BrazJOtorhinolaryngol.2014;80(4):346---353
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
REVIEW
ARTICLE
Overview
of
newborn
hearing
screening
programs
in
Brazilian
maternity
hospitals
夽
Hannalice
Gottschalck
Cavalcanti
a,∗,
Luciana
Pimentel
Fernandes
de
Melo
a,
Laisa
Flávia
Soares
Fernandes
Peixoto
Buarque
a,
Ricardo
Oliveira
Guerra
baDepartmentofPhonoaudiology,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil bDepartmentofPhysicalTherapy,UniversidadeFederaldoRioGrandedoNorte(UFRN),Natal,RN,Brazil
Received4June2013;accepted30October2013
Availableonline23May2014
KEYWORDS
Neonatalscreening; Hearingloss; Hearing
Abstract
Introduction:Newbornhearingscreeninghasasitsmainobjectivetheearlyidentificationof
hearinglossinnewbornsandinfants.Inordertoguaranteegoodresults,qualityindicatorsfor newbornhearingscreeningprogramsareusedasbenchmarks.
Objective:Toobserveanddescribetherealityofnationalnewbornhearingscreeningprograms
inBrazil,andtoevaluateiftheycanbereferredtoashavingqualityindicators.
Methods:Integrative literature review in databases such as MEDLINE, LILACS, SciELO, and
Google.
Results:22articleswereanalyzedinrelationtonewbornhearingscreeningcoverage,theplace
andperiod newborn hearing screeningwas performed,initial results,referraltodiagnostic procedures,losstofollow-up,andoccurrenceofhearingloss.
Conclusion:Transientotoacousticemissionswerethemostoftenusedscreeningmethodology.
Coveragevariedwidely,andonlyafewmaternitywardsachieved95%ofthecasesscreened. Referraltodiagnosticprocedures wasunder4%,butlackofadherencecanbeconsidereda barriertosuccessfulfollow-up.Theoccurrenceofhearinglossrangedfrom0%to1.09%.The involvementofgovernment,physicians,andsocietyisnecessary,sothatthegoalsofnewborn hearingscreeningcanbeachieved.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:CavalcantiHG,deMeloLP,BuarqueLF,GuerraRO. Overviewofnewborn hearingscreeningprograms in Brazilianmaternityhospitals.BrazJOtorhinolaryngol.2014;80:346---53.
∗Correspondingauthor.
E-mail:[email protected](H.G.Cavalcanti). http://dx.doi.org/10.1016/j.bjorl.2014.05.005
Overviewofnewbornhearingscreeningprograms 347
PALAVRAS-CHAVE
Triagemneonatal; Perdaauditiva; Audic¸ão
Panoramadosprogramasdetriagemauditivaneonatalemmaternidadesbrasileiras
Resumo
Introduc¸ão: a triagem auditiva neonatal (TAN) tem por finalidade a identificac¸ão, o mais
precoce possível, da deficiênciaauditiva em neonatos e lactentes. Paragarantir a eficácia e eficiênciadestes programas os índicesdequalidade em relac¸ão àtriagem,diagnóstico e intervenc¸ãoservemcomoorientac¸ãoeguia.
Objetivo: Conheceredescreverarealidadenacionaldosservic¸osdeTANnoBrasil,eavaliarse
osmesmospodemserconsideradoscomodetentoresdeindicac¸ãodequalidade.
Método: RevisãointegrativadaliteraturaembasescomoMedline,Lilacs,ScieloeGoogle.
Resultados: No total, 22 artigosforam analisados para esta revisão, referente à cobertura
da triagem auditivaneonatal, o local e período ondeaTAN foi realizada,resultados inici-ais,encaminhamentosparadiagnóstico,taxadeabandonodoprogramaeocorrênciadeperda auditiva.
Conclusão:Emissõesotoacústicastransientesfoiométododetriagemmaisutilizado.A
cober-turadaTANvarioumuitoepoucasmaternidadesatingiramamarcados95%.Oencaminhamento paradiagnósticoficouabaixodos4%,porémanãoadesãoaoprogramapodeserconsideradauma barreiraparaosucesso.Aocorrênciadeperdaauditivavariouentre0%---1.09%.Énecessárioum maiorenvolvimentodospolíticos,equipeshospitalaresedasociedadeparaatingirosobjetivos daTAN.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Hearing loss impacts onthe capacity tocommunicate, as well ason thesocial, emotional, and economic condition (lower education) of the individual; therefore, preven-tion is one of the strategies proposed to reduce this impact.
