ALP A ETAL.
10 REV ASSOC MED BRAS 2017; 63(1):10-12
RAPID COMMUNICATION
Synthetic cannabinoids in the kidneys
ALPER ALP1*, HAKAN AKDAM2, BANU YILMAZ AVCIOğLU1, SIBEL ERSAN1
1Nephrology, Tepecik Education and Research Hospital, Izmir, Turkey
2Department of Nephrology, School of Medicine, Adnan Menderes University, Aydin, Turkey
S
UMMARYStudy conducted at Tepecik Education and
Research Hospital, Nephrology, Izmir, Turkey
Article received: 6/24/2016 Accepted for publication: 6/26/2016
*Correspondence:
Tepecik Education and Research Hospital, Nephrology
Address: Güney Mahallesi, 1140/1, Sokak n. 1
Yenişehir, Konak, Izmir – Türkiye Postal code: 35000
http://dx.doi.org/10.1590/1806-9282.63.01.10
Acute kidney injury is an important cause of mortality and morbidity today and can occur due to several reasons. As time, geographic regions, and living conditions change, various etiological agents arise with nephrotoxic effects. Awareness of such nephrotoxic effects has been raised with the increasing frequency of addictive substance use, especially among young people in society.
Keywords: synthetic cannabinoids, acute kidney injury, toxicity.
I
NTRODUCTIONSynthetic cannabinoids (SC) are addictive substances with an increasing frequency of use among the young population. It is reported that the rate of synthetic cannabinoid use among United States (US) high school students is approxi-mately 11 to 12%.1 The detection of these substances in
plasma and urine samples by toxicology tests has some dif-iculties because producers frequently change the molecular structure to avoid breaking the law. This “ghost” effect and the relatively cheap price compared with other addictive substances make SCs popular among this population.
These compounds have several psychiatric, meta-bolic, and physiological effects. In recent years, cases of acute kidney injury (AKI) have appeared due to the use of cannabinoids. Most of these cases show complete im-provement without biopsy and, therefore, biopsy indings are known in a very limited number of such cases.
Although the general histopathological inding is consistent with acute tubular necrosis (ATN), there are also cases with detected indings of tubulointerstitial nephritis. It is important to enhance awareness in this regard and also to emphasize the likelihood of developing renal injury in addicted patients.
W
HAT ARE SYNTHETIC CANNABINOIDS?
Synthetic cannabinoids are marijuana-like, non-natural, chemically produced components. Their molecular struc-ture shows much similarity with Δ9-tetrahydrocannabinol (THC), the main active compound in marijuana. Although
they are similar, SCs are more potent molecules. They act like agonists for cannabinoid (CB) receptors. Cannabis-like (mimetic effect) components in SCs affect cell receptors (CB1 and CB2) in the brain, causing an effect 100 times more potent than THC contained in normal marijuana. SCs may not be as “innocent” as marijuana and have more potent and different side effects due to their biochemical differences. Some of these components are HU-210, CP 47, 497, JWH-018, JWH-073, JWH-398, and JWH- 250.
SCs are a group of substances with addictive and psychoactive effects, which is highly popular especially among young people due to its cannabis-like effects. The commercial products are sold under the name “k2,” “spice,” and “black mamba” in the US and the European Union (EU), and “Bonsai” and “Jamaica” in Turkey.
