w w w . r b o . o r g . b r
Original
Article
ACL
ideal
graft:
MRI
correlation
between
ACL
and
humstrings,
PT
and
QT
夽
Fabiano
Kupczik
a,
Marlus
Eduardo
Gunia
Schiavon
b,
Bruno
Sbrissia
b,
Rodrigo
Caldonazzo
Fávaro
b,
Rafael
Valério
c,∗aMScinSurgery,OrthopedistandHeadoftheKneeGroupatHospitalUniversitárioCajuru,PontifíciaUniversidadeCatólicadoParaná
(PUC-PR),Curitiba,PR,Brazil
bOrthopedistintheKneeGroup,HospitalUniversitárioCajuruPUC-PR,Curitiba,PR,Brazil
cResidentPhysicianinOrthopedicsandTraumatology,HospitalUniversitárioCajuru,PUC-PR,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13September2012 Accepted7November2012
Keywords:
Anatomy
Anteriorcruciateligament Magneticresonancespectroscopy
a
b
s
t
r
a
c
t
Objective:TheobjectiveofthisstudywastomeasureinMRIscans,thesizeoftheorigin, insertionandlengthoftheanteriorcruciateligamentandpossiblegraftforreconstruction surgeryincaseofinjury.Besidesthis,therewasacrossbetweenstatisticaldatatotestthe hypothesisofproportionalrelationshipbetweentheseanatomicalextent.
Materialsandmethods:52MRIexaminationsperformedbetween2008and2011werevalued atrandominalongitudinalretrospectiveepidemiologicalstudy.Tomeasurethewidthof theACLwasusedcoronalobliquetothelengthofthesagittalsection,forinsertingthetibial coronalfemoralinsertionandwasalsousedobliquecoronalsection.
Results:TheaveragediameteroftheACLwas4.80mm(3.1–8.3mm),withalengthof3.8cm (2.85–4.5cm).Theoriginrangedfrom9.7mmto15.4mm.Theaverageinsertiononthetibia was13.3mm.Theaveragediameterofthesemi-tendinouswas4.38mmandtheaverage diameterwas3.42mmgracilis.Thequadricepspresenteddiameterof7.67mm,alengthof 35.34mmand4.54mmpatellartendondiameterand26.62mminaveragelength.
Conclusion: Thesedataprovideimportantinformationforthepre-operativesurgeon, facil-itatingpreoperativeplanningandprovidingviablealternativesandavoidinginadequate grafts.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Enxerto
ideal
para
ligamento
cruzado
anterior:
correlac¸ão
em
ressonância
magnética
entre
LCA,
isquiotibiais,
tendão
patelar
e
tendão
quadríceps
Palavras-chave:
Anatomia
r
e
s
u
m
o
Objetivos:Mensuraremexamesderessonânciamagnética(RM)otamanhodaorigem,a inserc¸ãoeocomprimentodoligamentocruzadoanterior (LCA)eseuspossíveis enxer-tos paracirurgia de reconstruc¸ãoem caso de lesão. Além desse,fez-seo cruzamento
夽
StudyconductedattheHospitalUniversitárioCajuru,PontifíciaUniversidadeCatólicadoParaná,Curitiba,PR,Brazil.
∗ Correspondingauthorat:Av.SãoJosé,300,CristoRei,Curitiba,PRCEP80050-350,Brazil.
E-mail:[email protected],[email protected](R.Valério).
Espectroscopiaderessonância magnética
Ligamentocruzadoanterior
estatísticoentreosdadosparatestarahipótesederelac¸ãoproporcionalentreessasmedidas anatômicas.
Materiaisemétodos:Foramfeitos52examesdeRMentre2008e2011eavaliadosdemaneira aleatóriaemumestudoepidemiológicolongitudinalretrospectivo.Paraamensurac¸ãoda larguradoLCAfoiusadoocortecoronaloblíquo,paraocomprimentoocortesagital,para ainserc¸ãotibialocortecoronaleparaainserc¸ãofemuralocortecoronaloblíquo.