Inthiscontext,thenewbornhearingscreening(NHS)aims toidentify,asearlyaspossible,hearinglossinnewbornsand infants.Itassessesauditory functionthroughphysiological and electrophysiological measures of hearing. The goal is thereferralofinfantsatriskfordevelopinghearinglossto audiologicaldiagnosis,sothatinterventioncanbeinitiated asearlyaspossible.Therefore,thisprocessshouldbepartof theactionsthatcomprisecomprehensivehearinghealthcare duringchildhood.1
In some countries, NHS is an important tool for early detectionofhearinglossand,therefore,theeffectiveness and efficiency of these programsshould be analyzed and guaranteed.
Guidelines that outline recommendations and define quality measures as a method to evaluate the results of theseprogramshavebeencreated.Theyaretheso-called qualityindicators,whichrecommendthatthescopeof hear-ingscreening shouldbeconsidereduniversal, thatitmust assessatleast95%ofnewborns,andthatNHSshouldbe per-formedwithinthefirstmonthoflife.Theyalsorecommend referralofamaximumof4%ofbabiesscreenedfor diagno-sis;diagnosisattendanceofatleast90%ofreferredbabies andfollow-upatamaximumofthreemonthslater;diagnosis ofpermanentcongenitalhearinglossin1%---3%ofnewborns; and use of hearingaid onemonth afterattaining diagno-sis, with rehabilitation starting at 6 months of life. The screeningshouldpreferablybeperformedinthematernity
ward,beforehospitaldischarge,andshouldbeorganizedin twosteps(testandretest).2,3
In Brazil, there are 267 hearing screening services in 30 cities and 13 Brazilian states,4 figures considered low
for a country that currently occupies the fifth position in the world in terms of size and population; these ser-vices represent approximately 10% of neonates screened in the country.5 It seems that, unlike many developed
countries,universalNHSremainsachallengefor Brazil,as thesocioeconomicsituationandresource availabilityvary considerablyfromoneregiontoanother.
Studies indicate a prevalence of severe/profound con-genitalsensorineuralhearinglossof0.5---5/1000newborns, which is higher in developing countries5,6 and thus, early
diagnosis is of utmost importance for the appropriate communicationdevelopment.Consideringthefew epidemi-ological studies that describe the NHS programs and the diagnosisofhearinglossinBrazil,itisnecessarytoperform areviewofpublicationsontheoccurrenceofhearingloss ininfantsinBrazil. Thepurposeofthisreview,therefore, wastoanalyzeanddescribethenationalrealityofNHS ser-vicesinBrazil,andassesswhethertheycanbeconsidered ashavingqualityindication.Theoccurrenceofhearingloss, diagnosedbytheNHS,wasinvestigated.
Methods
348 CavalcantiHGetal.
used:MEDLINE,LILACS,SciELO,GoogleScholar,andthesis databasesofmajoruniversities.
The subject descriptors (DeCS) used were related to the intervention (neonatal screening, hearing screening, newborn) and the outcome (hearing, hearing loss, hear-ing disorder) in all possible combinations associated with theword‘‘Brazil’’.AllperiodsuntilFebruaryof2013were included,withnorestrictionsregardinglanguageof publi-cation.
To ensure that the most studies would be identified, journals and abstracts of the congresses of the Brazilian AcademyofAudiology,theBrazilianSocietyofSpeech Ther-apy, and the Brazilian Association of Otolaryngology and HeadandNeckSurgerybetween2008and2012,andofthe BrazilianSocietyofPediatricsbetween2006and2011were manuallyresearched.Thesedateswereselectedduetothe availabilityofonlineabstracts.Subsequently,thetitlesand abstractsofarticleswerereadbytworeviewers, indepen-dently.Thosethatconformedtotheinclusionandexclusion criteriawereselected. Afterthe selection, the reviewers mettoagreeupontheinclusionorexclusionofarticles.A manualsearchforreferenceswasalsoperformed.
The inclusion criteria used to describe NHS programs were: (a) population of neonates born in public or pri-vate maternity hospitals submitted to hearing screening withelectrophysiological measurements(transient evoked otoacoustic emissions [TEOAE] and/or distortion-product otoacoustic emissions [DPOAE] or/and brainstem auditory evokedpotential[BAEP]);(b)operationofhearingscreening programs for at least five months to avoid inconsistent resultsthatmayoccurduringtheinitialoperationofthese programs.8 The NHS must have been carried out in the
maternityhospitalandbeforedischarge;(c)descriptionof thehearingscreeningprocess;rateofscreeningsperformed inrelation tothenumberof babiesbornin thematernity hospital,thenumberof babieswhowereunabletoattain satisfactory results in the firstevaluation, the number of neonatesreferredtoretest,diagnosisanddescriptionofthe numberof thosethat did notcomplete the first phaseof hearingscreening,andpercentageofhearinglossfound.
