Abstract
Objective: To assess the bioavailability of a formulation of metformin hydrochloride 850 mg coated tablets as test, compared to a reference product with the same dosage form, in healthy volunteers of both genders.
Method: This clinical trial was designed as randomised, comparative, single-dose, open-label, two-period, two-sequence, crossover study under fasting conditions. 28 healthy volunteers (fourteen men and fourteen women) took part in the study. The 850 mg coated tablets formulations were administered in a single dose orally. Blood sam-ples were obtained prior to dosing and at 30 min, 1, 1:20; 1:40, 2, 2:20, 2:40; 3, 3:20, 3:40 4, 4:30, 5, 6, 8, 12, 16, 24 and 36 hours after drug administration with an one week washout period. Plasmatic concentrations of metformin were measured by specific and validated analytical methods based on high-performance liquid chromatography coupled to mass spectrometry (HPLC/MS). The pharmacokinetics pa-rameter AUC0-36h, AUC0-∞ and Cmax were tested for bioequivalence after log transformation of data and ratios of Tmax were evaluated non parametrically.
Findings: Data from this study showed that the test and the referen-ce formulation presented similar results, within the acreferen-ceptanreferen-ce range (80-125%) for AUC0-∞ (area under curve) and Cmax (maximum serum concentration of the drug) parameters, satisfying the bioequivalence criteria of the Brazilian Health Surveillance Agency and FDA.
Bioavailability of Different Formulations
of Metformin Hydrochloride in Healthy Volunteers:
a Comparative Study
ORIGINAL
Edilson Martins Rodrigues Neto1, Lídia Audrey Rocha Valadas Marques1, Gilmara Holanda da Cunha2, Andréa Vieira Pontes1, Patrícia Leal Dantas Lobo3, Gilberto de Nucci4, Manoel Odorico de Moraes Filho1, Maria Elisabete Amaral de Moraes1
1 Centre for Drug Research and Development, Federal University of Ceará (UFC), Fortaleza, CE, Brazil.
2 Department of Nursing, Federal University of Ceará (UFC), Fortaleza, CE, Brazil.
3 Dentistry Course, Campus Sobral, Federal University of Ceará (UFC), Sobral, CE, Brazil.
4 Department of Pharmacology, University of São Paulo (UFC), São Paulo, SP, Brazil.
Contact information:
Andréa Vieira Pontes.
Address: R. Cel. Nunes de Melo, 1000, Rodolfo Teófilo. Fortaleza, Brazil. CEP 60430-275.
Tel: +55 85 3366-8033
Introduction
Diabetes is a syndrome defined as a condition of heterogeneous metabolic disorder characterized by hyperglycemia resulting from defects in insulin se-cretion and action, or both. This chronic condition increases the risk of developing heart disease, cere-bral stroke and microvascular complications. There are frequent demonstrations of blindness, kidney failure and peripheral neuropathy. Currently, Type 2 Diabetes Mellitus (DM2) is a major public health diseases globally, having great impact on the eco-nomy of governments and individuals, as to their treatment, in addition to non-pharmacological mea-sures often becomes necessary the use of medica-tions [1].
Metformin is the drug of choice for the treatment of type 2 diabetes and is the most widely prescri-bed oral hypoglycemic agent due to its low toxicity profile and efficacy. The drug lowers blood glucose levels, especially leading to a decrease in hepatic gluconeogenesis, which leads to an average decrea-se in insulin levels, and also promotes glucodecrea-se up-take in muscle. Because of their anti-hyperglycemic properties and normalization of elevated levels of blood glucose, as well as DM2 is also used in poly-cystic ovary syndrome (PCOS) [2, 3].
Because of its widespread use and socio-eco-nomic difficulties of patients, they often choose by the use of generic drugs. Therefore, the refer-ence drugs and generics have in common the same active ingredient, but may differ from each other in relation to excipients and pharmaceutical pro-duction process. The Food and Drug
Administra-tion (FDA) and European Medicines Agency (EMA) regulations for generic drug product registration regulations require pharmacokinetic data obtained by comparative bioavailability trials between the formulation reference and test, analyzing the peak plasma concentration parameters (Cmax), area under the time curve from time 0 to time t (AUC0-t) and extrapolated to infinity (AUC0-∞). For the FDA, the test product should have a confidence interval (CI) of 90% in these three parameters, so that its ap-plication is met [2, 4].