Resultados: OdiâmetromédiodoLCAfoide 4,80mm(3,1–8,3mm)eocomprimentode 3,8cm(2,85–4,5cm).Aorigemvariouentre9,7mme15,4mm.Ainserc¸ãomédianatíbiafoi de13,3mm.Odiâmetromédiodosemitendíneofoide4,38mmeodiâmetromédiodográcil de3,42mm.Oquadrícepsapresentoudiâmetrode7,67mmecomprimentode35,34mme otendãopatelar4,54mmdediâmetroe26,62mmdecomprimentomédio.
Conclusão: Os dadosobtidosforneceminformac¸õespré-operatóriasimportantesparao cirurgião,facilitamoplanejamentopré-operatório,apresentamopc¸õesviáveiseevitam enxertosinadequados.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Becauseofthehighincidenceofanteriorcruciateligament (ACL)injuriesamongthepopulation,thesehavebeenthe sub-jectofmanyrecentstudies.1–7TheACLhasthefunctionof
themainstabilizerforanteriortranslationofthetibiaandhas secondaryparticipationinlimitingtheinternalrotationofthe knee.3,4,8
TheACLhasitsoriginintheposteriorportionofthelateral femoralcondyle.Ithasanintra-articularand extrasynovial pathandisinsertedlaterallyandanteriorlytothemedial tib-ialspine.Themodelthatismostacceptedtodaycomprises twobandsandwascreatedbyGirgisetal.6Inthis,an
antero-medial(AM)bandemergesmoreproximallyandposteriorly tothefemur,whiletheposterolateral(PL)bandismore dis-taland anterior.Thebandsare twistedalongtheir pathin theintercondylarregionandtheirinsertioninthetibia fol-lowstheorderthatgivesthemtheirname:anteromedialto AMandposterolateraltoPL.
BecauseoftheinstabilitycausedbyACLinjuryandthe pos-siblecomorbiditiesconsequenttoitsrupture,suchaschondral lesions, meniscal lesions and possibly early osteoarthro-sis,the recommended treatmentissurgical, withligament reconstruction.9,10
Severalgraft sourceshavenowbeen showntobe effec-tiveforACLreconstruction.Choosingtheidealgraftisdone onanindividualbasisaccordingtothepatient’sprofileand the nature of the injury, in addition to the surgeon’s per-sonalexperience.Graftsderivedfromthequadricepstendon andfromtheflexorshaveemergedasalternativesto patel-largrafts,followingstudiesrelatingtoanteriorkneepainand comorbiditiesinthe donorsite.11–14 Controversystillexists
withregardtochoosingtheidealgraft,andithasbeenshown intheliteraturethatoneofthemainfactorsinmakingthe decisionisthefinalwidthofthegraft.Graftsofwidthsless than 7mmtend tofail moreeasily, whilewider grafts are safer.12,13,15
Some studies have attempted to demonstrate possible predictive factors for the diameters of the grafts gener-allyusedinsurgicalreconstructionprocedures,amongACL measurements.12,16–19Inourreviewoftheliterature,wedid
not findany article that attempted toestablish a relation-shipbetweenthecharacteristicsoftheACLanditspossible grafts.
Thefirstobjectiveofthisstudywastomeasurethesizes oftheoriginandinsertionandthelengthoftheACLamong thepopulationofCuritiba,usingmagneticresonanceimaging (MRI)examination.Thepossiblegrafts forreconstructionof theACLweremeasured.Thesecondobjectiveofthisstudywas tocross-correlatebetweenthesedataandtestthehypothesis thattherewouldbeaproportionalrelationshipbetweenthe ACLmeasurementsandtheirpossiblegrafts.
Materials
and
methods
Afterapprovalhadbeen obtainedfrom theEthics Commit-teebymeansofthe“PlatformBrazil”website,followingethics assessment under presentation certificate number (CAAE) 01338212.5.0000.0100, we gathered datafrom examinations performedbetweenNovember2011andJanuary2012.Also, 52 MRI examinations performed between 2008 and 2011 werereviewedinaretrospectivelongitudinalepidemiological study.