Studies referring toaspecific subpopulationandlower qualitystudies (inconsistent data or confusing discussion) wereexcluded.
Descriptive studies were evaluated, as the purpose of thisreview wastoassessthe qualityof NHSservices per-formedinhospitalsinBrazilandthedescriptionofhearing lossprevalenceasaresultofNHS.
The presentation of the data is limited to descriptive informationand a narrative summary, due to the hetero-geneityofthearticles.The descriptionoftheNHSandits results andthe prevalence of hearing loss found in these studieswereselectedasoutcomes.
Results
Based on the search criteria, 195 citations were found, includingarticles,congress abstracts,masters degree dis-sertations,and doctoral theses. Of this total, 63 articles wereduplicatesandwereexcluded.Oftheremaining132 articles,thetitleand abstractwereread, and78articles
were readin full. Atotal of22 metthe inclusioncriteria andwereanalyzedforthisreview.9---34
When searching for studies describing NHS pro-grams in languages other than Portuguese, three arti-cles and one summary in English,16,23,27,34 13 abstracts
presented at congresses,10,16,17,19---22,24,27,30,31,33,34 and two
dissertations11,26werefound.
Newbornsthatdidnothavea satisfactoryperformance in the initial hearing screening are referred for retesting withinsevento30days.Ifthereisnoimprovementinthe electrophysiologicalresponses,theyarereferredto audio-logicaldiagnosis, whichevaluatesthemthroughbrainstem auditory evoked potential (BAEP), audiometric tests with visualreinforcement,andassessmentofmiddleearstatus. Mostservicesuseatwo-phaseprotocol:thefirstphaseisthe initialhearingscreeningandthesecond,theretest.Babies who donot have risk indicators for hearing loss and per-formed well inthe initialscreening aredischarged.Ifthe neonatehasa riskindicator forhearingloss, evenaftera goodperformance in thehearing screening,the babywill bereferredforhearingfollow-up.
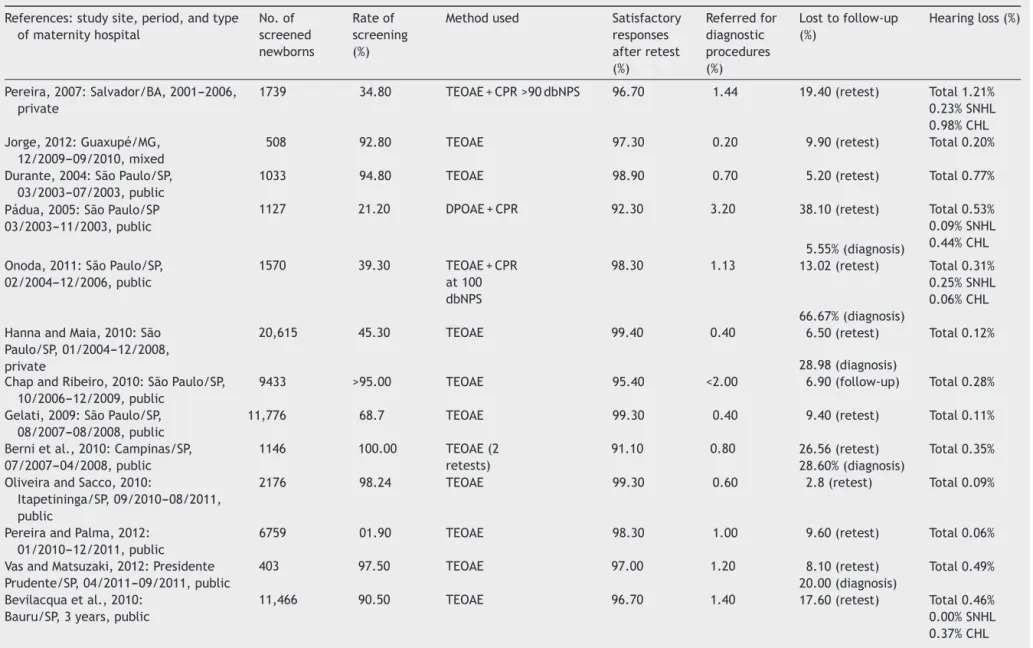
Table1 shows a summarized description of all articles inrelation tocities, maternityhospitalsinwhichNHSwas described,theperiodofstudyperformanceandresults,NHS rates, thefinaloutcomeof thefirstphase,the numberof newborns whodidnotattendretesting/diagnosis, andthe percentageofbabiesreferredforaudiologicaldiagnosiswho demonstratedhearingloss.