Some other well-known products containing SCs are “spice gold,” “spice silver,” “spice diamond,” “silver,” “yu-catan ire,” “sence,” “chill X,” “smoke,” “gnie,” “algerian blend.” The formal reports both from the US and EU in-dicate that the rate of SC use is growing faster every year. They can cause many health problems, from acute severe crises to several organ dysfunctions (arrhythmia, anxiety, agitation, confusion, hypertension, seizures, hallucinations, AKI, and myocardial infarction) and even death.2
S
YNTHETICCANNABINOID-
RELATED ACUTEKIDNEYINJURY
(SC-RAKI)
SYNTHETICCANNABINOIDSINTHEKIDNEYS
REV ASSOC MED BRAS 2017; 63(1):10-12 11
result of renal exposure is AKI. A study from the US found renal injury of approximately 0.9% due to SC use.3
The mechanism of renal injury is not yet clearly de-ined.4 Acute tubular necrosis seems to be the leading
etiology for AKI among these patients. However, classical hemodynamic collapse, hypotension or hypovolemic status for development of ATN may not be present. Car-diac effects of SCs are also very well-described. The nega-tive inotropic effects on hemodynamic processes may have impact on renal blood low decrease. These cardiac effects also may aggravate prerenal conditions. Rhabdo-myolysis and cannabinoid hyperemesis syndrome are the second most commonly seen etiologies.5 Also, direct
toxic effects of the SC molecules or addictive substances during elimination from the kidney may be responsible. Unfortunately, it is not clear which components are sponsible for their nephrotoxic effect. Some reports re-vealed that in particular XLR11 and UR-144 N-pentano-ic acid metabolite were detected in the serum and urine samples of the cases with SC-RAKI.6 An experimental
study of Barutta et al. showed that blockade of CB1 recep-tors has been shown to have protective effects on renal function and ameliorate albuminuria in diabetic mice.7
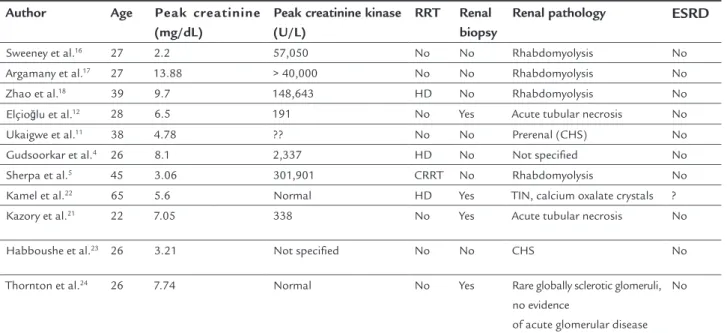
As we have a look at the literature, obviously, renal biopsy for SC-RAKI is not much preferred. The “prerenal” nature of AKI in these patients might have caused this approach. The renal biopsy applied cases mostly revealed ATN. To a rare extent, tubulointerstitial nephritis and
crescentic glomerulonephritis were reported (Table 1). Additionally, hypokalemia and hypertension may occur during SC use, but less frequently.8
R
EPORTED ETIOLOGIES FORSC-RAKI
Cannabinoid hyperemesis syndrome (CHS)
Cannabis is known for its anti-emetic effects; however, SCs may cause intractable nausea and vomiting. The most com-mon symptoms of the patients at hospital admission are nausea and vomiting due to SC use and those were consis-tent with ATN in kidney biopsies. This clinical situation is called as cannabinoid hyperemesis syndrome (CHS). Allen et al. described this entity irst in 2004.9 In some papers
“hyperemetic hydrophilic syndrome” is also used as synonym. This syndrome is more common in chronic users and courses with periodic vomiting (especially in the morning), abdominal pain or discomfort, and the desire for a hot shower. Long-term use of SCs is essential in provoking symp-toms. The cyclic pattern of these symptoms is pathogno-monic. Prerenal kidney injury may occur secondary to this presentation.10,11 Acute tubular necrosis is the most common
reason causing renal injury so biopsy may not be indicated
if the clinical presentation is as stated.12 A diagnostic
algo-rithm was described for such patients.13 The treatment
ap-proaches are palliative. Satisfactory results with haloperidol, intravenous NaCl 0.9%, paracetamol, lorazepam, ondanse-tron, and morphine use are reported in the literature.14,15
Rhabdomyolysis
Rhabdomyolysis was also shown to cause kidney injury in these cases. However, it is not clear whether direct toxic effects of compounds in SCs on muscles are respon-sible for this entity. Some other side effects of SCs like hypokalemia or hyperthermia may also have contribu-tion.16-18 In addition to these two clinical approaches,
unfortunately the pathophysiology of cannabinoid-asso-ciated renal injury has not been fully clariied. The treat-ment strategies for SC induced rhabdomyolysis did not differ from classical approaches.