Bioavailability studies have several functions, such as assessing the bioequivalence of drugs, evaluation of medicinal products with new active principles, evaluation of new formulations, evaluation of phar-maceutical forms of modified release, evaluation of medicinal products with more than one active in-gredient and assessment of change the regimen of a drug [4].
Therefore, we had up to evaluate the bioavail-ability of a 850mg metformin formulation coated tablet (test formulation) versus a 850mg metformin tablet formulation coated reference in the national market, to analyze the pharmacokinetic parameters of metformin formulations tested healthy fasting volunteers and inter-individual variability in relation to different organic groups, related to the gender.
Methods
Randomised, comparative, open-label, two-period, crossover study in which healthy subjets were given orally after a 8-hour overnight fast, in each distinct
Conclusion: These results indicate that the two formulations of metformin hydrochloride 850 mg coated tablets are bioequivalent, thus, it will be possible to ensure interchangeability between them, which can generate market competition and better access to this treatment.
Keywords
period, a single-dose of the test drug (Metformin 850mg) or the reference product (Glifage®) pro-duced by Merck S.A., according to the randomiza-tion plan.
This study was performed at the Clinical Pharma-cology Unit (UNIFAC) of the Federal University of Ceara and was conducted in accordance with the Declaration of Helsinki, and the protocol was appro-ved by the Ethics Committee of the Federal Univer-sity of Ceará, in Fortaleza, Brazil, with registration number 336.914. All subjects gave their written, informed consent and were free to withdraw from the trial at any time.
Subjects included in the study were considered healthy in the judgment of legally qualified profes-sionals, based on medical history, physical examina-tion and the hematological and biochemical labo-ratory tests prior to their enrollment. After a period of screening, 28 healthy volunteers (14 females and 14 males) who fulfilled the elegibility criteria were selected.
Inclusion criteria were: both genders, aged 18 to 50 years old, body mass index (BMI) between 18.5 and 28.7 kg/m2, good health conditions with no clinically significant diseases, ability to understand the nature and purpose of the study, including the risks and adverse effects, intention to cooperate with the researcher and act in accordance with the requirements of the entire clinical trial, which had to be confirmed by signing the informed consent form. Exclusion criteria were: diseases or health problems, addiction habits and pregnancy or breastfeeding.
Volunteers were informed that, with the excep-tion of oral contraceptives, no other drug could not be taken for at least four weeks prior to the study and until after its completion. They were also re-frained from ingesting alcohol, caffeine, chocolate, tea or coke containing beverages at least 12 hours before each dosing and until collection of the last blood sample.
The subjects received the drug Metformin Hy-drochloride 850 mg test and reference Metformin
Hydrochloride 850mg, for oral administration as a single dose, between 7:00 and 8:00 am, the day af-ter confinement in each period. Afaf-ter a minimum of eight hours fasting and evaluation of permanence in the inclusion and exclusion criteria, subjects received one of the formulations under study, having been recorded the absolute real-time medication.
Blood samples of 20 ml were collected for indi-vidual control curves patterns 10 ml for time zero through “venous line” heparin introduced in the surface of the volunteer’s forearm vein and other samples (7 ml) at the following intervals: 30 min, 1, 1:20; 1:40, 2, 2:20, 2:40; 3, 3:20, 3:40 4, 4:30, 5, 6, 8, 12, 16, 24 and 36 hours after the medication.
The blood samples were centrifuged at 3000 rpm for 12 minutes at 8°C. Immediately after cen-trifugation, plasma was removed (at least 1,0 ml) and stored in a suitable vial, also identified at the temperature -20°C freezer for storage in a specific biological samples located in the unit. The trans-port of samples to the analytical unit has occurred according to standard operating procedure for the transport of samples in the current driving period of the study.