Discussion
All hearing health programs should be analyzed in rela-tiontotheircost---benefitratio.Frequently,thedifficulties facedfortheirimplementationarenotfinancialor techno-logical.The lackofinfrastructureandsupportservicesfor family members,lack of qualitycontrol services and uni-fiedprotocols,follow-updifficulties,andhighcostsmaybe responsible for frequent poor outcomes.9 An appropriate
follow-up startedat themomentofthehearing screening procedure, progressingthroughtheaudiologicaldiagnosis, andtherebyallowinganinterventiontobeimplementedas earlyaspossibleisessentialforaneffectiveNHSprogram.35
TheUnitedStateswasthefirstcountrytoperformNHS, subsequentlyfollowedbymanyothercountries.Theinitial proposalintendedtodetecthearinglossinnewbornsatrisk, butexpanded totheearlyidentification ofhearingloss in all newborns.36 According tothestandards established by
JCIHandCOMUSA,1,2 foranNHSprogramtobeconsidered
universal,itmustreach,sixmonthsafteritsimplantation, a minimum of 95% of infants assessed during postpartum admission,orbeforeonemonthoflife.
Thisintegrativereviewincludedpublicationsrelatingto NHSprogramsinBrazilthatindicatetherates ofscreened newborns,resultsofNHSinthematernityhospitals, refer-ralsfordiagnosis, prevalenceofhearingloss, anddropout ratesatthefollow-up.
Therateofscreenednewbornsinthisreviewvaried sig-nificantly between studies, and only nine reached a 95% rate.16,18---20,22,24,29,32,34Privatehospitalsshowedlowerrates,
Overview
of
newborn
hearing
screening
programs
349
Table1 DescriptionoftheNHSinrelationtothetypeofmaternityhospital,city/town,timeperiod,percentageofbabiesscreenedinrelationtonumberoflivebirthsinthe sameperiod,resultofNHSafterthefirstphase,percentageofinfantsreferredfordiagnosticproceduresinrelationtothetotalscreenedinfants,percentageofbabiesthat lefttheprogramatsomestage,andpercentageofhearinglossinrelationtothetotalnumberofscreenedbabies.
References:studysite,period,andtype ofmaternityhospital
No.of screened newborns
Rateof screening (%)
Methodused Satisfactory responses afterretest (%)
Referredfor diagnostic procedures (%)
Losttofollow-up (%)
Hearingloss(%)
Pereira,2007:Salvador/BA,2001---2006, private
1739 34.80 TEOAE+CPR>90dbNPS 96.70 1.44 19.40(retest) Total1.21% 0.23%SNHL 0.98%CHL Jorge,2012:Guaxupé/MG,
12/2009---09/2010,mixed
508 92.80 TEOAE 97.30 0.20 9.90(retest) Total0.20% Durante,2004:SãoPaulo/SP,
03/2003---07/2003,public
1033 94.80 TEOAE 98.90 0.70 5.20(retest) Total0.77% Pádua,2005:SãoPaulo/SP
03/2003---11/2003,public
1127 21.20 DPOAE+CPR 92.30 3.20 38.10(retest) Total0.53% 0.09%SNHL 0.44%CHL 5.55%(diagnosis)
Onoda,2011:SãoPaulo/SP, 02/2004---12/2006,public
1570 39.30 TEOAE+CPR at100 dbNPS
98.30 1.13 13.02(retest) Total0.31% 0.25%SNHL 0.06%CHL 66.67%(diagnosis)
HannaandMaia,2010:São Paulo/SP,01/2004---12/2008, private
20,615 45.30 TEOAE 99.40 0.40 6.50(retest) Total0.12% 28.98(diagnosis)
ChapandRibeiro,2010:SãoPaulo/SP, 10/2006---12/2009,public
9433 >95.00 TEOAE 95.40 <2.00 6.90(follow-up) Total0.28% Gelati,2009:SãoPaulo/SP,
08/2007---08/2008,public
11,776 68.7 TEOAE 99.30 0.40 9.40(retest) Total0.11% Bernietal.,2010:Campinas/SP,
07/2007---04/2008,public
1146 100.00 TEOAE(2 retests)
91.10 0.80 26.56(retest) Total0.35% 28.60%(diagnosis)
OliveiraandSacco,2010:
Itapetininga/SP,09/2010---08/2011, public
2176 98.24 TEOAE 99.30 0.60 2.8(retest) Total0.09%
PereiraandPalma,2012: 01/2010---12/2011,public
6759 01.90 TEOAE 98.30 1.00 9.60(retest) Total0.06% VasandMatsuzaki,2012:Presidente
Prudente/SP,04/2011---09/2011,public
403 97.50 TEOAE 97.00 1.20 8.10(retest) Total0.49% 20.00(diagnosis)
Bevilacquaetal.,2010: Bauru/SP,3years,public
350
Cavalcanti
HG
et
al.
