we didn’t have anyt hing t o care for him wit h. Well m y
husband asked for m oney. [ Who did he ask?] A m an… for a loan,
wit h int erest - he charged us t en percent ( I nt erview 74) .
These loans can pay for hospit alizat ion cost s,
consult s, t he pur chase of m edicines and ev en food,
t he follow ing t est im ony confir m s t his:
Well, since one is always asking, due t hat you don’t
have for food or anyt hing, well, you approach t hose who have and
he did us t he favor of lending us m oney ( I nt erview 230) .
Ot h er r esou r ces u sed , ar e t h e p aw n in g of
pr oper t ies and t he sale of anim als:
At t im es we have gone int o debt , we pawn what we
have, we have sold one or t wo farm anim als ( pigs) , we ask t he
whole fam ily ( I nt erview 158) .
When povert y is m anifest ed next t o a healt h
p r o b l e m , a n i n c r e a s e i n e c o n o m i c e x p e n s e s i s
su p p osed , a sit u at ion t h at in cr eases t h e econ om ic
cr isis of t h e f am ilies. As h as been obser v ed in t h e
t est im on ies, if t h er e ar e n o econ om ic r esou r ces t o
access t h e in dispen sable - su ch as f ood - w h en an
i l l n e s s o c c u r s , o n e m u s t r e s o r t t o e x t r e m e
m ech an ism s or sit u at ion s t o ob t ain t h e n ecessar y
m on ey t o con f r on t t h e ex p en ses g en er at ed b y t h e
illn ess.
To observe t he way in which t he poor people
at t end t o t heir healt h is a way of verifying t he social
r ep r o d u ct i o n t h a t p a sses f r o m o n e g en er a t i o n t o
anot her ; w hich is t o say, j ust as t he w om an at t ends
t o her healt h in t he places consider ed t o be for t he
poor, t h e sam e t h in g h appen s f or h er ch ildr en an d
her gr andchildr en. They ex pr ess t his in t he follow ing
w a y :
Yes, when I was bad off j ust now, m y son didn’t give
m e few m oney and wit h t hat , som e days we at e and som e we
didn’t . [ Your older son work, does he work?] Yes, at t im es, right
now he hasn’t been w orking for a m ont h, [ Where does he w ork?]
He is a m ason t oo ( I nt erview 156) .
DI SCUSSI ON
Th e cu r r en t t en d en cy b et w een r esear ch er s
is t o r esor t t o quant it at iv e m et hodology t o m easur e
pov er t y ; and not t o appr oach t o qualit at iv e m et hods in or der t o r epor t h ow per son s liv e an d ex per ien ce
t hat pov er t y( 10). The few qualit at iv e r esear ches t hat
a p p r o a ch t h i s t h e m e co n si d e r t h e i m p o r t a n ce o f including t he analysis of t he subj ect ivit y in t he com plex
pov er t y phenom ena as a cent r al fact or w hich allow s
t o get closer t o t he socio- cult ur al dim ension of w hat
cu r r en t ly sign ifies t o be poor an d t o t h e ch allen ges t hat need t o be faced versus adversit y in healt h care
and at t ent ion( 15- 16). This st udy cont ribut es wit h rich life
in f or m at ion r egar din g pov er t y in r elat ion t o h ealt h , w hich allow s under st anding t he phenom ena.
Povert y is a det erm ining m ot ive in t he healt h
ca r e o f w o m en . A sp eci f i c ch a r a ct er i st i c o f a d u l t wom en wit h respect t o t he povert y sit uat ion in which
t hey live, is m anifest ed in t he fact t hat t hey are socially
d ep en d en t on t h eir sp ou se an d g r ow n - u p son s or
d a u g h t e r s. Th i s i s w h y t h e y ca n ’ t a cce ss h e a l t h ser v ices, h av e econ om ic su ppor t an d/ or be able t o
buy m edicines. As a consequence of t hat , t hey t end
t o say t hey are healt hy so t heir spouse and grown- up sons or daught er s w ill not hav e t o spend m oney on
t hem . The sit uat ion generally present s it self when t heir
spouses and/ or sons and daught ers are wit hout work. They avoid, in t hat case, any com m it m ent associat ed
wit h t heir healt h ( t o go t o a m edical consult or t o get
m edicine) so as not t o hav e t o ut ilize t he econom ic
help of t heir fam ily m em bers. They are adult w om en who don’t have t he educat ional opport unit ies and who
h a v e b a d o r n o n e p a i d j o b s. Th e St a t e d o es n o t
assu m e an y social r esp on sib ilit y f or t h is g r ou p of w o m en .