Tubulointerstitial nephritis
With respect to cannabinoid-associated kidney injury, the literature very rarely contains cases with acute tubuloin-terstitial nephritis, as well.19 Although acute
tubuloint-erstitial nephritis may be directly caused by the effect of SC, various nephrotoxic chemical substances or heavy metals added to these synthetic compounds that have no standardization may also have an effect on such biopsy results.20 There are very few reports of the co-existence of
SC-RAKI and tubulointerstitial nephritis in the litera-ture.19,21 In some cases tubular oxalate crystals
accompa-nying tubulointerstitial nephritis were described.22 There
is no speciic treatment for cannabinoid-associated effects. Support therapy, cardiac monitoring, and follow-up of consciousness and vital signs are essential.
C
ONCLUSIONALP A ETAL.
12 REV ASSOC MED BRAS 2017; 63(1):10-12
C
ONFLICT OF INTERESTThe authors declare no conlict of interest.
R
EFERENCES1. The Partnership for a Drug Free America and the MetLife Foundation, The Partnership Attitude Tracking Study (PATS): Teens and Parents, 2013. 2. Behonick G, Shanks KG, Firchau DJ, Mathur G, Lynch CF, Nashelsky M, et
al. Four postmortem case reports with quantitative detection of the synthetic cannabinoid, 5F-PB-22. J Anal Toxicol. 2014; 38(8):559-62.
3. Forrester MB, Kleinschmidt K, Schwarz E, Young A. Synthetic cannabinoid and marijuana exposures reported to poison centers. Hum Exp Toxicol. 2012; 31(10):1006-11.
4. Gudsoorkar VS, Perez JA. A new differential diagnosis: synthetic cannabinoids-associated acute renal failure. Methodist Debakey Cardiovasc J. 2015; 11(3):189-91.
5. Sherpa D, Paudel BM, Subedi BH, Chow RD. Synthetic cannabinoids: the multi-organ failure and metabolic derangements associated with getting high. J Community Hosp Intern Med Perspect. 2015; 5(4):27540. 6. Castaneto MS, Gorelick DA, Desrosiers NA, Hartman RL, Pirard S, Huestis
MA. Synthetic cannabinoids: epidemiology, pharmacodynamics and clinical implications. Drug Alcohol Depend. 2014; 144:12-41.
7. Barutta F, Corbelli A, Mastrocola R, Gambino R, Di Marzo V, Pinach S, et al. Cannabinoid receptor 1 blockade ameliorates albuminuria in experimental diabetic nephropathy. Diabetes. 2010; 59(4):1046-54.
8. Hermanns-Clausen M, Kneisel S, Szabo B, Auwärter V. Acute toxicity due to the conirmed consumption of synthetic cannabinoids: clinical and laboratory indings. Addiction. 2013; 108(3):534-44.
9. Allen JH, de Moore GM, Heddle R, Twartz JC. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut 2004; 53(11):1566-70.
10. Bhanushali GK, Jain G, Fatima H, Leisch LJ, Leisch LJ, Thornley-Brown D. AKI associated with synthetic cannabinoids: a case series. Clin J Am Soc Nephrol. 2013; 8(4):523-6.
11. Ukaigwe A, Karmacharya P, Donato A. A gut gone to pot: a case of cannabinoid hyperemesis syndrome due to K2, a synthetic cannabinoid. Case Rep Emerg Med. 2014; 2014:167098.
12. Elçioğlu OC, Başçı S, Bakan A, Aydin Bahat K, Özlük MY, Kiliçaslan I, et al. Synthetic cannabinoids associated acute kidney ınjury: case report. Turkiye Klinikleri J Nephrol. 2015; 10(2):43-6.