Theinclusioncriteriawerethatthepatientsshouldbe:(1) skeletallymatureandagedunder40years;(2)freefromany previousligamentinjuriesordegenerativelesions.
Theexclusioncriteriawere thatthepatientsshouldnot have:(1)anopengrowthplate;(2)previoussurgery;(3) previ-ousligamentinjury;(4)hyper-slackligaments;(5)degenerative diseases; (6) continuous corticoid use; or (7) intercondylar hypoplasia(widthofthedistalfemur/condylarfossa<0.2).
ThevariablesinthisstudyweremeasuredinMRI exami-nationsbyasinglemedicalradiologist.Forthisexamination, aSiemensMagnetomAvanto1.5t®machinewasused.Allthe
examinationswereperformedusingtheprotondensity tech-niquewithfatsuppression.
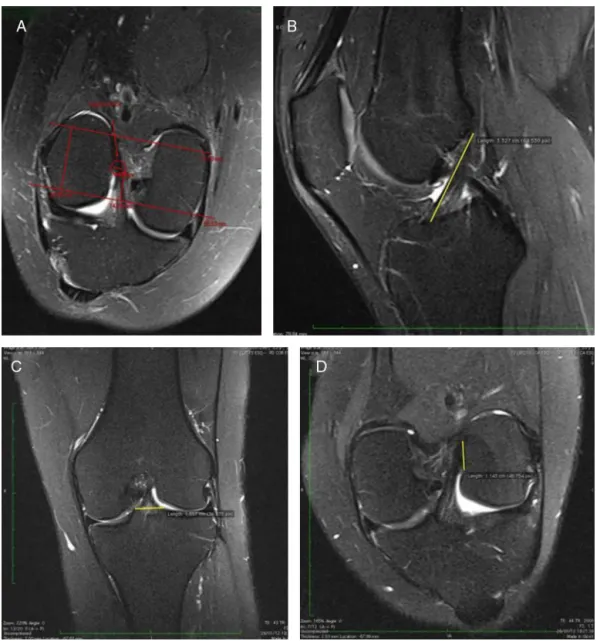
Fig.1–MeasurementofthewidthoftheACL(A);measurementofthelengthoftheACL(B);measurementofthetibial insertionoftheACL(C);measurementofthefemoraloriginoftheACL(D).
showedtheACLalongitsgreatestlength.Forthetibial inser-tionoftheACL,acoronalslicewasused,whichdemonstrated thegreatestthickness.Forthefemoralinsertion,anoblique coronalslicewasused(Fig.1).
Thetendonsofthesemitendinosusandgraciliswere mea-suredaroundtheirgreatestdiameterintheaxialplane,using themedialepicondyleastheslicelevel(Fig.2).
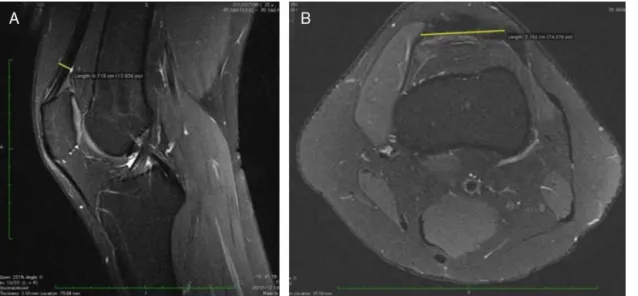
Tomeasuretheside-to-sidelengthofthequadriceps ten-don,anaxialsliceattheslicelevelof3cmproximallytothe patellarinsertionofthistendonwasused.The anteroposte-riordiameterofthetendonwasmeasuredusingasagittalslice atthesameslicelevel(Fig.3).
Tomeasuretheside-to-sidelengthofthepatellartendon, anaxialslice attheslice levelofhalfwayalongthe length ofthetendonwasused.Theanteroposteriordiameterofthe tendonwas measured ona sagittalslice atthe same slice level. The lengthof the tendon was measured on a sagit-talslicethatdemonstratedthegreatestlengthofthetendon (Fig.4).