Table1(Continued)
References:studysite,period,andtype ofmaternityhospital
No.of screened newborns
Rateof screening (%)
Methodused Satisfactory responses afterretest (%)
Referredfor diagnostic procedures (%)
Losttofollow-up (%)
Hearingloss(%)
4.20(diagnosis) Almeida,2009:SãoJosédos
Campos/SP,04/2007---12/2008, private
1541 100.00 TEOAE 98.70 0.20 34.70(retest) Notpossible
100.00(diagnosis) Barreira-Nielsen,2007:Vila
VelhaandVitória/ES, 2002---2005,public
4951 68.0 TEOAE+CPR at90dbNPS
94.60 0.50 46.30(retest) Total0.28% 0.20%SNHL 0.08%CHL 47.40(diagnosis)
Maggi,2009:SantaMaria/RS, 04/2007---03/2008,public
1198 66.56 TEOAE+CPR 97.00 1.40 17.65(retest) Total0.67% BoscattoandMachado,2012:Passo
Fundo/RS,07/2007---07/2010,public
5045 70.50 TEOAE(2 retests)
91.90 0.03 50.40(retest) Total0.04% 60.00(diagnosis)
Faistauer,2012:Canoas/RS, 10/2009---09/2010,public
2165 100.00 TEOAE 95.20 0.50 24.00(retest) Total0.2% 16.00(diagnosis)
NascimentoandNarciso,noyear: Maringá/PR,10/2003---09/2004 private
690 29.75 DPOAE 99.10 0.00 28.80(follow-up) Babywasnot assessed Mello,2011:Maringá/PR,2007---2008,
public
908 80.70 TEOAE+CPR 89.60 1.10 24.7(retest) Total0.44% 0.11%SNHL 0.33%CHL Mattosetal.,2011:Florianópolis/SC,
03/2005---08/2005,public
765 95.20 TEOAE+CPR
Tympanometryatretest
96.10 2.00 14.00(follow-up) Total0.32% Pinheiro,2009:Florianópolis/SC,2006,
public
1416 93.50 TEOAE+CPR
Tympanometryatretest
86.90 1.90 27.60(retest) Total0.28%
Overviewofnewbornhearingscreeningprograms 351
whorequesttheoptionalNHSservice.9Theprivate
mater-nityhospitalthathadgreatestsuccessinthescreeningrate wasexclusivefor treatmentofinsuredpregnantwomen.24
Thelackof95%coverageobservedinstudiesofpublic hos-pitals iscaused by earlydischarge anda smallnumberof audiologistsemployedtoperformthehearingscreeningin thesehospitals,makingitimpossibletoassesshearingduring atalltimes.16,17,21---24
The methodology used for the NHS was assessment through TEOAE,11,12,16---18,20---29,31---33 and DPOAE to a lesser
extent.30 Reducedcosts, betterobjectivity, andless
inva-siveness surely contributed to the preference for this method, compared to the use of BAEP, which evaluates the electrophysiological conduction of auditory stimuli to theperipheral portionof the brainstem.4 Somematernity
hospitals have added the cochlea palpebral reflex (CPR), throughtheuseofsingleormultiple bellsintheNHS,but thereisnoconsensusontheintensitytobeusedtoelicit such reflex.9,10,13,14,25,26,31---33 The protocols differ broadly
regardingthe typeandmodel ofequipmentused,aswell asthefollow-upcriteriaandprotocols.
MoststudiesshowedsatisfactoryNHSresponsesafterthe secondphaseofretesting,withmorethan96%successrate. Thelowestrateinthetwostudies31,33 canbeattributedto
unfavorableenvironmentalconditionsortotheinexperience oftheNHSaudiologisttoproperlyperformtheassessment.5
The percentageofinfantsreferred fordiagnosis remained below4%,whichistherecommendedrateandanindicator ofscreeningquality.