The w ay in w hich t he w om en per ceiv e t heir
social belonging t o t he m ost disfavor ed sect or of t he popu lat ion , is clear ly r ef lect ed in t h e ex per ien ce of
h e a l t h c a r e r i g h t s . Th i s e x p e r i e n c e i s i n i t i a l l y
underst ood as t he condit ion of care which corresponds
t o t h e poor f or t h e f act of bein g so. I n agr eem en t w it h t h is sam e con dit ion , t h e bar r ier s f or adequ at e
sanit ary at t ent ion are m ade evident and are expressed
in t h e con cr et e d if f icu lt ies t h at p r ev en t t h em f r om se e k i n g o u t a p r i v a t e p r a ct i t i o n e r o r a l t e r n a t i v e
classes w it h g r eat er econ om ic p ow er. Th is w ay of
per ceiv ing r est r ict ions in healt h car e and in t he cur e
of t heir illnesses, can be of such m agnit ude, t hat it
r e s u l t s i n a s i t u a t i o n t h a t b e c o m e s h a b i t u a l :
confor m it y w hen faced w it h t he per spect iv e t hat t he
d i sease w i l l p r o g r ess u n t i l d eat h . Th i s p er cep t i o n
appear s t o be associat ed w it h poor per sons because
of t he fact t hat t hey are vict im s of t heir own condit ions
wit hout t hinking t hat povert y is a socio- st ruct ural fact
t h at can b e t r an sf or m ed if econ om ic p olicies f av or
t he m aj or it y of t he social gr oups.
Som e m echanism s t o r eact and confr ont t he
lim it at ions im posed by povert y and illness exist when
f a ci n g e v e n t u a l m e d i ca l u r g e n ci e s. Fo r e x a m p l e :
financial loans, t he sale of farm anim als, t he pawning
of t he scar ce belongings ( a r adio, a t elev ision, et c.) ,
support from t heir social net w ork such as fam ily and
f r ien ds. Am on g t h ese, t h e loan is t h e m ost u t ilized
m ech an ism t o con f r on t a sit u at ion of u r g en cy an d
cr isis. Ther efor e, hav ing t he necessar y r esour ces for
t he daily car e r equir ed t o st r engt hen t heir healt h is
difficult t o achiev e.
Th e w o m e n e x p e r i e n c e t h e s i t u a t i o n o f
p ov er t y an d g en d er as som et h in g u n alt er ab le t h at
has alw ays exist ed and t hat w ill not likely change. A
r eact ion or r esponse t o t hese im posed lim it at ions is
n ot ob ser v ed . Th is p h en om en a can b e ap p r oach ed
fr om t he per spect ive of a sociological analysis of t he
m anagem ent of adversit y; social inequalit y is not only
ex pr essed in t h e scar cit y of m at er ial r esou r ces an d
lim it ed access t o healt h ser v ices but on t he lev el of
self – st r u ct u r e an d t h e m an ag em en t of ad v er sit y.
The wom en in t his st udy, given t he sit uat ion of pov ert y
in which t hey live, have a poor self- st ruct ure t hat lim it s
t heir dev elopm ent of m or e adequat e social net w or k s
an d m or e effect iv e st r at egies t o face t h e pr ocesses
of healt h and illness( 17).
CONCLUSI ONS AND RECOMMENDATI ONS
When appr oaching t o t he exper ience of poor
w om en in t his r esear ch - in r elat ion t o t heir healt
h-we ident ify t he following: t here is a clear idea t hat if
w om en h av e h ad econ om ic r esou r ces t h eir h ealt h
pr oblem w ill hav e been solv ed in anot her w ay ; t hey
ar e also conv inced t hat for being poor t hey hav e t o
c o n t e n t t h e m s e l v e s w i t h a b a d q u a l i t y m e d i c a l
at t ent ion, t his confor m it y m ak es t hem finally r esign
t o t he fact of eit her loosing a part of t heir own bodies
or even j ust wait for deat h.
Th e s e r e f l e c t i o n s g i v e r i s e t o c e r t a i n
quest ions: Why don’t t he wom en quest ion t heir social
sit uat ion in relat ion t o t he way in which t hey care for
and at t en d t o t heir h ealt h? How can w e giv e social
an d p olit ical v alu e t o t h at w h ich t h ey r ealize w it h
respect t o healt h care in t he hom e arena? These new
quest ions open lines of quest ioning for fut ure st udies.
I t is im por t ant t o be able t o m anage t he concept of
“ em pow er m ent ”, w hich is under st ood as t he capacit y
t o cr eat e, r ed iscov er n ew w ay s of ex er cisin g t h eir
p ow er f or t h e b en ef it of t h em selv es. Th e f em in ist
t h eor i es m ak e u se of t h i s con cep t u si n g i t i n t h e
an aly sis of social t r an sf or m at ion , accor d in g t o t h e
fem inist concept of t he world, in a way t hat supposes
a r adical alt er n at ion of t h e pr ocesses or st r u ct u r es
t hat reproduce t he subordinat e posit ion of t he wom en
such as gender( 18).
Recovering t he experience of poor w om en in
relat ion t o t heir healt h care in order t o m odify t hese
per sonal ex per iences w e pr opose, on one hand, t hat
t he st ak eholder s of healt h policies shall consider t he
im pr ov em ent of access and qualit y of healt h car e in
public healt h services; and, on t he ot her, t hat healt h
pr ofessionals m ust be sensible in or der t o apply t his
policy in spit e of t he social st at us of wom en.