13. Simonetto DA, Oxentenko AS, Herman ML, Szostek JH. Cannabinoid hyperemesis: a case series of 98 patients. Mayo Clinic Proc. 2012; 87(2):114-9. 14. Price SL, Fisher C, Kumar R, Hilgerson A. Cannabinoid hyperemesis syndrome
as the underlying cause of intractable nausea and vomiting. J Am Osteopath Assoc. 2010; 111(3):166-9.
15. Hickey JL, Witsil JC, Mycyk MB. Haloperidol for treatment of cannabinoid hyperemesis syndrome. Am J Emerg Med. 2013; 31(6):1003.e5-6. 16. Sweeney B, Talebi S, Toro D, Gonzalez K, Menoscal JP, Shaw R, et al.
Hyperthermia and severe rhabdomyolysis from synthetic cannabinoids. Am J Emerg Med. 2016; 34(1):121.e1-2.
17. Argamany JR, Reveles KR, Duhon B. Synthetic cannabinoid hyperemesis resulting in rhabdomyolysis and acute renal failure. Am J Emerg Med. 2016; 34(4):765.e1-2.
18. Zhao A, Tan M, Maung A, Salifu M, Mallappallil M. Rhabdomyolysis and acute kidney ınjury requiring dialysis as a result of concomitant use of atypical neuroleptics and synthetic cannabinoids. Case Rep Nephrol. 2015; 2015:35982. 19. Centers for Disease Control and Prevention (CDC). Acute kidney injury associated with synthetic cannabinoid use – Multiple states, 2012. MMWR Morb Mortal Wkly Rep. 2013; 62(6):93-8.
20. Wells DL, Ott CA. The “new” marijuana. Ann Pharmacother. 2011; 45(3):414-7. 21. Kazory A, Aiyer R. Synthetic marijuana and acute kidney injury: an unforeseen
association. Clin Kidney J. 2013; 6(3):330-3.
22. Kamel M, Thajudeen B. A case of acute kidney injury and calcium oxalate deposition associated with synthetic cannabinoids. Saudi J Kidney Dis Transpl. 2015; 26(4):802-3.
23. Habboushe J, Sedor J. Cannabinoid hyperemesis acute renal failure: a common sequela of cannabinoid hyperemesis syndrome. Am J Emerg Med. 2014; 32(6):690.e1-2.
24. Thornton SL, Wood C, Friesen MW, Gerona RR. Synthetic cannabinoid use associated with acute kidney injury. Clin Toxicol (Phila). 2013; 51(3):189-90.
TABLE 1 Recently reported cases of SC-RAKI (between 2013 and 2016).
Author Age Peak creatinine
(mg/dL)
Peak creatinine kinase (U/L)
RRT Renal
biopsy
Renal pathology ESRD
Sweeney et al.16 27 2.2 57,050 No No Rhabdomyolysis No
Argamany et al.17 27 13.88 > 40,000 No No Rhabdomyolysis No
Zhao et al.18 39 9.7 148,643 HD No Rhabdomyolysis No
Elçioğlu et al.12 28 6.5 191 No Yes Acute tubular necrosis No
Ukaigwe et al.11 38 4.78 ?? No No Prerenal (CHS) No
Gudsoorkar et al.4 26 8.1 2,337 HD No Not speciied No
Sherpa et al.5 45 3.06 301,901 CRRT No Rhabdomyolysis No
Kamel et al.22 65 5.6 Normal HD Yes TIN, calcium oxalate crystals ?
Kazory et al.21 22 7.05 338 No Yes Acute tubular necrosis No
Habboushe et al.23 26 3.21 Not speciied No No CHS No
Thornton et al.24 26 7.74 Normal No Yes Rare globally sclerotic glomeruli, no evidence
of acute glomerular disease No