Theratesdescribingthelackoffeedbackforretestvaried between5%and50%inpublichospitalsandbetween9%and 34%intheprivateandmixedhospitals.Thelackof adher-encefordiagnosisshowedhighrates,between5%and66% inpublichospitalsandbetween28%and100%intheprivate andmixedhospitals;theyarenoteworthy, asthe diagnos-ticfollow-upshowedloweradherencecomparedtoretest, perhaps becauseitis beperformed outside ofthe mater-nityhospital.ThecitiesinthecountrysideoftheSoutheast clearlyshowedhigherdiagnosisadherencerates;one expla-nationwouldbethathospitalsinsmallercitiesfacilitatethe organizationof NHS programs.São Paulo wasthe pioneer cityintheimplementationofNHS,andtheinitial discuss-ionsforimprovingthestructureoftheNHSprogramshave beendevelopedforalongerperiodoftime.37
The WorldHealthOrganization hasidentifiedsome key elements for the effectiveness of NHS programs. They includeprovidinginformationtoparents,physicians, audi-ologists, politicians, and educators about the importance of hearing and the consequences of a late diagnosis, the developmentof anNHSscreeningandfollow-upsystemat allstages,andfamilycenteredsupport.5
The present review found a proportion of hearing loss that ranged from 0% to 1.09%. This result differs from ratesfoundinotherstudiesindevelopingcountries,which reportedpercentagesofhearinglossbetween1%and53%.36
TheNHSwasimplementedinsomehospitalsandregionsin LatinAmerica,buttherearenoprogramsatanationallevel inthecountriesfromthisregion.37
Thelackofsystematizationinthecollectionandanalysis ofdatamakesitdifficulttodeterminetheactualprevalence of hearing loss in these newborns.37 Another explanation
for thelow rateof hearingloss innewborns found in this
study is the lack of a significant number of mothers who returnforretestingand/ordiagnosis.Thefollow-upforthe audiological diagnosis is essential for an NHS program to succeed. The percentage of those who return for retest-ingand/oraudiologicaldiagnosisafterdischargeisanindex thatdemonstratesboththeefficiencyofthemonitoring pro-graminthenewborn,inthesubsequenthearingassessment phases,aswellasthewillingnessofparentstocompletethe NHSprogram.
Income,loweducationallevel,andlownumberof prena-talconsultationsarereportedintheliteratureasobstacles to NHS completion.35,38,39 The lack of awareness by the
mothercan result in forgetfulness andlack of adherence tothefollow-up.15,40Studieshaveshownthatadherencein
allstagesofNHScanbeattainedwhenthemedicalstaffof thehospital,aswellasnurses,socialworkers,andspeech therapistsareinvolvedintheNHS.23,41---43Oneofthe
sugges-tionsfound intheliteraturetoreducethedropoutrateof theprogramistheaggregationoftheNHSintootherfederal programssuchasneonatalscreening tests,or growthand developmentmonitoringprogramsperformedinoutpatient clinics.23
Anothersuggestionis toadvisemothersabout theNHS andhearinglossinnewbornsindividually,tryingtomaintain afavorableandpeacefulenvironmentfortheemergenceof doubts.Thevocabularybetweentheprofessionaland par-entsshouldbesimpleandclear,andtheadvicecanbegiven byasocialworker.41
Theinterpretationofhearinglossprevalenceshouldbe consideredcarefully,especiallyastherewasno heterogene-ityinthemethodologyusedforhearingscreening,andthe dropoutrateintheretestordiagnosiswasdemonstratedto beveryhighinsomestudies.10,13---15,18,24,25,27,28,30,33,34
While countrieswithwell-established NHS services are currentlyconcernedwithdiagnosisfollow-upand rehabili-tation,Brazil isstillin itsinfancyfor theimplementation ofNHSprograms.Itisessentialtodiscussandorganizeall phasesinordertoachievethegoalofearlydiagnosis.
Conclusion
ThisliteraturereviewshowedthatmostNHSscreening pro-ceduresoccursat publichospitals,andlessthan50%were abletoreachtherate of95% of screenednewborns. Pro-tocolsvaryfromservicetoservice,hinderingcomparisons andtheestablishmentofqualitystandards.Non-adherence to the audiological diagnosis compromises the quality of service and represents one of the major challenges. The occurrence of hearing loss waslower than that expected when compared tothe literature. One factor responsible for this result may be the non-adherence to audiological follow-up.Specificadaptationstotheculturalcontextare necessarytoenableeffectivehearingscreeningprograms.
Conflicts
of
interest
352 CavalcantiHGetal.
References
1.Ministério da Saúde. Diretrizes deatenc¸ão da triagem audi-tiva neonatal. Brasilia:Ministério da Saúde; 2012. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/diretrizes atencaotriagemauditivaneonatal.pdf[cited10.02.13]. 2.American Academy of Pediatrics,Joint Committee onInfant
Hearing.Year2007 positionstatement: principlesand guide-lines for earlyhearing detection and interventionprograms. Pediatrics.2007;120:898---921.
3.Lewis DR,Marone SAM,MendesBCA, Cruz OLM, NóbregaM. Comitê multiprofissional em saúde auditiva COMUSA. Braz J Otorhinolaringol.2010;76:121---8.
4.GATANU.Grupodeapoio àtriagemauditiva neonatal univer-sal;[homepage].Availablefrom:http://www.gatanu.org[cited 20.02.13].
5.World Health Organization. Newborn and infant hearing Screening.In:Currentissuesandguidingprinciplesforaction. OutcomeofaWhoinformalconsultationheldatwho headquar-ters. 2009. Available from: http://www.who.int/blindness/ publications/NewbornandInfantHearingScreeningReport. pdf[cited13.02.13].