Statistical
methodology
Toinvestigatelinearassociationsbetweenthevariables, Pear-son’scorrelationcoefficientwasestimated.Thisestimatewas takenasevidenceinevaluatingthehypothesisofnull corre-lationinthepopulation.
pvalueslessthan0.05indicatedstatisticalsignificance.
Results
Fifty-twoMRIexaminationscovering31menand21women wereassessed.Thepatients’meanagewas28years,witha rangefrom18to36years.
Fig.2–Measurementofthewidthofthetendonsofthe semitendinosusandgracilis.
the optionalhypothesisoflinear correlationdiffering from zero.Insequence,thecorrelationestimatesandthep-values ofthestatisticaltestswerepresented.
Themeanwidth(diameter)oftheACLinthemiddlethirdof theintercondylarregionwas4.80mm(3.1–8.3mm).Themean
lengthoftheACLinthesagittalsliceswas3.8cm(2.85–4.5cm). TheoriginoftheACLrangedfrom9.7mmto15.4mm,witha meanof12.3mm.ThemeaninsertionoftheACLinthetibia was13.3mm,witharangefrom9.1to17.5mm.
Themeandiameterofthesemitendinosuswas4.38mm, witharangefrom3.4to7.2mm.Themeandiameterofthe graciliswas3.42mm,witharangefrom2.4to4.9mm.
Inrelationtothequadriceps,thediameterwas7.67mm, witharangefrom5.5to9.9mm.Thediameterofthepatellar tendonwas4.54mm,witharangefrom3.5to6.6mm.
Thelengthofthequadricepstendonwas35.34mm,witha rangefrom26.9to45.8mm.Thepatellartendonpresenteda meanlengthof26.62mm,witharangefrom22.4to35.7mm.
Datacorrelation
ThecorrelationcoefficientsbetweentheACLmeasurements andthesemitendinosusandgracilistendonsareexpressedin Table1.
The correlation coefficients between the ACL measure-mentsandthepatellartendonareexpressedinTable2.
Fig.3–Measurementoftheside-to-sidelengthofthequadricepstendon(A);measurementoftheanteroposteriordiameter ofthequadricepstendon(B).
Table1–CorrelationoftheACLwiththetendonsofthe semitendinosusandgracilis.
Variable Correlationcoefficient p-Value
ACLfemur
Semitendinosus 0.317 0.022
Gracilis 0.364 0.008
ACLtibia
Semitendinosus 0.064 0.654
Gracilis 0.072 0.611
ACLwidth
Semitendinosus 0.119 0.400
Gracilis 0.122 0.390
ACLlength
Semitendinosus 0.346 0.012
Gracilis 0.334 0.015
ACL,anteriorcruciateligament.
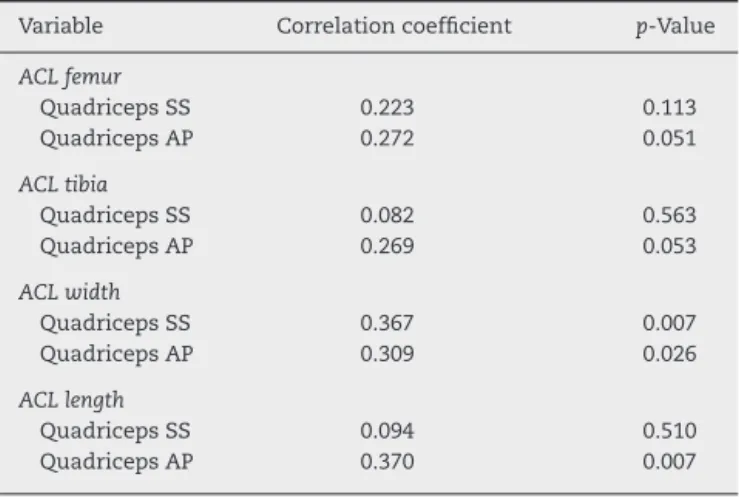
The correlation coefficients between the ACL
measure-mentsandthequadricepsareexpressedinTable3.