Plasma concentrations of metformin were quanti-fied by a specific and validated bioanalytical method based on high-performance liquid chromatography with detection by mass spectrometry (HPLC-MS), and human plasma used as a biological matrix, for quantification pharmacokinetics.
(AUC0-∞) was done by adding the value C36/Ke to the calculated AUC0-36 where C36 is the met-formin plasma concentration at 36h and Ke is the first-order terminal elimination rate constant. The elimination half-life (t1/2) was derived from this rate constant (t1/2 = ln(2)/Ke) where t1/2 is the half-life time, ln(2) is the Neperian logarithm and Ke is the elimination rate constant.
Relative bioavailability between the reference and test formulations was assessed on the basis of maximum plasma concentration of metformin (Cmax) and area under the plasma concentration versus time curve from time 0 to the last sampling time (AUC0-36h) by calculating the mean ratios and 90% confidence interval (CIs) on log-transformed data. The inclusion of the 90% CIs for the ratios in the 80% to 125% bioequivalence interval, were analyzed using a parametric test (ANOVA). The exis-tence of residual effect was made based on ANOVA sequence tests, using the P value obtained based
on F_stat of the sequence effect as a parameter (Sequence Hypothesis of Model effects). The varia-bility between the groups (sequence), periods and formulations was evaluated using ANOVA test. The softwares used to calculate the pharmacokinetic pa-rameters (Cmax) and AUC) and to carry out statistical analysis were WinNonlinTM, version 5.0 (Pharsight, Mountain View, CA); and GraphPad Prim, version 3.02 (Software Inc., San Diego, CA).
Results
The age of the subjects varied between 18 and 39 years old, with an average of 28.5 years old. In as-sessing the body mass index there was observed a variation of 19,39 to 28,18 kg/m² with an average of 23,7kg/m². Seven volunteers had BMI above 25 are considered overweight, but were included in the study because they have reached the limit of 30 kg/ m² BMI. Table 1 presents means and quantitative variation of these tests in the selection of volunteers
(Table 1).
Tables 2 and 3 show the subjects’ pharmacoki-netic data accordingly to gender, for the test and reference formulations (Tables 2 and 3). The
maxi-Table 1. Laboratory parameters of the study volun-teers (N=28). Fortaleza, CE, 2015.
Clinical analyte reference value
Average value of the volunteers
The range of variation
of the volunteers
Renal function
Urea
mg/dL
21-53 25.28 16-49
Uric acid 4.0-8.4 4.93 2.5-6.9
Creatinine 0.6-1.2 0.753 0.55-1.08
Liver function
TGO
U/L
17-59 22.14 15-34
TGP 21-53 19.14 7-37
Alkaline
phosphatase 38-126 64.93 39-122
Albumine g/dL 3.5-5.0 4.58 4.1-5.2*
Total bilirubin mg/dL 0.1-1.2 0.73 0.22-2.4*
Metabolic evaluation
Glucose
mg/dL
70-99 82.4 68-98
Total
Cholesterol less than 239 161.25 117-232
Triglycerides less than 199 82.43 31-177
Blood evaluation
Red cells milions/
mL 4.2-6.5 4.75 4-5.2
Hemoglobine g/dL 12-18 13.93 12.1-15.6
Hematocrit (%) 37-54 41.41 37.1-45.6
Leukocytes u/mL 3000-11000 7500 4200-12000*
Canes
(%)
1-6 1 1-1
Segmented 40-63 54.93 41-78*
Eosinophils 1-6 2.82 01-07*
Basophils 0-3 0.43 0-1
Lymphocytes 20-45 31.93 14-43
Monocytes 2-10 9.25 05-15*
Platelets u/mL 130000-400000 271.000 170000-390000
Table 2. Pharmacokinetic parameters of subjects obtained after the administration of the reference for-mulation, divided by gender. Fortaleza, CE, 2015.