6.Tucci DL,MersonMH,WilsonB. Asummaryof theliterature onglobalhearingimpairment:currentstatusandprioritiesfor action.OtolNeurotol.2010;31:31---41.
7.WhittemoreR,KnaflK.Theintegrativereview:update method-ology.JAdvNurs.2005;52:546---53.
8.Joint Commiteeon Infant Hearing.Year position statement: principlesandguidelinesforearlyhearingdetectionand inter-ventionprograms.Pediatrics.2000;106:798---817.
9.Pereira MCCS[dissertation] Estudoretrospectivo de um pro-gramadetriagemauditivaemneonatoselactentesnacidade deSalvador.SãoPaulo:PUCSP;2007.
10.Zumpano CE, Reis CP, Oliveira LFM. Perfil do programa de triagemauditivaneonatal doHospitalde Clínicasda Univer-sidadeFederaldeUberlândia(HC/UFU).In:Annalsofthe27◦
Encontro Internacional de Audiologia. 2012. Available from: http://www.audiologiabrasil.org.br/eiabauru2012/anais2012/ trabalhosselect.php?tt=Busca&idartigo=3309 [cited 22.12.12].
11.JorgeNG[dissertation]TriagemauditivaneonatalnoMunicípio deGuaxupé.MinasGerais,Campinas:UNICAMP;2012. 12.DuranteAS, CarvalloRMM,Costa MTZ, CianciarulloMA,
Voe-glesRL, TakahashiGM,etal. Aimplementac¸ãodeprograma detriagemauditivaneonataluniversalemumhospital univer-sitáriobrasileiro.Pediatria.2004;28:78---84.
13.Pádua FGM, Marone S, Bento RF, Carvallo RMM, Durante AS, Soares JC, et al. Newborn hearing screening program: a challenge for its implantation. Int Arch Otorhinolaryngol. 2005;9:189---94.
14.Onoda RM, Azevedo MF, Santos AMN. Neonatal hearing screening: failures, hearing loss and risk indicators. Braz J Otorhinolaryngol.2011;77:775---83.
15.Hanna KF, Maia PA. Triagem auditiva neonatal: incidên-cia de deficiência auditiva neonatal sob a perspectiva da nova legislac¸ão paulista. Rev Bras Saúde Matern Infant. 2010;10:257---64.
16.ChapChapMJ,RibeiroFM.JCIHguidelines:asuccessful expe-rienceatpublichospitalinSãoPaulo,Brazil.In:Proceedingsof theNHS2010Conference.2010.
17.GelatiCB,HannaKF,RabeloCM,CorreaDRLS,FragaSM.Triagem auditiva neonatalem 11776 neonatos;2009. Available from: http://www.audiologiabrasil.org.br/eiabauru2009/anais select.php?tt=buscaresult&cid=2244[cited22.12.12]. 18.BerniOS,AlmeidaEOC,AmadoBCTA,FilhoNA.Triagem
audi-tiva neonatal universal:índice de efetividade no retestede neonatos de um hospital da rede pública de Campinas. Rev CEFAC.2010;12:122---7.
19.OliveiraES.Triagemauditivaneonataluniversal:resultadosdos trêsprimeirosanoseumhospitalprivado;2011.Availablefrom: http://www.audiologiabrasil.org.br/eiamaceio2011/anais select.php?pg=temas&cid=2898[cited22.12.12].
20.Oliveira ES, Sacco MS. Triagem auditiva neonatal universal: resultados do primeiro ano de implantac¸ão em um hospital público; 2012. Available from: http://www.audiologiabrasil. org.br/eiabauru2012/anais2012/trabalhosselect.php?tt= Busca&idartigo=3370[cited22.12.12].
21.Pereira PKSP, Palma JRM. Implementac¸ão de um programa de triagem auditiva neonatal universal em um hospital geral; 2012. Available from: http://www.audiologiabrasil. org.br/eiabauru2012/anais2012/trabalhosselect.php?tt= Busca&idartigo=251[cited22.12.12].
22.Ruy VAS, Matsuzaki F. Análise da implementac¸ão do pro-grama de triagem auditiva neonatal universal do Hospital Regional de Presidente Prudente; 2012. Available from: http://www.audiologiabrasil.org.br/eiabauru2012/anais2012/ trabalhosselect.php?tt=Busca&idartigo=3433 [cited 22.12.12].
23.Bevilacqua MC, Alvarenga KF, Costa AO, Moret ALM. The universalnewbornhearingscreeninginBrazil:from identifica-tiontointervention.IntJPediatrOtorhinolaryngol.2010;74: 510---5.