Discussion
In correlating the ACL measurements among the popu-lation evaluated in this study, we found that the mean length was 38.13mm (28.5–45), the mean femoral origin was 12.31mm (9.7–15.4) and the mean tibial insertionwas 13.30mm(9.1–17.5).
Nostudyhasevaluatedexactlythesamemeasurementsas inthepresentstudy,butDienstetal.4foundameanlengthof
32mm,witharangefrom22to41,andwidthatthefemoral originrangingfrom7to12mm.
Duthonetal.7 foundthatthe meansizeoftheACLwas
30mm(7–12),thefemoraloriginwasbetween11and24mm andthetibialinsertionwasbetween8and12mm.
In the study by Zantopet al.20 the mean value forthe
femoraloriginwasfoundtobe11mmandthetibialinsertion wasapproximately13.2mm.
Table2–CorrelationbetweenACLandpatellartendon.
Variable Correlationcoefficient p-Value
ACLfemur
PatellartendonSS 0.438 0.001
PatellartendonAP 0.283 0.042
ACLtibia
PatellartendonSS 0.233 0.096
PatellartendonAP 0.173 0.221
ACLwidth
PatellartendonSS 0.415 0.002
PatellartendonAP 0.099 0.487
ACLlength
PatellartendonSS 0.451 0.001
PatellartendonAP 0.476 <0.001
AP,anteroposterior;ACL,anteriorcruciateligament;SS, side-to-side.
Table3–CorrelationbetweenACLandquadriceps tendon.
Variable Correlationcoefficient p-Value
ACLfemur
QuadricepsSS 0.223 0.113
QuadricepsAP 0.272 0.051
ACLtibia
QuadricepsSS 0.082 0.563
QuadricepsAP 0.269 0.053
ACLwidth
QuadricepsSS 0.367 0.007
QuadricepsAP 0.309 0.026
ACLlength
QuadricepsSS 0.094 0.510
QuadricepsAP 0.370 0.007
AP,anteroposterior;ACL,anteriorcruciateligament;SS, side-to-side.
Some studies in the literature stand out through their
attemptstoseekpredictivefactorsforpossiblegraftsforuse inreconstructingtheACL.12,16–19Xieetal.17analyzed235
Chi-nese peoplewiththeaimofseekingacorrelationbetween anthropometric factors,sports activity,age andgenderand thelengthanddiametermeasurementsoftheflexortendons. Theyfoundthatthemostimportantcorrelationbetweenthe diameterandlengthofthesemitendinosusandgraciliswere withtheindividual’sheight,genderandweight.
Alongthesamelineofresearch,Tumanetal.18conducted
acohortstudyon106patientsandconcludedthatheightwas themostimportantpredisposingfactorforflexordiameter, particularlyinwomen.
InthestudybyBickeletal.21therewasanimportant
cor-relationbetweensummedSTandGareasandvaluesgreater than18mm2inaxialMRIslices.Accordingtotheseauthors,
thisvaluewouldprovidesufficientgraftingin88%ofthecases. InastudyusingMRItoattempttopredictthesizeofthe flexortendongraft,Werneckeetal.16recommendedanarea
of10mm2forthegracilistendonand17mm2 forthe
semi-tendinosustendon,foraquadruplegraft.
Wedidnotfindanystudiesintheliteratureattemptingto correlatethecharacteristicsofACLwiththeirpossiblegrafts, bymeansofMRIexaminations.
Thereisnorecommendedstandardfortheleveloftheslice usedformeasuringpossiblegraftsforthecruciateligament. Wefoundstudiesintheliteraturethatusedthesameslices butwithdivergentreferencepointsorlevels.11,12,16,22
Tomeasuretheflexortendons,Werneckeetal.16usedthe
mostprominentportion ofthe medialepicondyleasa ref-erencepointfortheaxialslice.Erikssonetal.11usedaslice
5cmfromthekneejointand,inastudyonadolescents,Bickel etal.21usedthegrowthplatelineasareferencepoint.Lastly,
Rispolietal.22usedtheupperpoleofthepatellaasaparameter
foritsaxialslice.