Cmax
(ng/mL) Tmax (h) t(1/2) (h) β (1 /h)
ASC (0- 36h) (h*ng/mL)
ASC (0-∞) (h*ng/mL)
Male
Mean 1,208.15 3.61 4.70 0.16 8,454.01 8,537.08
SD 224.43 0.66 1.87 0.05 1,356.06 1,350.49
Minimum 881.12 2.67 3.13 0.07 5,457.39 5521.35
Maximum 1,570.44 5.00 10.13 0.22 10,204.52 10,241.77
CV(%) 18.58 18.26 39.84 28.54 16.04 15.82
Geometric Mean 1,188.64 3.55 4.44 0.16 8,341.43 8,426.30
Female
Mean 1,341.82 3.69 6.38 0.12 9,876.52 10,004.48
SD 267.79 0.82 2.77 0.04 2,639.74 2,619.22
Minimum 1,046.29 2.33 3.11 0.05 5,419.43 5,830.07
Maximum 1,844.41 5.00 14.00 0.22 14,808.71 14,949.10
CV(%) 19.96 22.12 43.43 35.66 26.73 26.18
Geometric Mean 1,317.94 3.60 5.93 0.12 9,548.31 9,692.09
Table 3. Pharmacokinetic parameters of subjects obtained after the administration of the test formulation, divided by gender. Fortaleza, CE, 2015. Fortaleza, CE, 2015..
Cmax
(ng/mL) Tmax (h) t(1/2) (h) β (1/h)
ASC (0- 36h) (h*ng/mL)
ASC (0-∞) (h*ng/mL)
Male
Mean 1372.57 3.69 5.61 0.13 9857.54 9968.19
SD 212.13 0.80 1.39 0.03 1995.31 2009.72
Minimum 974.07 2.67 4.13 0.08 6728.08 6823.33
Maximum 1817.70 5.00 8.36 0.17 14751.31 14913.65
CV(%) 15.45 21.60 24.68 22.35 20.24 20.16
Geometric Mean 1357.40 3.61 5.47 0.13 9677.14 9787.24
Female
Mean 1341.82 3.69 6.38 0.12 9876.52 10004.48
SD 267.79 0.82 2.77 0.04 2639.74 2619.22
Minimum 1046.29 2.33 3.11 0.05 5419.43 5830.07
Maximum 1844.41 5.00 14.00 0.22 14808.71 14949.10
CV(%) 19.96 22.12 43.43 35.66 26.73 26.18
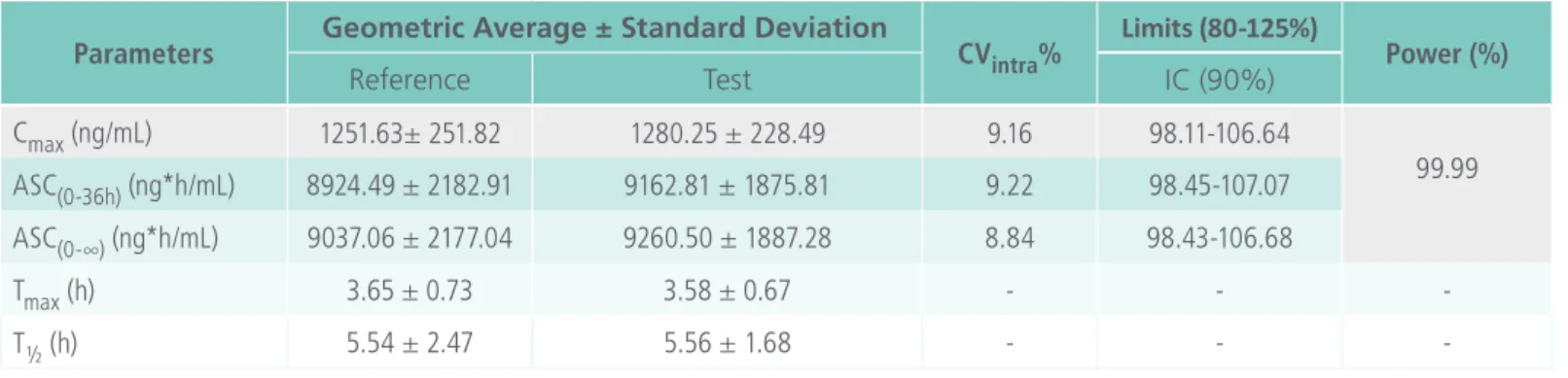
Table 4. Comparative statistical analysis of pharmacokinetic parameters between the two formulations (test and reference). Fortaleza, CE, 2015.