REFERENCES
1. Colom o C. Perspect iva de la salud int egral en m uj eres en sit uación de m arginalidad. En: López, C, Prado, R, C, Herranz JS, edit ores. Salud y Género [ Perspect ive of int egral healt h in w om en in m ar gin alit y sit u at ion . I n : Ber n is pp. Healt h an d Gender ] . Madr id: Ediciones de la Univ er sidad Aut ónom a de Mad r id ; 2 0 0 1 .
2. Cent ro de I nform ación de las Naciones Unidas para México, Cuba y República Dom inicana. [ Hom epage en la red] . [ Cit ado en 20 Ener o 2005] . Las car as de la pobr eza; [ 1 Búsqueda] . Disponible en : ht t p: / / w w w .unam .m x/ cinu/ com un/ com u44.ht m 2 0 0 3
3. Knaul F, Frenk J, Aguilar M A. Pobreza y salud. En: Sepúlveda J. Salud Panam er icana en el siglo XXI . For t alecim ient o de la coop er ación in t er n acion al y d esar r ollo d e cap it al h u m an o. Méx ico: I NSP; 2 0 0 2 . p . 4 7 - 5 5 .
4. Musgrove P. Pobreza y salud. Com ent arios. En: Sepúlveda J. Salud Panam er icana en el siglo XXI . For t alecim ient o de la coop er ación in t er n acion al y d esar r ollo d e cap it al h u m an o. Méx ico: I NSP; 2 0 0 2 . p. 5 7 - 9 .
5. sedesol. gob.m x [ Hom epage en la red ] . México: sedesol; [ cit ado 2 0 0 3 ] . Dispon ible en h t t p: / / w w w . sedesol. gob. m x / desr eg/ su pob. h t m .
7 . Salles V, Tuir an R. Muj er es y hogar es en Méx ico: ¿Cada vez m ás pobres? En: Cuent o cuest a la pobreza de las m uj eres: Un a p er sp ect i v a d e Am ér i ca La t i n a y el Ca r i b e. Méx i co : UNI FEM; 1 9 9 5 .
8. Pedrero M, Rendón T, Barrón A. Desigualdad en el acceso a opor t u n idades de em pleo y segr egación ocu pacion al por género. Sit uación act ual en México y propuest as. En: Cuent o cuest a la pobreza de las m uj eres: Una perspect iva de Am érica Lat in a y el Car ibe. Méx ico: UNI FEM; 1 9 9 5 .
9. hom as V. Using fem inist and social st r uct ural analy sis t o focus on t he healt h of poor w om an. Wom en & Healt h 1994; 2 2 : 5 - 1 0 .
10. Salles V, Tuirán R. ¿Cargan las m uj eres con el peso de la pobreza? Punt os de vist a de un debat e. En: García B. Muj er, géner o y población en Méx ico. Méx ico: Colegios de Méx ico, Sociedad Mex ican a de Dem ogr afía; 2 0 0 0 .
1 1 . Co r b i n J, S t r a u s s A . Gr o u n d e d t h e o r y r e s e a r c h : Pr o ce d u r e s, ca n o n s, a n d e v a l u a t i v e cr i t e r i a . Qu a l i t a t i v e Sociol 1 9 9 0 ; 1 3 : 3 - 2 1 .
1 2 . Glaser BG. Th eor et ical m em os. I n Glaser BG, ed it or. Advances in t he m et hodology of grounded t heory. Mill Valley ( CA) : Sociolog ical Pr ess; 1 9 8 9 . p . 8 3 - 9 2 .
1 3 . St r a u ss AL, Co r b i n J. Ba si cs o f q u a l i t a t i v e a n a l y si s: t echniques and pr ocedur es: Bev er ly Hills; Sage; 1 9 9 0 . 14. Lincoln YS, Guba EG. Nat uralist ic inquir y. Bever ly Hills: Sag e; 1 9 8 5 .
15. Enr íquez Rosas R. El r ost r o act ual de la pobr eza ur bana en Méx ico. Com er cio Ex t er ior Méx ico: 2 0 0 3 ; 5 3 : 5 3 2 - 9 . 16. Polakoff E, Gregory D. Concept s of healt h: w om en st ruggle for w holeness in t he m idst of povert y. Healt h Care for Wom en I n t . 2 0 0 2 ; 2 3 : 8 3 5 - 4 5 .
1 7 . Ge r h a r d t U. Co p i n g a n d s o c i a l a c t i o n : t h e o r e t i c a l r econ st r u ct ion of t h e lif e- ev en t appr oach . Sociol of Healt h I l l n e ss 1 9 7 9 ; 2 : 1 9 5 - 2 2 1 .
18. León M. Poder y em poderam ient o de las m uj eres. Bogot a: Facu lt ad de Cien cias y Hu m an idades; 1 9 9 7 .