Inourstudy,weusedthemedialepicondyleasareference, withinthesamecontextasWerneckeetal.16
intermediatepointbetweenthelowerpoleofthepatellaand theanteriortuberosityofthepatella.
Inrelationtothequadriceps,itwasnotpossibleto mea-sureitslengthbecausetheimagingevaluateddidnotinclude slicesclosetothethigh,i.e.thesiteoforigin.Weestablished areference point3cm from its insertioninthe patella for theevaluation,becausewebelievethattheproximallimitis muscularandthatthereisnoprecisepoint.
Inourstudy,themorphologicalcharacteristicoftheACL thatsinglyshowedthegreatestcorrelationwiththepossible graftswasthelengthoftheACL.However,therewasno cor-relationwiththeside-to-sidewidthofthequadricepstendon. Consideringthe individualityof each possible graft, we foundinterestingresults.Theflexortendonsshowedstrong correlationcoefficientswiththeACLinsertioninthefemur anditslength.However,therewasnocorrelationbetweenthe tibialinsertionandthewidthoftheACLintheintercondylar region.
Forthepatellartendon,themostfaithfulstandardswere thefemoraloriginandthelengthoftheACL.Thislast parame-teristheonethatbestpredictedtheanteroposteriordiameter ofthetendon.Fortheside-to-sidediameter,thecoefficients forthefemoraloriginandlengthwereequivalent.Neitherthe insertionoftheACLnoitswidthintheintercondylarregion showedanycorrelation.
Thequadricepstendonshowedanimportantrelationship withthe widthoftheACLintheintercondylarregion.This variablewasagoodindicatorbothfortheside-to-side diame-ter(greatestcorrelation)andfortheanteroposteriordiameter. However,thelengthoftheACLwasthevariablewiththe great-estcorrelationwiththeanteroposteriordiameter.
Investigationofgraftpredictionfactorsisafieldthatstill needstobeexploredwithinoursetting.Webelievethat indi-vidualizationofeachcasewithdifferentvariables,andwith summingoftheanthropometricandMRIdata,mayprovide guidance in choosingthe mostprecise and risk-free graft. Studieswithlargersamplesareneeded.
Conclusion
Themeasurementsfoundamongthepopulationstudiedwere similartothoseintheliterature,inrelationtobothlengthand originandinsertion.
WebelievethatinMRIexaminationsusingroutineslices, thebest wayofpredictingthediameters oftheflexor ten-donsandpatellartendonisthroughthelengthoftheACL.The widthoftheACListhebestpredictorforthequadriceps ten-don.ThelengthoftheACListhesinglecharacteristicthathas thebestcorrelationwiththepossiblegrafts,whilethetibial insertionisnotareliableparameter.
Ourdataprovideimportantpreoperativeinformationfor surgeons.Theyfacilitatepreoperativeplanning,provideviable alternativesandallowinappropriategraftstobeavoided.
Conflicts
of
interest
Theauthorsdeclarethattherewerenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KimSJ,JoSB,KimTW,ChangJH,ChoiHS,OhKS.Amodified arthroscopicanteriorcruciateligamentdouble-bundle reconstructiontechniquewithautogenousquadriceps tendongraft:remnant-preservingtechnique.ArchOrthop TraumaSurg.2009;129:403–7.
2.TsukadaH,IshibashiY,TsudaE,FukudaA,TohS.Anatomical analysisoftheanteriorcruciateligamentfemoralandtibial footprints.JOrthopSci.2008;13:122–9.
3.OdenstenM,GillquistJ.Functionalanatomyoftheanterior cruciateligamentandarationaleforreconstruction.JBone JointSurgAm.1985;67:257–62.
4.DienstM,BurksRT,GreisPE.Anatomyandbiomechanicsof theanteriorcruciateligament.OrthopClinNorthAm. 2002;33:605–20.