Parameters Geometric Average ± Standard Deviation CVintra% Limits (80-125%) Power (%)
Reference Test IC (90%)
Cmax (ng/mL) 1251.63± 251.82 1280.25 ± 228.49 9.16 98.11-106.64
99.99
ASC(0-36h) (ng*h/mL) 8924.49 ± 2182.91 9162.81 ± 1875.81 9.22 98.45-107.07
ASC(0-∞) (ng*h/mL) 9037.06 ± 2177.04 9260.50 ± 1887.28 8.84 98.43-106.68
Tmax (h) 3.65 ± 0.73 3.58 ± 0.67 - -
-T½ (h) 5.54 ± 2.47 5.56 ± 1.68 - -
-Table 5. Adverse events observed during the study. Fortaleza, CE, 2015.
Subject Adverse Event Intensity Causality Duration Treatment
9 Headache Low Not Related 8 hours Acetaminophen oral, a pill, 750 mg
14 Nausea and vomit Low Related 40 minutes Bromopride, oral, a pill, 10 mg
17 Vomit Low Possible 20 minutes Observation
18 Diarrhea Low Possible 1 hour Observation
Headache Remote
19 Diarrhea Low Possible 20 minutes Observation
Dor abdominal Moderate
20 Nausea and vomit Low Not Related 10 minutes Observation
21 Nausea and vomit Low Possible 40 minutes Bromopride, oral, one pill, 10 mg
22 Headache Low Remote 1 hour Dipyrone, oral, 30 drops, 500 mg/mL
24
Nausea Low Possible 1 hour
Observation Abdominal pain Moderate Possible
15 minutes
Diarrhea Low Possible
26 Abdominal pain Moderate Possible 20 minutes Observation
Diarrhea Low Possible
27 Nausea Low Possible 1 hour Observation
28 Headache Low Remote 1 hour Observation
mum concentrations (1274.99 and 1302.16 ng/mL for reference and testing respectively) and minimal concentrations (13.42 and 12.8 ng/mL) parameters were remarkably similar, confirming a similar disso-lution profile between the formulations and absorp-tion of drugs.
When analyzing the Cmax, AUC0-36h and AUC0-∞ parameters at Table 4, it is noticeable that the
variation is within the standard limits (80-125%), considering a confidence interval of 90%. It was also shown that both formulations had similar geo-metric means for the same parameters.
situations where the investigator prescribed medica-tion to treat the event, which was limited to the use of antiemetics and analgesics. The reported events were mostly gastrointestinal disturbances (nausea, vomiting and diarrhea), possibly related to the study drug, and headaches, unrelated or remotely related to the drug. Only one event (subject 14) was related to the study drug by the investigator (Table 5).
Discussion
This study supports strong similarity between test and reference formulations in the obtained pharma-cokinetic parameters, which are within the specified limits by the regulatory agency. The AUC0-∞ is an important pharmacokinetic parameter that numeri-cally describes the drug bioavailability, with the aim of quantifying the absorbed fraction that reached the systemic circulation and becomes available to exert its pharmacological effect. In this study are found mean values of 9270.78 and 9440.71 hr*ng/ mL for the test and reference formulation respec-tively.
In a study that investigated the pharmacokinetics of metformin hydrochloride tablets 850 mg in six nondiabetic volunteers it was found a mean AUC of 8900 h*ng/mL, similar to the data obtained in this study [5]. Another study found a mean of 15620 h*ng/ mL, following the administration of two tablets of the reference product of 500 mg in 12 healthy male volunteers. This elevated concentration was found probably due to the administration of a higher dose of 1000 mg [6].
Regarding the Cmax, this study found a mean re-sult of 1274.99 and 1299.80 ng/mL for the referen-ce and test formulations respectively, reached at the mean times (Tmax) of 3.65 and 3.58 hours after the drug administration. The metformin half-lives of the two analysed formulations was of 5.54 (reference) and 5.56 hours (test).