24.AlmeidaEOC,StelletALS,SantosRHA,GuimarãesVF,SilvaEF, HenriquesELV,etal.Indicadoresdequalidadenatriagem audi-tivaneonataluniversalnoprogramabebêUnimed-SãoJosédos Campos; 2009. Available from: http://www.audiologiabrasil. org.br/eiabauru2009/anaisselect.php?pg=buscaresult&cid= 2457[cited22.12.12].
25.Barreira-Nielsen C, Neto HAF, Gattaz G. Processo de implantac¸ãodeSaúdeauditivaemduasmaternidadespúblicas. RevSocBrasFonoaudiol.2007;12:99---105.
26.MaggiCR[dissertation]Programadetriagemauditivaneonatal: resultadosdesuaaplicac¸ãoemumHospitalUniversitário.Santa Maria,RS:UFSM;2009.
27.Francesschi CM, Tochetto T, Weich TM. Hearing loss inci-dencein neonatesborn through theBrazilianUnifiedHealth System in Santa Maria; 2010. Available from: http://www. audiologiabrasil.org.br/icaeia2010/ica2010anais.pdf [cited 22.12.12].
28.BoscattoSD,MachadoMS.TestedaorelhinhanohospitalSão VicentedePaulo:levantamentodedados.RevCEFAC.2012 [E-pubaheadofprint].
29.FaistauerM,AugustoTAM,FlorianoM,TabajaraCC,MartiniCM, SchmidtVB,etal.Implementac¸ãodoprogramadetriagem audi-tivaneonataluniversalemhospitaluniversitáriodemunicípio daregiãoSuldoBrasil:resultadospreliminares.RevAMRIGS. 2012;56:22---5.
30.Nascimento AAM, Narciso AR. Triagem auditiva neonatal opcional: resultados de uma maternidade em Maringá-PR. Instituto da audic¸ão. Available from: http://www. institutodaaudicao.com.br/artigos/artigo3.pdf [cited 03.02.13].
31.Mello JM,de La Puente LF,SawasakiLF,Rosa VAD.Critérios de qualidade de um programa de triagem auditiva neona-tal durante dois anos consecutivos; 2011. Available from: http://www.audiologiabrasil.org.br/eiamaceio2011/anais select.php?pg=temas&cid=3029[cited22.12.12].
32.MattosWD,CardosoLF,BissaniC,PinheiroMMC,ViveirosCM, Carreirão Filho W. Análise da implantac¸ão de programa da triagemauditivaneonatalem umhospital universitário.Braz JOtorhinolaryngol.2009;75:237---44.
Overviewofnewbornhearingscreeningprograms 353
34.Seco ALR, Bissani C, Assuiti LC, Pinheiro MMC, Lima AMP, Beresford PC. Follow up of children with failure in new-bornhearing screening inthe UniversityHospital ofFederal Universityof Santa Catarina in 2008; 2010. Available from: http://www.audiologiabrasil.org.br/icaeia2010/ica2010anais. pdf[cited22.12.12].
35.Cavalcanti HG, Guerra RO. The role of maternal socioeco-nomicfactorsinthecommitmenttouniversalnewbornhearing screeningin thenortheastern regionof Brazil.Int JPediatr Otorhinolaryngol.2012;76:1661---7.
36.StörbeckC.Childhoodhearinglossinthedevelopingworld.Int JChildHealthNutr.2012;1:59---65.
37.GarciaBG,GaffneyC,ChaconS,GaffneyM.Overviewof new-bornhearingscreeningactivitiesinLatinAmerica.RevPanam SaludPublica.2011;29:145---51.
38.OgunlesiTA,OgunlesiFB.Familysocio-demographicfactorsand maternalobstetricfactorsinfluencingappropriatehealth-care seekingbehavioursfornewbornjaundiceinSagamu,Nigeria. MaternChildHealthJ.2012;16:677---84.
39.Ensor T, m Cooper S. Overcoming barriersto health service access influencing the demand side. Health Policy Plan. 2004;19:69---79.
40.Arnold CL, DavisTC, Hamiston SG, Bocchini JA, Bass III PF, BocchiniA, et al. Infanthearing screening:stakeholder rec-ommendationsforparent-centeredcommunication.Pediatrics. 2006;117:S341---9.
41.FrancjozoMFC,FernandesJC,LimaMCMP,RossiTRF. Improve-mentofreturnratesinaneonatalhearingscreeningprogram. SocialWorkinHealthCare;2008.p.179---90.
42.ToddNM.Universalnewbornhearingscreeningfollowupintwo Georgiapopulations:newborn,motherandsystemcorrelates. IntJPediatrOtorhinolaryngol.2000;70:7.