5.StaeubliHU,AdamO,BeckerW,BurgkartR.Anteriorcruciate ligamentandintercondylarnotchinthecoronaloblique plane:anatomycomplementedbymagneticresonance imagingincruciateligament-intactknees.Arthroscopy. 1999;15:349–59.
6.GirgisFG,MarshallJL,MonajemA.Thecruciateligamentsof thekneejoint.Anatomical,functionalandexperimental analysis.ClinOrthopRelatRes.1975;106:216–31. 7.DuthonVB,BareaC,AbrassartS,FaselJH,FritschyD,
MénétreyJ.Anatomyoftheanteriorcruciateligament.Knee SurgSportsTraumatolArthrosc.2006;14:204–13.
8.PetersenW,TillmannB.Anatomyandfunctionoftheanterior cruciateligament.Orthopade.2002;31:710–8.
9.JacobsonK.Osteoartritisfollowinginsufficiencyofthe cruciateligamentinman:aclinicalstudy.ActaOrthopScand. 1977;48:520–6.
10.WoodsGW,O’ConnorDP.Delayedanteriorcruciateligament reconstructioninadolescentswithopenphyses.AmJSports Med.2004;32:201–10.
11.ErikssonK,HambergP,JanssonE,LarssonH,ShalabiA, WredmarkT.Semitendinosusmuscleinanteriorcruciate ligamentsurgery:morphologyandfunction.Arthroscopy. 2001;17:808–17.
12.KartusJ,LindahlS,StenerS,ErikssonBI,KarlssonJ.Magnetic resonanceimagingofthepatellartendonafterharvestingits centralthird:acomparisonbetweentraditionaland subcutaneousharvestingtechniques.Arthroscopy. 1999;15:587–93.
13.HamadaM,ShinoK,MitsuokaT,AbeN,HoribeS. Cross-sectionalareameasurementofthesemitendinosus tendonforanteriorcruciateligamentreconstruction. Arthroscopy.1998;14:696–701.
14.MillerMD,NicholsT,ButlerCA.Patellafractureandproximal patellartendonrupturefollowingarthroscopicanterior cruciateligamentreconstruction.Arthroscopy.1999;15: 640–3.
15.MaedaA,ShinoK,HoribeS,NakataK,BuccafuscaG.Anterior cruciateligamentreconstructionwithmultistranded autogenoussemitendinosustendon.AmJSportsMed. 1996;24:504–9.
16.WerneckeG,HarrisIA,HouangMT,SeetoBG,ChenDB, MacDessiSJ.Usingmagneticresonanceimagingtopredict adequategraftdiametersforautologoushamstring double-bundleanteriorcruciateligamentreconstruction. Arthroscopy.2011;27:1055–9.
17.XieG,HuangfuX,ZhaoJ.Predictionofthegraftsizeof 4-strandedsemitendinosustendonand4-strandedgracilis tendonforanteriorcruciateligamentreconstruction:a ChineseHanpatientstudy.AmJSportsMed.2012;40:1161–6. 18.TumanJM,DiduchDR,RubinoLJ,BaumfeldJA,NguyenHS,
cruciateligamentreconstruction.AmJSportsMed. 2007;35:1945–9.
19.TremeG,DiduchDR,BillanteMJ,MillerMD,HartJM. Hamstringgraftsizeprediction:aprospectiveclinical evaluation.AmJSportsMed.2008;36:2204–9.Erratumin:AmJ SportsMed.2009;37(4):836.
20.ZantopT,PetersenW,SekiyaJK,MusahlV,FuFH.Anterior cruciateligamentanatomyandfunctionrelatingto anatomicalreconstruction.KneeSurgSportsTraumatol Arthrosc.2006;14:982–92.
21.BickelBA,FowlerTT,MowbrayJG,AdlerB,KlingeleK,Phillips G.Preoperativemagneticresonanceimagingcross-sectional areaforthemeasurementofhamstringautograftdiameter forreconstructionoftheadolescentanteriorcruciate ligament.Arthroscopy.2008;24:1336–41.