Another study found a mean value of 1.7 mg/l for Cmax, higher than the two tested formulations
in this study [5]. Tmax had a mean time of 3 hours, which means that concentration peak was reached before both of our studied formulations. The half-life of metformin in this formulation was of 2.7 hours, a value much lower than those obtained in our research. In both studies the formulations were administered under fasting conditions.
A similar result was described in another research, wherein mean values for Cmax of 1.73 and 1.86 mi-crog/ml were reported, being achieved at 2.6 and 2 hours for the test formulation and reference, res-pectively. It was also observed Cmax values higher than in this study, as well as an earlier concentration peak. The half-lives of both formulations were lower than 3.1 hours [7].
After the administration of a 1000mg dose, another study reported mean values for Cmax of 2.385 g/ml reached at the mean time of 2.72 hours and an elimination half-life of 2.8 hours [6]. A half life of 3.8 hours was found after the administration of Metformin hydrochloride 850 mg tablets to 24 healthy volunteers [8].
Regarding the elevated mean values of the elimi-nation half-life in our tested formulations, it is inter-esting to note that it may be beneficial, compared with other formulations. Considering that the DM2 is a chronic and sometimes difficult to control disea-se, a metformin formulation that enables a greater drug residence time in the body can be useful for glucose control in diabetic patients.
which the drug acts in its molecular target modu-lating the physiological response [2].
The differences found between the tested formu-lations and the cited references can be explained by several factors, including: different formulations, population genetic factors and gender differences. In this study, we found significant differences in the pharmacokinetic parameters between the genders. Female subjects had a mean Cmax) of 1341.82 and 1372.57 g/mL for the reference and test formula-tion, respectively, while the male subjects had means of 1208.15 and 1144.67. These differences proba-bly are due to less intense metabolism of women, which generates a reduced drug clearance when compared to man [9].
Data from the AUC0-∞ parameter corroborates this information, showing once again superior phar-macokinetic mean values in women for test and reference formulations (10004.5 e 9938.15 h*ng/ mL) than in men (8537.08 e 8828.17 h*ng/mL). Re-nal excretion is also a very important factor to be considered in differences between genders, since it is known that women have a lower renal elimina-tion rate than men, which can be correlated well with expression of dose-dependent adverse events [10]. These pharmacokinetic differences between genders could be explored, since one of the cli-nical indications of Metformin is the treatment of polycystic ovary syndrome, a female condition with constant and prolonged treatment [11].
Regarding the adverse events, seventeen were reported during our study, mostly of mild intensity, only three moderate. Eleven events were classified as having a possible relationship with metformin, mainly gastrointestinal reactions. Twelve subjects presented at least one event during the study, only two of them were male. Four subjects had to be medicated for the presented reactions, being pres-cribed analgesics (paracetamol and dipyrone) and antiemetic agents (bromopride).
Literature references describe that the most com-mon side effects of metformin are gastrointestinal
reactions, especially nausea, vomiting, abdominal discomfort, cramps and indigestion. These effects are presented in about 10 to 25% of patients, es-pecially in early treatment. These effects can be re-duced if therapy starts with a low dose, gradually increasing, and tend to disappear with continued treatment [2].
Three subjects had headache complaints that can be correlated with abstinence from caffeine and other xanthines [12], which are prohibited substan-ces during the study period, as it could possibly alter the pharmacokinetics of the tested formulations, as they are metabolism inductors of several drugs [13].
Formulations containing metformin were well to-lerated, although there was an elevated incidence of adverse events in female subjects. The obtained data are consistent with the literature. It is described that the metabolism and disposition of drugs in wo-men can occur slowly than in man, due to metabolic (hepatic microsomal system) and physiological diffe-rences (renal clearance rates). Thus, females have a higher drug concentration peak that can lead to the increased incidence of adverse effects through a dose-dependent mechanism [10].
Conclusion
References
1. Ashcroft FM, Rorsman P. Diabetes mellitus and the beta cell: the last ten years. Cell. 2012;148:1160-71. Available from: http:// dx.doi.org/10.1016/j.cell.2012.02.010
2. Rodrigues Neto EM, Marques LARV, Ferreira MAD, Lobo PLD, Girão Júnior FJ, Camarão GC, et al. Metformina: uma revisão da literatura. Saúde e Pesquisa. 2015;8:355-62. Available from: http://dx.doi.org/10.17765/1983-1870.2015v8n2p355-362
3. Alexander GC, Sehgal NL, Moloney RM, Stafford RS. National trends in treatment of type 2 diabetes mellitus, 1994-2007. Arch Intern Med. 2008;168:2088-94. Available from: https:// dx.doi.org/10.1001%2Farchinte.168.19.2088
4. Van Der Meersch A, Dechartres A, Ravaud P. Quality of reporting of bioequivalence trials comparing generic to brand name drugs: a methodological systematic review. PLoS ONE. 2011; 6:e23611. Available from: http://dx.doi.org/10.1371/journal.pone.0023611
5. Robert F, Fendri S, Hary L, Lacroix C, Andréjak M, Lalau JD. Kinetics of plasma and erythrocyte metformin after acute administration in healthy subjects. Diabetes Metab. 2003; 29:279-83. Available from: http://www.em-consulte.com/en/ article/80210
6. Hu LD, Liu Y, Tang X, Zhang Q. Preparation and in vitro/in vivo evaluation of sustained-release metformin hydrochloride pellets. Eur J Pharm Biopharm. 2006; 64:185-92. Available from: http:// dx.doi.org/10.1016/j.ejpb.2006.04.004
7. Al Hawari S, AlGaai E, Yusuf A, Abdelgaleel A, Hammami MM. Bioequivalence study of two metformin formulations. Arzneimittelforschung. 2007; 57:192-5. Available from: http:// dx.doi.org/10.1055/s-0031-1296605
8. Porta V, Schramm SG, Kano KE, Koono EE, Armando YP, Fukuda K, Serra CHR. HPLC-UV determination of metformin in human plasma for application in pharmacokinetics and bioequivalence studies. J Pharm Biomed Anal. 2008; 46:143-7. Available from: http://dx.doi.org/10.1016/j.jpba.2007.10.007
9. Souza FC, Marques EB, Scaramello CBV. Variações interindividuais na farmacocinética clínica de cardiotônicos. Rev Bras Cardiol. 2013; 26:213-20. Available from: http://www.rbconline.org.br/ artigo/variacoes-interindividuais-na-farmacocinetica-clinica-de-cardiotonicos/
10. Costa VM, Bastos ML, Carvalho F. Género masculino vs feminino: factor relevante para as respostas farmacológicas e efeitos adversos de fármacos? Acta Farmacêutica Portuguesa. 2011; 1:55-64. Available from: http://www.actafarmaceuticaportuguesa. com/index.php/afp/article/view/32
11. Motta ELA, Domingues TS, Soares Júnior JM. O uso de sensibilizadores de insulina no tratamento de infertilidade em pacientes com síndrome dos ovários policísticos (SOP). Rev Bras Ginecol Obstet, 2012; 34:99-101. Available from: http://dx.doi. org/10.1590/S0100-72032012000300001
12.Campo-Arias A, Herazo YE. Cefalea como síntoma de abstinencia a la cafeína: un estudio poblacional. Rev. fac. med. 2008; 16:176-83. Available from: http://www. scielo.org.co/scielo.php?script=sci _ ar ttex t&pid=S0121-52562008000200005&lng=en
13. Cruzado L, Sánchez-fernández M, Cortez-Vergara C, Rojas-Rojas G. Manía inducida por bebidas energéticas con alto contenido de cafeína. Actas Esp Psiquiatr. 2014; 42:259-66. Available from: http://actaspsiquiatria.es/repositorio/16/91/ESP/16-91-ESP-259-262-556333.pdf
International Archives of Medicine is an open access journal publishing articles encompassing all aspects of medical scien-ce and clinical practiscien-ce. IAM is considered a megajournal with independent sections on all areas of medicine. IAM is a really international journal with authors and board members from all around the world. The journal is widely indexed and classified Q2 in category Medicine.